
Abstract
It remains largely unknown as to why some individuals experience substantial weight loss with obesity interventions, while others receiving these same interventions do not. Person-specific characteristics likely play a significant role in this heterogeneity in treatment response. The practice of precision medicine accounts for an individual’s genes, environment, and lifestyle when deciding upon treatment type and intensity in order to optimize benefit and minimize risk. In this review, we first discuss biopsychosocial determinants of obesity, as understanding the complexity of this disease is necessary for appreciating how difficult it is to develop individualized treatment plans. Next, we present literature on person-specific characteristics associated with, and predictive of, weight loss response to various obesity treatments including lifestyle modification, pharmacotherapy, metabolic and bariatric surgery, and medical devices. Finally, we discuss important gaps in our understanding of the causes of obesity in relation to the suboptimal treatment outcomes in certain patients, and offer solutions that may lead to the development of more effective and targeted obesity therapies.
Introduction
Obesity remains at epidemic proportions in the United States (US), affecting nearly 40% of adults and 19% of children. 1 There is significant evidence to support the complex and multifactorial etiology of this disease. 2 While numerous interventions for the treatment of obesity are associated with overall mean weight loss, the degree of weight loss attained on an individual level can be highly variable. For example, in the Satiety and Clinical Adiposity Liraglutide Evidence (SCALE) Obesity and Prediabetes Trial of nondiabetic adults with obesity, the mean weight loss achieved with liraglutide was 8.4 kg; however, the standard deviation was nearly as high at 7.3 kg. 3 Similar findings have been reported in the pediatric literature across various obesity interventions. 4 Such variability in individual response suggests that obesity is a heterogeneous disease and that person-specific characteristics may be important determinants of treatment effectiveness. Given both the degree of heterogeneity in the etiology of obesity and the variability in individual responsiveness to treatment, personalized medicine strategies have the potential to be more effective than current approaches that often apply treatment modalities broadly without accounting for individual patient-level differences. 5
The National Institutes of Health defines precision medicine as “an emerging approach for disease treatment and prevention that takes into account individual variability in genes, environment, and lifestyle for each person.” 6 The goal of precision medicine is to optimize therapeutic benefit and minimize risk by targeting an individual’s specific needs based on their phenotype, genotype, or psychological factors. Optimizing therapeutic benefit includes finding the most effective treatment for an individual as efficiently as possible, especially as a patient’s willingness to follow up and continue in management may be affected by whether or not they perceive a benefit from the initial treatment. 7
In this review, we discuss precision medicine as it applies to the clinical care of adults and youth with obesity. Following a brief review of the biopsychosocial determinants of obesity in general, we present data on what is currently known about the individual variability in the effectiveness of interventions for obesity, focusing on characteristics associated with or predictive of treatment responsiveness. We selected studies based upon a review of published literature from PubMed and Google Scholar using the following keywords: (‘Predictor’ OR ‘Predictors’) AND (‘Weight Loss’ OR ‘Weight Loss Response’ OR ‘Weight Reduction’) AND [‘body mass index (BMI)’ OR ‘Weight’] AND (‘Intervention’ OR ‘Treatment’ OR ‘lifestyle’ OR ‘lifestyle modification’ OR ‘pharmacotherapy’ OR ‘medication’ OR ‘bariatric surgery’ OR ‘metabolic surgery’ OR ‘device’ OR ‘medical device). We additionally performed searches on the specific pharmacotherapies, metabolic and bariatric surgeries, and device therapies mentioned. We included randomized controlled trials (RCTs), retrospective and prospective cohort trials, and observational studies. Given the broad scope of this review, our intent was to discuss general trends and not to include every article published in this field. Finally, we identify important gaps in the literature and offer potential solutions in an effort to accelerate the development of more effective and targeted treatments for obesity.
The biopsychosocial determinants of obesity
Obesity is a multifactorial disease with individual, environmental, and socioeconomic determinants (Table 1).4,8 Fully understanding the complexity of the general factors contributing to obesity makes one appreciate how difficult it is to develop individualized treatment plans. The role of many of these factors as predictors of response to obesity interventions have yet to be explored. In this section, we present a brief overview of biopsychosocial contributors to the development and progression of obesity as a framework for understanding the challenges of applying precision medicine approaches to this complex disease.
Proposed causes and risk factors for the development of obesity. a

Nonexhaustive.
A significant portion of BMI is heritable. 9 A Genetic Investigation of ANthropometric Traits consortium (GIANT) meta-analysis identified 97 BMI-associated loci in adults of European descent accounting for 2.7% of the variability in BMI. 10 In total, more than 250 BMI-associated loci have been discovered among adults of African, east Asian, and European descent, 11 with many of these same loci also identified in children. 12 The GIANT consortium additionally uncovered 941 near-independent single nucleotide polymorphisms (SNPs) associated with BMI among adults with European ancestry accounting for 6% of the variance in BMI. 13 These findings suggest that, while a multitude of loci and SNPs play a role in BMI heritability, the majority of the genetic sources for the variability in BMI remain unknown. Certainly, ethnic and population differences underlie the genetic predisposition to obesity development. 14
Numerous genetic mutations have been associated with the development of severe monogenic obesity [e.g. brain-derived neurotrophic factor, leptin, leptin receptor, melanocortin 4 receptor, proopiomelanocortin (POMC)]. 15 Moreover, several genetic syndromes, including Prader–Willi, Alstrom, and Bardet–Biedl syndromes, are implicated. For some of these rare forms of obesity, accounting for fewer than 5% of all cases, 16 targeted therapies have been discovered (e.g. leptin for congenital leptin deficiency, 17 alpha-melanocyte stimulating hormone analog for POMC deficiency 18 and Bardet–Biedl syndrome 19 ). However, true monogenic obesity with targeted therapies is rare. Most cases of obesity are polygenic in origin, and targeted therapies for these cases are not currently available and will be substantially more difficult to establish. Further, the mechanisms by which genetic variants contribute to the development of obesity are largely unknown.
Peptide hormones [e.g. insulin, ghrelin, glucagon-like peptide-1 (GLP-1)] and neurotransmitters (e.g. dopamine, serotonin, gamma-aminobutyric acid) play a significant role in the regulation of appetite, satiety, food reward, and addiction. Pharmacotherapies developed for the treatment of obesity target the actions of these specific hormones and neurotransmitters, and perhaps are influenced by certain genotypes.20,21 The interaction of these pharmacotherapies with endogenous gut–brain hormones and neurotransmitters, along with inter-individual differences in the functionality of receptors upon which these hormones interact, represent additional sources of variability in drug response.
In addition to genetic and physiologic factors, environmental and psychosocial determinants also play significant roles in obesity development and progression. For example, individuals of low socioeconomic status are more likely to live in neighborhoods with fewer physical fitness resources, 22 and such adverse surroundings increase the odds of being overweight by 20–60% in children. 23 In a study examining exposure to ‘healthy’ fast food meal advertising, a child’s fondness for fast food increased after such exposure; however, healthier dietary choices did not. 24 The home environment also impacts an individual’s likelihood of developing obesity, and may impact his or her response to therapeutic interventions.25,26 In addition, psychological factors must also be considered. For example, Sutaria and colleagues found that children with obesity compared with those with normal weight were significantly more likely to have depression. 27 Attention deficit–hyperactivity disorder has similarly been linked to obesity. 28
One potentially important link between these genetic, physiologic, and environmental determinants of obesity is epigenetics, or the heritable changes that influence gene expression without affecting the DNA sequence. 29 The recent development of epigenome-wide association studies (EWASs) allows for the investigation of such interactions. 30 For example, in a study of 2097 African-American adults, 37 methylation variants in blood were associated with BMI. 31 In another study, paternal obesity was associated with insulin-like growth factor-2 (IGF-2) hypomethylation among 628 newborns. 32 Indeed, those who are genetically predisposed to obesity development may be more susceptible to doing so when placed in increasingly obesogenic environments.
It is important to note that the potential causes of obesity listed above is not exhaustive, and numerous other factors have been associated with its development. These include prenatal weight gain and the presence of gestational diabetes in the mother, gestational weight, medications associated with weight gain, environmental toxins, and an individual’s microbiome, transcriptome, and proteome.33–35
Heterogeneity in the effectiveness of interventions for the treatment of obesity
While numerous studies have identified the characteristics associated with or predictive of weight loss response to obesity interventions, the most reliable predictors appear to be degree of adherence to the intervention, and early weight loss as a predictor of later or sustained weight loss (which is important to consider when determining whether to continue therapy).36–40 Most studies reporting person-specific characteristics associated with weight loss response were performed in adults; however, a few have examined these factors in children. In this section, we review the evidence on the characteristics associated with weight loss response to lifestyle modification therapy (LMT), pharmacotherapy, metabolic and bariatric surgery (MBS), and medical devices.
Lifestyle modification therapy
Table 2 summarizes studies identifying characteristics associated with weight loss response to LMT. Not surprisingly, a higher degree of adherence to various components of LMT and early weight loss have both been associated with better long-term outcomes.40–44 Psychosocial factors associated with improved weight loss response in adults include greater social support; 45 higher baseline exercise self-efficacy, 46 dietary restraint, 47 flexible cognitive restraint, 48 and motivation (in men); 48 lower levels of psychopathology (in women), 49 emotional eating, 48 and disinhibition; 47 and fewer exercise barriers 48 and previous dieting attempts. 46 In children, higher levels of global self-worth have positively predicted weight loss response, 50 while higher levels of disordered eating in the child and the presence of psychopathology in the mother have been identified as negative predictors.39,50,51
Predictors of weight loss response to lifestyle and behavioral interventions.
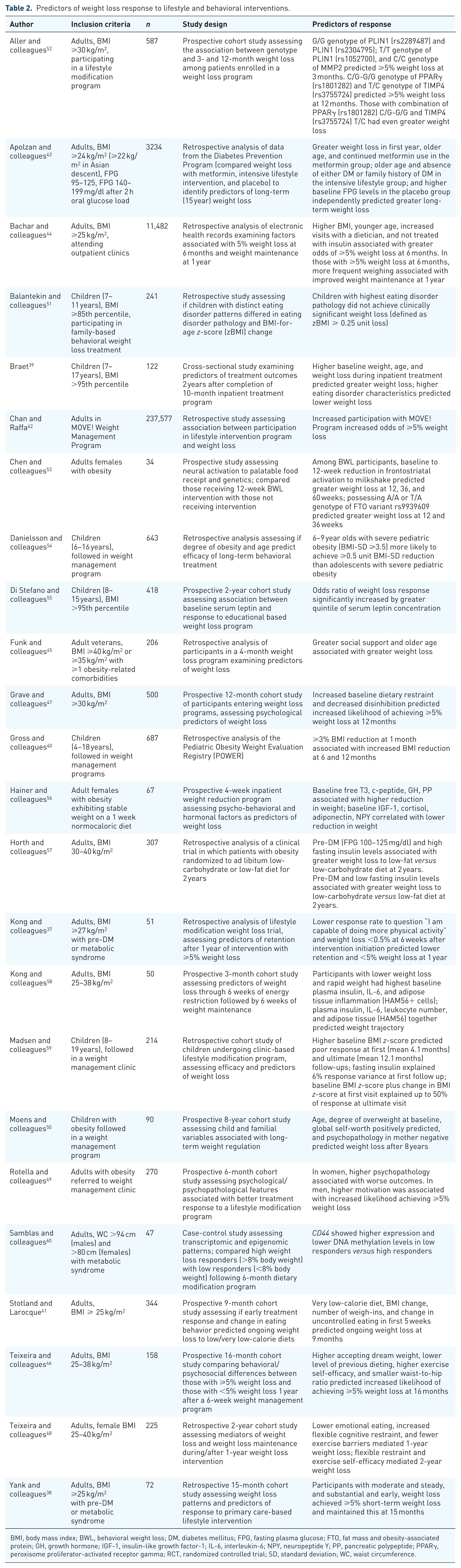
BMI, body mass index; BWL, behavioral weight loss; DM, diabetes mellitus; FPG, fasting plasma glucose; FTO, fat mass and obesity-associated protein; GH, growth hormone; IGF-1, insulin-like growth factor-1; IL-6, interleukin-6; NPY, neuropeptide Y; PP, pancreatic polypeptide; PPARγ, peroxisome proliferator-activated receptor gamma; RCT, randomized controlled trial; SD, standard deviation; WC, waist circumference.
Whether baseline weight status and age predict weight loss response to LMT remains unclear. In children, while Braet and Moens found that higher baseline weight predicted increased weight loss following inpatient and outpatient interventions, respectively, Madsen and colleagues showed that a higher baseline BMI z-score predicted a decreased weight loss to an outpatient intervention.39,50,59 In adults, both Heiner and colleagues and Azar and colleagues showed that higher baseline BMI was associated with greater weight loss to LMT programs.56,61 As for age, Moens and colleagues found that older age during an outpatient intervention positively predicted weight loss 8 years later in children, while Danielsson and colleagues showed that younger children were more likely to achieve clinically significant weight loss during a 3-year outpatient intervention.50,54 In adults, while Apolzan and colleagues and Funk and colleagues found that older age was associated with greater short and long-term weight loss to LMT programs, respectively, Bachar and colleagues found that younger age was associated with a higher odds of achieving 5% or greater weight loss at 6 months.43–45
Several studies have examined the hormonal characteristics associated with weight loss response to LMT. For example, in a 12-week prospective trial assessing weight loss predictors after energy restriction followed by weight maintenance, adults with decreased weight loss during restriction and rapid weight gain during maintenance had higher baseline insulin, interleukin-6, and adipose tissue inflammation markers compared with adults with increased weight loss during restriction and continued weight loss or stabilization during maintenance. 58 In a 4-week women-only inpatient intervention involving calorie restriction, supervised activity, and cognitive behavioral modification, baseline c-peptide, growth hormone, pancreatic polypeptide, and free T3 concentrations were associated with increased weight loss, while insulin-like growth factor-1, cortisol, adiponectin, and neuropeptide Y levels correlated with decreased weight loss. 56 In a 2-year longitudinal study assessing the association between baseline leptin levels and weight loss to an educational based program in children, the odds of weight loss increased with greater leptin concentrations. 55 Combined, these studies suggest that higher levels of inflammation (as expressed by such factors as adipose tissue inflammation, cortisol, adiponectin, and leptin) appear to be associated with a worse weight loss response to LMT. 55,56,58
Finally, a few studies have examined neural, genetic, and epigenetic predictors of weight loss response to LMT in adults. For example, Chen and colleagues studied neural activation to palatable food receipt and genetics in women who underwent a 12-week behavioral weight loss program. A greater reduction in frontostriatal activation to a milkshake from baseline to 12 weeks predicted increased weight loss at 12, 36, and 60 weeks, and possessing the A/A or T/A genotype of the fat mass and obesity-associated protein (FTO) variant rs9939609 predicted greater weight loss at 12 and 36 weeks. 53 Aller and colleagues found that polymorphisms in genes related to the regulation of fat storage and adipocyte structure adaptation predicted 3- and 12-month weight loss to an LMT program. 52 Samblas and colleagues showed that, among adults undergoing a 6-month dietary modification program, baseline CD44 in white blood cells showed lower expression and higher DNA methylation levels in those who achieved 8% or greater weight loss compared with those achieving less than 8%. 60 This suggests that CD44 gene transcription and methylation may be a useful biomarker for weight loss prediction. 60 Gardner and colleagues showed that, among adults with overweight and obesity prescribed either a healthy low-fat or low-carbohydrate diet, SNP multilocus genotype patterns were not associated with the dietary effects on weight loss for either diet. 62
Pharmacotherapy
There are five US Food and Drug Administration (FDA)-approved medications for the long-term management of obesity in adults: orlistat, phentermine/topiramate, lorcaserin, naltrexone/bupropion, and liraglutide. Phentermine is approved for short-term weight loss, and studies also have shown topiramate monotherapy63,64 and exenatide65,66 to be effective. In adolescents 16 years of age or younger, orlistat is the only US FDA-approved medication for weight loss; however, many of the medications used in adults are also used in pediatric weight management clinical settings. 67 It is important to note that our understanding of the underlying mechanisms leading to weight loss for many of these medications continues to remain incompletely understood.
Review of the RCTs leading to US FDA approval of the available obesity pharmacotherapies largely show a similar pattern: overall mean weight loss with considerable response variability on an individual level.2,68–70 Person-specific characteristics likely contribute to the heterogeneity in weight loss response seen in these large-scale RCTs. To date, numerous studies have examined characteristics associated with weight loss response to obesity pharmacotherapies (Table 3). A majority of these investigations involve orlistat71–76 and GLP-1 receptor agonists (GLP1-RAs)77–85 in individuals with overweight/obesity, or topiramate in individuals with seizure disorders with or without obesity.86–89 Studies evaluating hormonal, genotypic, and neuronal predictors of weight loss response are rare.78,90,91
Predictors of response to obesity pharmacotherapies.

BMI, body mass index; DM, diabetes mellitus; DPP4, dipeptidyl peptidase-4; fMRI, functional magnetic resonance imaging; HbA1c, hemoglobin A1c; HNF1A, hepatocyte nuclear factors 1-alpha; INSR, insulin receptor; LMT, lifestyle modification therapy; NB16, 16 mg naltrexone SR/360 mg bupropion SR; NB32, 32 mg naltrexone SR/360 mg bupropion SR; RCT, randomized controlled trial; SCALE, Satiety and Clinical Adiposity Liraglutide Evidence; SNP, single nucleotide polymorphism; SU, sulfonylureas; T2DM, type 2 diabetes mellitus; WC, waist circumference.
Early weight loss is the most commonly described predictor of sustained weight loss in response to obesity pharmacotherapies. Rissanen and colleagues and Toplak and colleagues both found that weight loss of 5% or greater at 3 months predicted sustained weight loss with orlistat at 1 and 2 years, respectively.74,75 Smith and colleagues analyzed pooled data from the Behavioral Modification and Lorcaserin for Overweight and Obesity Management (BLOOM) trials and reported similar results with lorcaserin. 92 In analyses of pooled data from the Contrave Obesity Research (COR) and SCALE trials, Fujioka and colleagues found that those with 5% or greater weight loss at 4 months were more likely to maintain clinically significant weight loss 1 year after starting liraglutide 79 and naltrexone/bupropion, 97 respectively. In a study of adolescents and adults with epilepsy prescribed topiramate, 3-month weight loss predicted greater BMI reduction at 6 months. 89
Increased hunger and food intake, as well as decreased satiety, are commonly identified baseline eating behavior characteristics associated with increased weight loss response to obesity pharmacotherapies. Such findings have been noted in analyses involving exenatide, 85 topiramate, 89 phentermine, 93 and topiramate/phentermine. 95 For example, in a prospective trial of adults prescribed phentermine, Thomas and colleagues found that increased desire to eat and lower cognitive restraint at baseline were more common in those experiencing 5% or greater weight loss after 2 months compared with those with less than 5% weight loss. 93 In an analysis of pooled data from the COR trials, Dalton and colleagues showed that those with the greatest improvement in craving control at 8 weeks had increased weight loss 56 weeks after starting naltrexone/ bupropion, which is not surprising given naltrexone’s mechanism as an opiate receptor agonist. 96
Whether sex predicts weight loss response to obesity pharmacotherapies remains unclear. In a retrospective analysis of adults prescribed orlistat, self-reported weight loss was significantly greater in males than in females; however, compliance, which can be challenging with this medication due to gastrointestinal side effects, was not formally assessed. 72 In contrast, Kazerooni and Lim examined weight loss outcomes after topiramate initiation in a Veteran population and found that the prevalence of 5% or greater weight loss after 1 year was 14% higher in females than in males. 94 Similarly, female sex predicted a greater BMI reduction 3 months following exenatide initiation in adolescents with severe obesity, a finding also described in adolescents with insulin resistance receiving metformin.85,98 Sex differences in weight loss response to obesity pharmacotherapies may be related to medication–hormonal interactions known to be different between sexes, including leptin which is present in higher concentrations in females compared with males at all BMI levels.85,99
Only a few studies have explored physiologic, pharmacokinetic, and genotypic predictors of weight loss response to obesity pharmacotherapies. For example, Halawi and colleagues showed that delayed gastric emptying at 5 weeks correlated with increased weight loss with liraglutide at 4 months, suggesting that gastric emptying may be a biomarker of responsiveness to determine those suitable for prolonged treatment with this medication. 81 Wilding and colleagues performed a retrospective analysis of pooled data from RCTs involving liraglutide and found that increased drug exposure (assessed by area under the concentration–time curve) was associated with greater weight loss. 82 In a 4-week trial using functional magnetic resonance imaging (fMRI) to assess neuronal activation to lorcaserin, Farr and colleagues demonstrated that baseline amygdala, parietal, and visual cortex activations correlated with decreased caloric intake and BMI among adults with obesity. 90 Additionally, in a study of DNA samples from participants who completed RCTs assessing topiramate for obesity treatment, carriers of a haplotype T-C-A in the INSR gene, and the SNP rs55834942, had greater weight loss compared with noncarriers. 91
Specifically, in adults with type 2 diabetes mellitus (T2DM) prescribed GLP1-RAs, a lower hemoglobin A1c level seems to predict an improved weight loss response.78,83 Further, a higher baseline weight status,80,84 longer duration of treatment, 80 and previous use of dipeptidyl peptidase 4 inhibitors 84 have also been associated with better weight loss outcomes. Overall, while some predictors of weight loss response to obesity pharmacotherapy have been uncovered, there is a myriad of others yet to be elucidated.
Metabolic and bariatric surgery
Table 4 summarizes studies identifying characteristics associated with weight loss response to MBS. A majority of these studies involve Roux-en-Y gastric bypass (RYGB),100–113 with a few evaluating vertical sleeve gastrectomy (VSG), 114 laparoscopic adjustable gastric banding (LAGB),115–117 biliopancreatic diversion (BPD), 118 sleeve gastroplasty, 119 or a pooling of data from multiple procedures.120–124 Overall, studies exploring predictors of weight loss response to MBS in adolescents are rare.108,116
Predictors of response to metabolic and bariatric surgery.
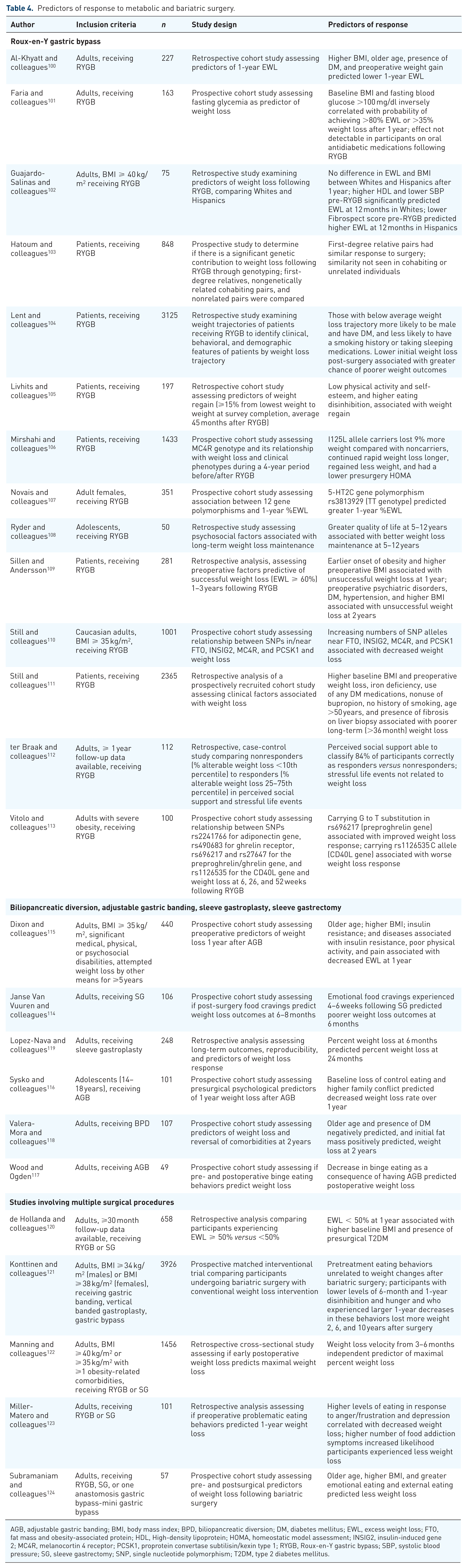
AGB, adjustable gastric banding; BMI, body mass index; BPD, biliopancreatic diversion; DM, diabetes mellitus; EWL, excess weight loss; FTO, fat mass and obesity-associated protein; HDL, High-density lipoprotein; HOMA, homeostatic model assessment; INSIG2, insulin-induced gene 2; MC4R, melanocortin 4 receptor; PCSK1, proprotein convertase subtilisin/kexin type 1; RYGB, Roux-en-Y gastric bypass; SBP, systolic blood pressure; SG, sleeve gastrectomy; SNP, single nucleotide polymorphism; T2DM, type 2 diabetes mellitus.
Similar to the other interventions, early weight loss predicts sustained weight loss, as noted in studies of adults who underwent sleeve gastroplasty, RYGB, and VSG.119,122 The most commonly identified predictor of worse response appears to be a higher baseline BMI as seen with RYGB,100–101,109,111 LABG, 115 and VSG. 120 Older age, fasting glycemia, and the presence of T2DM have additionally been associated with worse outcomes as seen in studies examining RYGB,100,101,104,111 LAGB, 115 VSG,111,120 and BPD. 118 Al-Khyatt and colleagues, Lent and colleagues, and Sillen and Andersson all showed that the presence of diabetes at baseline predicted worse weight loss response to RYGB, while Dixon and colleagues showed that baseline insulin resistance was associated with decreased weight loss 1 year following LAGB.100,104,109,115
Numerous investigations have examined psychosocial and eating behavior determinants of weight loss response to MBS. For example, the perception of social support has been associated with better response to RYGB, 112 and decreased binge eating appears to predict greater weight loss to LAGB in adults. 117 Among adolescents who underwent RYGB, greater weight-related quality of life was associated with weight maintenance 5 or more years after MBS. 108 Factors that have been associated with worse weight loss response to MBS include the presence of emotional food craving (with VSG 114 ), food addiction symptoms (with VSG or RYGB 123 ), loss of control eating (with LABG 116 ), and higher levels of eating in response to anger, frustration, or depression (with VSG or RYGB 123 ). Lower physical activity and self-esteem, and higher eating disinhibition, have been associated with long-term weight regain following RYGB. 105
A few studies have explored the genetic predictors of weight loss response to MBS, specifically to RYGB. For example, a longitudinal study by Hatoum and colleagues comparing first-degree relatives, nongenetically related cohabiting pairs, and nonrelated pairs undergoing RYGB found that, while first-degree relatives had a similar weight loss response to surgery (only a 9% difference in excess weight loss between members of each pair), no similarities were seen between cohabiting and unrelated individuals. 103 Carrying the I125L allele variant of MC4R, 105 the 5-HT2C gene polymorphism rs3813929 (TT genotype), 107 and a G to T substitution in rs696217 (preproghrelin gene), 113 have all been associated with improved weight loss response, while carrying the rs1126535 C allele (CD40L gene) 113 and increasing numbers of SNP alleles near FTO, insulin-induced gene 2 (INSIG2), MC4R, and PCSK1 have been associated with worse response to RYGB. 110
Medical device therapy
Studies examining predictors of weight loss response to medical devices are rare, and all have involved adults undergoing intragastric balloon therapy (Table 5).125–127 Consistent with other treatment modalities, early weight loss appears to predict sustained weight loss response.126,127 In two separate studies, older age was associated with greater weight loss.125,126 As for psychosocial factors, higher education level and social relationship scores, a strict exercise commitment, and increased number of follow-up visits have all been predictive of increased weight loss 6 months after intragastric balloon placement.125–127 Future studies are needed to explore the factors predictive of weight loss response to other medical devices, including vagal blockade and aspiration therapies.
Predictors of response to device therapy.
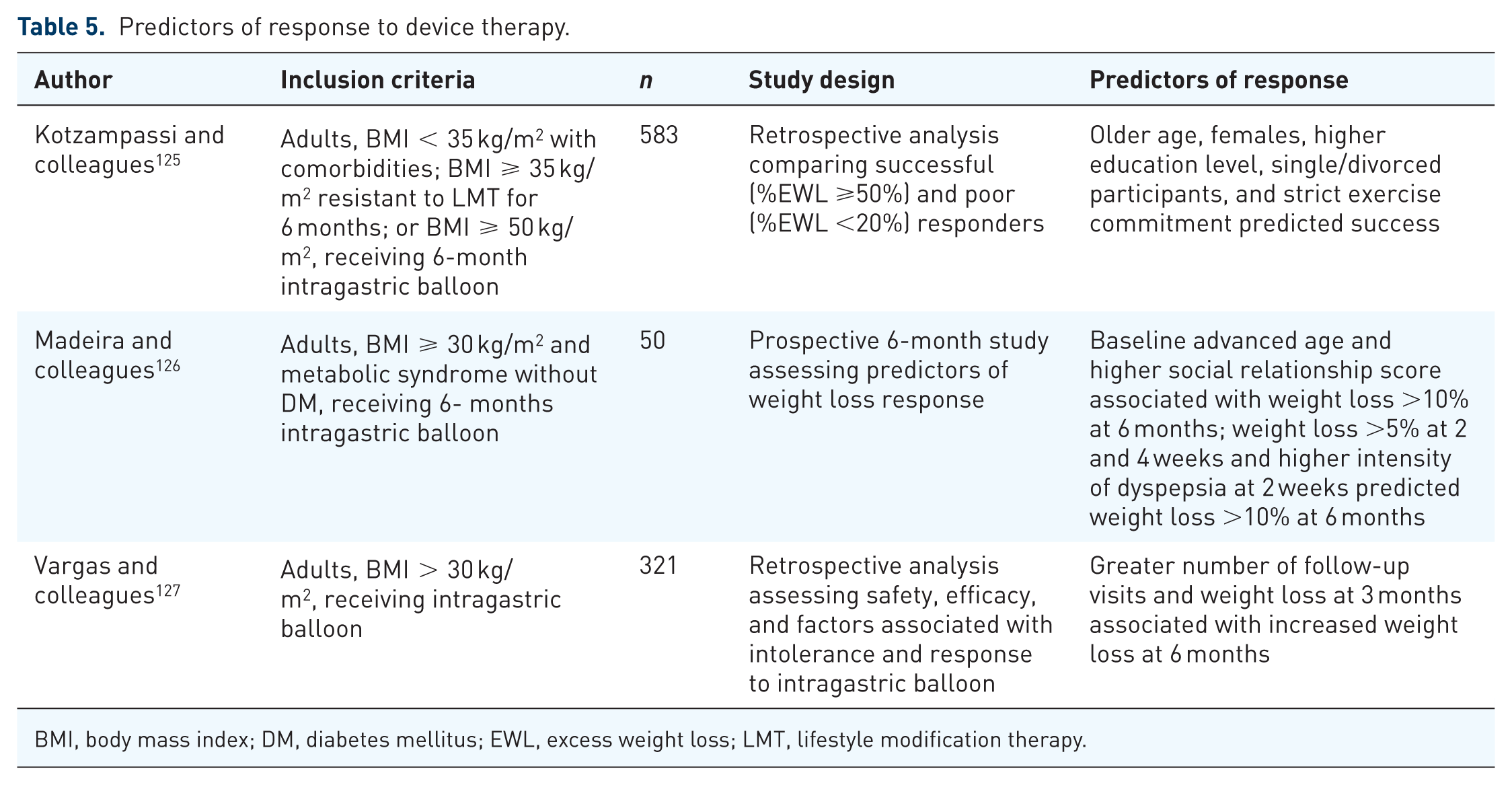
BMI, body mass index; DM, diabetes mellitus; EWL, excess weight loss; LMT, lifestyle modification therapy.
Gaps and opportunities for future research in the development of targeted therapies for obesity
It was 30 years ago that the American Diabetes Association proposed two classes of diabetes mellitus (DM): insulin-dependent (type 1) and insulin-independent (type 2). 128 Over time, new subgroups were discovered, including latent autoimmune diabetes in adults and mature onset diabetes in the young (MODY). A recent cluster analysis suggested five DM subtypes in adults, each with different patient characteristics and risks for complications. 129 Moreover, it has become clear that the treatments for DM, including therapy type (e.g. sulfonylureas for HNF1A- or HNF4A-MODY) and efficacy, differ depending on the underlying cause. Our understanding of the etiologies underlying obesity may not be far ahead of where our understanding of the etiologies underlying DM were not long ago. Similar to DM, the substantial degree of heterogeneity seen in individual response to weight loss interventions is likely due to an equally large degree of heterogeneity in the cause. Without a clearer understanding of the specific etiology or distinct phenotypes, which may be complex and are unlikely based upon single features, the development of directed treatments will be challenging.
While targeted treatments for several forms of monogenic obesity have emerged, most cases of obesity are polygenic in origin. In polygenic obesity, groups of alleles at different gene loci have variants each contributing a small additional effect towards body weight regulation. It may be that every individual with obesity carries his or her own specific polygenic variants.130,131 While precision medicine, as an approach, may be presently better suited for the treatment of monogenic obesity, continued advancements in genetics, pharmacogenetics, and epigenetics may eventually elucidate pharmacotherapeutic options for polygenic forms.
The rise of electronic health records (EHRs) and the subsequent creation of EHR-enabled clinical discovery cohorts may provide a valuable tool for examining person-specific characteristics associated with weight loss to interventions in the real-world setting. EHRs can be combined across multiple institutions to increase sample size and statistical power. 132 This is especially helpful for exploring outcomes to interventions in smaller groups of individuals, or for evaluating rare medication side effects. Integrating ‘-omic’ data (e.g. genomic, metabolomic) into the EHR will improve the capacity for identifying additional sources of variability in drug–response relationships that are too challenging to identify from smaller-scale studies. Further, large-scale observational studies combining EHR data with machine learning statistical techniques may allow us to better determine phenotypic characteristics associated with weight loss response to obesity interventions. That said, the heterogeneity in the approach to medical weight management and the inconsistent timing of patient evaluations leads to missing or flawed data, thereby limiting the amount of aggregated data that can be collected from EHR studies. Further, while correlation can be determined from such observational studies, causation cannot be, and compliance often cannot be readily assessed.
Similar to the way that combining meta-analyses has increased our identification of the loci and SNPs contributing to the development of obesity and the metabolic syndrome,10,11 combining data from obesity interventional trials may help us better identify subgroups of responders to various treatments. This is especially pertinent in pediatric obesity, where most studies are small and subgroup analyses are therefore limited. Fortunately, attempts are underway to standardize these processes, at least in the adult realm. The Accumulating Data to Optimally Predict obesity Treatment (ADOPT) Core Measures project was designed to provide investigators with tools to generate evidence through the use of common measures following four domains: behavioral, biological, environmental, and psychosocial. 133 Accumulating data on these factors will help inform the design and delivery of effective, tailored obesity treatments. 134
As mentioned previously, several phenotypic predictors of weight loss response have already been elucidated. The most consistently identified predictors of later response to an intervention are early response and higher adherence, 36 which should be reported in clinical trials. Increased baseline appetite and decreased satiety predict better response, while the presence of disordered eating and psychopathology predict worse response to several interventions.47–49,51,85,95,105,123 While these identified ‘primordial’ predictors represent the beginning of our understanding into person-specific characteristics predictive of weight loss response, many are not specific enough to help us tailor therapy. For example, given that increased hunger predicts greater weight loss response to exenatide, 85 topiramate, 89 and phentermine, 94 adding this variable to a pharmacotherapy selection algorithm may not help in the decision-making between these three options. In order to differentiate between which therapies to consider for each patient, we need to uncover personalized predictors that are specific to each intervention. Incorporating neuroimaging (e.g. fMRI), biobanks, and data repositories into studies evaluating characteristics associated with weight loss will help us discover predictors that are more precise.
Finally, future studies should also examine predictors of weight loss response to mobile health technologies, such as smartphone applications. Presently, evidence showing that these tools improve weight loss is mixed;135–138 however, as with other interventions improved adherence appears to predict greater weight loss response.139,140 Studies should also examine the optimal timing for treatment interventions. Such investigations should focus on determining the window of opportunity for when an intervention should be initiated in order to achieve the best possible response. Given that, among adolescents who develop obesity the most rapid weight gain appears to occur between the ages of 2 and 6 years, earlier interventions are likely needed. 141 The time course for beginning, discontinuing, or intensifying treatment in any population remains elusive and will require further investigation.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
J.R.R. received research support in the form of drug/placebo from Boehringer Ingelheim. C.K.F. received research support from Novo Nordisk. S.D.S. received grant funding from Astra Zeneca Pharmaceuticals. A.S.K. received research support (drug/placebo) from Astra Zeneca Pharmaceuticals and served as a consultant for Novo Nordisk, WW, and Vivus Pharmaceuticals but did not accept personal or professional income for these activities. The other authors have no disclosures.