
Abstract
Background:
Diabetic retinopathy (DR) is the most common microvascular complication of diabetes mellitus (DM) and the foremost cause of blindness. This study aimed to assess the level of awareness of DR and its related risk factors among patients with DM in Jeddah, Saudi Arabia.
Methods:
A cross-sectional study was conducted among patients with DM attending primary health care centers at the Ministry of Health in Jeddah. A structured, pretested, self-administered questionnaire was used to collect information on the sociodemographic and DM- and DR-related characteristics of the patients.
Results:
A total of 377 patients were enrolled. About 82.6% of the patients were aware that DM can affect their eyes, and they listed physicians, ophthalmologists, television, and family members as common sources of information on the topic. About 36% of the patients reported that their doctors had not advised them about it. More than half responded that they did not feel their vision to be affected by DM. More than 58% had never been diagnosed with DR. About 35% did not go to their eye checkups, even though around 59% thought that DR could lead to blindness. Of the 64% of patients whose DM was well controlled, 11% and 25% listed surgery and laser treatment, respectively, as available treatment options for DR. The following factors were found to be significant in relation to the subjects’ awareness that DM can affect their eyes: the patients’ perception of their doctors’ advice about DR; the experience of having their vision affected by DM; the knowledge that DR may lead to blindness; the practice of going to eye checkups.
Conclusions:
Despite having good awareness about DM and its effects on eyes, the patients exhibited a relative lack of awareness about DR. Considering the association of DR with DM, its increasing magnitude is a potential burden on the community and health systems.
Introduction
The prevalence of diabetes mellitus (DM) is increasing globally in both developed and developing countries, 1 and it is estimated that the number of patients with DM will double by 2025, 2 making it a major public health problem. 3 In 2013, Saudi Arabia, with a high prevalence of 24%, was ranked seventh out of the top 10 countries for the prevalence of DM in people aged 20–79 years. 4 Worldwide, DM is a leading cause of blindness due to its ocular complications. 5
Diabetic retinopathy (DR) is the most common microvascular complication of diabetes 6 and the foremost cause of blindness in working-aged people and patients who are aged 55 years or older.7,8 DR is considered a significant blinding disease and is included in the disease-control strategy of the VISION 2020 initiative.9,10 It is estimated that up to 84.5% of patients with DM who have had the disease for more than 20 years will develop DR.2,11,12
In a national study in Saudi Arabia, the prevalence of DR was found to be 19.7%, 13 whereas other studies suggested a prevalence ranging from 16.7% to 31%.14–16 Both type 1 and type 2 DM can lead to DR. 17 DR is classified into two types: nonproliferative and proliferative. The former type may cause impaired vision if the macula is affected. 18 Proliferative DR can also result in blindness, and it is more serious. 19
Major risk factors related to the development and advancement of DR are a long duration of DM,20,21 poor glycemic control,21,22 hypertension,21,23 dyslipidemia, 24 nephropathy, 25 pregnancy, 26 and gender. 11 Control of the modifiable risk factors through periodic eye examinations and timely interventions has been shown to delay the progression of DR. 27
To help medical practitioners detect DR in its earliest and most treatable stages, the American Diabetes Association and the American Academy of Ophthalmology published guidelines for dilated retinal examinations. Patients with type 1 DM should begin their annual examinations 5 years after their diagnosis; those with type 2 DM should have an annual examination starting at the time of the diagnosis.28,29
Awareness of DM and DR, along with their health impacts and treatment, can be considered vital in motivating patients to pursue appropriate eye care and may, therefore, assist in dealing with visual impairment. In addition, for early diagnosis and treatment of DR, it is crucial to have a strong awareness of DR and its risk factors. 30 A lack of awareness about DM, DR, the importance of regular eye examinations, and the benefits of treatment among both primary care physicians and their patients can lead to poor compliance with guidelines, 31 delays in referral, and presentation with advanced DR, 32 all of which may impact the patient’s quality of life and the financial costs to health systems. 33 Despite the well-documented importance and magnitude of the issue in the literature, limited studies have explored the awareness of DR among patients with DM in the developing world,34–36 and the same dilemma exists in Saudi Arabia. More studies have focused on prevalence, screening, and the effects of DR around the world.37,38 Since DM and DR are continuously growing problems in the Saudi population and cause socioeconomic burdens for the healthcare system, this study aimed to assess the level of awareness of DR and its related risk factors among patients with DM in Jeddah, Saudi Arabia.
Methodology
A cross-sectional study was conducted in Jeddah, between 1 September and 31 December 2016. Jeddah is the second-largest city in Saudi Arabia; it is the main port of the country on the Red Sea, with an area of more than 1500 km and a population of more than 3.4 million. In Jeddah, there are 12 governmental hospitals, 38 primary healthcare centers (PHCCs), more than 30 private hospitals, and 128 polyclinics. The study was conducted among patients with DM attending the 38 PHCCs at the Ministry of Health in Jeddah City. All such patients attending the clinics during the study period were considered eligible to participate in the study. Patients re-visiting the PHCC during the study period or patients (or their relatives) who were reluctant or unable to provide written informed consent were excluded. The sample size of 377 was calculated using the single proportion equation in the Raosoft software package, 39 based on the assumption that the rate of DR awareness is 50% with a margin of error of 5% at the 95% confidence interval. A systematic random selection of every second patient with DM attending the PHCCs at the Ministry of Health was performed.
The structured questionnaire used in the study was prepared after a thorough literature review of papers relevant to the awareness of DR. The regional and local contexts were also considered to better fit the questionnaire with the study population and objectives. The questionnaire was validated by a group of experts in ophthalmology and family medicine. The final questionnaire included three parts: (a) sociodemographic characteristics (i.e. age, gender, marital status, smoking status, income, chronic illness, and education level); (b) DM-related characteristics (e.g. age diagnosed with DM, DM duration, type of DM, etc.); (c) DR awareness (e.g. diabetes can affect the eyes, can DR result in blindness, do you go for eye checkups, reasons for undergoing your first eye screening, barriers to doing eye screening, etc.). A pretest of 30 patients with DM in similar settings suggested minor revisions to the wording and layout of the study questionnaire. The questionnaire was self-administered when the patients visited the chronic illness clinics at their PHCCs. The data analysis was performed using Statistical Package for the Social Sciences version 21 (SPSS, 21) software. Other than exploring descriptive statistics, the chi-square test was used to find the association of awareness that DM can affect eyes with general DR awareness. Ethical approval was conducted by the research and ethics committees of the Ministry of Health and the King Abdulaziz University Hospital. Confidentiality was maintained and written or verbal consent was obtained from all the participants.
Results
In total, 377 questionnaires were selected for analysis. About 60% of respondents were above 50 years of age, with almost equal male and female representation. More than 67% were married, and about 57% were nonsmokers. Nearly 80% had an income of less than 10,000 Saudi Riyal per month. More than half of the study participants indicated that they had hypertension and/or dyslipidemia. A little over 33% reported a university-level education. A summary of the baseline characteristics is provided in Table 1.
Sociodemographic characteristics.

Around 30% of the study participants were between 35 years and 50 years of age. About 56% had been diagnosed with DM for more than 10 years. Around 75% of patients were being treated by either general or family physicians. About 60% were using oral hypoglycemic drugs (OHD) or a combination of diet, exercise, and OHD as a treatment. Almost 63% of patients were being treated at PHCCs. Above 73% reported a follow-up frequency of once in 6 months. More than 75% used a glucometer at home, and about 41% checked it when they felt unwell. Good sugar control was reported by about 64% of patients. A summary of the DM-related characteristics is given in Table 2.
Diabetes mellitus-related characteristics of patients.

DM, diabetes mellitus; OHD, oral hypoglycemic drugs.
When respondents were asked for their perspective on complications that may arise if DM is poorly controlled, they reported that eye disease, coronary artery disease, nephropathy, and stroke were more likely to happen, as shown in Figure 1.
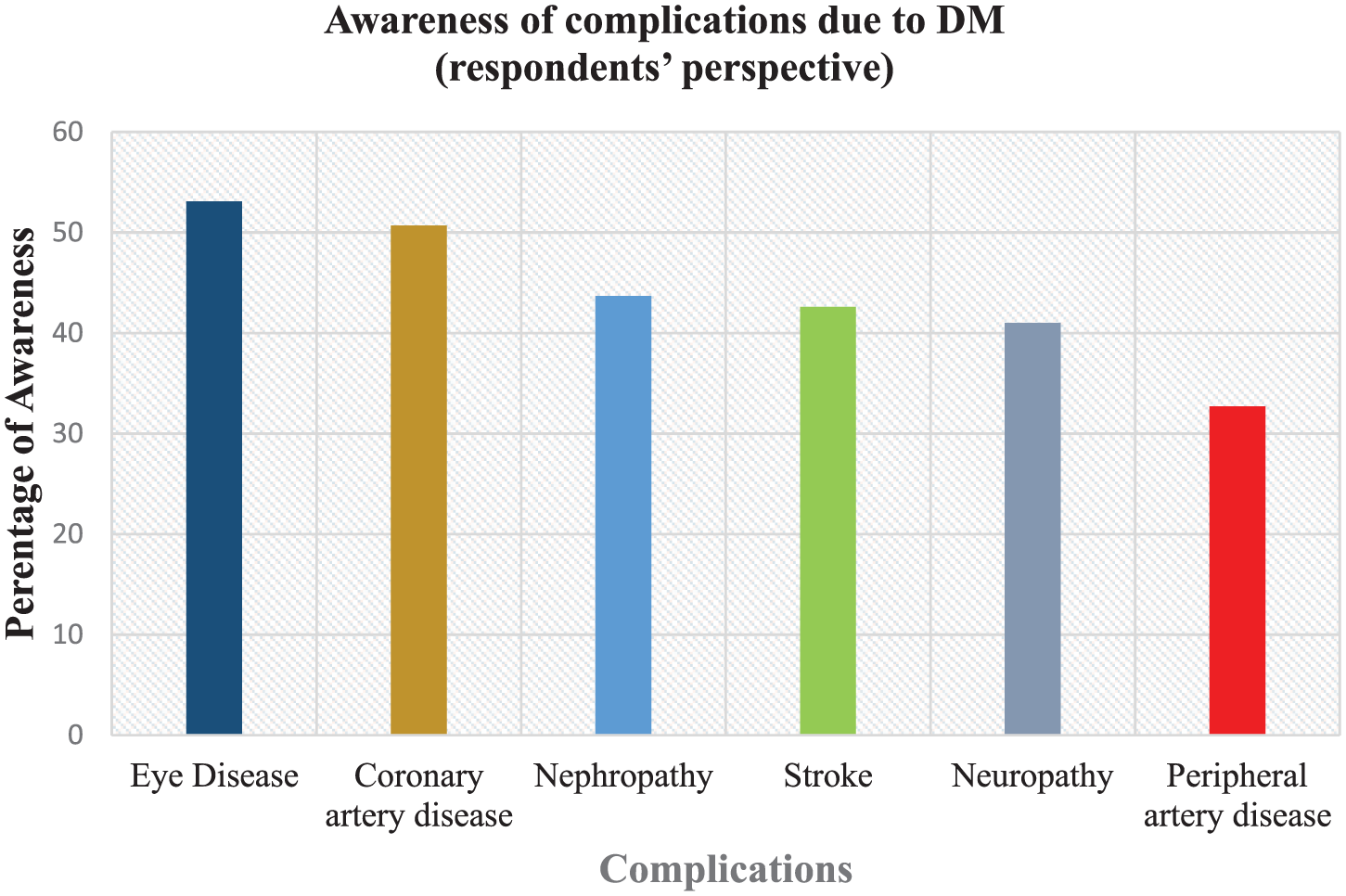
Awareness of complications due to diabetes mellitus (respondents’ perspective).
About 82.6% of the patients responded that they were aware that DM can affect their eyes. Their most frequent sources of information were physicians, ophthalmologists, television, family members, or someone else with DM, as shown in Figure 2.

Sources of information for patients who were aware that diabetes mellitus can affect eyes.
About 36% of the patients reported that they did not know anything about DR or their doctors had not advised them about it. More than half responded that they did not feel that their vision was affected by DM. More than 58% were never diagnosed with DR. About 35% did not go to their eye checkups, even though 59% thought that DR could lead to blindness. A doctor’s referral was the most frequent reason reported for undergoing the first eye screening, while a lack of knowledge about DR was the most frequently reported barrier to not undergoing an eye screening earlier. More than 63% of the patients thought that a person with DM should undergo an eye checkup once a year or every 6 months. About 42% responded that glasses may improve eyes that are affected by DM. Of the 64% who reported good control of their DM, 11% and 25% reported surgery and laser treatment, respectively, as available treatment options for DR. The following factors were found to be significant in relation to the subjects’ awareness that DM can affect their eyes: the patients’ perception of their doctors’ advice about DR; the experience of having their vision affected by DM; the knowledge that DR may lead to blindness; the practice of going to eye checkups. A summary of these responses is given in Table 3.
Association of awareness that diabetes mellitus can affect eyes with general diabetic retinopathy awareness (respondents’ perspective).

The chi-square statistic is significant at the 0.05 level. DM, diabetes mellitus; DR, diabetic retinopathy.
Discussion
This study explored the sociodemographic characteristics of, and awareness of DM and DR among diabetic patients visiting PHCCs in Jeddah .
Sociodemographic characteristics
The results of this study showed that most of the patients were from 35 years to 50 years of age, and the majority (around 80%) were from either low- or middle-income backgrounds. Hypertension and/or dyslipidemia were the most common comorbid conditions in the study population. Most of the population, around 76%, did not have a university-level education, with about 25% reported to be illiterate.
DM-related characteristics
More than half of the patients had been diagnosed with DM for more than 10 years. Many studies have highlighted the importance to DR of a longer duration of diabetes, alongside other risk factors.40,41 About 60% of the patients were using OHD or a combination of diet, exercise, and OHD as a treatment, and the majority were being treated by either general or family physicians. PHCCs were the place of treatment for almost 63% of the patients. The follow-up frequency of the majority was less than 6 months, and most patients used a glucometer at home, particularly when they felt unwell. This routine suggests a good awareness of DM. This could also be the reason why their perception of having good sugar control was found to be a little higher than in a similar study. 42
Among the complications that may arise if DM is poorly controlled, eye disease, coronary artery disease, nephropathy, and stroke were reported more often than others, also suggesting patients’ awareness of DM. However, these findings show relatively less awareness in this context in comparison with other studies. 42 Another study found that patients with DM who were unaware of DM complications had a four-fold increase in risk of major DM-related complications compared with those who were aware. 30
DR-related characteristics
When asked if they were aware that DM can affect the eyes, more than 82% of subjects gave a positive response. Subjects older than 30 years were found by Dandona and colleagues 43 to have an increased awareness of the likelihood of DM to cause impaired vision. The current study also showed a higher percentage of awareness compared with a study from India (37.1%) 1 but had findings comparable with those from Malaysia and Turkey.35,42 Among respondents who responded positively, the most frequent sources of information were physicians, ophthalmologists, television, family members, or someone else with DM. Several study findings suggested limited communication between doctors and their patients regarding DR: about 36% reported that they did not know about DR or that their doctors had not advised them about it. More than half responded that they did not feel that their vision was affected by DM, and about 35% did not go for their eye checkups. These findings align with similar studies44,45 but show relatively lower awareness than other studies.32,46
A doctor’s referral was the most frequently reported reason for undergoing the first eye screening, a finding also observed in a study conducted in Malaysia. 42 This also highlights the importance of health providers at primary care centers, as emphasized in a study in Ireland. 47 In contrast, a lack of knowledge about DR was the most frequently reported barrier for not undergoing an eye screening earlier; this has also been observed in other studies. 42 In addition, more than 36% of patients either said that a person with DM should undergo an eye checkup every 2 years or when they have vision problems or they had no knowledge. This is a considerable number, but one that agrees with an observation from a few similar studies.47,48 As health providers are usually considered to be the first point of access for patients who need treatment and health education,44,45,49 this finding also indicates some awareness gaps regarding DR compared with DM in general.
Surprisingly, about 59% of the subjects thought that DR could lead to blindness, but more than half had no knowledge or thought that glasses may not improve eyes that are affected by DM; this reflects their concern but shows that they are relatively less aware of DR compared with DM. Other findings also suggested a lack of awareness: more than 34% of subjects said that surgery and laser are not available treatment options for DR, and some patients responded that good control of DM cannot be helpful for DR. This finding is similar to another study conducted in India that also highlighted some gaps in treatment awareness and the necessity for more aggressive plans for awareness.1,44,45,49
The following factors were found to be significant in relation to the subjects’ awareness that DM can affect their eyes: the patients’ perception of their doctors’ advice about DR; the experience of having their vision affected by DM; the knowledge that DR may lead to blindness; the practice of going for eye checkups. These results also align with earlier findings of this study and highlight potential points to be considered for increasing patients’ awareness of DR. Possibly, care providers’ lack of expertise and training or their excessive focus on treatment rather than prevention might be the reason for low awareness about DR, but this needs further exploration.
Limitations of the study included the following: patients with DM were taken only from primary care centers and only from Jeddah, with no private sector information; and the questionnaire led mostly to descriptive findings and did not produce any scores that could better measure the issues and perform further inferential analyses. Furthermore, only the patients’ perspectives were recorded. Possibly, the findings could have been strengthened by obtaining the providers’ and other stakeholders’ perspectives on the issues discussed here. Despite these limitations, the study gives a superficial picture of the issue and also demonstrates the need for more studies to explore further the holistic context of the issue.
Overall, despite the subjects’ good awareness of DM, a relative lack of awareness of DR was observed among the study respondents. The study found that more than half of them had been diagnosed with DM for more than 10 years, which worsens the scenario, as the chances of DR rise with a longer period of diabetes; there may also be increased morbidities associated with DM because it is one of the leading causes of visual impairment. 37 Increased awareness of DR may lead to a better understanding of the disease process and may also underscore the importance of regular eye examinations for the early detection and treatment of DR, thereby reducing its sight-threatening complications.
Conclusion
This study showed a relative lack of awareness of DR compared with DM and its effects on eyes among the patients in the study population. Considering the association of DR with DM, the increasing incidence of DR may be a potential burden on community and health systems. This study suggested that all stakeholders, including policymakers and especially health providers, should prioritize building awareness. In addition, all available and feasible resources should be channeled toward reducing the burden of DR.