
Abstract
The pandemic acute respiratory syndrome coronavirus 2 (SARS-CoV-2) named COVID-19 is causing a severe health emergency, and an individual’s hormonal milieu may play an important role in both susceptibility to infection and severity of clinical course. We analyzed the role of testosterone in the immune response, and we hypothesized possible mechanisms to explain the high incidence of COVID-19 infection and a worse clinical course in elderly male patients. Testosterone may impair the immune response, and this effect could explain the greater susceptibility of men to infection. Transmembrane serine protease 2 (TMPRSS2) plays a crucial role in the entry of the virus into the respiratory epithelial cells, leading to COVID-19 disease. It is crucial to emphasize that testosterone levels and chemical castration (e.g. by androgen deprivation therapy for prostate cancer) may have contrasting roles in the phases of COVID-19 infection. Whereas low testosterone levels may be protective against the initial susceptibility (due to a restoration of immunological functions and a block of TMPRSS2), low testosterone may stimulate a worse clinical course in the advanced COVID-19 infection as it could exacerbate or activate the cytokine storm. If testosterone levels play these different roles, it is necessary to carefully identify patients for any indicated testosterone manipulation.
Keywords
Introduction
The global COVID-19 pandemic is causing a health emergency throughout the world. 1 From the beginning of the pandemic, clinical studies have shown that the main risk factors for mortality from COVID-19 are older age, male sex and comorbidity. 2 Given that male sex and older age are significant risk factors for a severe course of COVID-19, investigators have hypothesized that the hormonal milieu may play an important role both in the susceptibility to infection and in the severity of the clinical course. 3 Differences between the male and female in immune responses are well known.4,5 The two most important factors accounting for the sex bias in immunity are genetics and sex hormones. 6 In this short review, we analyzed the role of testosterone on the immune response and hypothesized possible mechanisms to explain the high incidence of COVID-19 infection and a worse clinical course in elderly male patients. Moreover, given the conflicting findings on the role of testosterone from clinical and epidemiological studies in patients with COVID-19 infection, we tried to propose a model to explain these reports.
Testosterone, immune response, prostate cancer and COVID-19 infection: evidence for a link?
Evidence point to an immunosuppressive role of testosterone on different components of the immune system and also suggests a role of testosterone in the different phases of the immune response. 7 The negative effect of testosterone on the immune response has been evaluated in numerous preclinical studies, and can be summarized in the following effects shown by Trigunaite et al.: 8 androgens (1) appear to be protective in autoimmunity but promoting of cancer, (2) suppress antibody (Ab) response to vaccination and infection, (3) suppress inflammatory immune cells like dendritic cells and macrophages, (4) promote regulatory immune cells like myeloid-derived suppressor cells (MDSCs), and (5) dampen the development and function of T and B cells. Therefore, there is increasing evidence that testosterone acts negatively on the immune response in both bacterial and viral infections, and this powerful immunosuppressive effect could explain the greater susceptibility of males to infections including COVID-19, the lower incidence of autoimmune diseases in men than women, and the lower response to vaccines in men compared with women.9–11 However, exceptions to this assumption have been reported, such as coxsackievirus-induced myocarditis (CIM). According to Di Florio et al., the higher serum T levels compared with low circulating estrogen in males during CIM contributes to reactive oxygen species generation in mitochondria, causing a worse illness progression. 12
An additional human model to study the impact of androgens on the immune response can be offered by patients with Klinefelter syndrome (Ks).13,14 In patients with Ks, azoospermia and infertility are almost inevitably present; however, a broad spectrum of phenotypes has been described, probably due to a different profile of testosterone levels and mosaic forms of the syndrome.15,16 Oketni et al. evaluated the immunological profile of patients with Ks and idiopathic hypogonadism without replacement therapy, suggesting that both humoral and cellular immunity is enhanced in male hypogonadism. Moreover, Ks patients had increased frequency of anti-extractable nuclear Ab and anti-cardiolipin Ab positivity compared with idiopathic hypogonadotropic patients. 17 The tendency to develop autoimmunity in Ks could be due to the expression of additional active genes present on the X chromosome, as recently proposed by Wang et al. 18 However, it is also possible that in Ks patients testosterone deficiency and increased levels of estradiol are contributing factors for this enhanced auto-Ab production. These data suggest a role of hypogonadism in the immune response, including autoimmunity. Indeed, Ks is strongly associated to autoimmune diseases like systemic lupus erythematosus and rheumatoid arthritis.19–21 Importantly, testosterone replacement therapy has been tested in animal and human models of autoimmune disease with encouraging results.22–24
Another important field in which the link between testosterone levels and immunological response could be speculated is prostate cancer (PC) and its treatment, mainly androgen deprivation therapy (ADT). PC is an age-related disease and ADT is the first-line treatment for locally advanced and metastatic disease. 25 If testosterone impairs the immune response, we may predict that ADT can restore immune function and protect against infections. However, to date there are no clinical data on the benefit of ADT in microbial infection. In contrast, there is indirect evidence that supports the role of ADT in activating the immune system. 26 Thymic involution can be reversed in mouse and rat models after orchiectomy, and this regrowth is characterized by an increase in the weight and cellularity of the thymus. Moreover, this can be reversed when androgens are re-administered to the castrate subject.27,28 Sex steroid ablation significantly enhances lymphopoiesis, as reported by Goldberg et al. in an autologous hematopoietic stem cell transplantation mouse model. 29 These observations confirm that androgens have an immunosuppressive effect, and ADT might function to reverse this suppression. If testosterone has an immunosuppressive action, we can expect it to play different roles in the various stages of the natural history of COVID-19 infection.
Androgen deprivation therapy and COVID-19 susceptibility
SARS-CoV-2 viral entry into host cells is dependent on angiotensin converting enzyme 2 (ACE2) and transmembrane serine protease 2 (TMPRSS2), which have been found to be expressed in human lungs and other tissues, including prostate and testis. 30 TMPRSS2 plays a crucial role in the entry of the SARS-CoV-2 virus into the respiratory epithelial cells, leading to COVID-19 disease. 31 TMPRSS2 is expressed in prostate epithelium and is regulated by androgen receptor (AR). Men diagnosed with PC and treated with the luteinizing hormone-releasing hormone (LHRH) agonist leuprolide, or doses of estradiol sufficient to induce castrate serum levels of testosterone, showed significantly lower TMPRSS2 transcripts, when compared with untreated controls (p < 0.01). 32 The finding that TMPRSS2 plays a crucial role in the entry of the SARS-CoV-2 virus into the respiratory epithelial cells, leading to COVID-19 disease, has led to speculation of a role of ADT in patients with COVID-19 infection. In this context, ADT could be useful through a dual mechanism: (1) blocking TMPRSS2 by interfering with the entry of the virus at the lung level, and (2) improving the immune response through blunting of the immunosuppressive effects of testosterone. However, epidemiological data in patients with PC under ADT have shown conflicting results. Montopoli et al. 33 analyzed the role of ADT in a large and unselected series of patients with PC obtained from the cancer database of Veneto (Italy). They observed that patients on ADT had lower rates of SARS-Cov-2 infection [4/5273 cases versus 114/37 161, odds ratio (OR) 4.05, 95% confidence interval (CI) 1.55–10.59, p = 0.00043]. In contrast, Caffo et al. 34 observed a higher lethality from SARS-CoV2 (25% versus <13.0%), when compared with the population of infected Italian males of the same age among a population of metastatic hormone-sensitive PC (mCSPC) and metastatic castration-resistant PC (mCRPC) on ADT. More recently, Klein et al. 35 did not observed a protective role of ADT from SARS-Cov-2 infection (OR 0.93, 95% CI 0.54–1.61, p = 0.8) in a cohort of 1,779 men with PC. Given the differences in the populations analyzed, the conflicting results of these studies could be consistent with a more complex role of testosterone in the immune response and the clinical course and pathophysiology of patients with COVID-19 infection. 3
Pathogenesis and clinical course of COVID-19 infection: hypothesis for a double-edged role of testosterone
Clinical manifestations of COVID-19 infection vary from asymptomatic or pauci-symptomatic cases to complicated cases that develop severe pneumonia and lead to death. 36 Acute respiratory distress syndrome (ARDS) represents the final stage for many critically ill patients, and evidence suggests a specific role for a cytokine storm. 37 Since the beginning of COVID-19 infection, it is known that the severe course of the disease occurs mostly among elderly patients. 38 The relationship between testosterone levels and age is well documented. It is generally known that during life, testosterone levels decrease after puberty.39,40 The incidence of low testosterone and symptoms of hypogonadism in men aged 40–79 years varies from 2% to 6%41,42 and hypogonadism is more prevalent in the oldest men with obesity and co-morbidities such as dysmetabolic disturbances. 40 Moreover, it is generally accepted that levels of testosterone <300 ng/dl can be regarded as the cut-off to define that a patient is affected by hypogonadism. 43
Based on the role of androgens in the immune response and on the variation in androgen levels throughout life, we may speculate that testosterone could play a double-edged role in the natural history of COVID-19 infection. 44 In the early phase, the immunosuppressive action of testosterone could explain males’ greater susceptibility to infection when compared with women in all age groups. When the infection has been established, in elderly males who frequently develop ARDS lower testosterone levels related to age could result in a lower immunosuppressive effect and thus a more robust cytokine response. In the aging male, a lower testosterone level is associated as a risk factor for the development of illnesses such as hypertension, diabetes and cardiovascular disease, and on proinflammatory cytokines.3,45,46 Therefore, hypogonadism may have a protective role on the initial COVID-19 infection, but may also lead a patient toward a more severe clinical course. Based on these considerations we can also expect that ADT for PC may lower susceptibility to COVID-19 infection and lead to a worse course in an advanced phase (Figure 1).
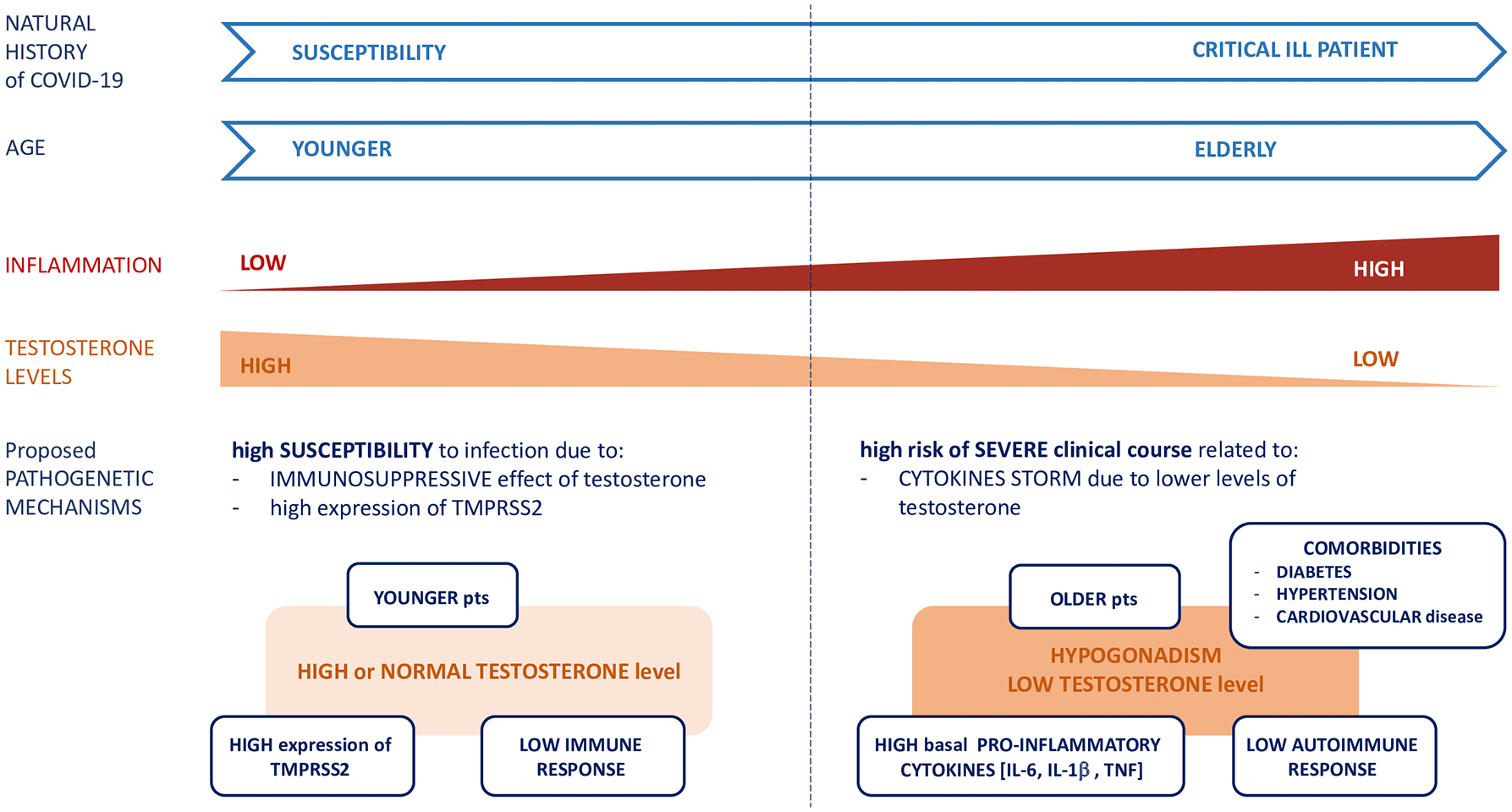
Double-sided role of testosterone in COVID-19 infection related to male age and clinical course.
Testosterone levels and severity of clinical course in patients with COVID-19 infection
Given the immunosuppressive effect of testosterone, we can expect that patients with COVID-19 infection and ARDS have lower testosterone levels. Clinical studies on this topic seem to confirm this finding. First, Rastelli et al. 47 showed that lower baseline total testosterone levels predict poor prognosis and mortality in SARS-CoV-2-infected men in a series of 31 male patients affected by SARS-CoV-2 pneumonia and recovered in the respiratory intensive care unit. Similar results were reported by Salciccia et al., 48 where total testosterone levels were significantly lower in the ARDS patients compared with patients without ARDS (p = 0.003) and higher serum testosterone levels were independently associated with a lower risk of invasive oxygenation (OR: 0.43, 95%CI: 0.23–0.85; p = 0.016). In addition, low total testosterone levels were associated with a worse clinical COVID-19 phenotype, and inversely correlated with interleukin-6 (IL-6) levels (p = 0.002). Çayan et al. 49 investigated the effect of serum total testosterone on the prognosis of a large prospective cohort of 221 consecutive male patients (>18 years old) with laboratory-confirmed SARS-CoV-2 who had been hospitalized due to COVID-19. They observed that baseline serum total testosterone levels were negatively associated with ICU admission (p = 0.001). Moreover, they observed that serum T levels significantly decreased from pre-COVID-19 level (458 ± 198 ng/dl) to 315 ± 120 ng/dl at the time of COVID-19 (p = 0.003). This observation confirms not only that hypogonadism is a risk factor for a worse clinical course, but also suggests that hypogonadism and the consequent loss of immunosuppressive effects may represent a pathogenetic mechanism of the virus through testicular involvement. There is some preliminary evidence that the testis may be a target of SARS-Cov-2: SARS-CoV-2 may enter into the host cell by binding to ACE2 30 that is expressed in Leydig and Sertoli cells, as observed by several authors. 50 However, the expression of an entry route at the testicular level is not sufficient to confirm that the testis represents a target organ for SARS-Cov-2. Indeed, the virus should be isolated from testicular specimens of patients with COVID-19 infection or detected in semen samples. Li et al. 51 reported the presence of SARS-CoV-2 in semen samples of six patients; however, these data were not confirmed in subsequent studies.52,53 Given the methodological differences and the type of population analyzed in these studies, seminal fluid as a possible route of transmission remains controversial. 54 It is important to note that one study did report a case of male patient who died from COVID-19 infection in which SARS-Cov-2 was isolated from testis specimen, 55 while others have failed to prove this finding. 52 However, in all these studies a significant seminiferous tubular injury reduced Leydig cells, and mild lymphocytic inflammation was observed. 55 The results of these studies do not allow us to state that SARS-Cov-2 can affect the testis like other viruses (i.e. HIV, mumps), yet they highlight that the testes of patients affected by SARS-Cov-2 can be damaged both in the seminiferous component and in the Leydig cells, likely as a consequence of a generalized inflammatory state. 56
Testosterone target therapy: future strategies in patient with COVID-19 infection
The discovery of the role of TMPRSS2 in the entry of the SARS-CoV-2 virus into the respiratory epithelial cells led to the speculation for a role of ADT in the treatment of patients with COVID-19 infection.32,33 To date, on Clinicaltrial.gov there are two trials involving drugs used for ADT in the treatment of COVID-19 patients: Degarelix (NCT04397718) a gonadotropin-releasing hormone (GnRH) antagonist used in metastatic Hormone Sensitive Prostate Cancer (mHSPC), 57 and Enzalutamide (NCT04475601), a new generation anti-androgen inhibiting the expression of androgen-regulated proteins, such as TMPRSS2, commonly used in mCRPC. All these studies are in the recruiting stage and involve critically ill patients with COVID-19 infection. Based on the controversial clinical data reported by previous experiences,33–35 and the potential double-edged role of testosterone in the natural history of COVID-19 infection, we may speculate that ADT could be contraindicated in a critically ill patient, as the loss of the immunosuppressive effect of circulating testosterone could exacerbate the cytokine syndrome. If testosterone levels play a different role in the susceptibility and overt disease phases, it is necessary to carefully select the type of patient as well as the indicated testosterone manipulation (testosterone replacement therapy or ADTs) (Figure 2). This aspect clearly has important clinical repercussions in patients with PC receiving ADT or candidates for ADT. If low testosterone levels give an advantage in the susceptibility phase to infection due to a restoration of immunological functions and through the block of TMPRSS2, we can hypothesize that ADT could represent a prevention strategy for patients at increased risk of mortality from COVID-19. In this context, one trial is available on clinicaltrial.gov (searched on) with the aim to explore the protective role of dutasteride in patients with COVID-19 infection not hospitalized (NCT04446429). Dutasteride is a 5α-reductase inhibitor (5-ARI) able to block conversion of testosterone to dihydrotestosterone, commonly used for benign prostatic hyperplasia and androgenetic alopecia with a better tolerability profile than ADT. If low testosterone levels can protect from infection, hypogonadism represents a clear risk factor for unfavorable results when the infection has occurred. Available clinical data indicate low testosterone levels as a risk factor for the need of assisted mechanical ventilation and poor outcomes in patients with COVID-19 infection.47–49 Screening for low testosterone levels is needed for early identification and treatment of men at high risk of mortality from COVID-19. 58 Currently testosterone replacement therapy is recommended in hypogonadal patients mainly for its effects on erectile function, cognitive function and mineral bone density. However, there are consistent data on the role of testosterone replacement therapy as modulator of the immune response in patients with Acquired Immune Deficiency Syndrome (AIDS) and autoimmune diseases.24,59,60 The effect of testosterone supplementation therapy is associated with a reduction or complete abrogation of spontaneous ex vivo production of IL-1β, IL-6 and Tumor Necrosis Factor (TNF)-α as reported by Corrales et al. 61 Given the effect on proinflammatory cytokines and the favorable safety profile of testosterone supplementation therapy, we can hypothesize a role for testosterone therapy in patients with hypogonadism and COVID-19 infection, in which cytokine syndrome plays a key role. To date, there have been no clinical trials on this topic; however, testosterone supplementation therapy should be tested in hypogonadal patients with COVID-19 infection in randomized controlled clinical trials.
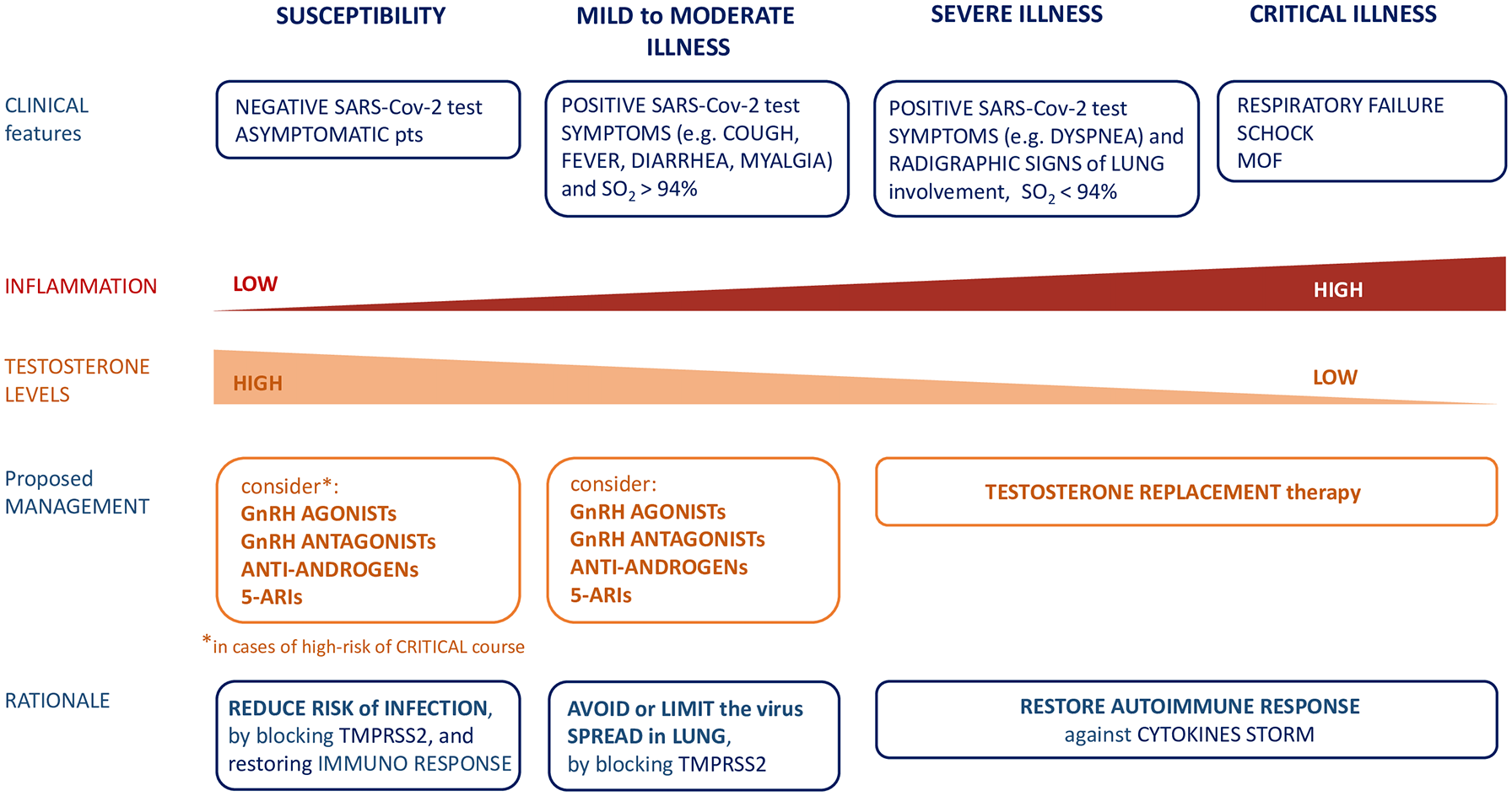
Proposed management of COVID-19 patients according to testosterone levels and stage of disease.
Conclusions
Testosterone levels and their effect on the immune response can explain some of the differences in COVID-19 incidence and mortality between males and females. However, it is crucial to emphasize that testosterone and testosterone ablation used in PC may have opposing roles in the different phases of COVID-19 infection: low testosterone levels may be protective against the initial susceptibility and stimulate a worse clinical course in the advanced COVID-19 infection.
Footnotes
Author contribution(s)
Salciccia, Stefano: Corresponding Author, Conceptualization, Methodology, Writing-original draft; Del Giudice, Francesco: Investigation, Methodology, Writing-review & editing; Eisenberg, Michael: Formal analysis, Methodology, Writing-review & editing; Mastroianni, Claudio Maria: Methodology, Supervision, Writing-review & editing; De Berardinis, Ettore: Data curation, Investigation, Writing-review & editing; Ricciuti, Gian Piero: Methodology, Validation, Writing-review & editing; Viscuso, Pietro: Data curation, Investigation, Writing-review & editing; Zingaropoli, Maria Antonella: Data curation, Formal analysis, Writing-review & editing; Pasculli, Patrizia: Data curation, Investigation, Writing-review & editing; Ciardi, Maria Rosa: Data curation, Formal analysis, Methodology, Writing-review & editing; Sciarra, Alessandro: Conceptualization, Methodology, Writing-original draft; Maggi, Martina: Data curation, Methodology, Writing-original draft.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.