
Abstract
Objective:
Some studies have shown that metformin can reduce body weight. However, metformin has not been officially approved as a medicine for weight loss because its effect on different populations remains inconsistent. This meta-analysis aimed to summarize the weight loss effect of metformin quantitatively.
Method:
The randomized controlled and high-quality case-control trials of metformin monotherapy in obesity treatment were eligible. Baseline body mass index (BMI) was chosen as a self-control to compare the changes in BMI of different populations before and after treatment. All changes were calculated as differences between the final and initial BMI values (with negative values indicating a decrease). Results were presented as weighted mean difference (WMD) with a 95% confidence interval (CI 95%). Subgroup analysis was performed based on baseline BMI, age, daily dose, and duration of medication.
Results:
A total of 21 trials (n = 1004) were included, and the meta-analysis of metformin treatment in different populations showed that metformin has a modest reduction in the BMI of included participants (WMD −0.98; 95% CI, −1.25 to −0.72), and the reduction of BMI was most significant in the simple obesity population (WMD −1.31; 95% CI, −2.07 to −0.54). The subgroup analysis showed that metformin treatment significantly reduced BMI in obesity patients with a BMI >35kg/m2 (WMD −1.12; 95% CI, −1.84 to −0.39) compared with before treatment. BMI in the high dose group decreased by 1.01 units (WMD−1.01; 95% CI, −1.29 to −0.73) and BMI did not continue to decrease significantly after treatment of more than 6 months.
Conclusion:
Patients treated with metformin experienced about a one-unit reduction in BMI at the end of treatment. But whether this decreased value produced enough weight loss (5% of baseline body weight) to qualify as a “weight loss drug” as current guidelines require, requires larger specific randomized control trials.
Introduction
Obesity, which is defined as a body mass index (BMI) ⩾30 kg/m2, has been a challenging health problem worldwide. It has become a major contributor to the global disease burden.1–4 Obesity is a chronic disease and a risk factor for other comorbidities. The recent study of adult BMI trends in 200 countries 5 shows that the prevalence of obesity increased from 3.2% to 10.8% in men and 6.4% to 14.9% in women from 1957 to 2014. The global prevalence of morbid obesity is 0.64% and 1.6% in men and women, respectively. Obesity is also associated with nearly 200 complications, including diabetes, cardiovascular disease, high blood pressure, and stroke, which severely threaten human health. 2
In May 2016, the American Association of Clinical Endocrinologists (AACE) and American College of Endocrinology (ACE) announced the clinical practice guidelines for comprehensive medical care of patients with obesity. According to the guidelines for the management of overweight and obese adults, most individuals need to measure body weight frequently and avoid weight gain by adjusting their diet and physical activities. 6 However, long-term cohort studies show that people with obesity, but without any metabolic disorder, remain at risk for various obesity-related complications. 7 Obesity treatment with lifestyle modifications often fails. 8 Therefore, medications also play an important role in obesity management and can help improve health for people who have failed to lose weight by diet and exercise. 9
Five treatment methods have been approved by the US Food and Drug Administration (FDA) for the long-term treatment of obesity. These drugs include orlistat, phentermine + topiramate, lorcaserin, naltrexone + bupropion, and liraglutide. In addition to weight reduction via orlistat by inhibiting fat absorption, the other drugs all act on the central nervous system pathways, reducing appetite or increasing satisfaction to reduce weight. The side effects of weight loss drug mainly include dizziness, nausea, constipation, insomnia, and other symptoms.1,9 Phentermine can be used as monotherapy in short term or as fixed-dose combinations with topiramate in long treatment. Naltrexone for weight loss is only used in fixed-dose combinations with bupropion. Orlistat is a long-acting and powerful specific gastrointestinal lipase inhibitor. This drug inhibits the enzymes responsible for the digestion of fat in the human gastrointestinal tract and prevents the absorption of fat in the digestive tract, thereby reducing calorie intake and weight control.9,10
Many studies support that metformin can promote weight loss in overweight or obesity patients.11–13 A systematic review that included 946 10–16-year-old obese adolescents demonstrated a significant reduction in BMI [−1.38; 95% confidence interval (CI), −1.93 to −0.82] after metformin treatment. 11 Broad evidence based on clinical trials supports the efficacy and safety profiles of metformin in diabetes and weight gain prevention. 14 In addition, the side effects of metformin are relatively mild. The most common side effect of metformin is gastrointestinal reaction, which decreases with increasing medication period and careful dose escalation. 15 Furthermore, metformin has many advantages, such as improvement of insulin resistance (IR) in people with obesity and alleviation of hyperandrogenism in women with polycystic ovary syndrome (PCOS).16,17 Therefore, as a possible weight loss-promoting drug, conducting an in-depth study on the potential weight loss benefits of metformin is reasonable.
However, metformin has not been officially approved as a weight-reduction medicine. 4 Different reports indicate inconsistencies in the weight loss effects of metformin. Moreover, no systematic review has been conducted regarding the weight reduction effect of metformin in different populations. The present meta-analysis aimed to further investigate the effectiveness of metformin on weight loss, explore the feasibility and effectiveness of metformin as a potential weight loss medicine, and possibly provide a basis for the establishment of clinical obesity management and obesity management guidelines.
Methods
Search strategy
Studies were identified by searching PUBMED, the Cochrane library, and the Chinese National Knowledge Infrastructure for eligible studies published between January 1, 1998 and March 31, 2019. References cited in the primary articles were also manually searched. Meta-analysis was performed following the PICO format: treatment of obese patients (P) with metformin (I) compared with the placebo/lifestyle/monotherapy (C) outcomes related to weight loss or changes in BMI (O). The basic terms for literature search were as follows: “metformin” and “weight loss” or “weight reduction” and “obesity” and “body mass index” or “BMI”.
Study selection
Randomized controlled trial (RCT) or high-quality case-control, which evaluated the efficacy and safety of metformin was eligible. All titles and abstracts were filtered to exclude unqualified research. The full text of the remaining studies was read for further identification. Metformin monotherapy was selected to eliminate the result interference of combined medication. The selection criteria for the meta-analysis were as follows: (i) intervention with metformin or comparison of metformin with a control, (ii) published RCT, cohort study, and case-control study, (iii) reported changes in BMI before and after treatments, and (iv) metformin treatment at least 1 month and mean dosage report. The exclusion criteria for the meta-analysis were as follows: (a) incomplete research design and extraction failure of effective data, (b) other diseases of patients that affect body weight, and (c) the use of medicine reducing body weight before or during metformin intervention.
Data extraction
The extraction and collation of the data were independently conducted by XR and RP for quality. The risk of bias in these studies was assessed by TG and DS. Data were extracted as follows: source of study (first author and publication year), population characteristics (mean age, baseline BMI), methodology design (study design and blind method), and metformin intervention (dose, intervention length); changes of BMI were calculated as differences between the final and initial BMI values (with negative values indicating a decrease).
Statistical analysis
The BMI data were presented in the form of mean ± standard deviation (SD) for statistical analysis. The BMI data were presented in the form of standard error (SE) in the four studies.18–21 The values were converted into SD based on the following formula: SE = SD/√N. The baseline BMI was chosen as self-control to compare the changes in BMI before and after treatment. Data from the 21 studies were combined using the random-effects model of STATA 12.0. The results were presented by the weighted mean difference (WMD) for continuous variables with a CI 95%. I square (I2) was used to assess heterogeneity across studies, with I2 values > 50% representing high heterogeneity. Influence analysis was conducted to determine the effect of individual study on the aggregate result. A funnel plot was employed to assess publication bias.
According to guideline for the management of overweight and obesity in adults, obesity is divided into grades I, II, and III with BMI of 30–34.9, 35–39.9, and >40 kg/m2, respectively. Overweight is defined as 25–29.9 kg/m2. Moreover, the dose of metformin was stratified by extracting the data contained in all studies. Low and high doses were defined as <1500 and >1500 mg/d, respectively.
Quality assessment
The quality of each study was assessed using the Cochrane “Risk of bias” tool. The considered factors included seven parts: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcomes, selective reporting, and other biases. DS and TG independently assessed the quality of the included studies.
Results
Search result
A total of 546 non-duplicated records were identified in this meta-analysis, 485 of which were excluded at the level of title or abstract, and 61 full-text articles were evaluated. The literature was further screened in accordance with the correlation, study design, results, dose, and intervention length of metformin. Finally, a total of 21 eligible studies (with 1004 participants) were included in the meta-analysis (Figure 1).

PRISMA flow diagram detailing process of study selection for the meta-analysis.
Characteristics of included studies
The 21 articles, which focused on the effects of metformin in overweight and obese patients, were published from 2000 to 2018. The characteristics of the included studies are shown in detail in Table 1. A total of 1004 participants with age (mean) ranging from 7 to 56 years old and baseline BMI (mean) ranging from 26 kg/m2 to 41 kg/m2 were included. The length of metformin intervention ranged from 3 months to 32 months (Table 1).
Baseline characteristics of the included articles.

BMI, body mass index; IFG, impaired fasting glucose; IR, Insulin resistance; MET, metformin; PCOS, polycystic ovary syndrome; RCT, randomized controlled trial; T2DM, type 2 diabetes mellitus.
Number of Participants is the number of metformin treatment group.
In the 21 studies, 11 RCTs and 1 case control were found relevant to the treatment of simple obesity.18–20,22–30 Meanwhile, six studies were related to PCOS obesity treatment.21,31–35 Furthermore, two trials were associated with type 2 diabetes mellitus (T2DM) obesity treatment.36,37 These studies were combined in one group because impaired fasting blood glucose and IR are the early symptoms of T2DM. A manual search was performed to supplement the literature on women with IR. 38 In nine studies,18–22,29–31,33,37,38 lifestyle intervention was used as the control group. In 11 studies,18–22,29–31,33,37,38 participants in the metformin and control group also received lifestyle intervention. The performance of lifestyle interventions during metformin treatment was not mentioned in eight studies23–28,32,36 (Table 1).
Risk of bias assessment
The details of the risk of bias assessment are summarized in Figure 2. No study was considered low quality. Bulatova 37 found more than one generic metformin prescription to patients and possible variations in efficacy between generics. Cheang showed that no randomized control group has been designed in a long-term retrospective study. 34 However, having a control group of women treated with a placebo for three years is infeasible. The present study was included considering the importance of data from long-term observational studies. Clarson et al. 23 found that some participants exited the study because they had reached a target BMI or had undertaken independent physical activities. Some patients have been busy to attend weekly exercise sessions. These factors may interfere with the results. Blinding of participants and personnel was not mentioned in the six studies18,21,25,35,37,38 (Figure 2).

Summary assessment of risk of bias of the included studies.
Meta-analysis of metformin treatment on BMI in different populations
Modest reduction in BMI (WMD −0.98; 95% CI, −1.25 to −0.72) was observed in the total population, demonstrating a small statistical heterogeneity (p = 0.999, I2 = 0.0%). The BMI of simple obesity was reduced by 1.3 units (WMD −1.31; 95% CI, −2.07 to −0.54). In T2DM obesity, BMI had a modest decrease (WMD −1.00; 95% CI, −1.30 to −0.70). Both results were statistically significant (test of WMD = 0: z = 7.41, p = 0.000; Figure 3).
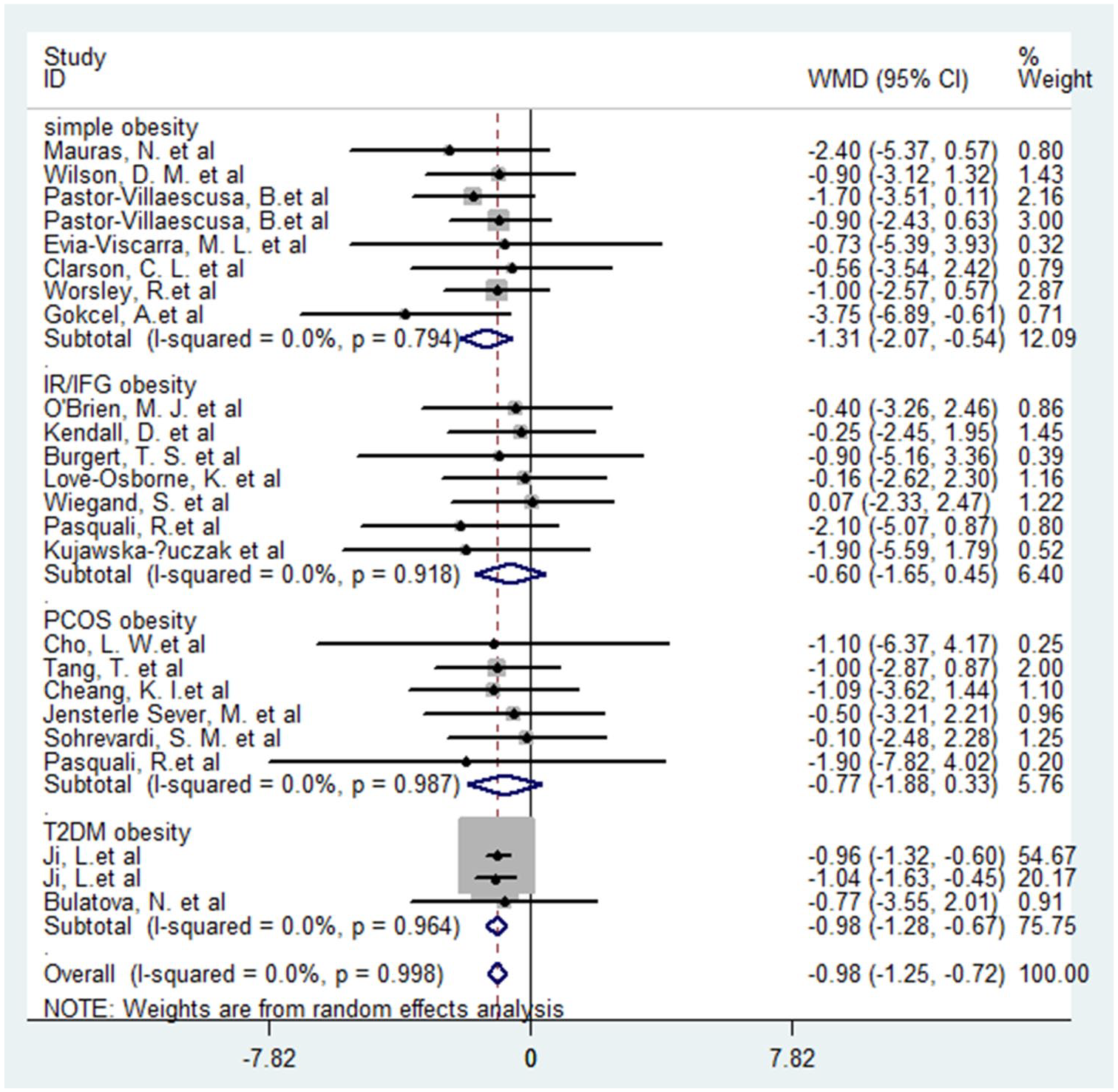
Meta-analysis of metformin treatment on BMI in different populations.
Analysis of subgroups
Subgroup stratified analysis was conducted to further analyze the effect of metformin on weight loss, as shown in Table 2. Subgroup analysis was performed by stratifying baseline BMI of participants, age, dosage, and treatment length (Table 2).
Subgroups analysis.

BMI, body mass index; CI, confidence interval; WMD, weighted mean difference (used for the study of continuous variables with the same unit of measurement in meta-analysis).
Baseline BMI of participants
Table 2 shows that the estimates for all groups were statistically significant. Analysis indicated that metformin treatment had significant reductions in BMI (WMD −1.12, −1.84 to −0.39) in Class II and III obesity (BMI > 35 kg/m²) compared with baseline BMI. This finding may indicate improved effects of metformin for patients with a BMI > 35 kg/m2 (Table 2).
Mean age of participants
Subgroup analysis of mean age of participants was conducted. The three groups were 7–18, 19–39, and 40–56 years old. Analysis indicated that metformin treatment have significant reductions in BMI (−1.02, 95% CI, −1.13 to −0.73) in older adults compared with baseline BMI, and in adolescents the BMI decreased about 0.8 units (−0.84; 95% CI, −1.52 to −0.16) (Table 2).
Dose of metformin
Analysis of metformin dose showed that high doses of metformin treatment have a significant reduction in BMI (WMD−1.01; 95% CI, −1.29 to −0.73) compared with baseline BMI. And the BMI decreased about 0.9 units (WMD −0.88; 95% CI, −1.63 to −0.14) at the end of low dose metformin treatment (Table 2).
Treatment length of metformin
Subgroup analysis of different intervention lengths (<6, 6, and >6 months) is shown in Table 2. Compared with baseline BMI, 6 months of metformin treatment showed the most evident reduction in BMI (WMD −1.09; 95% CI, −1.71 to −0.47). In the four included studies (n = 171),19,23,26,34 metformin intervention lasted 6 months or more. However, after 6 months of metformin treatment, there was no significant decrease in BMI. Research has found that, after 12 months of treatment, most of the patients have regained their weight 11 (Table 2).
Comprehensive analysis of metformin effect on BMI
The use of a three-dimensional histogram to demonstrate the effect of metformin on BMI had been attempted. Metformin in the treatment of simple and T2DM obesity showed that patients with a higher BMI obtained significant benefits, as respectively shown in Figure 4(a) and (b). Considering the WMD of BMI in simple overweight patients (−1.23), classes I (−1.10) and II (−2.1) obesity had evident reductions (z = 3.4, p = 0.001). In T2DM obesity, the WMD of BMI in patients with class II obesity (−1.62) also demonstrated significant reductions (z = 6.5, p = 0.000). Figure 4(c) shows the effect of metformin intervention length on obese patients at different degrees. However, no significant difference was found between the two treatment times (z = 2.33, p = 0.020). High dose metformin (>1500 mg/d) was more effective in reducing BMI, especially in obese patients with a BMI larger than 35 kg/m2. As shown in Figure 4(d), high dose of treatment in overweight patients (−0.96, 95% CI, −1.32 to −0.6), class I obesity (−1.0, 95% CI, −1.51 to −0.48), and class II obesity (−1.30, 95% CI, −2.15 to −0.45) had minimal heterogeneity (p = 0.986, I2 = 0.0%) and good significance (z = 1.27, p = 0.000).

Comprehensive analysis of metformin effect on BMI.
Sensitivity analysis and funnel plot
No significant heterogeneity was observed in these studies. In addition, the funnel diagram was roughly symmetrical, suggesting a slight influence of publication bias (Begg’s Test: p > | z| = 0.264; Egger’s test: p > | t | = 0.702; Figure 5).

Funnel plot of weighted mean difference in BMI.
Discussion
The mechanism of metformin’s effect on body weight may be multifactorial. Long-term follow-up from the Diabetes Prevention Program demonstrates that the primary weight loss mechanism of metformin is improving IR and decreasing food intake. 40 Recent studies highlighted that gastrointestinal physiology and circadian rhythm changes by metformin also regulate fat oxidation and storage in the liver, skeletal muscles, and adipose tissues.41,42
A recent systematic review found that metformin treatment is associated with BMI reduction (MD −0.86; 95% CI, −1.44 to −0.29) in children and adolescents in comparison with placebo. 12 This finding is a high-quality report of weight management and intervention in children and adolescents; the report indicates that the weight loss effect is different between subgroups (age and male percentage). However, the suitability of the situation in children and adolescents for other populations remains unclear. In addition, a recent study found that orlistat and metformin exhibited similar effects on BMI (WMD −0.65%; 95% CI, −2.03 to 0.73) in women with PCOS. 13 Most results of BMI changes in systematic reviews for metformin based on different populations are similar but different in magnitude.
In the present meta-analysis, baseline BMI was chosen as a self-control to compare the changes in BMI of different populations before and after metformin treatment. Self-control is a common study method that explains the experimental results through the changes of the same population before and after intervention. When studying the effect of metformin on BMI, choosing baseline BMI as self-control can minimize the influence on the result from different control groups. Even if the control group was a lifestyle intervention, the standard of exercise and patient dependence vary significantly.
Overall, a reduction in baseline BMI with metformin therapy for 6 months was calculated at approximately 1 unit in all included populations. Simple obesity patients had the most evident decrease in BMI (WMD −1.31; 95% CI, −2.07 to −0.54, I2 = 0%). In addition, metformin can relieve diabetes symptoms and reduce BMI (WMD −0.98; 95% CI, −1.25 to −0.72) for T2DM obesity. The present meta-analysis indicated that metformin treatment was beneficial for obesity patients with BMI >35 kg/m2. This finding was also consistent with the results of studies in other single populations.4,43–46 A dose comparison considering the weight loss effect of metformin in obese women with PCOS demonstrated that substantial weight reduction is potentially achievable with high doses of metformin. 47 This result is consistent with the current subgroup analysis. This analysis indicates that high-dose metformin treatment was more effective in reducing weight than low dose.
The advantage of the current study lies in its extensive population, comprehensive subgroup analysis, and intuitive results. In general, this study was the first meta-analysis of metformin effectiveness in weight loss that included several populations for comprehensive analysis. Metformin significantly affected simple obesity, and patients with severe obesity showed a significant reduction in BMI.
The present study has several limitations, including the number of studies and incomplete population inclusion. Some unpublished negative results may not be included. The data were analyzed by self-control, although the influence of different degrees of lifestyle intervention in various studies is excluded in theory, there might be some defects. The source data were not complete when using the three-dimensional histogram to demonstrate the effect of metformin on BMI. Therefore, some biases in the meta-analysis may exist, and more in-depth and detailed RCTs are necessary.
Conclusion
The results of the present meta-analysis indicate that metformin treatment had a modest reduction on BMI. Metformin is a good choice for overweight and obese individuals at high risk for diabetes. Patients treated with metformin experienced about a one-unit reduction in BMI at the end of treatment. Similar BMI reductions were observed in subgroup analyses including treatment duration, investigated populations, and metformin dose. However, whether this decreased value produced enough weight loss (5% of baseline body weight) to qualify as a “weight loss drug” as current guidelines require, requires larger RCTs involving specific height and weight.
Supplemental Material
s_Figure_6 – Supplemental material for Effects of metformin in obesity treatment in different populations: a meta-analysis
Supplemental material, s_Figure_6 for Effects of metformin in obesity treatment in different populations: a meta-analysis by Ruiyang Pu, Dian Shi, Ting Gan, Xiaoyu Ren, Yupei Ba, Yanbei Huo, Yana Bai, Tongzhang Zheng and Ning Cheng in Therapeutic Advances in Endocrinology and Metabolism
Supplemental Material
s_Figure_7 – Supplemental material for Effects of metformin in obesity treatment in different populations: a meta-analysis
Supplemental material, s_Figure_7 for Effects of metformin in obesity treatment in different populations: a meta-analysis by Ruiyang Pu, Dian Shi, Ting Gan, Xiaoyu Ren, Yupei Ba, Yanbei Huo, Yana Bai, Tongzhang Zheng and Ning Cheng in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
Author Contribution(s)
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This work is supported by the Belt and Road Special Project of Lanzhou University (No.2018ldbrzd008) and the Natural Science Foundation of China (No. 81673248).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.