
Abstract
Objectives:
Diabetic neuropathy (DN) in the elderly is a common complication of diabetes that can negatively influence balance control. In this study, we aimed to evaluate the efficacy of balance training program on postural stability of diabetic patients.
Patients and methods:
In this randomized clinical trial, 34 elderly DN patients were divided into intervention (n = 17) and control (n = 17) groups. The experimental group underwent a balance training program using the Biodex Balance System (BBS) for 10 sessions. All subjects in both groups were assessed using timed ‘up and go’ (TUG) test, the Berg balance scale, and the fall risk and postural stability tests, at baseline and at the end of the study.
Results:
TUG (p = 0.01), fall risk index (p = 0.002), anterior/posterior index (p = 0.01), medial/lateral index (p = 0.04), overall stability index (p = 0.01) and Berg balance scale (p = 0.04) were significantly improved after the training in the intervention group, but had no significant differences in the control group. The changes in TUG (p < 0.001) and fall risk index (p < 0.001) in the intervention group were significantly higher than those in the control group.
Conclusion:
According to our results, balance training would improve postural stability and balance in elderly patients with DN.
Introduction
Diabetes mellitus is one of the most frequent chronic diseases, with an increase in the global prevalence [Javadzadeh et al. 2013]. Diabetic neuropathy (DN) is one of the most common and long-term complication of diabetes that worsens over time. DN is a complex and progressive disorder, characterized by symmetrical distal degeneration of peripheral nerves, leading to symptoms of pain and sensory loss [Boulton et al. 2005]. During normal standing, somatosensory inputs from the legs and feet contribute to postural stability [Wu and Chiang, 1997]. Postural instability and balance disorder are a common finding in DN due to decreased proprioception and increased reflex reaction time [Boucher et al. 1995; Lord et al. 1994; Said, 2007; Uccioli et al. 1994]. Balance problems are also caused by movement strategy impairment, biomechanical structural disorders and disorientation [Akbari et al. 2006]. People with DN have balance disorders even with open eyes and are vulnerable to falls [De Oliveira et al. 2008]. Reaction and recovery times from sudden postural changes are delayed in diabetic patients that comprise further risk factors for falls [Lee et al. 2013].
It seems that strategies to improve DN patients’ adjustment to postural changes could reduce postural instability and fall risk. There are various reports about intervention programs including balance training to improve stability in this population [Allet et al. 2010; Mattacola and Lloyd, 1997; Morrison et al. 2010; Speers et al. 2002; Tsang et al. 2007]. Training with regard to sensory, ankle and hip strategies by exposing the patients to external perturbations with small movements of sway will improve balance and postural control in DN [Horak, 2006; Salsabili et al. 2011].
The Biodex Balance System (BBS) has been used as an assessment tool in a range of different populations; but it has recently gained attention in balance training. It is a relatively new instrument and there is only a limited amount of published data regarding its use. BBS has been recommended as an effective tool for balance and postural stability training in different neurologic diseases. Our group evaluated the efficacy of training with BBS on balance of multiple sclerosis patients and observed that BBS is safe and could improve the balance ability of the patients with multiple sclerosis [Eftekhar-Sadat et al. 2015]. The beneficiary effects of training with BBS on postural stability are also reported in patients with DN [Akbari et al. 2012].
There is a possible role for postural training with BBS in improving the balance and stability of DN patients. In this study we aim to evaluate the efficacy of balance training with BBS on DN patients’ balance and postural stability.
Methods
In this randomized clinical trial, we recruited 112 patients with diabetes mellitus and peripheral neuropathy over 6 months referred to physical medicine and rehabilitation clinics in Tabriz, Iran, by an endocrinologist for neuropathy evaluation and electrodiagnostic studies. Diabetes type 2 patients between 50–70 years old with moderate or severe DN on the Toronto scale [Perkins and Bril, 2003] with confirmed peripheral neuropathy by electrodiagnostic tests, ability to stand and walk independently, and body mass index (BMI) <30 were included. Exclusion criteria were diabetic ulcer, infection or partial amputation in feet, neurologic or orthopedic problem or severe pain affecting balance, history of repeated ankle sprains in the year prior to the study, and visual problems leading to an inability to see the stabilometer cursor, and chronic medical problems (other than diabetes) that limited participation. We excluded 68 patients due to inclusion and exclusion criteria (Figure 1).
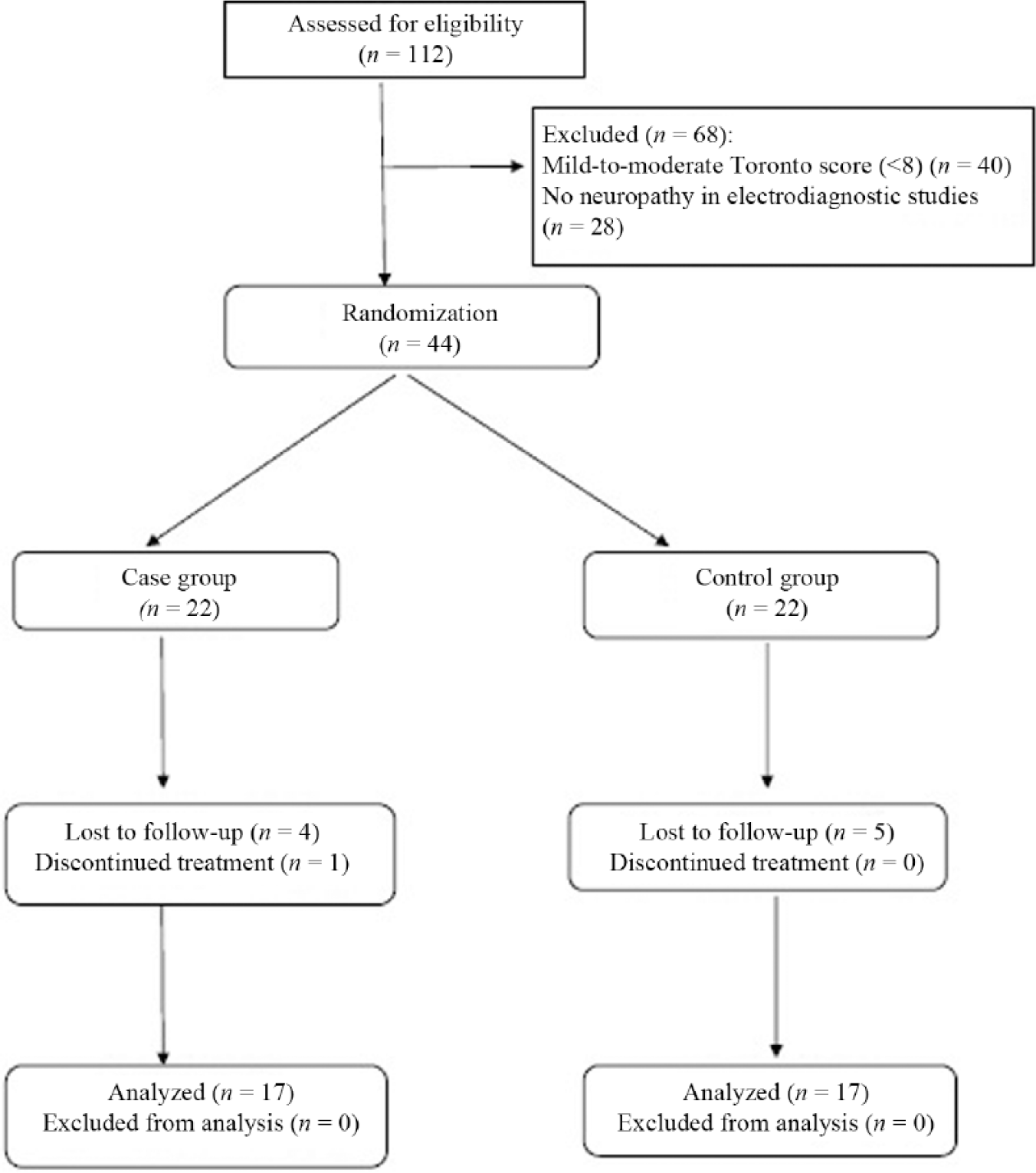
Randomization chart.
Patients were randomly assigned to experimental (n = 22) and control (n = 22) groups using an online randomization website (www.randomization.com). Five patients from the control group and four patients from the experimental group were lost to follow up and one patient from experimental group discontinued treatment for personal issues; none of the patients were excluded or left the study for the causes related to the study protocol. The final evaluation was performed with 17 patients in each group. Before testing, all subjects signed an informed consent form approved by the university institutional review board. Personnel performing the measurements and evaluating outcome were blinded to groups’ identities.
The trial is powered to detect an effect size of d ⩾0.70 as statistically significant in a two-tailed test with α = 0.05 and power of 0.95 with N = 16 per condition. As there was the possibility that some patients would not complete the study, we included 22 patients in each group.
Baseline findings including descriptive information such as age, sex, BMI, Toronto score, diabetic history and medication were recorded. In addition, the BBS score, timed up and go (TUG) test and Berg balance scale were measured before and after training by a researcher blinded to the training.
Patients in the control group received physiotherapy with infrared and transcutaneous electrical nerve stimulation (TENS) modalities for 30 minutes, 3 times a week for 10 sessions. The experimental group received physiotherapy similar to the control group as well as postural stability training with the Biodex® Balance System (Biodex 945-302, Biodex Medical Systems Inc., Shirley, New York) for 10 sessions. Postural stability training simulates specific movement patterns or strategies by placing markers on specific locations on the screen grid. This training program is commercially available. In each session, the subjects attempted to touch targets nine times using an onscreen cursor maneuvered by the subjects’ legs on the device’s platform. The platform stability was set to 6 (moderately stable). A trainer blinded to the evaluated measurements performed all the BBS sessions and supervised the physiotherapy sessions.
The BBS is used to measure a subject’s ability to maintain balance while doing functional tasks. It assesses the static and dynamic balances by using usual tasks such as reach, standing position and transferences. The test includes 14 items that are common in everyday life. Each item of the BBS is rated on a five-point scale. For the fall risk test, subjects were tested on the BBS using the fall risk test protocol in order to evaluate the efficacy of the balance training intervention. In the fall risk test, the platform is unstable and subjects’ sway is used to calculate the fall risk index. According to the standard software configuration, 2 trials of 20 seconds each at a stability level of 8 were calculated with 10 seconds rest between trials. Fluctuations around the zero point, established prior to testing when the platform is stable, are presented as the findings of this test. For the Postural Stability test, 3 20-second trials were conducted with one minute intervals between them. The platform is fixed and subjects’ sway is used to calculate the overall stability index (OSI). The BBS software sampled the deviations in the anterior–posterior (AP) and medial–lateral (ML) directions at a rate of 20 Hz and calculated the AP index (API), ML index (MLI) and OSI during a given task. These indices were calculated using the degree of oscillation of the platform, in which low values indicated that the individual had good stability. For each mode, the average of three tests was considered the subject index.
The Berg balance scale [Berg et al. 1992] assesses static and dynamic balance abilities with excellent test–retest reliability for patients with multiple sclerosis. It consists of 14 items of increasing difficulty which are scored on a five-point Likert scale (0–4). The maximum possible score is 56 and lower scores indicate more impaired balance.
We also evaluated TUG before and after training in both groups. Patients were asked to perform the TUG at their self-selected habitual walking speed. Before testing, a trained evaluator provided standardized verbal instructions regarding the test procedures. For this test, patients were seated and instructed to walk 3 meters, turn around, walk back to the chair and sit down. The stopwatch would be started on the command ‘ready, set, go’ and stopped as the participant sits down. The average of three tests was considered the mean TUG.
Statistical analysis
All statistical tests were performed using SPSS for windows Version 17 (Chicago, IL, USA). Quantitative data were presented as mean (interquartile range), while qualitative data were demonstrated as frequency and percentage (%). The Mann–Whitney U test for quantitative data and chi-squared test or Fisher’s exact test, as appropriate for qualitative data, were used to compare data between groups of patients. A paired samples t-test was used to compare findings before and after training in each group. A p value of <0.05 was considered statistically significant.
Results
A total of 34 patients with DN including 22 females and 12 males with mean age of 58.94 ± 6.97 years were included in experimental (n = 17) and control (n = 17) groups. Table 1 shows baseline findings for both groups. There were no significant differences between groups.
Baseline findings for both groups.
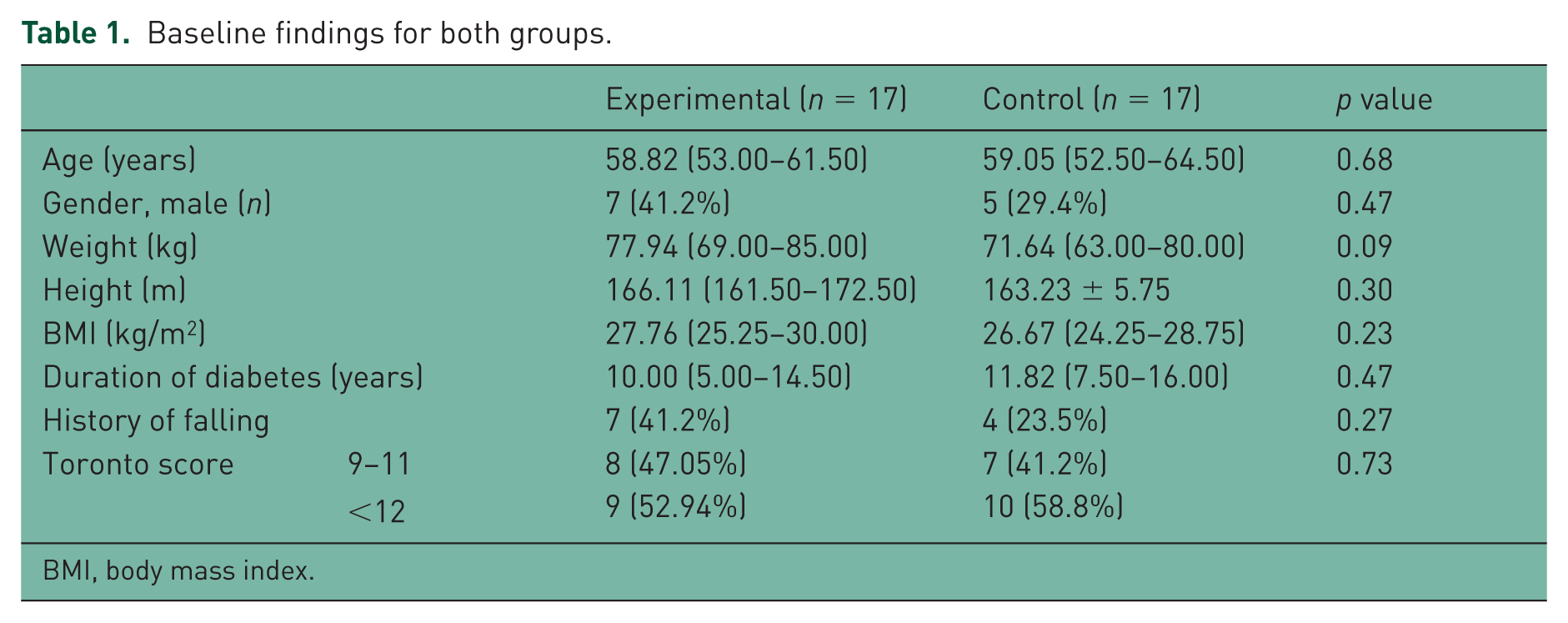
BMI, body mass index.
The Berg balance scale, BBS and TUG results before and after the training are shown in Table 2. There was no significant difference between groups before the training; however, compared with the control group, fall risk (p < 0.001), API (p = 0.01) and OSI (p = 0.003) were significantly lower after training in the experimental group. Comparing the results before and after the training in each group, we observed no significant differences in the control group. However, in the experimental group, TUG (p = 0.01), fall risk (p = 0.002), API (p = 0.01), MLI (p = 0.04) and OSI (p = 0.01) was significantly reduced and the Berg balance scale (p = 0.04) was significantly increased after the training.
Berg balance scale, timed up and go, and Biodex balance system results before and after training.

p is two-sided significant.
API, anterior–posterior index; MLI, medial–lateral index; OSI, overall stability index; TUG, timed up and go.
For better evaluation of the findings between groups and to assess the possible effects of BBS on postural stability, changes in scores in all outcomes during study period were calculated (Table 3). Significant reductions in TUG and fall risk index were observed in the experimental group compared with the control group. The experimental group had also higher changes in Berg balance scale, API, MLI and OSI, but the difference was not significant.
Changes (in percentages) in the Berg balance scale, timed up and go, and Biodex Balance System results during balance training.
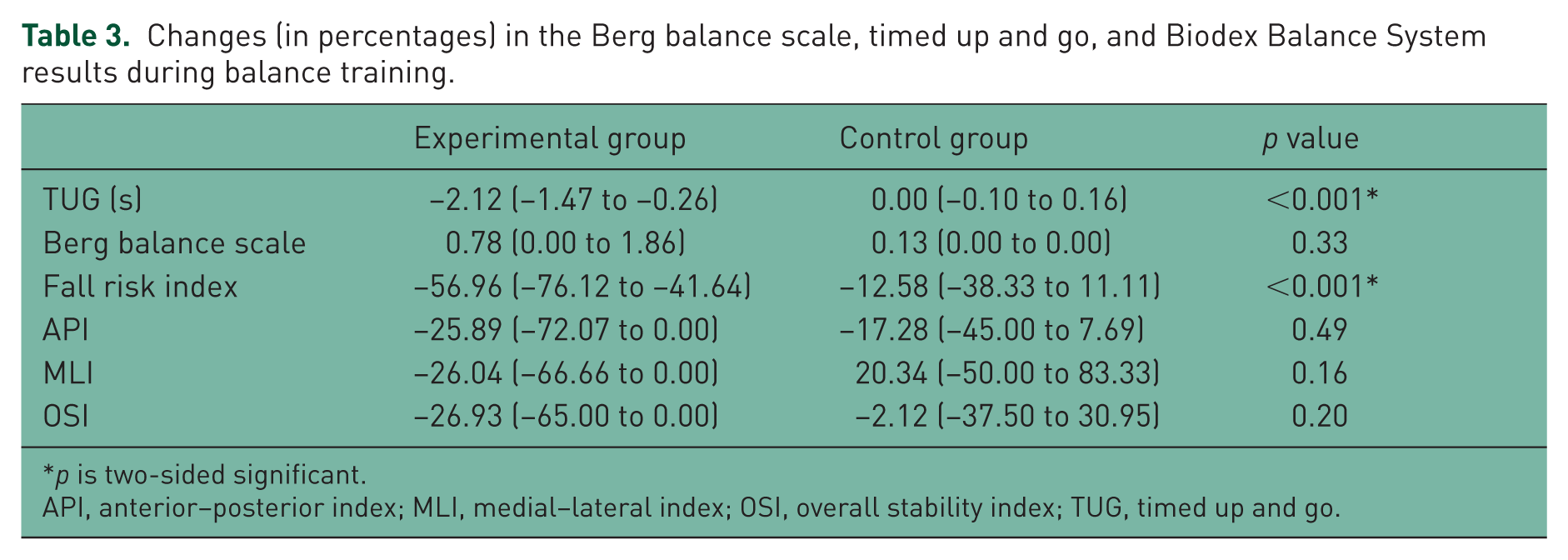
p is two-sided significant.
API, anterior–posterior index; MLI, medial–lateral index; OSI, overall stability index; TUG, timed up and go.
Discussion
In this study we evaluated the effects of 10 session balance training on diabetic patients with moderate to severe neuropathy. We designed the study to compare the differences in balance and postural control in DN patients between experimental and control groups after balance training with BBS. We also measured changes in the TUG test and Berg balance scale to better understand the changes after balance training and to reduce the possible instrument related effects on stability results. We observed that, in the experimental group, patients’ balance control and risk of fall was significantly improved after the training which had no difference in the control group. BBS, TUG and Berg balance scale indices were all significantly improved after the treatment in patients receiving balance training with BBS. Bulat and colleagues observed that a balance training class was safe and effective in improving balance outcomes in a cohort of elderly veterans at risk for falls with significant increase in berg balance score [Bulat et al. 2007].
The usefulness of balance training with BBS in improving postural stability and balance is well-demonstrated in previous studies in elderly people, especially those with neuropathy, diabetes and DN [Akbari et al. 2006, 2012; Salsabili et al. 2011]. Similarly, Morrison and colleagues showed that, following training, the diabetic group exhibited a significant decline in falls risk [Morrison et al. 2010]. This improvement was due to the improved proprioception and muscle strength. Salsabili and colleagues observed better balance performance after balance training in patients with DN which was independent of the severity of the neuropathy [Salsabili et al. 2011]. All variables of BBS were significantly improved. Allet and colleagues found that patients in the intervention group increased gait velocity, balance, muscle strength and joint mobility, and decreased their fear of falling [Allet et al. 2010].
This study in some respect was similar to the study by Akbari and colleagues which evaluated 10 patients with DN and 10 normal well-matched control groups [Akbari et al. 2012]. In their study, patients received balance training with BBS for 10 sessions, and improved OSI and API after training was similarly observed in their experimental group. Similar results were observed in our study. Unlike in the study by Akbari and colleagues, our control group consisted of patients with DN; to prevent the possible learning effects in experimental group, we also measured TUG and Berg balance scale which also showed significant improvement in the experimental group. We also measured the changes in outcomes and observed significant differences in TUG and risk of fall changes in the experimental group compared with the control group, which also demonstrates the efficacy of the training with BBS.
Laughton and colleagues reported greater amounts of sway in the AP direction and greater muscle activity during quiet standing in the elderly compared with young subjects [Laughton et al. 2003] and Lim and colleagues observed that older subjects have low directional control and low on-axis velocity in front–back rhythmic weight shift than right–left [Lim et al. 2003]. We observed that, after treatment, API and OSI in the experimental group were significantly lower than the control group, but was not significant for MLI. This could be attributed to the fact that OSI and API are correlated to neuropathy in lower limbs [Aly et al. 2008] and the role of AP stability is more evident in overall stability [Arnold and Schmitz, 1998]. It is presumed that AP stability is more related to the activation of ankle and plantar foot muscles. These muscles are more prone to be affected by DN than proximal body muscles [Akbari et al. 2006], while the abductor and adductor muscles of hip control the ML movement and stability, and are less affected [Nashner and McCollum, 1985].
Increasing age, previous falls history, increased postural sway, and presence of diabetes and peripheral neuropathy are major risk factors for falling and postural instability [Close et al. 2005; Maurer et al. 2005; Richardson and Hurvitz, 1995; Schwartz et al. 2002, 2008]. It is also shown that peripheral neuropathy in different neurologic disease and in older adults with diabetes mellitus often results in mobility-related dysfunction and balance impairments [Ayromlou et al. 2013; Bonnet et al. 2009; Emam et al. 2009; Goldberg et al. 2008]. Elderly diabetic people demonstrated an inferior performance in TUG, showing a reduction of mobility and an increased risk of falls compared with a group of elderly without diabetes [Alvarenga et al. 2010]. However, there were differences in TUG test among studies on diabetic patients [Alvarenga et al. 2010; Cordeiro et al. 2009]. Cordeiro and colleagues reported the mean TUG rest of 15.7 ± 6.5 seconds [Cordeiro et al. 2009], which is higher than the values in our study. The heterogeneous results are suggestive of the effect of other factors on postural stability. Fulk and colleagues found that neuropathy might not be the only cause of impaired balance in people with diabetes mellitus and that diabetes itself might negatively impact the postural control system [Fulk et al. 2010].
Due to the variable findings about factors affecting postural stability in diabetic patients, it seems the balance is multifactorial and it is hard to define a matched experimental and control group to evaluate the effects of training with the BBS. Considering the improvement in the Berg balance scale, TUG and BBS indices after training with no complications and trauma during sessions, it could be concluded that balance training with BBS has beneficiary effects in improving DN related postural instability.
It is not surprising that the experimental group scored better than control group in terms of measures assessed by BBS system, simply because one group practiced this particular task while the other did not. To reduce the risk of bias and avoid learning effect, the first test for all patients was performed for familiarity. However, we also measured TUG and Berg balance scale to better evaluate the BBS effects. As mentioned above, the changes in TUG and risk of fall measured by BBS were significantly better in the experimental group, which is also indicative of the efficacy of the BBS for balance training.
This study has some powers and limitations; we included only those patients with moderate-to-severe Toronto score and confirmed neuropathy with electrodiagnostic studies, which allowed a better evaluation of the effects on DN patients with lower bias on the results. Because of the inclusion criteria and the need to have both the above mentioned criteria, we studied a small group of DN patients which is also a limitation of the study. Having experimental and control groups also helped with better comparison of the therapeutic results. However, the results should be interpreted cautiously as the patients had severe scores and the sample size was small for a randomized clinical trial.
Conclusion
Balance training with BBS improved TUG, Berg balance scale and BBS indices, especially the risk of falling significantly in the experimental group, and could be used as a useful device in treating DN patients with postural instability and risk of falling.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported financially by the Physical Medicine and Rehabilitation Research Center, Tabriz University of Medical Sciences, Tabriz, Iran.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.