
Abstract
Hyperinsulinaemic hypoglycaemia (HH) is a biochemical finding of low blood glucose levels due to the dysregulation of insulin secretion from pancreatic β-cells. Under normal physiological conditions, glucose metabolism is coupled to β-cell insulin secretion so that blood glucose levels are maintained within the physiological range of 3.5–5.5 mmol/L. However, in HH this coupling of glucose metabolism to insulin secretion is perturbed so that insulin secretion becomes unregulated. HH typically occurs in the neonatal, infancy and childhood periods and can be due to many different causes. Adults can also present with HH but the causes in adults tend to be different. Somatostatin (SST) is a peptide hormone that is released by the delta cells (δ-cells) in the pancreas. It binds to G protein-coupled SST receptors to regulate a variety of location-specific and selective functions such as hormone inhibition, neurotransmission and cell proliferation. SST plays a potent role in the regulation of both insulin and glucagon secretion in response to changes in glucose levels by negative feedback mechanism. The half-life of SST is only 1–3 min due to quick degradation by peptidases in plasma and tissues. Thus, a direct continuous intravenous or subcutaneous infusion is required to achieve the therapeutic effect. These limitations prompted the discovery of SST analogues such as octreotide and lanreotide, which have longer half-lives and therefore can be administered as injections. SST analogues are used to treat different forms of HH in children and adults and therapeutic effect is achieved by suppressing insulin secretion from pancreatic β-cells by complex mechanisms. These treatments are associated with several side effects, especially in the newborn period, with necrotizing enterocolitis being the most serious side effect and hence SS analogues should be used with extreme caution in this age group.
Introduction
Hypoglycaemia is a common biochemical finding in the newborn, infancy, childhood and adulthood periods. In children hypoglycaemia may be due to many different causes. 1 Adults can also present with hypoglycaemia but the underlying causes tend to be different. The most severe form of hypoglycaemia, in children and adults, is hyperinsulinaemic hypoglycaemia (HH). In HH the secretion of insulin from the pancreatic β-cell becomes unregulated and uncoupled from glucose metabolism, so that insulin secretion becomes inappropriate for the blood glucose level, leading to persistent and recurrent hypoglycaemia. In children the congenital forms of HH are more common than in adults and the clinical presentation in newborns and infants is typically with severe and persistent hypoglycaemia. 2 The medical management of newborns and infants with severe forms of HH is complex and some patients are treated with somatostatin analogues, both short and long acting (such as octreotide and lanreotide respectively) to suppress insulin secretion, so that blood glucose levels can be maintained within the normal range. 3 Somatostatin (SST) is a peptide hormone that is released by the delta cells (δ-cells) of the pancreas and has powerful effects on insulin and glucagon secretion from the pancreatic β-cell and α-cell respectively. Although SST analogues are widely used in the treatment of HH both in children and in adults, to our knowledge, no reviews have been published on this subject previously. In this review we will first give the clinical background of the different types of HH; then, we discuss the physiology and pharmacology of SS; outline the use of SS analogues for treating different types of HH; review the literature on the use of SS analogues for treating HH and finally we discuss the side effects related to the use of SS analogues for HH.
Background to hyperinsulinaemic hypoglycaemia
HH is a biochemical finding of low blood glucose levels in the presence of dysregulated insulin secretion. It typically presents with severe and persistent hypoglycaemia. 2 Under normal physiological conditions, glucose metabolism is coupled to β-cell insulin secretion so that blood glucose levels are maintained between 3.5 mmol/L and 5.5 mmol/L. However, in HH this coupling of glucose metabolism to insulin secretion is perturbed so that insulin secretion becomes unregulated. 4
HH is a major cause of severe and persistent hypoglycaemia in children, especially in the newborn period. 5 The congenital forms of HH (shown in Table 1) are more common in children than in adults. In adults an insulinoma is the commonest cause of endogenous HH. HH is also observed in patients who have undergone gastric by-pass surgery for obesity and the secondary cause is due to the side effects of medications such as sulphonylureas. Clinically it is important to make the diagnosis of HH as quickly as possible and stabilize the blood glucose levels as the episodes of hypoglycaemia can lead to brain damage, especially in the newborn. Table 1 lists all the causes of HH.
Causes of hyperinsulinaemic hypoglycaemia.

HH in children
In children, HH can be transient (secondary to maternal diabetes, intrauterine growth retardation or perinatal asphyxia) or permanent. The transient forms of HH usually resolve spontaneously but occasionally may need treatment. 6 The commonest cause of transient HH in the newborn period is secondary to maternal diabetes mellitus (gestational or pre-gestational) and in the vast majority of newborns this will resolve within a few days. Some newborns with intrauterine growth retardation or perinatal asphyxia may have a protracted form of HH which will require treatment. 6
The permanent forms of HH are due to genetic causes that perturb the normal physiological mechanisms of regulated insulin secretion from the pancreatic β-cell. Currently, genetic mutations in 14 different genes lead to different forms of permanent HH, which lead to a spectrum of severity ranging from mild, moderate to severe HH. 7 The most severe forms of HH are due to mutations in ABCC8/KCNJ11, which encode the SUR/KIR6.2 proteins, respectively, of the pancreatic β-cell KATP channels.8,9 These KATP channels play a pivotal role in linking the metabolism of glucose inside the β-cell to changes in the β-cell membrane potential, intracellular calcium homeostasis and insulin secretion. 4 Mutations in the ABCC8/KCNJ11 lead to unregulated insulin secretion and in most cases to severe hypoglycaemia, which is usually medically unresponsive.
In the congenital forms of HH that occur in children, there are two main histological subtypes, namely diffuse and focal HH,10,11 and in a few patients, atypical forms have been described. 11 In diffuse HH the whole of the pancreas is affected whereas in focal only a small region of the pancreas is involved in the abnormality. In terms of clinical management, children with focal lesions can now be identified pre-operatively and the focal lesion can be removed surgically, providing a cure for hypoglycaemia. 12 In contrast, infants with the diffuse type of HH usually do not respond to medical therapy and will require a near-total pancreatectomy, which leads to the development of diabetes mellitus and pancreatic exocrine insufficiency. 13 Therefore, given that infants with diffuse HH develop diabetes following near total pancreatectomy, if it is possible they should be managed aggressively medically. 14 The use of SST analogues (both short-term and long-term) is one form of medical therapy where it might be possible to avoid the need for partial or subtotal pancreatectomy in these patients. Interestingly, in the atypical forms of HH, there is evidence to suggest that the δ-cells that secrete SST might be increased in numbers and may contribute to the pathophysiology. 15
HH in adults
Insulinoma
Insulinomas are the most common functioning endocrine neoplasm of the pancreas, occurring most commonly in the fifth and sixth decades 16 with an incidence of about 1–4 million.17,18 Presentation during childhood is extremely rare but both benign and malignant cases have been reported in children. 19 The majority (90%) of insulinomas are benign, solitary, intrapancreatic and <2 cm in diameter. Classically, symptoms become evident in the fasting state or following exercise; however, it is now known that insulinoma can also present with postprandial symptoms. 20 Somatostatin analogues have been used for the management of adult patients with both benign and malignant insulinomas.
Postprandial hyperinsulinaemic hypoglycaemia after gastric by-pass surgery
Roux-en-Y gastric by-pass is a surgical procedure used in the management of morbid obesity mostly in adults but now also being used in adolescents. Postprandial HH (PPHH) is a well-recognized complication of this procedure. It was first described in 2005 in six patients who had undergone Roux-en-Y gastric by-pass surgery. 21 PPHH is relatively common after gastric by-pass, with approximately 30–40% of patients reporting symptoms of hypoglycaemia in one study. 22 Biochemically, patients show hypoglycaemia with exaggerated insulin and glucagon-like peptide-1 (GLP-1) responses following meal ingestion with early enhancements of hepatic insulin sensitivity and later improvements in peripheral insulin sensitivity. 23 GLP-1 has a stimulatory and trophic effect on pancreatic β-cells, and plasma levels increase after a meal and can lead to hyperinsulinaemia and hypoglycaemia.24,25
Background to SST
Krulich et al. 25 first observed that hypothalamic extracts of rats and sheep contain a growth-inhibiting factor. Further, Brazeau et al. 26 isolated and characterized a peptide that inhibited the release of growth hormone from rat anterior pituitary cells. This peptide was named somatostatin (somatotroph release-inhibiting factor). It was hypothesized to be a neurohumoral substance that regulates growth hormone secretion from the pituitary gland through inhibition. A similar substance was extracted by Hellman and Lernmark from pigeon pancreatic islets that inhibited insulin release. 27 These and subsequent observations identified it as a chemical substance that inhibits hormone secretion in the hypothalamus, pancreas and other secretory cells in the gastrointestinal tract (gut), salivary glands and other excretory systems. It has several important roles and functions as paracrine, autocrine or as true hormones. 28 SST, variously known as SMS, SOM, SST, growth hormone-inhibiting hormone or somatotropin release-inhibiting factor (SRIF), is a cyclic tetradecapeptide. While there are six different SST genes in vertebrates, humans only have a single gene (SST).29,30
Immunoreactive SST is initially synthesized as a preprohormone peptide that consists of 116 amino acids which is cleaved into prosomatostatin, which has 92 amino acids. Prosomatostatin further undergoes C-terminal post-translational processing to generate somatostatin-14 (SST14) and somatostatin-28 (SST28). 30 SST is a peptide hormone that binds with G protein-coupled SST receptors to regulate a variety of functions which include neurotransmission, cell proliferation and inhibition of insulin, glucagon and other hormones. 31 Somatostatinergic neurons are also active inhibitors in the anterior and neural lobe of the pituitary glands, limbic system, brain stem and spinal cord that control the output of excitatory neurons. 32
Role of SST in pancreatic islet cells
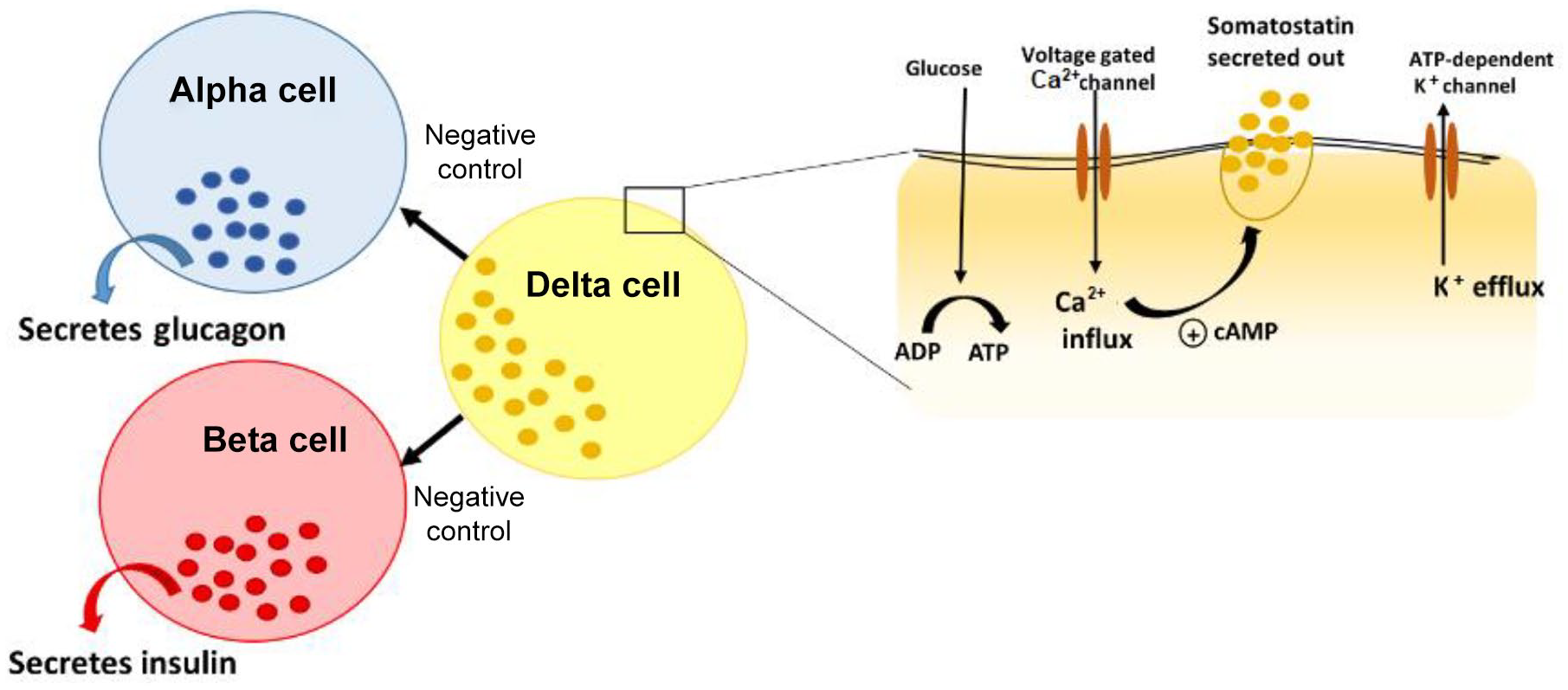
The endocrine pancreas consists of beta (β), alpha (α), delta (δ), pancreatic polypeptide and epsilon (ε) cells (Figure 1) present in the Islet of Langerhans. 33 The predominant type of cell in the islet is the centrally located β-cell (50–60%), which is responsible for secreting insulin in response to rising blood glucose levels, whereas the SST δ-cells comprise about 5%. 34 Glucagon and SST are secreted and released by the α-cells and δ-cells respectively. The close proximity of these cells within the islet facilitates paracrine regulation of hormone production and activity. 35 Metabolites such as glucose, ketone bodies or amino acids act as stimuli to regulate the islet cell hormone production. 36 Although there is no direct evidence that suggests an important role for SST in glucose homeostasis, it has been proposed that disruptions to paracrine interactions (between the β-cells and δ-cells) could lead to alterations in glucose metabolism.34,37
Role of SST in regulation of insulin secretion and β-cell physiology
SST is involved in the regulation of both insulin and glucagon secretion in response to changes in glucose levels by negative feedback mechanism. 34 In response to high blood glucose levels, insulin is secreted and, once normoglycaemia is attained, the loss of physiological stimulus inhibits insulin secretion from β-cells. Also, there is inhibition from within the islet which is proposed to be mediated by SST. 38 The exact molecular mechanism behind this regulation is unknown, but several mediators have been proposed. 39 SST14 and SST28 are the biologically active forms of SST. 40 SST14 is the more predominant inhibitor of α-cell-mediated glucagon secretion, while SST28 inhibits insulin secretion from β-cells. 41 However, SST treatment at very low glucose levels does not attenuate insulin secretion. This suggests that the mechanism of action could be glucose metabolism dependent. 42
SST acts primarily via five transmembrane G-protein coupled SST receptor (SSTR) types (SSTR1–SSTR5) with SSTR1, SSTR2 and SSTR5 being highly expressed in β-cells. 43 The five receptors share common signalling pathways such as the inhibition of adenylyl cyclase, activation of phosphotyrosine phosphatase and modulation of mitogen-activated protein kinase through G-protein-dependent mechanisms. Also, each receptor may have specific signalling mechanisms such as SSTR2–5 being coupled to inward rectifying K+ channels, SST binds to the SST receptor on the β-cell and inhibits the activation of voltage gated calcium channels and ATP sensitive K+ channels. This reduces cyclic adenosine monophosphate (cAMP) levels thereby inhibiting the release of insulin.44,45 Activation of SSTR by G-protein coupling inhibits adenylyl cyclase activity that leads to reduced cyclic AMP and diminished insulin secretion, 46 as seen in Figure 2.

Mechanism of action of somatostatin (SST) on insulin secretion by negative feedback. SST binds to the SST receptor on the β-cell and inhibits the activation of voltage gated calcium channels and ATP sensitive K+ channels. This reduces cyclic adenosine monophosphate (cAMP) levels thereby inhibiting the release of insulin.44–46
It has been postulated that the inhibitory effect of SST on insulin secretion may be through alterations in voltage-gated calcium channels, particularly inhibition of L type channel. 47 β-cells at stimulatory glucose concentrations, exposed to SST, show a significant reduction in intracellular calcium levels that results in diminished insulin secretion, suggesting a Gβγ complex-mediated signalling. 39 In MIN6 cell lines, SST can inhibit glucose-induced electrical activity by the combined activation of ATP sensitive potassium (KATP) channel and G-protein coupled inward rectifying potassium channel, suggesting that there may be some involvement of the KATP channels in response to SST. 48 Further, gamma-aminobutyric acid (GABA), which is an inhibitory neurotransmitter, is released by the β-cells, which mediates negative feedback for the δ-cells. 49 GABA is involved in both activities: in autocrine positive feedback, which helps to produce a quick response to hypoglycaemia, as well as in paracrine negative feedback control of the β-cells, thus maintaining an optimal islet cell output after attaining normoglycaemia. 49 Another peptide hormone, Urocortin3 (Ucn3) is expressed by β-cells and α-cells in humans, which stimulates secretion of both insulin and glucagon. 50 Ucn3 is stored in insulin granules and in the event of hyperglycaemia is released along with insulin. This provides a negative feedback loop via corticotropin-releasing hormone receptor 2a receptors to SST, which in turn inhibits the release of insulin. 51 More recent data in mice and in human islets show that insulin-stimulated SST secretion plays a key role in regulating serum glucagon secretion. 52
Interaction of SST with other pancreatic hormones
Endogenous SST secreted from δ-cells has paracrine effects on the regulation of insulin and glucagon secretion but the physiological significance of this regulation is still unclear. While SSTR5 seems to be a negative regulator of insulin secretion, SSTR2 inhibits glucagon secretion. 53 SST receptor knockout mice have been generated in order to understand the physiological roles of SSTR receptors. Global SSTR knockout mice were generated in order to investigate the role of δ-cell-secreted SST in the regulation of insulin and glucagon secretion in vitro and in vivo. 38 This study showed that δ-cell SST exerts a tonic inhibitory influence on insulin and glucagon secretion. Viable, fertile SSTR5 knockout mice that are otherwise healthy, exhibit no apparent phenotypic abnormalities. 54 Pancreatic islets from these mice show increased insulin content as compared with wild-type islets. These mice exhibited decreased blood glucose and plasma insulin levels and increased leptin and glucagon concentrations compared with wild-type mice. SST analogue 28 was not able to inhibit insulin secretion in knockout islets as effectively as from wild-type islets. In contrast, islets from SSTR2 knockout mice show no difference in basal glucagon and insulin secretion while potassium/arginine-stimulated glucagon secretion was approximately 2-fold higher when compared with wild-type islets. 42 Neither SST nor any SSTR-selective agonist inhibited basal glucagon or insulin release. SST14 potently inhibited stimulated glucagon secretion in islets from wild mice and much less effectively in islets from SSTR2 knockout mice. Both of these studies in mice suggest that SSTR5 is important for regulating insulin secretion and SSTR2 for glucagon secretion.
Ghrelin positive ε-cells are located in the periphery of the pancreatic islet. Although ghrelin mainly controls appetite, it can also regulate the secretion of insulin and SST. The effects of ghrelin on insulin secretion and glucose physiology are complex and not completely understood. Broglio et al. 55 first showed that an intravenous injection of ghrelin leads to a decrease in insulin secretion and an increase in the blood glucose level. In another study an infusion of ghrelin led to an increase in the serum level of SST. This increase in the SST level could explain the reduction in the insulin level. 56 Thus, ghrelin has complex effects on insulin and SST secretion and blood glucose levels.
Background to SST analogues
SST has anti-proliferative, anti-secretory and anti-angiogenic properties, which makes it useful in the treatment of certain diseases of the gastrointestinal system, pancreas, peripheral neurons and the retina, among others. 57 However, the half-life of SST is only 1–3 min due to quick degradation by peptidases in plasma and tissues. This requires a direct continuous intravenous injection to produce the therapeutic effect. These limitations prompted the discovery of octapeptide analogues octreotide and lanreotide. 58 Their mode of delivery is either subcutaneous injections or infusions or by intravenous route.
Octreotide was the first US Food and Drug Administration (FDA) approved synthetic SST analogue (SMS 201-995), marketed as Sandostatin® and available in a conventional and a long acting formulation (Sandostatin LAR®). The Sandostatin LAR® formulation contains octreotide distributed within polymer microspheres and it is available for intramuscular injection.
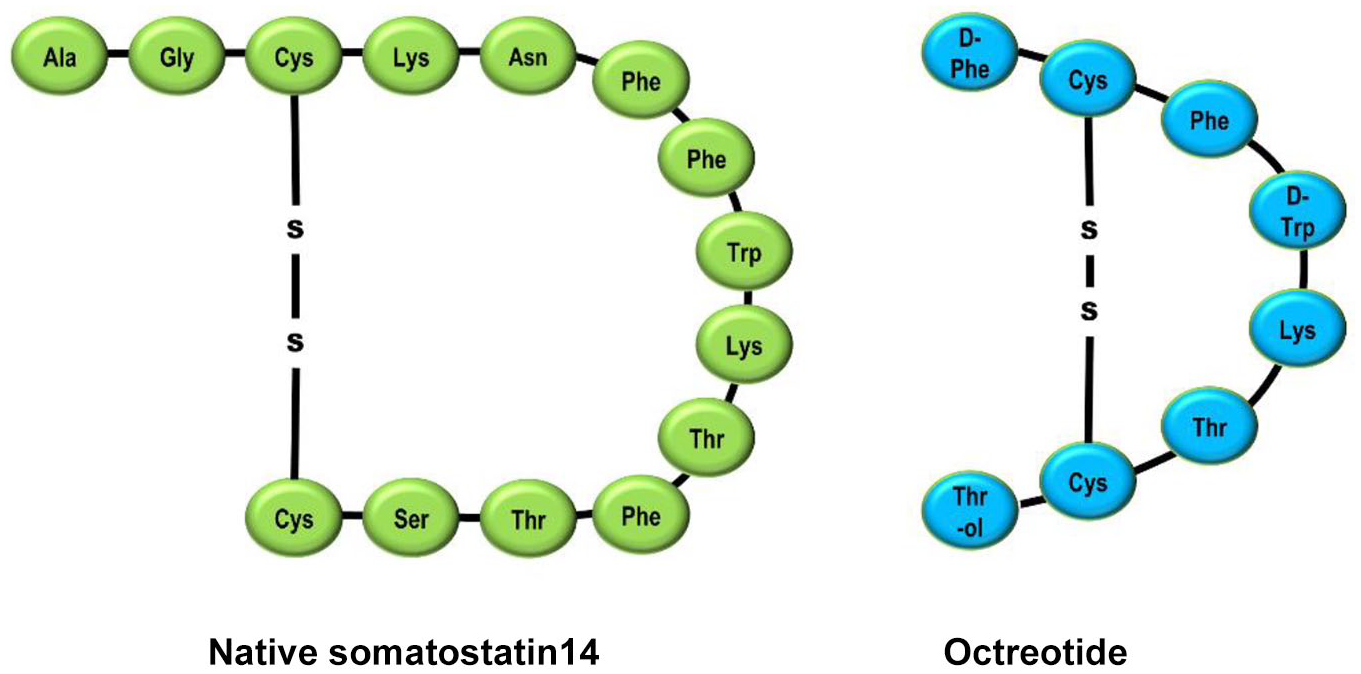
Octreotide is an octapeptide in which the four amino acid sequence essential for the biological activity of the native hormone is retained. However, incorporation of N-phenylalanine, L-terminal amino alcohol, D-tryptophan and a cysteine bridge makes the molecule very resistant to metabolic degradation. 59 The half-life of octreotide is 90–120 min via subcutaneous administration and has a pharmacodynamic action lasting 8–12 h. Octreotide binds primarily to SSTR2 and SSTR5 with a low affinity to SSTR3. The selective binding to SSTR2 results in increased therapeutic benefits and fewer adverse effects. Octreotide has 40 times greater potency than SST in inhibiting growth hormone (GH) secretion. It has also demonstrated the ability to inhibit insulin and glucagon secretion in the pancreas. 60 Figure 3 shows the structure of SST and SST analogue octreotide.
The development of long-acting formulations of SST analogues which require only weekly or monthly injections can improve patient compliance. In particular, lanreotide (LAN) Autogel®, which is a viscous aqueous formulation supplied in ready-to-use prefilled syringes, can be administered every 28–56 days. Lanreotide is a cyclic octapeptide that is widely used for adults with neuroendocrine tumours. Pasireotide is a novel short synthetic SST analogue which exhibits high affinity binding to four of the five human SRIF receptor subtypes and has potent, long lasting inhibitory effects on GH and Insulin like Growth Factor (IGF-I) release. 61
The oldest and most common use of these SST analogues is in the treatment of acromegaly and hormone dependent pituitary tumours 17 where they control the hormonal imbalance as well as produce a tumour stabilizing effect. 62 These are drugs of choice in gastrointestinal tumours such as VIP-oma, gastrinoma, glucagonoma, insulinoma and both typical and atypical carcinoid syndrome for symptomatic relief. Other, newer, uses for these drugs include endocrine tumours such as well differentiated thyroid tumours, pheochromocytoma and adrenocortical tumours as well as non-endocrine tumours such as small cell lung cancer and melanoma. They are very effective in conditions such as portal hypertension and oesophageal variceal bleeding, peptic ulcer and short bowel syndrome. Ophthalmologic indications include Graves’ ophthalmopathy and diabetic retinopathy among others. 63
Octreotide has been shown to be beneficial in insulin dependent diabetes mellitus by increasing insulin sensitivity and in non-insulin dependent diabetes mellitus it reduces insulin resistance. 64 It is also proposed to be useful in the prevention of diabetic complications such as diabetic retinopathy. 65 However, the use of octreotide in diabetes mellitus and diabetic retinopathy is not registered and is experimental. Another potential use of octreotide is in imaging, namely somatostatin receptor scintigraphy (octreoscan), which helps to visualize autoimmunological processes in conditions such as lymphoma, medullary thyroid cancer and breast cancer. 66
The role of SST analogues in treatment of HH
Use of SST analogues in children with HH
The congenital forms of HH typically present with severe and persistent hypoglycaemia. The management of HH typically involves having a stepwise approach to assessing the response to different forms of medical therapy. 2 In the acute situation blood glucose levels are stabilized with concentrated intravenous glucose infusions and/or feeds. A bolus or a subcutaneous infusion of glucagon may also be used in the acute scenario. Once the biochemical diagnosis of HH is established the first line therapy is with diazoxide. Genetic testing for the important causes of HH is now a key component in the management of patients with HH. Currently, diazoxide is the only drug approved by the FDA for the treatment of children with HH. Patients with mutations in ABCC8/KCNJ11 encoding the SUR1/KIR6.2 components of the pancreatic β-cell typically do not respond to treatment with diazoxide (most of the other genetic forms of HH will respond to therapy with diazoxide). In these cases, when diazoxide fails, second-line treatment options for children are limited. In 1977 Hirsch et al. 67 first described the infusion of synthetic cyclic SST in an infant with severe HH. This improved the blood glucose levels and reduced circulating serum insulin levels. The authors then treated the patient with single subcutaneous injections of 50 µg of protamine zinc SST, which also improved pre-prandial blood glucose levels. In another early study, in 1981, Roti et al. 68 demonstrated an improvement in the blood glucose level in a patient with HH in response to an intravenous infusion of SST but no improvement in the blood glucose level in response to protamine zinc-SST, a long acting SRIF preparation. In the same year Aynsley-Green et al. 69 reported the effect of SST infusion in two infants presenting at 9 weeks and 5 days of age with severe HH. In both infants normoglycaemia was restored with suppression of insulin secretion. The plasma concentrations of glucagon, cortisol, growth hormone, motilin, pancreatic polypeptide, gastric inhibitory of polypeptide, neurotensin, gastrin and vasoactive intestinal peptide decreased markedly during the SST infusion. In 1985 Bougnères et al. 70 used native cyclic SST in an infusion pump to treat a child with HH and achieved normal blood glucose levels. Also, in 1985 Wendal et al. 71 treated 11 infants with SST and showed that it was very reliable in the treatment of neonatal hypoglycaemia due to hyperinsulinism for a limited period of time until subtotal pancreatectomy was performed. These initial studies established the physiological basis for using SST in infants with HH. Then in 1986 Bruining et al. 72 reported the use of long-acting SST analogue SMS 201-995 (octreotide) in a newborn with severe HH. The patient presented with severe hypoglycaemia and seizures. The intravenous infusion of this analogue (gradually increasing the dose from 2 to 50 µg/24 h) dramatically reduced circulating insulin levels and stabilized blood glucose levels.
SST analogues (such as octreotide) are now frequently used as second line therapy for children who are not responsive to diazoxide and there are now a large number of studies supporting the use of SST analogues for childhood HH. 73 Many studies document the use of SST analogues for treating childhood HH, dating back to 1977.14,27,67–175 However some patients with HH do not respond to SST analogue treatment.
Interestingly, in some parts of the world where diazoxide is not available then octreotide has been used even as a first line therapy. 176 SST analogues have also been used in the long term where in some patients with severe HH the need for pancreatectomy can be avoided. 14 The dose range is typically between 5 and 25 µg/kg per day (maximum dose can go to 40 µg/kg per day) administered either intravenously, subcutaneously by continuous infusion, or as 6–8 hourly subcutaneous injections for short- and long-term treatment of hyperinsulinaemia. 2
The development of long-acting formulations of SST analogues which require only weekly or monthly injections can improve patient compliance. In particular, lanreotide (LAN) Autogel®, which is a viscous aqueous formulation supplied in ready-to-use prefilled syringes, can be administered every 28–56 days. 177 Since its introduction into clinical practice, several studies have evaluated the clinical utility of LAN Autogel® in the medical treatment of children with HH. The first study described two patients with HH who were initially managed with diazoxide and octreotide but then at the ages of 4 and 4.5 years were started on lanreotide acetate (Somatuline Autogel), administered by deep subcutaneous injection of 30 mg once a month. 98 This allowed the patients to come off the diazoxide and the daily octreotide injections and normoglycaemia was maintained. In the study by Le Quan Sang et al. 102 10 patients underwent replacement of their three daily subcutaneous octreotide (Sandostatin, Novartis) injections by a single and monthly intramuscular injection of long-acting release (LAR) octreotide (Sandostatin LP, Novartis). The study concluded that LAR octreotide was efficient, well tolerated and contributed to a clear simplification of the medical care. In another multicentre study, 106 involving six different centres in Europe, data were obtained retrospectively from 27 patients with HH who received long-acting SST analogues. These included information on glycaemic stability, auxology and adverse effect profile in clinical follow-up assessments. The study concluded that long-acting SST analogues are effective in glycaemic control of patients with HH. Several other studies have also now documented the beneficial effects of long-acting octreotide formulations in children with different forms (focal and diffuse) of HH. 110
The pharmacodynamics and pharmacokinetics of octreotide have largely been studied in adults with no studies in children. In blood, octreotide is mainly distributed in the plasma with about 65% bound to lipoproteins. Octreotide administered by subcutaneous injection is rapidly absorbed, with peak concentrations of 5.2 ng/mL occurring around 25 min after a 100-µg dose in adults. The apparent half-life of octreotide is approximately 1.7 h, which is significantly greater than the 1–3-min half-life of SST (in adults). 178 The effects of octreotide are variable, but can last for up to 12 h, and approximately 32% of a dose is excreted in the urine as unchanged drug. 179 Dosage adjustments may be required in infants with impaired renal function which leads to decreased clearance and increased half-life. 178 Table 2 compares the pharmacology of short and long acting octreotide formulations.
Comparison of octreotide, lanreotide and Sandostatin LAR.

LAR, long-acting release.
Use of SST analogues in the management of PPHH after Roux-en-Y gastric by-pass
A number of different treatment options have been proposed for the management of PPHH after Roux-en-Y gastric by-pass. 180 These include having frequent high-fibre meals and reduction or elimination of simple carbohydrates in the diet, and using medications such as acarbose, diazoxide, calcium channel blockers and octreotide. 181 Long-acting octreotide formulations (such as Sandostatin-LAR) have been used in the management of PPHH due to Roux-en-Y-gastric-bypass with equal efficacy as octreotide in suppressing hypoglycaemic symptoms. 182 In one large study comparing the efficacy of subcutaneous octreotide with that of the long-acting LAR formulation on 30 patients, it was found that the administration of LAR octreotide improved the oral glucose tolerance results, symptoms and quality of life in patients with postoperative dumping. 183 Several other studies have described the use of short- and long-acting SST formulations for the management of PPHH due to Roux-en-Y-gastric-bypass.24,184,185
Use of octreotide in HH due to sulphonylureas
HH due to sulphonylureas (either due to treatment or to intentional overdose) can also be managed with octreotide. Sulphonylurea poisoning can lead to severe hypoglycaemia especially in children and in the elderly, which may be refractory to intravenous glucose infusion. In these cases, octreotide can be used to treat hypoglycaemia. 186 Even in children with accidental poisoning due to sulphonylureas, octreotide has been safely used to restore normoglycaemia. 187 In 1993 Boyle et al. 188 tested the hypothesis that octreotide could reverse sulphonylurea induced HH in eight normal subjects administered glipizide on three occasions. They found that octreotide reduced and in four of eight subjects entirely eliminated the need for exogenous glucose after a large overdose of glipizide and concluded that octreotide was safe and effective and should be considered as a logical therapeutic alternative for this metabolic emergency. Patients have also been described with sulphonylurea induced HH who are refractory to treatment with boluses of dextrose but respond to octreotide. 189 Since the first reports, there have been numerous studies190–217 describing treatment of sulphonylurea overdoses with octreotide. In virtually all the studies that reported the use of octreotide, there were no serious adverse effects.
Use of SST analogues in patients with insulinoma
In 1975 Curnow et al. and Christensen et al.218,219 both reported the use of SST in patients with insulinoma. In both cases the infusion of SST improved the blood glucose profile of the patients. Following these two studies, several other studies were then also published which documented the efficacy of SST as well as a potential aid in diagnosis in patients with both benign and malignant insulinoma.220–225
For adults with insulinoma, the first report on the use of a SST analogue was in 1979, when a new long-acting octapeptide analogue of SST, Des AA1, 2, 4, 5, 12, 13 D Try8 SST, was tested in eight patients with different pancreatic endocrine tumours. 226 The analogue was given subcutaneously and suppressed the tumour-derived hormones in patients with insulinomas, glucagonomas and gastrinomas for up to 24 h. The prolonged action appeared to be the result of slow release from the injection site and there were no side effects reported. Long-acting SST analogue (SMS 201-995) was used in the early 1980s in patients with, again, both benign and malignant insulinomas.227,228 Since these early studies numerous studies have documented the beneficial effects of SST analogues in insulinoma.
The use of SST analogues in the scintigraphic imaging of insulinomas and in the medical management of these tumours seems to be restricted to a subgroup of patients. SSTR2 and 5 are the predominant subtype receptors expressed in about 70% of malignant insulinomas whereas SSTR1 is present in about 50% and SSTR3 and 4 in approximately 15–20%. 229 Interestingly some insulinomas do not express any SSTR. In insulinomas where there are no SST receptors, octreotide will aggravate hypoglycaemia due to suppression of glucagon and growth hormone. 230 So, a test dose of octreotide is suggested before commencing treatment. Pasireotide, another SST analogue which can target multiple receptors, was reported to achieve better glycaemic control than octreotide and lanreotide in a patient with malignant insulinoma. 231
Octreotide during pregnancy
The use of octreotide during pregnancy seems to be associated with poor outcome, as reported in two studies,232,233 but in another study 114 octreotide treatment was found to be effective in controlling endogenous hyperinsulinism during pregnancy and did not affect physiological changes during pregnancy such as insulin-resistance or placental GH level with no abnormalities in the foetus.
In the report by Skajaa et al., 232 a woman with a genetic form of HH was given octreotide during the first four pregnancies, resulting in two cases of early termination of pregnancy on parental request and two cases of inappropriate foetal growth and unviable outcome. The following two pregnancies, treated with diet only, had a successful outcome. In the second report, by Geilswijk et al., 233 treatment of the mother with octreotide (who was also affected by a genetic form of HH) led to foetal growth restriction. These two observations suggest that octreotide should be used with caution during pregnancy in mothers who have genetic forms of HH.
Octreotide use in small for gestational age infants with HH
A case series of neonates born small for gestational age with HH were successfully treated with octreotide infusion and the blood glucose was corrected with no complications. 176
Octreotide use in Beckwith–Wiedemann syndrome and HH
There have been two cases of newborns with Beckwith–Wiedemann syndrome and HH who were managed with SST analogues, again with no complications.118,122
Side effects of SST analogues in patients with HH
The local subcutaneous injection of octreotide can cause pain, a sensation of stinging and burning as well as redness and swelling. Common gastrointestinal adverse effects of octreotide include delayed gastric emptying, reducing gallbladder contraction, nausea, abdominal cramps, diarrhoea, malabsorption of fat, and flatulence. 234 STT analogues inhibit the secretion of GH, prolactin, thyrotropin, cholecystokinin, gastric inhibitory peptide, gastrin, motilin, neurotensin, secretin, glucagon, insulin and pancreatic polypeptide. They also inhibit the exocrine secretion of amylase of salivary glands; hydrochloric acid, pepsinogen, and intrinsic factor of gastrointestinal mucosa; and enzymes and bicarbonate of pancreas and bile in the liver. 235 The suppression of GH (and IGF-I) and thyroid hormones, in theory, can lead to stunting of growth; however, in clinical practice, the suppressive effects of octreotide seem to be overridden with no major long-term problems. 3 In one study assessing the long-term impact of octreotide in children with HH, where the mean ± standard deviation duration of follow-up on octreotide therapy was 52.4 (±33.8) months (range 6 months to 9.5 years), it was found that transient elevation of liver enzymes and asymptomatic gallbladder pathology were the most prevalent long-term side effects of octreotide therapy. 126 There was no correlation between the dose or the duration of octreotide therapy and the development of liver dysfunction and gallbladder pathology and no long-term effects on growth. Octreotide can decrease gallbladder contractility and bile secretion, leading to steatorrhoea, cholestasis, hepatic dysfunction and cholelithiasis.236,237 Blood flow to the splanchnic circulation is decreased by octreotide; hence, it must be used cautiously in babies at risk of necrotizing enterocolitis (see below). Table 3 lists all the side effects reported due to the use of SST analogues in children with HH.
Reported side effects of somatostatin analogues.

Necrotizing enterocolitis
Necrotizing enterocolitis (NEC) is a disease mainly of premature infants and associated with a high mortality rate. It typically presents with abdominal distension, bilious vomiting and bloody stools, which can lead to sepsis and shock in severe cases. NEC is characterized by coagulation necrosis of the intestine, bacterial overgrowth and inflammation. 240 The first report in the literature of octreotide-related NEC was in 2010 by Laje et al. 238 In this study, out of 197 neonates who developed NEC, four had no risk factor for NEC, except that they were being treated with octreotide. The authors reported that NEC occurred in 2% of neonates who were treated with octreotide for HH. See Table 3, which lists the studies reporting NEC in patients with HH due to SST analogue therapy. All reported cases of NEC associated with octreotide use in infants with HH occurred in neonates younger than 1 month of age and within 15 days of commencing octreotide therapy, at doses of 15–27 µg/kg per day. 241 However, a case of late-onset NEC in a patient with Beckwith–Wiedemann syndrome and HH, who was treated with a relatively low dose of octreotide, has also been reported. 134
The mechanism of octreotide induced NEC in patients with HH is not completely clear. But it is known that octreotide reduces superior mesenteric artery blood flow as well as portal venous blood flow and blunts the normal postprandial rise. The reduction in blood flow seems to be dose dependent. 242
Tachyphylaxis
The major limiting factor for the use of octreotide in children with HH is the associated tachyphylaxis. Nearly all patients show resistance to the continued use of octreotide, even to increasing doses.3,130 Some patients develop tachyphylaxis soon after treatment whereas in others it may take weeks or months to develop. The underlying mechanisms leading to tachyphylaxis are not known but might involve SSTR down-regulation, or G protein uncoupling and/or receptor internalization. 243
Future directions
Although most children with HH show a good initial response to treatment with octreotide the response becomes less effective over time due to the tolerance effect. Therefore, more potent SST analogues are required with less tolerance. Pasireotide is a relatively new SST analogue with increased affinity for SSTR5 and with a longer half-life. 244 Its affinity for SSTR5 is thought to be 40 times that of the other analogues. It has been used primarily for the treatment of Cushing’s disease due to increased adrenocorticotrophic hormone secretion. However, in adults with PPHH due to gastric by-pass, it has been shown to be effective in comparison with octreotide. 184 Pasireotide has not been trialled in children with congenital forms of HH but it might offer potential treatment options for some forms of HH in the childhood period. Thus, one of the future directions could be to undertake a clinical trial of pasireotide use in children with HH and assess its effectiveness.
Peptide receptor radionuclide therapy (PRRT) is a relatively new mode of treatment for patients (mostly adults) with inoperable, usually metastasized, neuroendocrine tumours. SST analogues are radiolabelled and can bind with high affinity to the cancer cell expressing the SST receptor. PRRT has been reported to be effective in adults with malignant insulinomas, with one study reporting successful control of blood glucose in five patients with malignant insulinomas. 245 PRRT treatment has not been reported in children with HH, thus this could be another potential treatment modality which needs further exploration.
Conclusion
SST has a key physiological role in the inhibition of insulin and glucagon secretion from the pancreatic β-cells and δ-cells respectively, hence the use of its analogues in the treatment of different forms of HH. The precise molecular mechanisms involved in the inhibition of insulin and glucagon secretion are not known. Due to SST’s short half-life SST analogues have been developed which are used to treat various conditions, including different forms of HH in children and adults. Both octreotide and the long-acting formulations are effective in the management of patients with HH. In the neonatal period, octreotide must be used with caution as there is a risk of developing NEC.
Footnotes
Author contribution(s)
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.