
Abstract
There have been several new treatment approaches established for the management of hyperglycemia in type 2 diabetes (T2D), with treatment guidelines listing both glucagon-like peptide 1 receptor agonists (GLP-1 RAs) and basal insulin therapies as considerations for patients who have failed to control their blood glucose with oral antidiabetic agents. New studies have highlighted the importance of initiating combination therapy earlier in the T2D disease process to avoid clinical inertia and prevent the long-term complications arising from uncontrolled diabetes. Until recently, both GLP-1 RAs and basal insulin therapies were only available as single agents, but there are now two combination pen devices that deliver both a GLP-1 RA and basal insulin simultaneously. This article reviews the current clinical evidence evaluating the use of these combination GLP-1 RA/basal insulin preparations to treat T2D, presents both potential benefits as well as possible downsides with the use of these agents, and discusses the current place in therapy these products represent in the management of T2D.
Introduction
Type 2 diabetes (T2D) is a chronic, progressive disease affecting over 400 million people globally and over 30 million people in the United States. 1 The disease is a result of multiple pathophysiologic defects including insulin resistance, reduced beta cell function, increased hepatic glucose output, inappropriate glucagon secretion, and decreased incretin effect. 2 Good glycemic control is crucial in order to reduce the risk of long-term disease-related complications such as retinopathy and kidney disease.3,4 This goal remains difficult to achieve in a large portion of patients with T2D, despite a growing armamentarium of treatment options. Data from the National Health and Nutrition Examination Survey showed that only 57% of people with diabetes achieved a goal A1C <7% in 2003–2004. 5 Another study showed that only 52.5% of people with diabetes achieved a goal A1C <7% in 2007–2010. 5 A more recent study showed that, while the use of antihyperglycemic agents has changed significantly from 2006 to 2013, the proportion of patients achieving an A1C <7% declined from 56.4% to 54.2%. 6
Current treatment recommendations by the American Diabetes Association (ADA) recommend a stepwise approach to achieving glycemic control starting with the initiation of metformin and adding therapy every 3 months until glycemic control is reached. 3 Unfortunately, clinical evidence suggests that significant delays in treatment intensification are common. Khunti et al. found that the median time to add a second oral antihyperglycemic agent in T2D patients with an A1C >7% was 2.9 years. 7 Khunti et al. also found that, in patients treated with basal insulin, the median time from basal insulin initiation to treatment intensification was 4.3 years. 8
These studies highlight the continued need for effective and durable treatment approaches as well as better intensification strategies to achieve and sustain glycemic control. A more physiologic approach to treatment in which combination therapy is initiated earlier in the disease process to target multiple pathophysiologic defects may be more appropriate.2,9,10
Combining basal insulin with a glucagon-like peptide 1 receptor agonist (GLP-1 RA) has many potential benefits. Basal insulin is a recommended treatment option at many stages of T2D and is effective at lowering fasting plasma glucose (FPG). The dose can be titrated to the individual patient’s needs; however, it increases the risk of hypoglycemia and weight gain. GLP-1 RAs are also recommended treatment options at multiple stages of T2D and have complementary mechanisms of action to basal insulin. GLP-1 RA increases glucose-dependent insulin secretion, decreases glucose-dependent secretion of glucagon, slows gastric emptying and increases satiety. Short-acting GLP-1 RAs (exenatide, lixisenatide) primarily lower post-prandial glucose (PPG) and longer-acting GLP-1 RAs (albiglutide, dulaglutide, exenatide XR, and liraglutide) lower both FPG and PPG. GLP-1 RAs are attractive add-on options to basal insulin because they decrease weight and have a low risk of hypoglycemia, however they do cause gastrointestinal (GI) adverse effects (AEs). Clinical studies have demonstrated improved glycemic control and low risk of hypoglycemia and weight gain with the combination of basal insulin plus a GLP-1 RA. 11
Until recently, basal insulin and GLP-1 RAs had to be administered separately. Combining basal insulin with a GLP-1 RA in a single injection may have additional benefits such as improved adherence. This review will focus on the two recently approved fixed-ratio basal insulin/GLP-1 RA co-formulations: insulin glargine (iGlar) U-100/lixisenatide (iGlarLixi) and insulin degludec (iDeg) U-100/liraglutide (iDegLira).
Fixed-ratio basal insulin/GLP-1 RA co-formulations
iGlarLixi is a fixed-ratio co-formulation of a once-daily long-acting basal insulin, iGlar (100 units/ml) and a short-acting, once-daily GLP-1 RA, lixisenatide (33 μg/ml; Soliqua 100 units/33 μg) (Figure 1) indicated to improve glycemic control in adults with T2D inadequately controlled on basal insulin (<60 units daily) or lixisenatide. 12 iDegLira is a fixed-ratio co-formulation of a once-daily long-acting basal insulin, iDeg (100 units/mL) and a long-acting, once-daily GLP-1 RA, liraglutide (3.6 mg/ml; Xultophy 100 units/3.6 mg) indicated to improve glycemic control in adults with T2D inadequately controlled on basal insulin (<50 units daily) or liraglutide. 13 Both agents were approved by the Food and Drug Administration (FDA) in November 2016 and are available as single injections administered via disposable pen devices. Doses should be administered once daily (at the same time each day with or without food for iDegLira and within 1 h prior to the first meal of the day for iGlarLixi) and are titrated based on the basal insulin component.

Example of combination product labeling on pen injector device.
Pharmacokinetics and pharmacodynamics
Insulin degludec
iDeg is a basal insulin with an ultra-long duration of action developed for once-daily administration. The half-life of iDeg is >25 h in patients with T1D and T2D, and the drug reaches steady state within 3 days of administration.13,14 Upon subcutaneous injection, iDeg forms long, soluble multi-hexamer chains that result in a soluble depot in the subcutaneous tissue from which iDeg monomers gradually separate. 15 This results in a flat and stable pharmacokinetic and pharmacodynamic profile, allowing for reduced fluctuations in its glucose-lowering effect across one dosing interval. 16
Insulin glargine
iGlar is a long-acting basal insulin developed for once daily administration. It is indicated to improve glycemic control in adults and children with T1D and adults with T2D. 17 The half-life of iGlar is approximately 12 h in patients in patients with T1D. 18 IGlar was designed to have low aqueous solubility at neutral pH, but is completely soluble at pH 4 of its injection solution. The acidic solution become neutralized upon subcutaneous injection, leading to the formation of microprecipitates. This allows for slow release of small amounts of iGlar and a relatively constant pharmacokinetic and pharmacodynamic profile over 24 h with no pronounced peak. 17 This is also true when given as a combination product with lixisenatide.
Lixisenatide
Lixisenatide is a synthetic analogue of exendin-4, with about 50% amino acid sequence homology to human GLP-1, that acts as a selective GLP-1 receptor agonist. 19 Two clinical trials evaluating the pharmacokinetic effects of lixisenatide showed the mean half-life to be approximately 3 h when administered in doses ranging from 5 to 20 µg in patients with T2D taking oral antidiabetes agents. 20 Lixisenatide concentrations increased in a dose-dependent manner, reaching peak concentrations between 1 and 2 h. 20 Once-daily dosing of lixisenatide has been shown to be effective despite its relatively short half-life due to its high affinity for the GLP-1 receptor and inhibition of gastric emptying. 19 Increased doses of lixisenatide are also correlated with increasing area under the concentration curve (AUC). 20 When lixisenatide is administered in combination with iGlar, the Cmax is lower but the AUC is generally comparable with that when lixisenatide is administered alone. 12 Following subcutaneous administration of iGlarLixi, the median tmax of lixisenatide ranged from 2.5 to 3.0 h in patients with T2D. There was a 22–34% decrease in Cmax of lixisenatide compared with separate simultaneous administration of iGlar and lixisenatide, which is not likely to be clinically significant. 12 There are also no clinically relevant differences in rate of absorption when administered subcutaneously in the abdomen, thigh, or arm. In addition, the iGlarLixi ratio has no impact on the pharmacokinetics of lixisenatide when administered alone versus when given as Soliqua 100/33. 12
Liraglutide
Liraglutide is an incretin mimetic with 97% amino acid sequence homology to human GLP-1, that acts as a long-acting, selective GLP-1 agonist. 21 This results in a longer half-life of approximately 13 h and a protracted pharmacokinetic profile suitable for once-daily administration. 22 Following subcutaneous injection, liraglutide demonstrates a relatively slow rate of absorption with maximum concentrations being achieved in 8–12 h and absolute bioavailability of about 55%. 21 Liraglutide has a dose–response relationship with regards to Cmax and AUC, increasing proportionally over the therapeutic dose range of 0.6–1.8 mg. 21 Exposure to liraglutide concentrations are considered comparable upon subcutaneous administration in the abdomen, thigh, and arm. 21 The combination of liraglutide with iDeg (Xultophy®) shows similar pharmacokinetic and pharmacodynamic profiles compared with its individual parts. 13 No clinically significant differences have been reported.
Clinical data
iGlarLixi
One phase II study (LixiLan proof-of-concept) as well as two phase III studies (LixiLan-O and LixiLan-L) were conducted to evaluate the clinical safety and efficacy of the iGlar U-100/lixisenatide combination (iGlarLixi). Specific details regarding the trial methods and efficacy outcomes are found in Table 1. Specific adverse event rates across the trials are listed in Table 2.
Trial methods and efficacy outcomes for iGlarLixi and IDegLira.
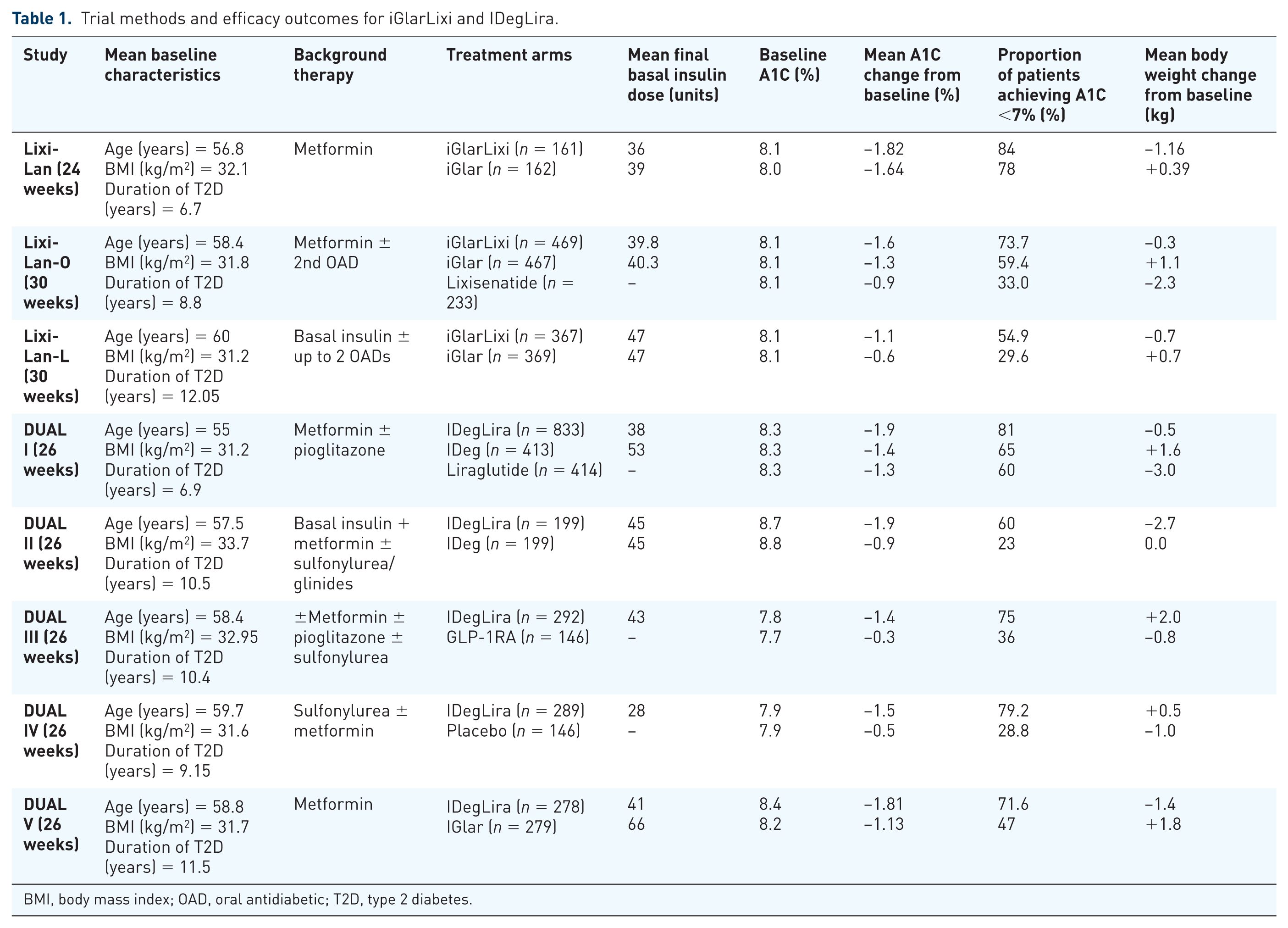
BMI, body mass index; OAD, oral antidiabetic; T2D, type 2 diabetes.
Specific adverse event rates seen across the clinical trials for iGlarLixi and IDegLira.

GLP-1RA, glucagon-like peptide-1 receptor agonists; NR, not reported.
The LixiLan proof-of-concept study compared the efficacy and safety of the combination iGlarLixi versus iGlar once daily in patients with T2D who were inadequately controlled on metformin alone. 23 A total of 323 subjects with an average A1C of 8.1%, average age of 57, and an average body mass index (BMI) of 32.1 kg/m2 were enrolled in this 24-week trial with a primary endpoint of change in A1C from baseline. Patients were initiated on iGlarLixi 10 units/5 μg or iGlar 10 units, administered subcutaneously within 1 h before breakfast and were titrated based on units of iGlar to achieve a target FPG of 80–100 mg/dl.
Patients taking iGlarLixi had significantly greater reductions in A1C compared with iGlar (−1.82% versus −1.64%, p = 0.01) and greater reductions in 2-hour PPG levels compared with iGlar (−70 mg/dl versus −12 mg/dl, p < 0.0001). Treatment with iGlarLixi was associated with weight loss compared with weight gain with iGlar and there were no significant differences in hypoglycemia between groups. Rates of nausea and vomiting were overall low, but higher in patients taking iGlarLixi compared with iGlar, but discontinuation rates due to GI AEs were low. The authors concluded that iGlarLixi demonstrated superior glycemic control with weight loss, no increased risk of hypoglycemia and a low incidence of nausea and vomiting compared to iGlar alone.
The LixiLan-O study compared iGlarLixi with iGlar and lixisenatide individually in insulin-naïve patients with T2D who were inadequately controlled after at least 3 months of treatment with metformin ± a second oral antidiabetic (OAD) agent. 24 A total of 1170 subjects with an average A1C of 8.1%, average age of 58, and an average BMI of 32 kg/m2 were enrolled in this 30-week trial with a primary endpoint of change in A1C from baseline. Patients on iGlar were initiated on 10 units once daily and titrated to a target FPG of 80–100 mg/dl with a maximum dose of 60 units/day. Patients on lixisenatide were initiated on 10 μg once daily for 2 weeks and then increased to 20 μg once daily. Patients on iGlarLixi were initiated on 10 units/5 μg once daily and titrated based on iGlar units to a target FPG of 80–100 mg/dl with a maximum dose of 60 units/20 μg, using two pens with different iGlar:lixisenatide dose ratios (2:1 and 3:1).
Patients taking iGlarLixi had significantly greater reductions in A1C compared with iGlar or lixisenatide alone (−1.6%, −1.3%, and −0.9% respectively, p < 0.0001 for both) and significantly more patients taking iGlarLixi achieved an A1C <7% compared with iGlar or lixisenatide alone (73.7%, 59.4%, 33%, p < 0.0001 for both). Mean body weight decreased with iGlarLixi and lixisenatide but increased with iGlar. The rates of hypoglycemia were similar between the iGlarLixi and iGlar groups, but lower in the lixisenatide group. Nausea, vomiting, and diarrhea were the most common side effects in the iGlariLixi group but occurred less frequently than in the lixisenatide group. Discontinuation rates due to GI AEs were low, but higher in the lixisenatide group compared with the iGlarLixi group.
The LixiLan-L study compared iGlarLixi with iGlar in patients with T2D inadequately controlled on basal insulin ± up to two OADs (metformin, sulfonylurea, glinide, SGLT-2 inhibitor, or DPP4 inhibitor). 25 During the 6-week run-in phase, metformin was continued, other OADs were discontinued, and patients on other basal insulins were transitioned to iGlar and all doses were optimized. A1C decreased during the run-in phase by 0.4%. Patients with A1C >7%, but FPG ⩽140 mg/dl, and iGlar dose ⩽50 units were randomized to iGlar once daily at any time of day and titrated to a maximum dose of 60 units once daily or iGlarLixi once daily within 1 h before breakfast. The iGlarLixi dose was based on the iGlar dose during the run-in phase. Patients taking ⩾30 units/day started with iGlarLixi 30 units/10 μg using a 3:1 pen; patients taking <30 units/day started with iGlarLixi 20 units/10 μg using a 2:1 pen. The dose was titrated based on iGlar units to a FPG target of 80–100 mg/dl.
Patients taking iGlarLixi had significantly greater reductions in A1C compared to patients taking iGlar (−1.1% versus −0.6%, p < 0.0001) and more patients taking iGlarLixi achieved an A1C <7% (54.9% versus 29.6%, p < 0.0001). Body weight decreased in the iGlarLixi group and increased in the iGlar group (−0.7 kg versus +0.7 kg, p < 0.0001) and hypoglycemia rates were similar between groups. The rates of GI AEs were low in both groups, but significantly more common in the iGlarLixi group compared with the iGlar group.
IDegLira
There were five phase III clinical trials conducted on the degludec/liraglutide combination (IDegLira), coined the DUAL™ (Dual Action of Liraglutide and iDeg) clinical trial programs. Specific details regarding these trials are found in Table 1. Specific adverse event rates across the trials are listed in Table 2. All of the DUAL trials utilized ‘dose steps’ terminology for the combination IDegLira, with each dose step containing 1 unit of IDeg and 0.036 mg of liraglutide.
DUAL I randomly assigned 1663 adult T2D subjects to IDegLira, IDeg or liraglutide on a 2:1:1 ratio. 26 The primary endpoint for the trial was change in hemoglobin A1C after 26 weeks, to assess noninferiority of IDegLira compared with iDeg [upper 95% confidence interval (CI) margin of 0.3%], and superiority of IDegLira compared with liraglutide (lower 95% CI margin of 0). Subjects had a mean age of 55, mean A1C of 8.3%, and a mean BMI of 31.2 kg/m2. For the IDegLira and IDeg groups, dosing started at 10 units of IDeg or 10 dose steps of IDegLira and was titrated upwards twice a week, with a prebreakfast mean glucose target of 72–90 mg/dl. Patients using liraglutide monotherapy started at 0.6 U and titrated up weekly to achieve the 1.8 mg dosing. IDegLira successfully demonstrated noninferiority to iDeg (estimated treatment difference −0.47%, 95% CI −0.58 to −0.36, p < 0.0001) and superiority to liraglutide (treatment difference −0.64%, 95% CI −0.75 to −0.53, p < 0.0001) after 26 weeks. Weight loss was highest in the liraglutide group (−3.0 kg), followed by the IDegLira group (−0.5 kg), with the IDeg group gaining weight (+1.6 kg). The authors noted similar rates of adverse events across the three groups, with the iDeg monotherapy group predictably having the lowest rates of GI side effects, and the liraglutide monotherapy having lowest rates of hypoglycemia. Of note, the IDegLira group reported lower rates of nausea compared with the liraglutide group (8.8% compared with 19.7%) and lower rates of hypoglycemia compared to the iDeg group (1.8 events per patient year compared with 2.6 events per patient year).
The DUAL II trial compared the efficacy of the combination IDegLira with iDeg alone in patients using basal insulin and metformin with or without a secretagogue. 27 A total of 413 subjects with an average A1C of 8.8%, average age of 57–58, and an average BMI of 33.7 kg/m2 were enrolled in this 26-week trial with a primary endpoint of change in A1C from baseline. Patients in both groups started with 16 units of IDeg or 16 dose steps of IDegLira. Titration occurred twice a week utilizing a predefined titration algorithm, with a prebreakfast mean glucose target range of 72–90 mg/dl. The IDegLira group demonstrated a statistically significant improvement in A1C compared with the iDeg group (A1C treatment difference of −1.1%, 95% CI −1.3 to −0.8, p < 0.0001). Rates of hypoglycemia were comparable between the groups, with 24% in the IDegLira group and 25% in the iDeg group. Nausea was reported as low in both groups, at 6.5% in the IDegLira group and 3.5% in the iDeg group, and the IDegLira group documented a 2.7 kg weight loss effect, compared with no weight change in the iDeg group (p < 0.0001). The authors concluded that IDegLira demonstrated superior glycemic control while maintaining a similar side-effect profile and providing the additional benefit of weight loss to subjects.
The third phase III trial with this combination, the DUAL III, studied the effects of IDegLira in T2D patients who were on maximum doses of GLP-1 therapy with concomitant oral diabetes therapies. 28 The primary outcome was change from baseline A1C intending to establish superiority of the combination IDegLira compared with maximum dose of GLP-1 therapy in patients with T2D. Patients’ mean age was 58, mean baseline A1C was 7.8% for IDegLira and 7.7% for the GLP-1 group, and mean BMI was 33 kg/m2. Similar to the DUAL II trial, initial dosing was 16 units or 16 dose steps, with a twice-weekly titration targeting a mean prebreakfast glycemic range of 72–90 mg/dl. After 26 weeks, the IDegLira group successfully demonstrated superiority, with an estimated A1C treatment difference of −0.94% (95% CI −1.11 to −0.78%, p < 0.001). The authors did note a weight loss difference that favored the unchanged GLP-1 group, with the estimated treatment difference of 2.89 kg (95% CI 2.17–3.62, p < 0.001). With regards to safety, hypoglycemia rates in the IDegLira group were 2.82 episodes per patient-year of exposure (PYE), compared with 0.12 episodes per PYE with the unchanged GLP-1 group. Nausea was documented as occurring in 3.1% of patients in the IDegLira group, compared with 4.1% of patients in the unchanged GLP-1 group. Two major adverse cardiovascular events (MACE) occurred during the 26 weeks, both confirmed to be a stroke, and both occurring in the IDegLira treatment group.
DUAL IV examined the effects of the new combination drug in patients using sulfonylureas as background therapy, with or without metformin. 29 Importantly, this study population was insulin-naïve. A total of 435 subjects were randomized in this 26-week trial to IDegLira or placebo in a 2:1 ratio, with the primary outcome of A1C change from baseline. The study population had an average A1C of 7.9%, an average age of 59–60 and an average BMI of 31–32 kg/m2. Patients started with 10 dose steps and titrated upward similar to previous trials, with a twice-weekly schedule targeting a mean fasting blood glucose of 72–108 mg/dl. This trial successfully established superiority of IDegLira compared with placebo, with an estimated treatment difference of 1.02% (95% CI −1.18 to −0.87, p < 0.001). With regards to adverse events, nausea was reported in 4.5% of the treatment group, compared with 3.4% of the placebo. Patients in the IDegLira group showed a mean weight gain of 0.5 kg, while patients in the placebo group had a mean weight loss of −1.0 kg, demonstrating a treatment difference of 1.48 kg (95% CI 0.90–2.06, p < 0.001). Hypoglycemia occurred at a rate of 41.7% of the treatment group and 17.1% with placebo. Of note, most of these hypoglycemic episodes were mild to moderate in nature, with only two episodes (0.7%) being reported as severe with the treatment group, and zero episodes in placebo.
The final phase III trial evaluating IDegLira was the DUAL V trial. This 26-week trial assessed the noninferiority of IDegLira compared with iGlar in T2D patients previously using iGlar and metformin. 30 The primary endpoint was change of A1C from baseline, with a noninferiority upper CI margin of 0.3%. A total of 557 patients enrolled in the trial with an average age of 58.8, average A1C of 8.4% in the IDegLira group and 8.2% in the iGlar group, and average BMI of 31.7 kg/m2. Patients using glargine alone continued on the dose they were utilizing prior to enrollment; patients in the IDegLira group discontinued their glargine and started IDegLira at 16 dose steps. Both groups utilized a twice-weekly titration algorithm based on a prebreakfast mean glucose target of 72–90 mg/dl. The IDegLira group had a maximum dose of 50 units of iDeg/1.8 mg of liraglutide; there was no maximum dose for the iGlar group. This trial established noninferiority and met criteria for statistical superiority with IDegLira, demonstrating an estimated treatment difference of −0.59% (95% CI −0.74 to −0.45%, p < 0.01). Patients in the IDegLira group had a mean weight loss of 1.4 kg, compared with mean weight gain in the iGlar group of +1.8 kg, with an estimated treatment difference of −3.20 kg (95% CI −3.77 to −2.64, p < 0.001). Nausea was reported at a higher rate with IDegLira (9.4% compared with 1.1%), although the authors noted that when evaluating nausea adverse events by week, only ⩽4% of the IDegLira patients reported this side effect in any given week interval. Hypoglycemia rates were reported as 2.23 per PYE in the IDegLira group, and 5.05 episodes per PYE in the iGlar group, with an estimated rate ratio between groups of 0.43 (95% CI 0.30–0.61, superiority, p < 0.001).
Dosing and administration
Both combination products recommend stopping both the basal insulin and GLP-1 agonist therapy prior to starting the combination. For iGlarLixi, the recommended starting dose is 15 units (15 U/5 μg) for patients previously using 30 units or less of basal insulin, and 30 units (30 U/10 μg) for patients using 30–60 units of basal insulin, administered subcutaneously once daily within an hour of the first meal. 12 The maximum dose is 60 units (60 U/20 μg). For IDegLira, the recommended starting dose is 16 units (16 U/0.58 mg) given subcutaneously once a day. The maximum dose for this product is 50 units (50 U/1.8 mg). 13 Both products have a suggested titration schedule based upon average glucose readings and established glycemic goals, with LixiLan suggesting changes of 2–4 units once weekly and IDegLira suggesting a 2 unit change every 3–4 days until glycemic targets are achieved. In both cases, the number listed in the device window correlates to the basal insulin units to be delivered.
Place in therapy
The benefits of combining a GLP-1 agonist with insulin therapy has been well documented, and is mentioned as one possibility by treatment guidelines for the management of hyperglycemia in T2D from the European Association for the Study of Diabetes (EASD)/ADA. 31 Within the stepwise therapy approach, patients whose blood glucose remain elevated despite OAD treatment often progress to injection therapy with treatment intensification. This can be challenging to initiate, and is often delayed due to perceived biases regarding injections and lack of resources to adequately train patients on administration. A combination, once-daily injection may help with this transition by providing an easy initiation to injection therapy that does not compromise the effectiveness of either agent. Of note, however, is the fact that the FDA approved both products for T2D patients who were inadequately controlled on either basal insulin or a GLP-1 agonist, suggesting patients should already be using injection therapy before utilizing these products. While hypoglycemia does occur with combination GLP-1/basal insulin treatment, studies suggest that the rates are comparable, if not slightly better, than rates seen with insulin therapy alone. Utilizing GLP-1 therapy in combination with basal insulin reduces the overall insulin requirement needed to adequately manage patients’ glycemia, likely leading to both less hypoglycemia episodes and less weight gain. Basal insulins have also been shown to pose much lower risk of hypoglycemia compared with patients using both basal and bolus insulin, so the use of these products could help familiarize patients with the process on injecting medications, and provide good A1C benefit, without the acute risk of hypoglycemia seen with basal/bolus regimens. The positive weight loss effects provided by GLP-1 agonists will also offset some of the weight gain traditionally seen with insulin therapy, as shown by the trials presented in this review. Patients titrate the dose in steps, usually by averaging morning glucose readings, to approach specified glycemic ranges. There were also lower rates of GI AEs reported with the combination therapies in clinical trials, possibly because this slow titration, which starts with very low concentrations of GLP-1 agonist (lower than the monotherapy titration), may help patients adjust to the medication better. Adherence is another consideration with the combination products; studies have shown that patients’ adherence to insulin therapy decreases as the number of daily injections increases.32,33 Delivering two medications with one daily injection may avoid nonadherence issues.
There are disadvantages to combination therapies delivered together. Patients who experience severe side effects with initiation of a new drug therapy are often strongly averse to using that product; in the case of combination products such as these, a bad initial reaction to the therapy could condition the patient to avoid both drug classes, which are among the best therapeutic tools for managing diabetes. There is also a risk of medication errors, as patients may forget to discontinue their previous treatment, which may be duplicated in the combination product. Particular care should be given to counseling patients about stopping any monotherapy duplicate prior to initiating treatment with the combination product (Figure 1). In addition, the pen devices show only the insulin units in the window, without reference to the GLP-1 dose, which could lead to confusion or dosing errors. Again, providing training and education to patients about the device is key for them to understand how these medications should be titrated and dosed. Another potential disadvantage to the combination products is that any increases to dosing affect both the GLP-1 component as well as the insulin, with no ability to vary either individual component. Providers who may want to continue to increase insulin while leaving the GLP-1 dose constant would not be able to do so. There is a maximum amount of insulin that can be delivered as well (60 units with the iGlarLixi, 50 units with IDegLira), so T2D patients with higher insulin resistance that require greater insulin doses would need individual products for therapy. Cost is always a consideration; depending on the health plan, specific GLP-1 agonists and specific insulin products may be preferred over these combination products. Choosing formulary products may help to save patients money, even if they have to give multiple injections instead of just one a day.
There are no trials directly comparing the two combination GLP-1/basal insulin products. Indirectly comparing the two, there are a few notable differences. Lixisenatide has different pharmacokinetics compared with liraglutide, and is considered to have greater effects on post-prandial blood glucose and less effects on fasting blood glucose. The clinical impact of this difference is debatable; the A1C reductions across the studies suggest similar effects of approximately 1% to >1.5% reduction with combination therapy. The data suggest that IDegLira may have overall slightly better impacts on A1C reduction across trials, but it should also be noted that the prespecified glycemic targets were also more aggressive in the DUAL trials, which could account for this difference. Comparing the DUAL V trial with the LixiLan-L, where both combination products were compared with the use of iGlar, both preparations established superiority over glargine therapy, with IDegLira showing an additional −0.59% A1C lowering, and iGlarLixi showing similar reductions of −0.50%. Notably, IDegLira did demonstrate statistically lower rates of hypoglycemia, whereas iGlarLixi demonstrated similar rates of hypoglycemia compared with iGlar treatment. This could be due to the second notable difference between products; the iDeg inclusion within IDegLira, which has been shown to be more predictable and cause less hypoglycemic events compared with iGlar. 34 Overall, however, it is difficult to draw any definitive conclusions on the efficacy between the products without a direct head-to-head comparison. Finally, it should be noted that recent data have demonstrated that patients with high cardiovascular risk may receive cardiovascular benefit with the use of liraglutide monotherapy. 35 Recognizing that these data cannot be extrapolated to the combination product, it is still encouraging to see macrovascular benefit with the GLP-1 component. Lixisenatide currently has not demonstrated similar cardiovascular benefit, either by itself or in combination.
Conclusion
The two new combination products, IDegLira and iGlarLixi, provide additional options for clinicians and patients that may help ameliorate some of the side effects seen with insulin therapy by itself, while still providing clinically robust A1C improvements. Providing a once-daily injectable option that contains two effective pharmacologic agents may help clinicians transition patients who need treatment intensification more easily. Providers will be limited in customizing doses of the individual components with these products, and there is a risk that a patient who is intolerant to the combination therapy may be averse to using either class of medication in the future.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Wesley Nuffer and Ashley Guesnier have no conflicts of interest to declare. Jennifer Trujillo has served as a consultant on the Sanofi ad board.