
Abstract

Dear Editor,
Primary hyperparathyroidism (PHPT) is slowly becoming an ‘asymptomatic’ disorder. The diagnostic incidence has increased considerably due to the introduction of modern multichannel biochemical analysis, including routine assay of serum calcium. 1 The elevated parathyroid hormone (PTH) levels in PHPT are related to a shift in the set point of calcium-regulated PTH secretion such that despite the normal inverse sigmoid relationship, higher plasma calcium levels are needed to suppress PTH.2,3 Such high levels of PTH lead to increased renal resorption of calcium, increased osteoclastic bone resorption, phosphaturia and increased renal synthesis of 1,25(OH)2D (calcitriol), which in turn increases intestinal calcium absorption.2,4,5
Symptomatic and asymptomatic PHPT are both characterized by hypercalcaemia. In all forms of PHPT, kidney and bones are the chief target organs. Renal manifestations of PHPT include nephrolithiasis, nephrocalcinosis and hypercalciuria. In western countries, 70–80% patients with PHPT are asymptomatic but 20–30% of the symptomatic patients commonly manifest nephrolithiasis. 6 The rate of nephrolithiasis is variable in different case series and ranges from less than 10% to over 70%.7,8 Despite being classified as asymptomatic disease, patients with PHPT and kidney stones are symptomatic by definition and imaging studies have reported nephrolithiasis in 7–15% patients.9,10 By contrast, only 2–8% of patients with urolithiasis have been reported to have PHPT.11,12 The aetiology of renal stones is multifactorial; however, hypercalciuria is considered to be one of the primary risk factors. All patients with hypercalciuria don’t develop kidney stones but a significant proportion of patients may suffer from silent nephrolithiasis. Currently, it is not possible to confidently predict which patients with asymptomatic PHPT will actually develop kidney stone disease based on biochemical measurements on blood and urine samples alone.
We performed a retrospective analysis of 124 patients with PHPT who attended our endocrine clinics from October 2010 to December 2017. PHPT was diagnosed based on the presence of persistent hypercalcaemia with elevated or inappropriately normal PTH levels. Anthropometric, clinical and biochemical data of patients was recorded from their first visit to the clinic. Our patients were elderly (65.1 ± 12.3 years) and predominantly female (78.2%; n = 97). Radiological investigations [X-ray of the kidney, ureter and bladder (KUB); ultrasound of KUB (USS); and computed tomography (CT) scans of KUB] were performed during follow ups at the discretion of the clinicians who saw the patients initially. As some patients underwent more than one radiological imaging study, multiple positive results for ‘individual patients’ were therefore considered to be ‘one episode of stone disease’ to avoid duplication. The overall prevalence of occult urolithiasis was 14.5% (18/124 patients) of which 10 patients were male. Individually, CT KUB was most sensitive in locating silent stones (40.5%) in comparison with USS KUB (11.5%) and X-ray KUB (33.4%) (Table 1). In patients who had both CT and USS KUB (n = 16), 4 patients (25%) had positive results and 10 patients (62.5%) had negative results on both scans respectively. With any modality of imaging the most common location of stones was within the kidney (n = 11) followed with a combination in the pelvic ureteric junction (PUJ) and ureter (n = 5) and in the kidney and ureter (n = 2). In patients ‘with stones’, adjusted calcium (2.88 ± 0.32 versus 2.83 ± 0.20 mmol/l; p = 0.18), PTH (14.6 ± 11.0 versus 12.4 ± 7.4 pmol/l; p = 0.13) and urinary calcium/creatinine ratio (UCaCr) (0.76 ± 0.73 versus 0.65 ± 0.68 mmol/mmol; p = 0.25) were higher but not statistically significant but the renal function [creatinine: 87.9 ± 22.0 versus 74.6 ± 19.2 µmol/l; p = 0.004 and estimated glomerular filtration rate (eGFR): 71.6 ± 15.0 versus 76.8 ± 14.8 ml/min/1.73m2; p = 0.08] was significantly worse in comparison with patients ‘without stone’ disease. In a mutually adjusted multivariate logistic regression analysis of biochemical variables versus presence or absence of urolithiasis excepting gender (r = 0.31; p = 0.009), none of the other variables were predictive of renal tract calcifications.
Stones detected by different modes of imaging.
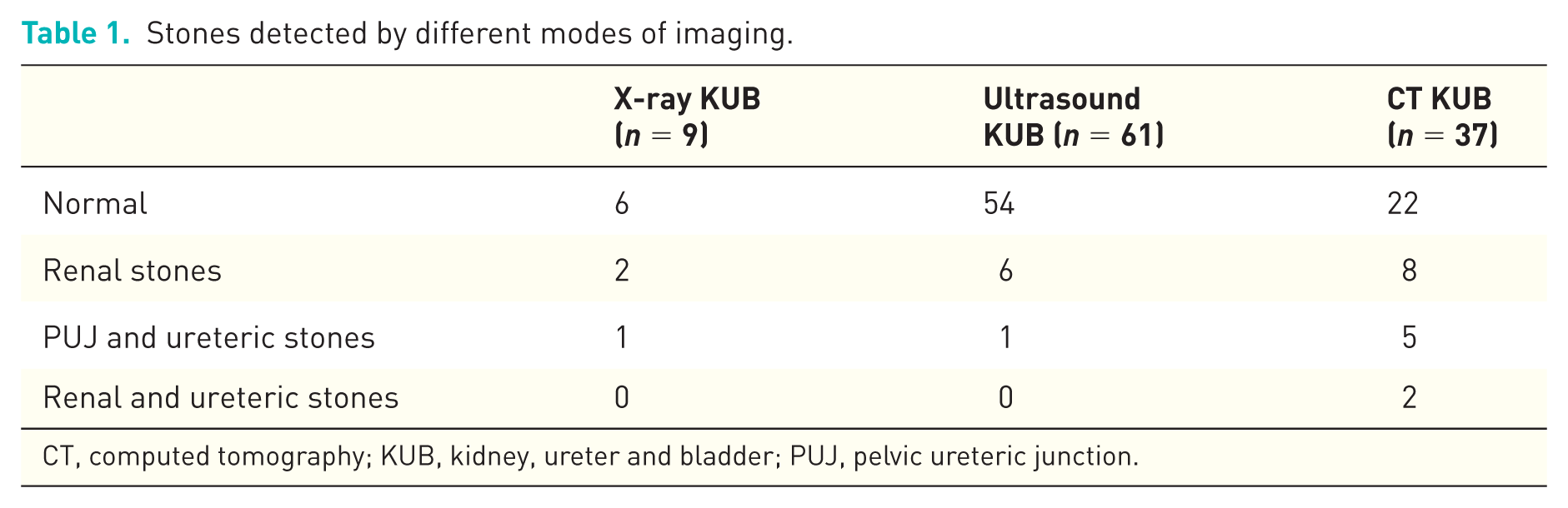
CT, computed tomography; KUB, kidney, ureter and bladder; PUJ, pelvic ureteric junction.
Our study demonstrated an overall prevalence of occult or silent stones in about 15% of patients. This is in agreement with other case series7–10,13,14 although the rates are widely variable due to the difference in cohorts, renal imaging and availability of clinical parameters. Such findings raise pertinent questions regarding reclassification of PHPT patients and might thus lead to a surgical decision in patients who are otherwise ‘asymptomatic’. Moreover it also raises the issue of use of routine imaging of the renal tract in these patients as undetected urolithiasis may lead to infection, urinary tract obstruction and loss of renal function as evidenced by elevated creatinine and eGFR in our patients. Urolithiasis alone may not contribute to the decline in renal function 15 but this may also be related to the extent and duration of hypercalcaemia.16,17
The best method for diagnosing renal tract stones remains debatable but CT scans appear to be more sensitive as evident from our and other studies.18,19 In our series, biochemical parameters did not differ significantly between ‘stone formers’ and ‘nonstone formers’ although other authors have demonstrated a higher risk of stone formation in patients with high urinary calcium levels.15,20 Cassibba and colleagues, 21 showed that in patients with PHPT, overt nephrolithiasis is associated with higher levels of serum calcium and PTH confirming the role of PHPT as a risk factor with further suggestions that silent nephrolithiasis helps to identify a more active and severe form of disease and these patients meet surgical indication more frequently than PHPT without stone disease. In contrast with these suggestions, we could not characterize the predictive risk factors for stone formation in PHPT, except that it was more prevalent in the male population.
We therefore conclude that nearly 15% of patients with PHPT may have silent or occult renal tract stone disease who are otherwise classified as ‘asymptomatic’. All patients after a diagnosis of PHPT, should have imaging of the renal tract as identification of asymptomatic renal tract stone disease is an indication for surgery, and by this approach patients can be cured who would otherwise develop stones during follow up.
Footnotes
Ethics approval and informed consent
The study was approved by the Research and Development (R&D) department of Cwm Taf University Health Board, UK (approval number: CT/895/17/18). As patients were not identified at any point of the analysis, the R&D department determined that informed consent was not necessary for this retrospective study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest