
Abstract
Background:
Criteria for the preoperative diagnosis of non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) have not yet been confirmed. This study aimed to analyze differences in clinicopathological characteristics between follicular variant of papillary thyroid carcinoma (FVPTC) subtypes to determine which parameters are relevant in differentiating NIFTP from other variants.
Methods:
We retrospectively analyzed the records of 199 patients with a preoperative diagnosis of FVPTC who underwent thyroid surgery at Seoul St. Mary’s Hospital (Seoul, Korea) from 2011 to 2015. Clinicopathological features were analyzed retrospectively via a complete review of medical charts and pathology reports of patients.
Results:
The NIFTP and invasive encapsulated FVPTC (EFVPTC) groups showed relatively benign features, with a majority of the patients categorized as Bethesda category III (25.8% and 25.6%, respectively) or IV (34.8% and 30.2%, respectively), while the infiltrative FVPTC group showed more malignant features, with more patients categorized as category V (28.6%) or VI (47.6%) (p < 0.001). BRAF V600E mutations were significantly less prevalent in the NIFTP group (0%) and invasive EFVPTC group (4.7%) compared with the infiltrative FVPTC group (34.9%) (p < 0.001). Multivariate analysis showed that absence of BRAF V600E mutation (OR 20.311, p = 0.004) and lymph node metastasis (odds ratio 10.237, p = 0.004) were significantly associated with NIFTP.
Conclusion:
Although Bethesda category was a statistically significant factor in distinguishing FVPTC subtypes, it was not effective in conclusively distinguishing NIFTP and invasive EFVPTC. Absence of BRAF V600E mutation and lymph node metastasis are important features in distinguishing NIFTP from other subtypes.
Introduction
Follicular variant of papillary thyroid carcinoma (FVPTC) is the second most common subtype of papillary thyroid carcinoma (PTC) 1 and is composed of two distinct subgroups, encapsulated (EFVPTC) and infiltrative. EFVPTC is further subdivided into non-invasive EFVPTC and invasive EFVPTC based on invasion of the capsule by tumor cells.2,3 Overall, non-invasive EFVPTC exhibits a less aggressive clinical course compared with other variants of PTC.4,5 In 2016, Nikiforov et al. 3 suggested that non-invasive EFVPTC should be renamed to exclude the word ‘carcinoma’ from its nomenclature and introduced the term “non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP)”. This was an attempt to better reflect the indolent nature of NIFTP as compared with invasive EFVPTC or infiltrative FVPTC. 3 For a diagnosis of NIFTP, the lesion needs to be encapsulated or clearly demarcated and show a follicular growth pattern with no well-formed papillae. 6 Absence of psammoma bodies, vascular or capsular invasion, and tumor necrosis are also characteristic of NIFTP. Meticulous examination of the entire tumor capsule and tumor is required to exclude the presence of papillary structures and other histologic features found in classic PTC.3,7
Although the histopathologic features and diagnostic criteria of NIFTP are well-determined, criteria for preoperative diagnosis using sonographic or fine needle aspiration (FNA) findings have not yet been confirmed.8,9 A few studies have attempted to differentiate NIFTP, invasive EFVPTC, and infiltrative FVPTC based on sonographic or histologic findings.9,10 NIFTP generally shows a less aggressive clinical course than infiltrative FVPTC and other PTC variants. Thus, as a general practice guideline, single lobectomy alone is considered sufficient for treatment of NIFTP. 11 Accurate preoperative diagnosis of NIFTP would help to reduce unnecessary extensive surgery and avoid unnecessary radioactive iodine treatment. Therefore, this study aimed to analyze differences in clinicopathological characteristics between FVPTC subtypes to determine which parameters are relevant in differentiating NIFTP from other variants.
Materials and methods
Patients
We reviewed the medical records, radiological examinations, and pathologic slides of 206 patients diagnosed with FVPTC based on the final surgical pathology result. Patients underwent thyroid surgery at Seoul St. Mary’s Hospital (Seoul, Korea) from 2011 to 2015. Part of the current dataset was used in our previous studies.12,13 One hundred and ninety-nine patients were included for analysis, as seven patients were excluded due to loss of follow-up. Approval was obtained from the Institutional Review Board of Seoul St. Mary’s Hospital, Catholic University of Korea (No. KC20RISI0411), which waived the requirement for informed consent due to the retrospective nature of the study.
Ultrasonography
Ultrasonography (US) examination is a standard diagnostic tool for evaluating thyroid lesions. Based on sonographic findings, FNA biopsy can be performed, which plays a crucial role in preoperative histopathologic diagnosis of thyroid nodules. The Thyroid Imaging Reporting and Data System guidelines were revised in 2017, which categorize thyroid nodules based on sonographic findings as follows: 1, no nodule; 2, benign: spongiform or partially cystic nodule with comet tail artifact or pure cyst; 3, low suspicion: partially cystic or iso-hyperechoic nodule without any of three suspicious US features (microcalcification, non-parallel orientation/taller than wide, and spiculated/microlobulated margin); 4, intermediate suspicion: solid hypoechoic nodule without any of three suspicious US features or partially cystic or iso-hyperechoic nodule with any of three suspicious US features; and 5, high suspicion: solid hypoechoic nodule with any of three suspicious US features. 14
All preoperative USs were performed by experienced radiologists who specialized in thyroid imaging. FNA cytology and core needle biopsy (CNB) were performed with procedural guidance using real-time US.
Cytologic and histologic diagnoses
Cytology and pathology slides were examined by a single pathologist with proficient experience in thyroid cancer. According to the Bethesda System for Reporting Thyroid Cytopathology, the FNA cytology and CNB results were classified as follows: category I (non-diagnostic), II (benign), III (atypia of undetermined significance), IV (follicular neoplasm), V (suspicious for malignancy), and VI (malignant).
All patients underwent lobectomy alone or total thyroidectomy with or without modified radical neck dissection. NIFTP and FVPTC were diagnosed according to the criteria proposed by Nikiforov et al.3,7 and the World Health Organization Classification of Tumours of Endocrine Organs. 15 The whole tumor specimen was submitted for pathologic examination. The revised criterion including the absence of papillae was applied for the diagnosis of NIFTP and FVPTC. 7 FVPTC was subdivided into invasive EFVPTC and infiltrative FVPTC. The exclusion criteria for NIFTP included any true papillae, necrosis, psammoma bodies, mitosis (⩾3 per 10 high-power fields), or transcapsular/vascular invasion. The representative cytologic and histologic images of NIFTP are shown in Figure 1.

Representative cytologic and histopathologic findings in non-invasive follicular thyroid neoplasm with papillary-like nuclear features with NRASQ61R mutation. (a) Cytologic findings show microfollicles with nuclear features of papillary thyroid carcinoma, including chromatin pallor, nuclear grooves, and nuclear membrane irregularities (ThinPrep liquid based preparation, Papanicolaou stain, ×400). (b) Histologic examination reveals a well-defined follicular-patterned tumor with a fibrous capsule fully encapsulating the entire nodule (hematoxylin–eosin stain, ×40). (c) High-power view of the same tumor shows a microfollicular growth and no true papillae. Tumor cells reveal nuclear enlargement, nuclear overlapping, nuclear grooves, and chromatin clearing (hematoxylin–eosin stain, ×400).
Molecular analysis of BRAF V600E and NRAS mutations
Genomic DNA was isolated from 10-μm-thick formalin-fixed, paraffin-embedded tissue sections and was used for molecular testing for BRAF and NRAS. Tumor areas were manually dissected under a stereomicroscope. Mutational analysis of BRAF V600E was performed with Sanger sequencing, as previously described. 12 NRAS mutation was performed deleted using Sanger sequencing or pyrosequencing, as previously described.12,16 NRAS mutational analysis was performed by extracting DNA from unstained paraffin-embedded (FFPE) tissue sections of specimens surgically resected after manual dissection of the tumor area. Polymerase chain reaction (PCR) using primers targeting codon 61 was performed using the PyroMark PCR kit, and pyrosequencing was performed. The NRAS mutation status was considered positive if the mutant allele percentage was ⩾5%.
Statistical analysis
Continuous variables are reported as means with standard deviation; categorical variables are presented as numbers with percentages. Student’s t-test was used to compare continuous variables and Pearson’s chi-square test or Fisher’s exact test was performed to compare categorical variables as appropriate. Univariate and multivariate logistic regression analyses were performed to identify factors associated with malignancy; results are presented as odds ratios (ORs) with 95% confidence intervals (CIs). p < 0.05 was considered significant. All statistical analyses were performed using Statistical Package for the Social Sciences software, version 24.0 (IBM Corp., Armonk, NY, USA).
Results
Comparison of baseline clinical characteristics between NIFTP and FVPTC subtypes
The clinical characteristics of FVPTC subtypes are summarized in Table 1. There were no significant differences according to age or gender. The differences in Bethesda category were statistically significant (p < 0.001). The NIFTP and invasive EFVPTC groups were more frequently diagnosed as Bethesda category II or III than infiltrative FVPTC. However, in the infiltrative FVPTC group (n = 63), only two (3.0%) patient were classified under categories II and III. Meanwhile, most patients with infiltrative FVPTC were categorized under class IV (20.6%), V (28.6%), or VI (47.6%).
Clinical characteristics of NIFTP and FVPTC subtypes.

Data are expressed as number (%) or mean ± standard deviation.
A p-value of <0.05 was considered statistically significant.
Comparison between subtypes of FVPTC.
Comparison between the NIFTP and non-NIFTP groups.
EFVPTC, encapsulated follicular variant papillary thyroid carcinoma; FVPTC, follicular variant papillary thyroid carcinoma; mRND, modified radical neck dissection; NIFTP, non-invasive follicular thyroid neoplasm with papillary-like nuclear features; TT, total thyroidectomy.
The clinical characteristics between the NIFTP and non-NIFTP groups were compared. Based on the Bethesda category, the FNA cytology results showed that the NIFTP subgroup had less aggressive features than the non-NIFTP group. The NIFTP group was commonly classified under categories III (25.8%) and IV (34.8%), and the non-NIFTP group under categories V (25.5%) and VI (33.0%). The results significantly differed (p = 0.011).
Comparison of baseline clinicopathological characteristics between NIFTP and FVPTC subtypes
Table 2 shows the differences in the clinicopathological characteristics of FVPTC subtypes. Pathological features such as tumor size, thyroiditis, and multifocality did not significantly differ between the NIFTP and non-NIFTP subtypes. Extrathyroidal extension (ETE) was exclusively found in infiltrative FVPTC and not in the NIFTP or invasive EFVPTC groups. The prevalence of NRAS mutation was significantly higher in NIFTP (32.6%) and invasive EFVPTC (32.6%) compared with infiltrative FVPTC (11.1%) (p = 0.006). BRAF V600E mutation was not found in NIFTP, but found in two (4.7%) invasive EFVPTCs and 22 (34.9%) infiltrative FVPTCs (p < 0.001). Lymphatic invasion was significantly more prevalent in the infiltrative FVPTC than in invasive EFVPTC and NIFTP (p = 0.006). Vascular invasion was commonly observed in invasive EFVPTC and infiltrative FVPTC (p = 0.007).
Clinicopathological characteristics of NIFTP and FVPTC subtypes.

Data are expressed as number (%) or mean ± standard deviation.
A p-value of <0.05 was considered statistically significant.
Comparison between subtypes of FVPTC.
Comparison between the NIFTP and non-NIFTP groups.
EFVPTC, encapsulated follicular variant papillary thyroid carcinoma; ETE, extrathyroidal extension; FVPTC, follicular variant papillary thyroid carcinoma; NIFTP, non-invasive follicular thyroid neoplasm with papillary-like nuclear features.
Lymph node metastasis was noted in one (1.1%) of 89 patients with NIFTP, three (7.0%) of 43 patients with invasive EFVPTC, and 22 (31.7%) of 63 patients with infiltrative FVPTC (p < 0.001).
Univariate and multivariate analyses of clinical parameters associated with NIFTP
Table 3 shows the results of the univariate and multivariate analyses of clinical parameters associated with NIFTP. Univariate analysis showed that Bethesda category III (OR 5.750, p = 0.050), absence of lymphatic invasion (OR 11.234, p = 0.021), negative BRAF V600E mutation (OR 25.756, p = 0.002), and absence of lymph node metastasis (OR 12.054, p = 0.001) were significantly associated with NIFTP. Among these risk factors, multivariate analysis showed that negative BRAF V600E mutation (OR 20.311, 95% CI 2.639–156.341, p = 0.004) and absence of lymph node metastasis (OR 10.237, 95% CI 2.031–41.525, p = 0.004) were significantly associated with NIFTP.
Univariate and multivariate analyses of clinical parameters associated with non-invasive follicular thyroid neoplasm with papillary-like nuclear features.
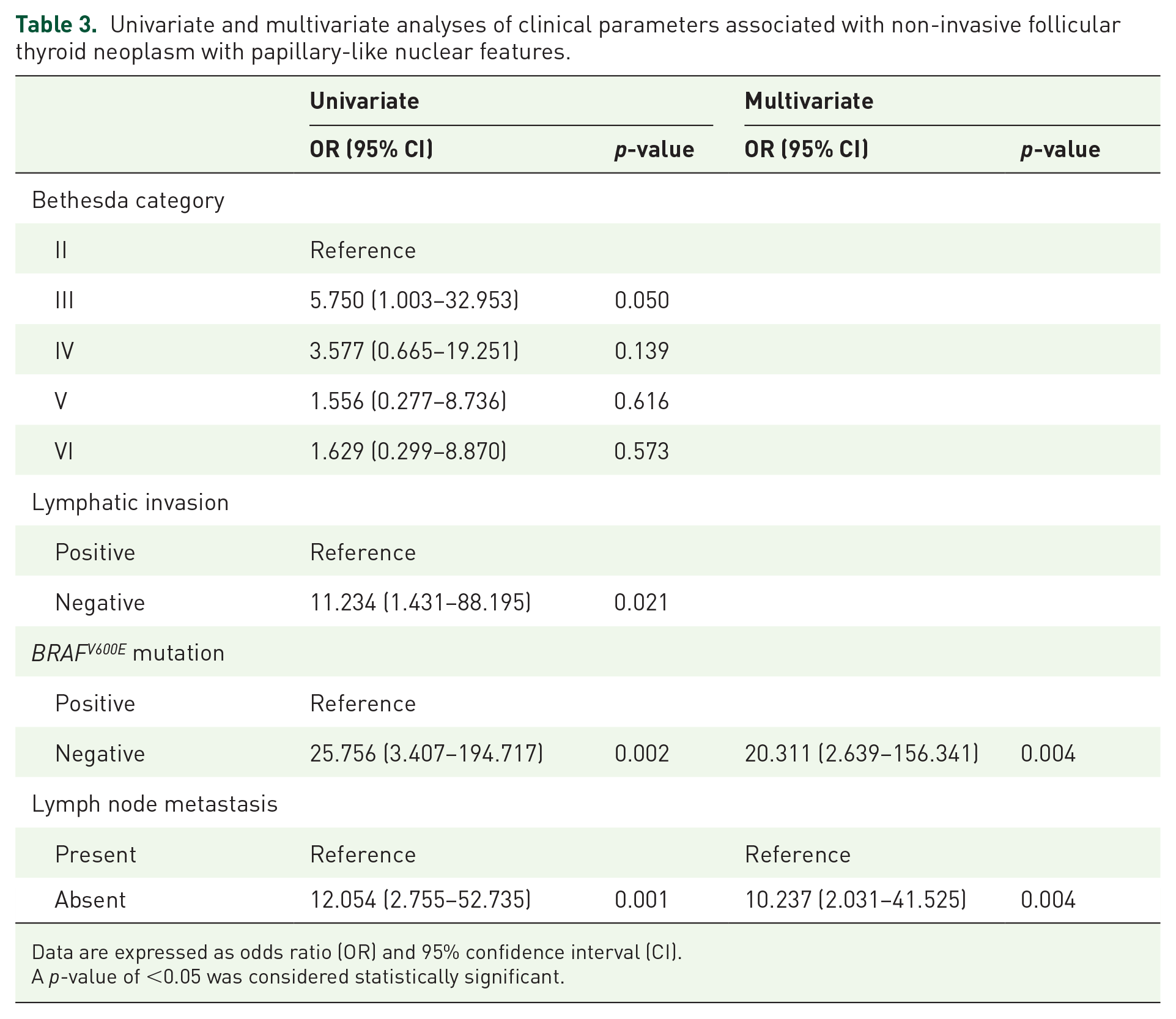
Data are expressed as odds ratio (OR) and 95% confidence interval (CI).
A p-value of <0.05 was considered statistically significant.
Discussion
The incidence of FVPTC and the diagnosis of PTC rapidly increased after 2000. 17 Thus, FVPTC is considered a heterogeneous disease with two distinct biological groups. 18 The two main subtypes of FVPTC are infiltrative and encapsulated with invasion. Infiltrative FVPTC has an infiltrative border without a fibrous capsule.3,6,19 Since EFVPTC without vascular or capsular invasion has an excellent prognosis after complete resection, even when treated with lobectomy alone,3,11 the term NIFTP was proposed to prevent overtreatment of these indolent tumors.3,7,11 NIFTP commonly has indolent behavior, and lobectomy alone is a sufficient treatment. Neither total thyroidectomy nor radioiodine treatment is required.4,9
At present, the preoperative differentiation of FVPTC subtypes is difficult. The diagnosis of NIFTP can only be made after surgical resection. Several studies have investigated preoperative US or FNA cytology findings associated with NIFTP, as both diagnostic modalities play an important role in early evaluation of thyroid nodules.
Hahn et al. 10 reported that increasing tumor invasiveness is positively correlated with more suspicious ultrasound features as defined by the Korean Society of Thyroid Radiology Thyroid Imaging, Reporting, and Data System (K-TIRADS) and American Thyroid Association guidelines; a significantly higher proportion of non-NIFTP lesions were classified as K-TIRADS 5 compared with NIFTP lesions. Lee et al. 20 reported that although K-TIRADS 3 was the most common sonographic classification in the NIFTP and invasive EFVPTC groups, no NIFTP was classified as K-TIRADS 5, in contrast to the invasive EFVPTC group.
In a retrospective NIFTP study, Rosario et al. 21 reported that approximately 25% of patients exhibited cytology suspicious for malignancy while cytology was indeterminate in approximately two-thirds. However, further cytological and/or molecular characteristics need to be identified for accurate diagnosis; a diagnosis of NIFTP cannot be rendered on cytological grounds and requires examination of a surgical specimen. 22 A meta-analysis by Bongiovanni et al. reported FNA findings in NIFTP patients similar to our results, with most patients showing indeterminate findings (Bethesda category I, 3%; II, 10%; III, 30%; IV, 21%; V, 24%; VI, 8%). 23 In a study by Song et al., 24 NIFTP were frequently assigned an indeterminate cytological diagnosis, and most were classified under category III or IV based on the Bethesda system, making the preoperative prediction of NIFTP impossible. Our findings in preoperative FNA cytology differ from previous studies. The proportions of category VI in NIFTP, invasive EFVPTC, and infiltrative FVPTC were 21.3%, 11.6%, and 47.6%, respectively, in our study. This may be attributed to the fact that all patients underwent surgery. Among them, one-third had undergone total thyroidectomy. However, our results are in accordance with previous findings that Bethesda categories III and IV were the most common FNA cytology findings. Univariate analysis also identified Bethesda category III as a significant factor associated with NIFTP.
BRAF V600E is an oncogenic mutation of the BRAF gene, which causes a valine-to-glutamic acid change in codon 600 of the BRAF protein and is associated with more invasive clinicopathologic characteristics of PTC, such as LN metastasis and ETE, and tumor aggressiveness. 25 NRAS mutations occur in 5–15% of patients with thyroid cancers. Moreover, they are a characteristic of the follicular subtype and are found in tumors without BRAF mutations or RET/PTC rearrangements. NRAS mutations in the follicular thyroid carcinoma have been associated with more aggressive disease and distant metastasis. 26
NIFTPs predominantly have RAS-like mutations.3,19,27 Point mutations in the RAS (NRAS, HRAS, or KRAS) genes are observed in up to 60% of patients with NIFTP, and other point mutations are found in the EIF1AX, PTEN, and DICER1 genes. Gene fusions are noted in the PPARG and THADA genes. 24 BRAF V600E mutations are not detected in NIFTP. However, BRAF K601E mutations are found in about 5% of patients with NIFTP. 19
Paulson et al. 28 reported that among 27 RAS-mutant thyroid tumors, 15 (56%) showed NRAS mutation, nine (33%) showed HRAS mutation, and three (11%) showed KRAS mutation. Twenty-four cases had preceding FNA biopsy results and NIFTP accounted for 59% of the RAS-mutant carcinomas and 63% of the RAS-mutant carcinomas with indeterminate diagnosis. In our study, NRAS mutation was more commonly found in NIFTP and invasive EFVPTC than in infiltrative FVPTC. However, NRAS mutation could not be used to differentiate NIFTP from invasive EFVPTC.
A previous study has found that a small proportion of patients with NIFTP harbored BRAF V600E mutations. However, complete examination of the parenchyma and the strict use of the no papillae criterion for the diagnosis of NIFTP may have excluded these cases. 12 After the molecular examination of 39 NIFTP cases, Brandler et al. reported that most (67%) patients harbored RAS mutations, of which 72% were NRAS mutations. None of the patients showed BRAF V600E mutations, which is in accordance with previous studies.
According to previous reports, FVPTCs have a relatively benign appearance on US. Common features include solid internal content, ovoid-to-round shape, smooth margin, isoechogenicity, and hypoechoic rim, which are similar to the features of other follicular cell tumors, including nodular hyperplasia, follicular adenoma, and even follicular carcinoma.10,29 Yang et al. 30 compared US features of NIFTPs and invasive EFVPTCs and found that NIFTPs were typically well-circumscribed, oval-to-round with a hypoechoic rim, and hypervascular; microfollicular nodules were hypoechoic while macrofollicular nodules were isoechoic. In comparison, invasive EFVPTCs were distinguished by hypoechogenicity with irregular or lobulated margins and infiltrative FVPTCs by avascularity and hypoechogenicity with blurred margins. Although we did not compare US features in this study, further studies should investigate sonographic features associated with NIFTP.
Final surgical pathology in this study suggested that the histopathologic characteristics of NIFTP showed a less aggressive nature compared with non-NIFTP. Features such as ETE and lymphovascular invasion were predominantly found in the non-NIFTP group. However, not all reports have consistently shown that NIFTP has a completely benign clinical course. Parente et al. 31 identified 102 patients with NIFTP after reviewing 4790 cases of PTCs from Canada. Of these patients, five (4.9%) presented with lymph node metastasis and one with distant metastasis. Despite complete submission of the tumor nodule and adjacent parenchyma, the series showed distant metastasis characterized by a 6.4-cm tumor, which was non-invasive based on an evaluation of serial sections. Studies have shown that these findings may indicate a limitation in pathology practice guidelines in the evaluation of NIFTP. 31 Kim et al. 32 reported that nine (12%) of 74 patients with NIFTP presented with lymph node metastasis in Korea. However, five of nine had coexisting PTCs. Hence, the high proportion of patients with lymph node metastasis may not be representative, and the risk of occult malignancy should always be considered. In our study, one of 89 patients with NIFTP presented with lymph node metastasis. Although the overall clinical behavior of NIFTP, compared with non-NIFTP, is favorable, these findings confirmed that NIFTP should be classified as a borderline or low-grade tumor.31,32
Although surgical resection is the treatment of choice for NIFTP in Korea, its indolent behavior suggests that conservative management may be sufficient. NIFTP behaves indolently in a benign fashion, similar to follicular adenoma. This distinctive clinical behavior is further supported by its molecular profile: NIFTPs have a molecular profile similar to follicular adenoma or carcinoma. On the other hand, infiltrative FVPTCs have molecular profiles that more resemble classical PTCs.12,33 Considering that most NIFTPs have indeterminate cytology on FNA cytology, initial conservative therapy and watchful surveillance may precede surgery. Since an accurate diagnosis ultimately depends on the final pathology of the resected specimen, individualized therapy based on molecular findings may be considered.
There are several limitations to our study. First, this was a retrospective analysis of patients from a single center, which can lead to selection bias. Second, US examinations were performed by different radiologists and interobserver variability may have affected the results. Third, patients underwent surgery performed by different surgeons. Although patients underwent operation in a single center, the decision to undergo surgery or to observe may have differed according to the surgeon’s discretion. However, a strength of this study was that all cytologic and pathologic slides were reviewed by a single, experienced pathologist, which increased the uniformity of diagnosis.
Conclusions
Although Bethesda category was a statistically significant factor in distinguishing infiltrative FVPTC, NIFTP, and invasive EFVPTC, it was not effective in conclusively distinguishing NIFTP and invasive EFVPTC. The absence of BRAF V600E mutation and lymph node metastasis are important features in distinguishing NIFTP from other subtypes. A notable strength of this study was the uniformity of our pathologic diagnosis. Further studies on preoperative examination such as ultrasound findings of NIFTP and other subtypes are needed.
Footnotes
Authors contribution
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education. (NRF-2015R1D1A1A01058798).