
Abstract
Scars caused by skin injuries after burns, wounds, abrasions and operations have serious physical and psychological effects on patients. In recent years, the research of scar free wound repair has been greatly expanded. However, understanding the complex mechanisms of wound healing, in which various cells, cytokines and mechanical force interact, is critical to developing a treatment that can achieve scarless wound healing. Therefore, this paper reviews the types of wounds, the mechanism of scar formation in the healing process, and the current research progress on the dual consideration of wound healing and scar prevention, and some strategies for the treatment of scar free wound repair.
Introduction
Skin, as the first barrier against external invasion, is the largest organ of the human body, which has many important functions, such as preventing the invasion of pathogens, preventing mechanical forces and infection, and preventing thermal dysregulation, and so on. 1 Meanwhile, skin is also an active immune organ, which carries the innate immune system of cellular elements and the adaptive immune system. 2 However, skin injury cannot be avoided in daily life, and the repair of the skin is an extremely complex process. 3 The healing of skin wounds requires the cooperation of multiple cells from different lineages, as well as the careful coordination of multiple cytokines and signaling pathways in the wound site. 4 Without interference from the external environment, wound healing will be carried out in a highly orderly manner according to certain biological processes, which generally includes four independent but overlapping stages of hemostasis, inflammation, proliferation, and remodeling. 5 The ideal healing of skin wounds is regeneration while seriously damaged skin tissue is repair, it forms scar tissue, which looks thicker and tougher than normal skin, but is actually not as functional as normal skin. Because the essence of scar is an abnormal tissue without normal skin tissue structure and physiological function, which has lost the tissue vitality of normal skin. 6 Cell fibrosis and excessive deposition of disordered ECM dominated by collagen lead to the formation of scar. 7 Although large scar or covering on joint surface can cause great harm, the formation of scar is not uncontrollable. The fetal skin starts to leave scar in the late pregnancy, which indicates that human skin has the ability to regenerate at least to a certain extent. 8 However, there is a lack of review on the mechanism of skin scar formation and the methods to prevent or reduce scar formation. In this review, we introduced the types of skin wounds, the mechanism of scar formation in the healing process, and the current strategies to avoid or reduce scar formation.
Type of skin wounds
There are various etiologies of skin injury, which can be caused by not only external factors such as burns, surgery and trauma, but also by internal factors, such as local blood supply disturbances. 9 Tissue injury can trigger a series of physiological reactions. If these reactions are coordinated and can continuously promote wound repair. On the contrary, if the normal wound healing process is interrupted for some reason, leading to wound infection, or the wound cannot be healed due to some potential disease (Figure 1). 10 It is usually divided into acute wound (<4 weeks) and chronic wound (⩾4 weeks) according to the healing time of wound. Acute wounds are associated with external injuries to intact skin, including surgical trauma, bites, burns, minor scratches, and abrasions. On the other hand, chronic wounds are usually caused by large and deep burns or surgical trauma, by the impact of biofilms, or by endogenous causes which eventually damage the integrity of dermal and epidermal tissues.11,12 Skin damage has gradually evolved into a clinical problem, seriously affecting people’s bodies and psychology, and causing huge economic losses. 3
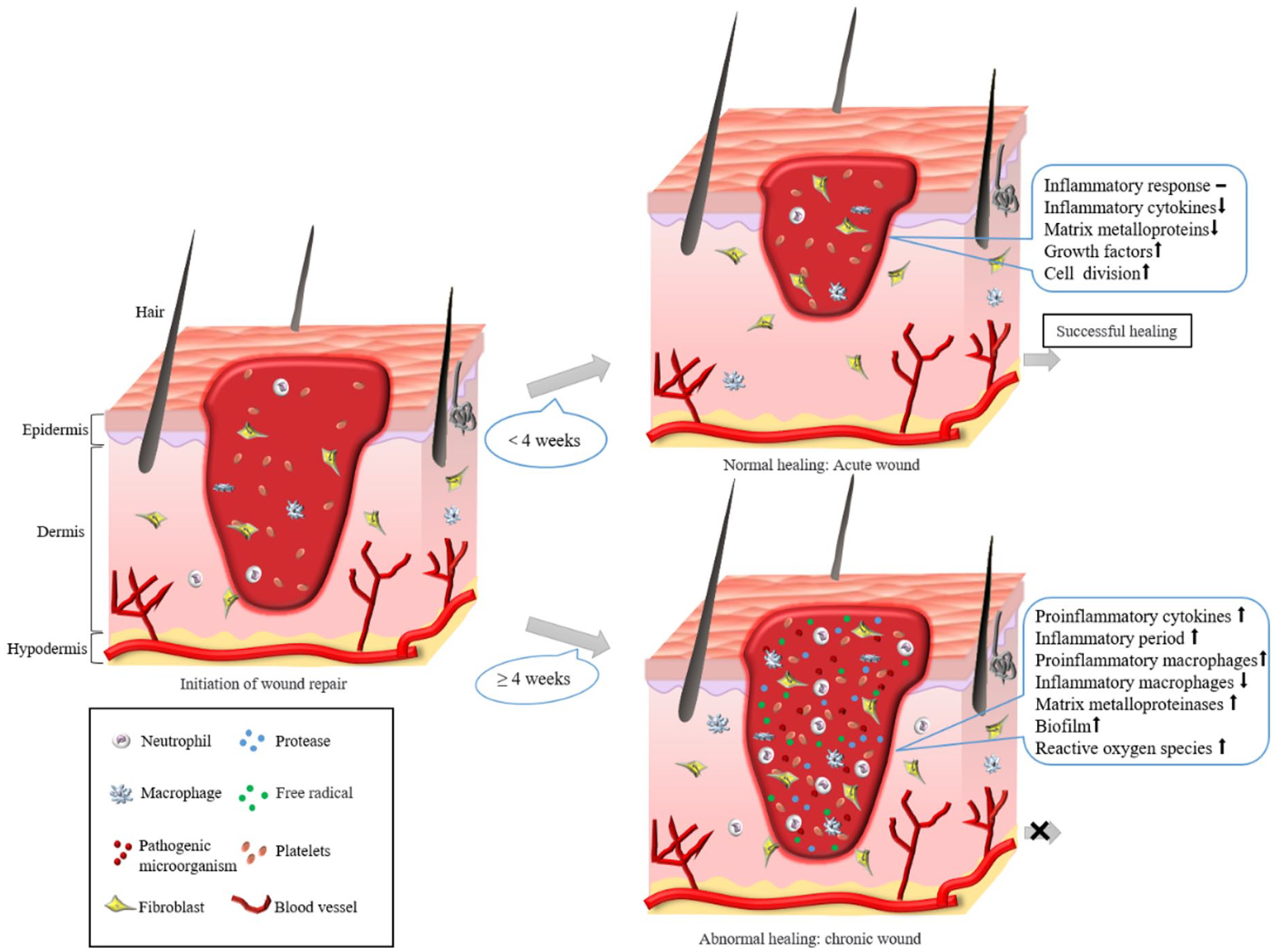
Schematic diagram of acute and chronic wound healing.
The formation mechanism of acute wounds
Acute wound usually refers to the wound formed suddenly in the process of injury repair such as surgical incision, burn and scald wound, superficial skin wound and wound caused by tear. 13 Most acute wounds with small wounds only need to be cleaned around the wound and treated briefly, they can be quickly healed according to the normal healing steps. Acute wound has no underlying cause, so there are normal inflammatory response, less inflammatory cytokines and matrix metalloproteins (MMP), higher concentration of growth factors, faster cell division, and shorter healing time. 14 The first thing is to stop bleeding when the skin suffers from acute injury, so as to prevent excessive blood loss. The inflammatory response is then induced by the inflammatory cells (such as neutrophils and macrophages) that are recruited into the wound to eliminate pathogens and clear the wound. 15 Subsequently, macrophages engulf neutrophils, induce proinflammatory macrophages (M1) to transform into anti-inflammatory macrophages (M2), alleviate inflammatory reaction, and induce wound healing to enter the proliferation phase. 16 Finally, after a series of molecular events, the acute wound healed rapidly in a relatively short time, and finally recovered the tissue integrity. 17 However, for some deep wounds (such as large burns, deep lacerations, and destructive wounds) that are beyond the ability to heal themselves, professional doctors are required to cut and suture under local anesthesia to avoid infection and speed up the healing of the wound. 18 Notably, the tough, recyclable, degradable elastomer material holds promise for use as surgical sutures. 19 In addition, oral wounds usually heal quickly within a relatively short period of time. Because oral mucosal tissue has a strong regenerative and repair capacity, and epithelial cells can rapidly proliferate and differentiate to promote wound healing. The moist microenvironment in the mouth is conducive to cell regeneration and tissue repair on the wound surface, and saliva in the oral cavity contains various substances such as enzymes and immunoglobulins that can inhibit the proliferation of microorganisms at the wound, helping to maintain a clean environment for oral wound healing. However, exposed skin wounds are more susceptible to dryness, infection, and other factors, which affect the speed of wound healing. 20
The formation mechanism of chronic wounds
Physiological factors can help wound heal quickly in the process of wound healing, but these complex factors are easy to change, leading to chronic wound. 21 Depending on the etiology, nearly all chronic wounds can be classified as pressure ulcers, diabetic ulcers, and vascular ulcers (e.g. arterial and venous ulcers). 22 First of all, pressure ulcers are usually caused by the long-term compression of the injured part, the inability of blood to reach the wound, and malnutrition, leading to skin necrosis and ulceration, thus losing normal function. 23 Secondly, diabetes ulcers mainly occur in diabetes patients. Many complications of diabetes hinder wound healing, including endothelial dysfunction, increased inflammation, and peripheral neuropathy. 24 Finally, venous ulcer is caused by the impairment of the function of venous valve, which leads to the obstruction of blood return. In severe cases, it causes venous hypertension, and then leads to chronic inflammation through a series of processes. On the contrary, arterial ulcer is tissue ischemia and injury caused by blockage of blood flow to limbs. 25
Although the etiology varies, the common features of all chronic wounds possess a persistent and intense inflammatory environment. 26 High levels of pro-inflammatory factors (such as IL-6, IL-1β, and TNF-α) are present in chronic wounds for a long time, leading to the growth of the inflammatory phase of wound healing. It is worth noting that in chronic wounds, there are too many M1 macrophages, which persist but do not transform into M2 macrophages. Therefore, these macrophages secrete a large number of matrix metalloproteinases (MMPs), degrade proteins and destroy the temporarily formed ECM, preventing wound healing from entering the proliferation phase.27,28 During normal wound healing, macrophages engulf dead neutrophils, a behavior that promotes the transformation of macrophages convert to anti-inflammatory cells to alleviate inflammation. 16 However, in chronic wounds, the ability of macrophages to engulf dead neutrophils is reduced, which leads to ineffective relief of severe inflammatory environment. For another, chronic wounds are vulnerable to bacterial infection. In most cases, although bacteria exist, the wound will still heal normally, but in some cases, bacteria will prevent the wound from healing. 29 The bacteria that infect wounds are mainly Staphylococcus aureus, Escherichia coli, and Hemolytic streptococcus, etc. Because they can secrete high glycosylated matrix and form biofilm with bacteria, which can reduce the expression activity of type I collagen in wounds, leading to damage of granulation tissue. Moreover, persistent wound infection will reduce the level of growth factor and degrade fibrin, and will also aggravate inflammation, eventually leading to failure of wound healing and becoming a chronic wound. 30 At the same time, the effect of biofilm on chronic wound infection is unquestionable. Chronic wounds provide an ideal habitat for the formation of biofilm. Biofilms are microorganisms growing on biological and abiotic surfaces, mainly fixed communities of bacteria which can easily attach to the wound fragments and infect the wound due to impaired host immune response. These microbes are embedded in an extracellular polymer to provide enhanced protection against antimicrobial agents. 31 As chronic wounds arrest in the inflammatory stage for a long time, resulting in an increase in reactive oxygen species (ROS) production, ROS can exacerbate tissue injury by promoting leukocyte adhesion and proinflammatory factors, while also inhibiting keratinocytes and keratinocyte migration and epithelialization. Higher levels of ROS can also destroy newly synthesized granulation tissue and prevent the accumulation of ECM leading to non-healing chronic wounds. 32 In addition, there are other factors that can also cause a wound to evolve into a chronic wound, for example, aging-related factors can hinder the normal healing of wounds with age, including impaired cellular responses to stress, some underlying biochemical reactions, and so on. Cells in the elderly have a high degree of senescence, and the ability of wound cells to respond is reduced, so this group of people is at higher risk for chronic wounds. Older people have a high degree of cell aging and a reduced ability to respond to wound cells, so these people have a higher risk of developing chronic wounds. 33 It is worth noting that, malnutrition with low protein content can also hinder normal healing, resulting in chronic wounds. 34
The healing of skin wounds and scar formation
The ideal healing of skin wounds is regeneration rather than repair. Skin injury repair refers to the process of blood clotting and recovery immediately after injury. In this process, local cell repositioning and collagen precipitation occur, so as to restore the damaged tissue. However, scar is usually produced instead of re-establishing the normal tissue structure. 35 Skin injury regeneration means that when the tissue is damaged only by the epidermis or superficial dermis, it can produce the same structure as the original tissue, and some epidermal appendages will also form. The new skin will be the same as the original skin, without causing scars. However, if the skin injury is too serious, it will inevitably form a large number of fibrous tissues covering in the process of repair, resulting in the formation of scars, thus causing the skin to lose its integrity and beauty. 36 Wound healing is a dynamic and complex process involving a large number of cells and cytokines, and each cell cooperates and communicates closely with each other to achieve rapid and effective repair of damaged tissue. 37 However, pathological wound healing occurs if the disorder occurs in the wound healing process. 38 The normal formation or overgrowth of scar during wound healing and the possible causes are summarized, as shown in Figure 2.
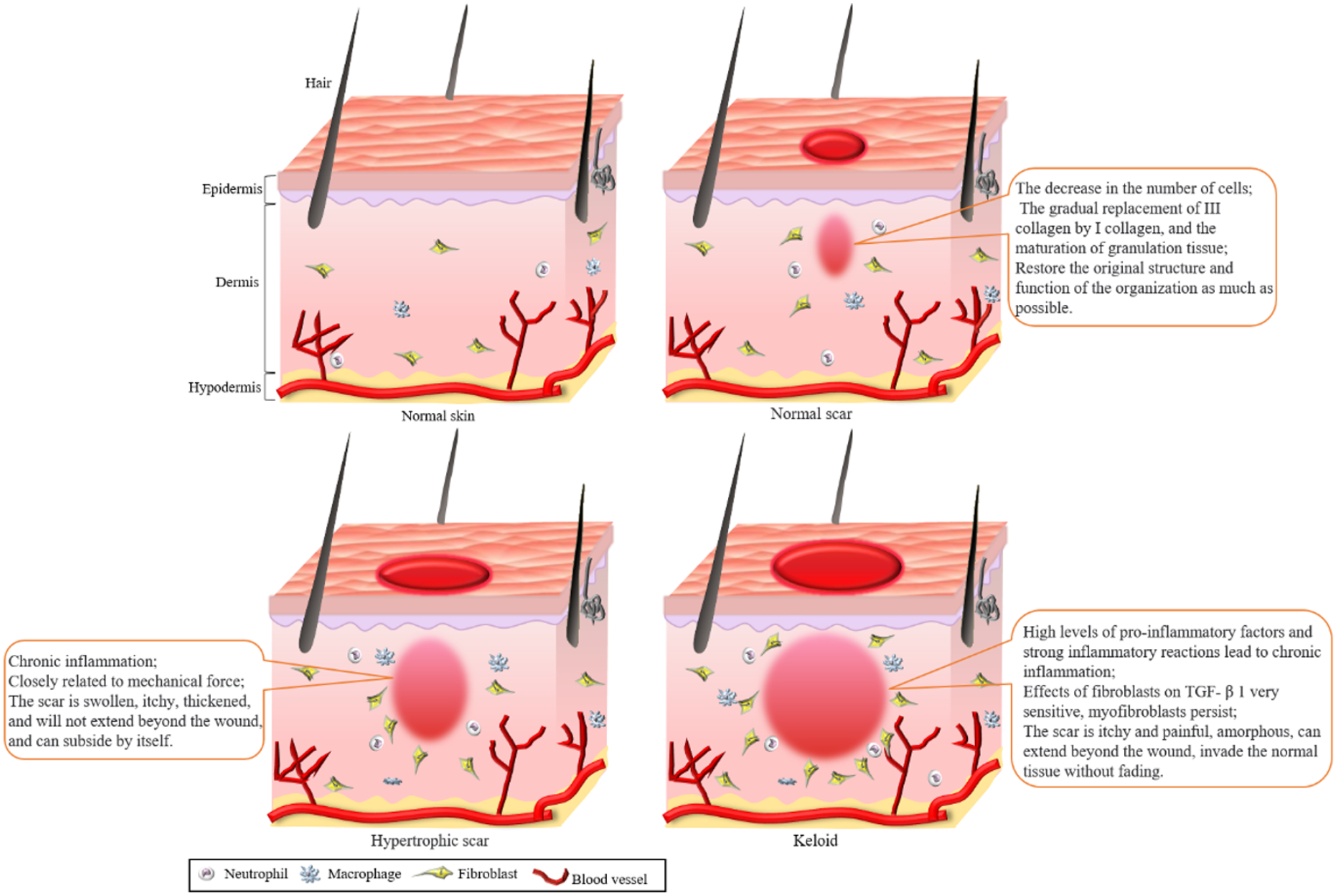
Different scars formed by wound healing under physiological or pathological conditions.
Scar formation during wound healing under physiological conditions
When the skin is injured, the damaged blood vessels constrict rapidly to reduce blood flow, forming blood clots through the rapid aggregation of platelets and the formation of fibrin clots to prevent the damaged vessels from continuing to bleed. 39 In addition, when fibrin clot is involved in hemostasis, it can not only serve as a temporary ECM to provide a platform for cell migration, but also release biologically active factors to attract inflammatory cells, such as platelet-derived growth factor (PDGF), epidermal growth factor (EGF), fibroblast growth factor-2, interleukin-8, and transforming growth factor-β (TGF-β). 40 Inflammation is caused by inflammatory cells recruited to the wound, such as monocytes and neutrophils, which clear foreign bodies, damaged endogenous tissues, and bacterias. 41 Moreover, monocytes can differentiate into macrophages under the action of local cytokines. Mature macrophages continue the clearance process, engulfing microorganisms, apoptotic cells, and tissue debris. Macrophages that have antibacterial effects during the inflammatory phase are considered M1-type macrophages.42,43 However, most M1 macrophages undergo apoptosis after removing tissue fragments and pathogens, and a few are transformed into M2 macrophages under the effect of cytokines. M2 macrophages are responsible for the transition from the wound healing process to the proliferation phase. They promote the transition of wound healing from the inflammatory phase to the proliferation phase by releasing vascular endothelial growth factor (VEGF), PDGF, and TGF-β. 44 After the inflammatory phase, wound healing enters a proliferative phase, in which multiple activities are involved, including re-epithelialization, neovascularization, and synthesis of granulation tissue. 45 Re-epithelialization mainly refers to the migration, proliferation and differentiation of keratinocytes, so as to form epidermal tissue with certain protective ability to prevent further wound damage. Under the action of cytokines and vascular growth factors, endothelial cells begin to divide and proliferate, migrate to areas without or with fewer blood vessels, and gradually form capillary buds. 46 Because of capillaries, blood can flow into the wound to provide sufficient oxygen and nutrition for the repair of injury. In the meantime, fibroblasts migrate to the wound and release a large amount of ECM which mainly composed of collagen, fibronectin, glycosaminoglycan, proteoglycan and hyaluronic acid (HA) to form granulation tissue and replace damaged tissue. 47 In addition, fibroblasts can also be transformed into myofibroblast that secretions α- Smooth muscle actin (α-SMA) to promote wound contraction. Finally, the wound healing enters the remodeling stage, which is also the longest stage, lasting for weeks, months, or even years. 48 The main characteristics of this stage are gradual apoptosis of related cells, gradual replacement of type III collagen by type I collagen, and maturation of granulation tissue. 49 Through remodeling, the structure and strength of the tissue can be improved, and the original structure and function of the tissue can be restored as much as possible. This stage is clinically manifested as a palpable scar. 6
Excessive growth of scar during wound healing under pathological conditions
All scars have some amount of fibrosis caused by excessive and abnormal deposition of extracellular matrix. 50 It is a normal phenomenon for mammals to produce scar tissue during wound healing. 51 However, the wound site of pathogens and cell debris increase during infection, resulting in phagocytes cannot be cleared in time, so the immune system will mobilize more phagocytes. Although they continue to clean up pathogens and cell debris, the released proteins and metabolites cause more cells and molecules to accumulate around the wound, which leads to a more intense inflammatory response, resulting in more severe scars. 52 There are two types of pathological scars: keloids and hypertrophic scars. Keloids are itchy and painful, grow amorphous, and the scarring can extend beyond the wound boundary and invade normal tissue without regressing. 53 In keloids, there is a strong inflammatory response and high levels of pro-inflammatory factors, which lead to the formation of chronic inflammation that pushes the keloid beyond the bounds of the wound. Moreover, fibroblasts are very sensitive to TGF-β1, cell proliferation is rapid, apoptosis is slow, and myofibroblasts capable of secreting α-SAM persist. 48 Therefore, fibroblasts and myofibroblasts produce a large amount of collagen and other components of ECM under the effect of cytokines, thus accelerating fibrosis and forming pathological scar tissue. 54 Since keloids’ constant growth and invasion of surrounding tissues are in line with the characteristics of tumors, and the abnormal activity of fibroblasts and excessive secretion of collagen are in line with the pathological changes of tumors, however, they do not metastasized to other tissues and organs, and effective curative effect can be obtained after treatment, so keloids are actually classified as benign tumors. 55 Clinical studies have shown that many factors have been identified to play a role in the development of keloid, such as genetic factors, endocrine factors, stress, hyperactive inflammation, and immune status. 56 Keloid patients often show familial scarring, which indicates that keloid has a genetic predisposition. At the same time, epigenetic inheritance may also affect the formation of keloids. For example, epigenetic modification caused by non-coding RNA and DNA methylation can also induce the excessive proliferation of fibroblasts to form keloids.57,58 On the other hand, hypertrophic scars usually bulge, itch and thicken, but the scars do not extend beyond the wound area, and they will subside spontaneously within a few years. Hypertrophic scars may vary from person to person, but they vary depending on the location of injury and usually occur in joints and other parts susceptible to stretching. They are closely related to external mechanical forces, which trigger fibrosis by affecting growth factors and other mechanical receptors, thus leading to the formation of hypertrophic scars. 59 However, no matter which kind of pathological scar is, it is characterized by chronic inflammation. Inflammatory reaction can promote fibroblasts to enter the proliferation state. Activated fibroblasts and myofibroblasts are the most important cells, they secrete large amounts of components of the ECM, such as collagen, lead to excessive accumulation and cross-linking of the ECM, ultimately leading to pathological scarring.60,61
The factors affecting scar formation
Skin scarring is the final step in mammalian tissue repair. Every year, millions of people are scarred by postoperative skin injuries, trauma or burns. Although scar formation is a normal product of wound healing, it affects both esthetics and normal skin function. 62 In the process of wound repair, rapid inflammatory reactions can prevent infection and other factors from damaging the body, but they can also lead to the generation of scars. 52 Moreover, overexpression of connective tissue growth factor (CTGF), TGF-β1, and α-SMA during wound healing can promote fibroblast activation and excessive accumulation of ECM, which leads to cell fibrosis and eventually scar tissue generation. 63 The formation of scar tissue is a highly complex process, the number and rate of reproduction of cells, the expression level of cytokines, and the interaction between cells and factors, and even the mechanical force of the wound site will affect the formation of scars. In addition, scar formation is also affected by the depth of the wound, which refers to the depth from the epidermis to the inside. If the wound affects only the epidermis and leaves the rest of the cortex untouched, such as friction, abrasions, and minor burns, it usually does not leave a scar. Wounds that only hurt the dermis, such as shallow degree burns, incisions, usually leave less visible scars. If the wound encroaches on the dermis and even reaches the subcutaneous tissue and deep tissue, such as severe burns and destructive injuries, it usually leaves obvious scars and affects tissue function. 64 Ideally, tissue repair regenerates the original tissue rather than scarring. 65 Therefore, in order to achieve scar free wound healing, we need to explore the mechanism of scar formation at a deeper level. 62 The following is a summary of various factors affecting scar formation (Figure 3).
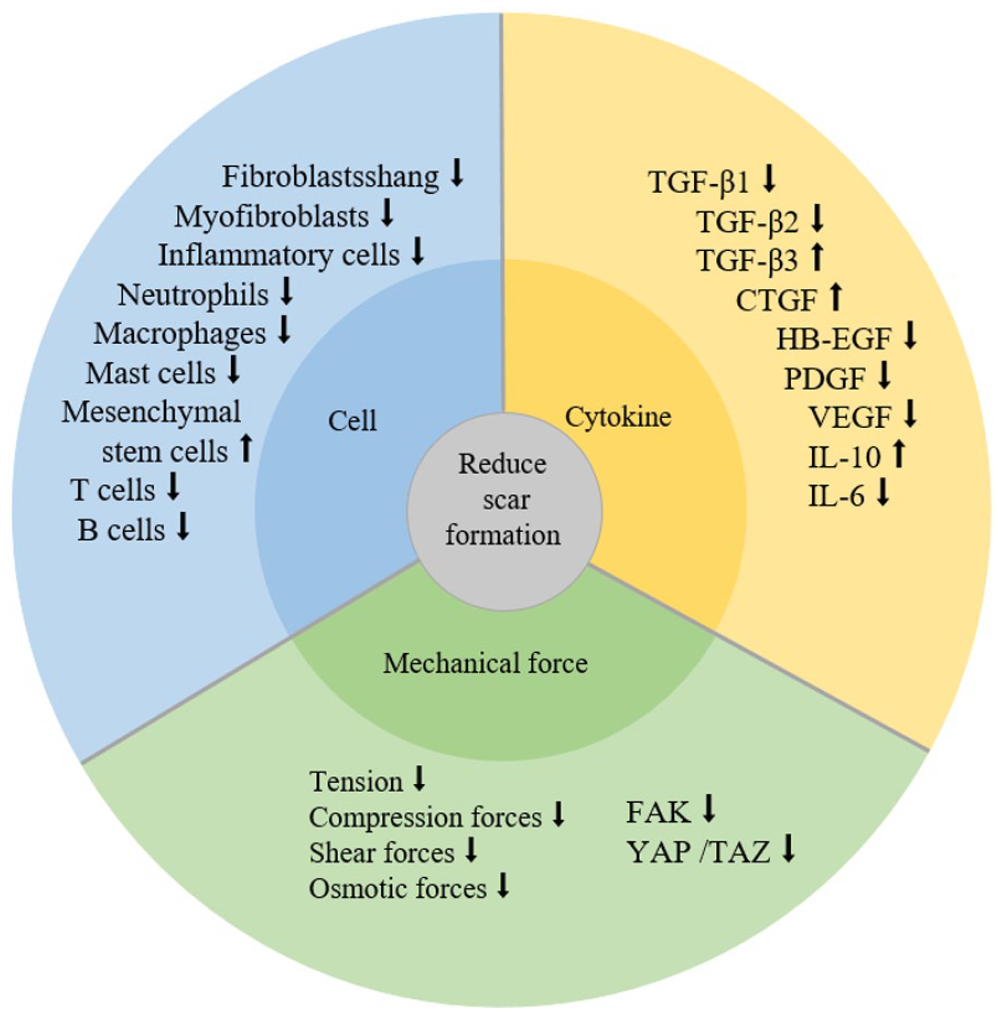
Several factors affecting scar formation at the wound.
Cells involved in the scar formation
Fibroblasts are important for promoting wound healing through wound contraction. Activated fibroblasts differentiate into myofibroblasts, producing large amounts of collagen and ECM, which is an important cause of scarring. 66 Interestingly, this kind of myofibroblast is plastic and can be transformed into adipocytes under the action of bone morphogenetic protein, which can reduce the excessive accumulation of cellular fibrosis and collagen, and ultimately reduce scars. 67 During wound healing, inflammatory cells are recruited into the wound and cause an inflammatory response. In the early stages of repair, the main role of inflammatory cells is to remove damaged ECM and prevent wound infection. 68 Then, some activated inflammatory cells can accumulate collagen and ECM by affecting the activity of fibroblasts, eventually leading to the creation of scar tissue. What’s more, the intensity of inflammation is directly related to the formation of scars, and an excessively strong inflammatory response can even lead to the formation of pathological scars. On the contrary, the inflammatory reaction is significantly reduced in the process of scarless wound healing of the fetus, which further explains the relationship between inflammation and scar formation. For example, neutrophils are important inflammatory cells, and when the skin is injured, they first migrate to the wound to promote the formation of an inflammatory response. However, in the process of scar free healing of fetal wound, the number of neutrophils significantly decreased compared to adult wounds, and they express low levels of adhesion molecules, which indicates that the number of neutrophils is related to scar formation.69,70 In addition, macrophages also play an irreplaceable role in wound healing, which can promote cell proliferation, differentiation and migration, as well as the formation and remodeling of ECM. However, the main feature of less scar in oral mucosal wound healing is the small number of macrophages, which indicates that macrophages also affect the formation of scar tissue. 71 Mast cells are thought to be the transition from scarless to scarred wound healing, because they can affect collagen production and accumulation and affect the formation of scar tissue. Therefore, by blocking the function of mast cells, scar formation can be effectively reduced. 72 Mesenchymal stem cells (MSCs) are important cells involved in wound healing, exhibiting many enhanced tissue regeneration capabilities, which can promote the formation of wound neovascularization and reduce inflammatory responses. 73 Meanwhile, MSCs can regulate immune cells recruited to wounds due to tissue damage. When MSCs enter the inflammatory environment, their immune regulation ability will be activated by relevant cytokines. 74 Therefore, MSCs can regulate the migration and proliferation of immune cells, reduce the intensity of the immune response, shorten the inflammatory phase, thereby inhibiting the occurrence of wound healing fibrosis. 75 It has been reported that scarring can be reduced by injecting MSCs in rabbits. 76
Cytokines involved in the scar formation
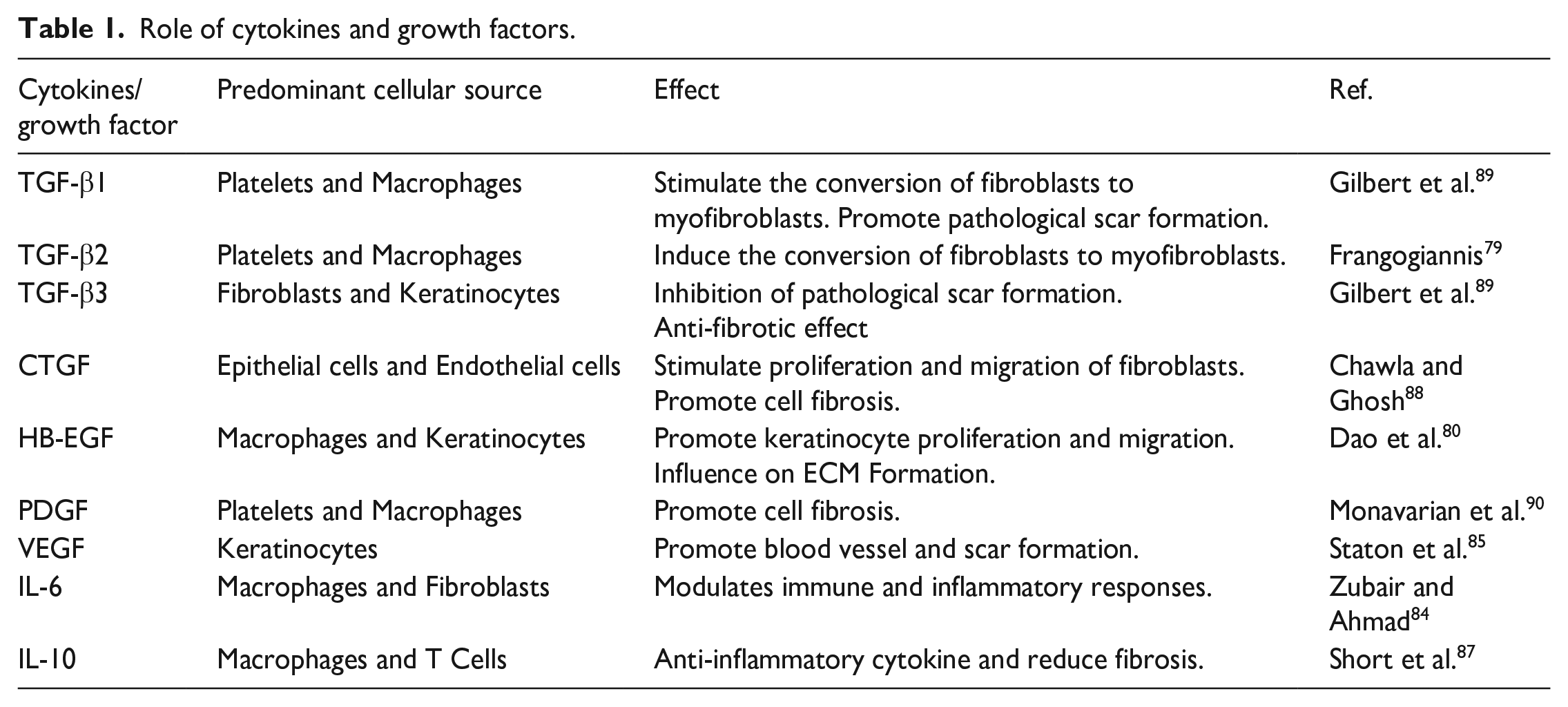
TGF-β is an important signaling pathway in the wound healing process, and its absence can hinder wound healing. There are three different subtypes of TGF-β (TGF-β1, TGF-β2, and TGF-β3), each encoded by different genes. 77 TGF-β1 and TGF-β2 are related to scar formation, because the addition of exogenous antibodies to inhibit these phenotypic transforming growth factors in wound models can effectively reduce scar formation. However, TGF-β3 has the opposite function, it has anti-fibrotic effect, and the proportion of TGF-β3 in the scarless wound healing of the fetus is higher. 78 Furthermore, CTGF is a downstream mediator of TGF-β, and the addition of TGF-β or CTGF promoted granulation tissue formation in wound models, while the addition of both factors resulted in fibrosis. 79 Heparin-bound epidermal growth factor (HB-EGF) also is important, it can affect the proliferation and migration of keratinocytes, as well as the production of ECM, which can promote rapid wound healing and regeneration. 80 PDGF can stabilize newly synthesized capillaries in granulation tissue, stimulate fibroblast differentiation into myofibroblasts to promote fibrosis, and regulate the expression of MMPs to affect the remodeling phase of wound healing. 81 Therefore, PDGF is commonly used to treat chronic wounds and as a profibrotic agent to accelerate collagen deposition. From scarless wound to scar healing, the expression of PDGF increased significantly, only 24 h in fetal scarless wound and 72 h in adult wound, which further indicated that PDGF played an important role in scar formation. 82 Besides, Wnt signaling pathway is composed of Wnt protein, regulatory protein and receptors, which participate in a variety of biological processes and regulate skin wound healing, such as promoting cell proliferation and differentiation, promoting the formation of new blood vessels at the trauma, promoting various organ fibrosis, and regulating the periodic growth of hair follicles. High expression of Wnt3 and Wnt10 can activate fibroblasts, ultimately leading to fibrosis. 83 VEGF is a key cytokine in angiogenesis in the early stage of wound healing. Due to tissue injury, capillaries are destroyed and the wound is deprived of oxygen, which upregulates the expression of hypoxia-inducible factor-1α, and finally induce cells to express VEGF receptors to promote the formation of new blood vessels.84,85 Surprisingly, VEGF can affect the production of scar tissue in addition to promoting angiogenesis in the wound. The expression of VEGF in the wound of scarless fetus is inhibited, and the addition of exogenous VEGF can also induce scar, which indicates that VEGF is related to scar formation. 86 Interleukin-10 (IL-10) can stimulate the production of high molecular weight HA in fibroblasts through related signal transducers, which makes fibroblasts show regenerative phenotype. Therefore, IL-10 is an effective anti-inflammatory factor that reduces fibrosis formation, and its expression level is related to scar formation. 87 In contrast, IL-6 can promote inflammation by activating macrophages or monocyte chemoattractant protein-1 (MCP-1), thereby promoting fibrosis and leading to scar formation. Related studies have shown that the expression level of IL-6 in scar-free fetal wounds is low, IL-6 mRNA exists only for 12 h and lasts for 72 h in adult wounds. 88 The cytokines involved in scar formation and their effects are summarized in Table 1.
Role of cytokines and growth factors.
Mechanical force affects scar formation
In addition to the influence of chemical signals, the mechanical forces acting on the wound site can also affect tissue repair and scar formation. 91 Therefore, when the wound is in the part where the mechanical force continues to increase, significant increase in scars can be observed after the wound has healed. On the contrary, when the mechanical force at the wound decreases, there are fewer scars. 92 Some studies have shown that reducing the mechanical tension of wound site through tension shielding has been proved to be effective in reducing scar formation. 93 Moreover, many mechanical factors (such as osmotic force, shear force, and compressive force) also have an important impact on scar formation during wound healing. In particular, the wounds in the joints, back and sternum are exposed to high mechanical loads, so the scar area after wound healing is large. 94 When the external mechanical force is sensed by the mechanical receptors on the cell membrane, this signal will be transmitted to the cell through the cell membrane, and then the signal pathway in the cell will be activated. 95 Fibroblasts and keratinocytes are two of the most important mechanical sensitive cells in wounds. They can activate focal adhesion kinase (FAK) through the mechanical signal transmitted by integrin. FAK is closely related to mechanical transmission, and is also related to cell adhesion, proliferation, migration, movement and collagen accumulation. 96 Therefore, in the process of skin healing after FAK knockout, the production of cytokines related to scar formation, such as TGF-β and monocyte chemoattractin-1 (MCP-1), will be down-regulated, thus reducing the scar area after healing. It shows that mechanical force can induce the expression of related cytokines by activating FAK, and then induce the aggregation and fibrosis of inflammatory cells, and finally lead to the generation of scars.97,98 Yes-associated protein (YAP) and PDZ-binding motif (TAZ) are activators related to cell transcription. They can exchange between cytoplasm and nucleus in response to the influence of mechanical force on cells. In the nucleus, YAP /TAZ proteins promote tissue regeneration and cell proliferation by controlling the expression of genes related to wound healing. 99 Mechanotransnduction through YAP mainly leads to the transformation of wound En-1-negative fibroblasts into En-1-positive fibroblasts, which ultimately leads to the formation of scars. Therefore, it is essential to reduce the formation of scars after wound healing by inhibiting the mechanotransduction of YAP. 100
The latest techniques to reduce or prevent scar formation
With the understanding of mechanisms of scar formation, various technologies for reducing scar or promoting scarless have been developed. The aim of regeneration engineering is to develop a method that can regenerate tissues or organs after injury. 90 A variety of latest techniques and methods to promote scar-free wound healing were introduced.
Tissue therapy approaches based on biological sources
Skin transplantation has been widely used for wound healing, which can be divided into autotransplantation, allotransplantation and xenotransplantation according to the source. First of all, autotransplantation refers to removing a piece of skin tissue from another part of the patient’s body and transferring it to the wound site. This method has no immune rejection, but its feasibility is very limited. 101 Second, allotransplantation or xenotransplantation refer to transplanting a piece of skin from other donors (human or other species) and then transferring it to the donor. 102 Because the fetus has scarless characteristics, skin transplantation using animal or human fetus as a donor can achieve skin regeneration. 101 In addition, the acellular dermal matrix is produced by a series of treatments on the skin of humans or other mammals, which can prevent transplant-induced immune rejection by removing antigenic epitopes from donor cells, and has excellent properties similar to the natural extracellular matrix. 103 Therefore, transplantation of acellular dermal matrix to the wound site can promote wound repair without promoting excessive accumulation of ECM. 104 Acellular fish skin (AFS) is another source. Because AFS is very similar to human skin in structure, it has porous structure, good biological stability and biocompatibility. AFS transplantation can provide a suitable environment for wound repair, promote wound healing, reduce the intensity of inflammatory reactions, and thereby reduce scar formation. 105 What’s more, Tilapia acellular dermal matrix (TADM) was prepared to simulate the ECM microenvironment of wound site, as shown in Figure 4. The use of TADM in full-thickness wounds has shown that it can guide cell infiltration, promote the formation of new blood vessels at the wound site, reduce inflammatory reactions, regulate the expression level of cytokines, promote wound healing and reduce scar area. 106 Moreover, due to its natural ECM structure and good biological characteristics, human amniotic membrane can prevent infection, relieve pain, maintain a moist environment of the wound, inhibit the expression of proinflammatory factors and resist fibrosis, thus inhibiting the formation of scars. 107 Further, a dehydrated human amniotic chorionic membrane (dHACM) was used to treat skin burns, and wound healing rates were significantly improved and the incidence of hypertrophic scars and contractures was greatly reduced. This shows that dHACM is a safe, feasible and superior alternative to layered skin grafting. 108 Therefore, in order to reduce immune rejection, the transplantation of allotransplantation or xenotransplantation combined with the application of acellular matrix technology has great application potential in the treatment of wound healing and the prevention of scars.
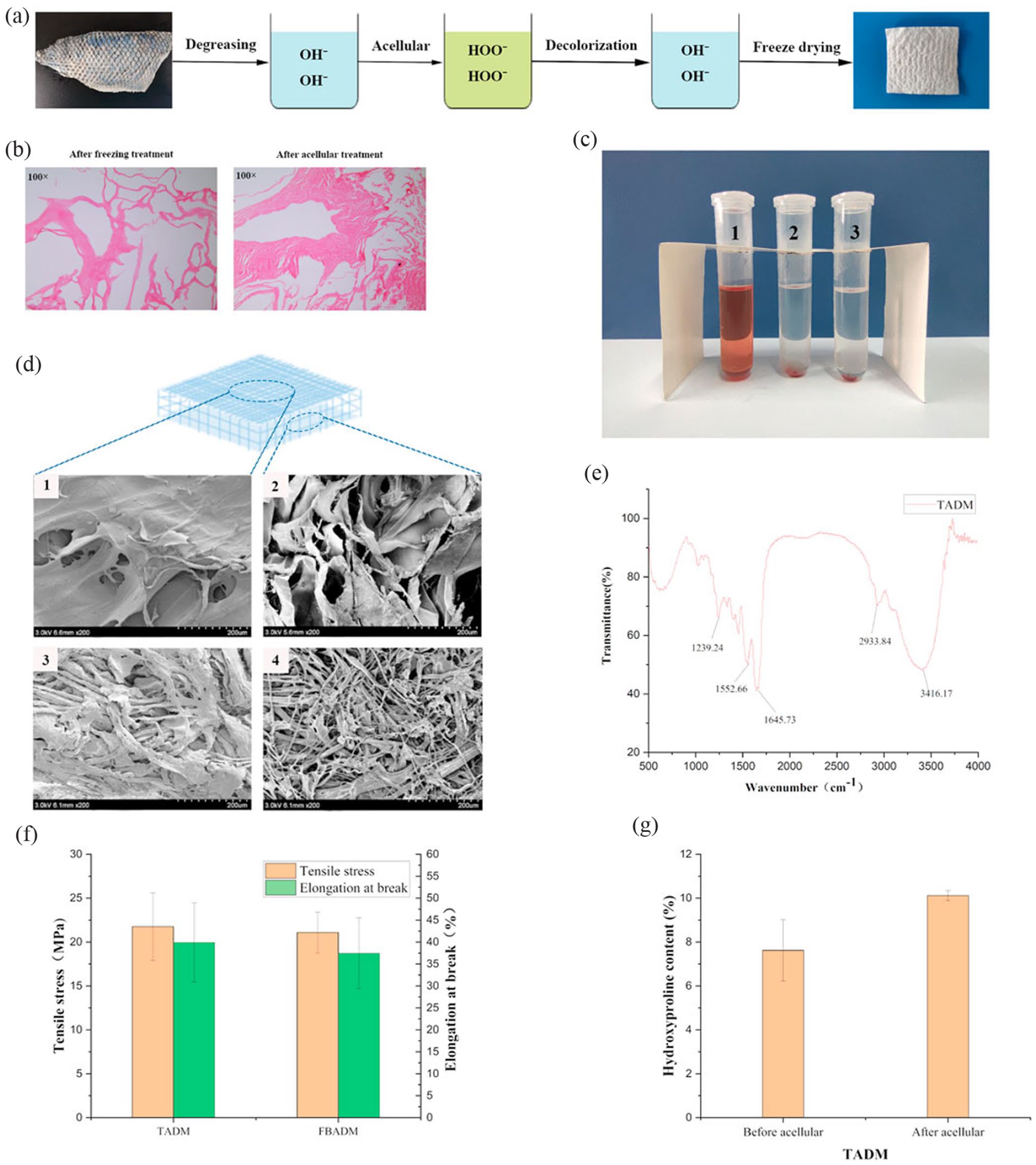
Preparation and characterization of tilapia acellular dermal matrix: (a) is the flow chart of tilapia acellular dermal matrix preparation, (b) is the H&E staining map of tilapia skin before and after acellular treatment, the cells in the frozen fish skin have been broken, there are no obvious cellular characteristics, and there is no cell structure at all after further decellularization, (c) is the result diagram of hemolysis, (d) is the scanning electron microscope, (e) is the Fourier transform infrared spectrum (FTIR), amide A/B/Ⅰ/Ⅱ/Ⅲ and other type I collagen characteristic peaks are obvious, (f) is the comparison of mechanical properties of each sample, and (g) is the comparison of hydroxyproline content of tilapia skin before and after acellular. 106
In short, the use of biological tissue materials is the simplest way to obtain the structure and function of natural ECM, and wound repair can be completed quickly. However, it is still necessary to seriously and comprehensively evaluate the combination of materials and resident cells in the wound. In order to promote the rapid wound healing and inhibit the formation of scar, more biological and physiological studies are needed.
Cell-based therapy
Keratinocytes and fibroblasts play an important role in wound healing, and the use of these two cells is beneficial to provide growth factors and cytokines, thereby promoting regeneration of skin lesions. 109 Epidermal grafts (CEGs) are epithelial sheets made by culturing keratinocytes and can be used as a skin substitute to promote healing. Related studies have shown that when CEGs are applied to skin wounds, it can promote faster epithelialization and reduce scarring. 110 Meanwhile, CEG can also release factors, such as VEGF, TGF-β and MMPs, so as to promote wound healing. 111 By using transplanted keratinocytes on the wound surface, the wound showed faster healing speed, less collagen deposition and reduced scar area. 112 Furthermore, fibroblasts are another source, and transplantation of autologous or allogeneic fibroblasts in vitro can accelerate the re-epithelialization. Using fetal dermal fibroblasts, an ECM with high levels of collagen and HA was formed, and the expression of anti-inflammatory factors was shown to be upregulated, while fibrosis-inducing factors were downregulated. 113 Interestingly, there is also a certain link between keratinocytes and fibroblasts, and co-culture of the two cells and then transplantation into the wound exhibits strong immunosuppressive properties, reduces immune responses, enhances cytokine expression, and reduces scarring. 114 Because the inflammatory reaction is less and the wound heals quickly when the oral mucosa is damaged, the oral mucosal cell sheet prepared with oral mucosal cells can accelerate wound healing and reduce the formation of scars. Therefore, mucosal cell transplantation resulted in faster wound healing, less scar formation, and decreased expression of pro-fibrosis factors such as α-SMA, TGF-β 1 and fibronectin. 115
On the other hand, due to the unique biological properties of stem cells, cell therapy methods using stem cells (such as epidermal stem cells, MSCs, and pluripotent stem cells) as sources have also achieved important results. 116 For example, transplantation of epidermal stem cells into wounds shows higher healing rate and hair growth rate, so it has great application potential in scar free skin repair. Moreover, MSCs are widely present in various parts of the body, such as muscle, fat and bone marrow. Meanwhile, MSCs also have the ability to differentiate directly, which is a beneficial mechanism to promote scar free wound repair 30 Bone marrow-derived mesenchymal stem cells (BMSCs), fetal mesenchymal stem cells, and adipose-derived mesenchymal stem cells have all shown promising effects in skin injury repair, and transplantation into wound sites can lead to reduced wound size and promote more epithelialization. 117 In addition to their ability to differentiate, MSCs also possess paracrine signaling, which is the main role in promoting scar-free wound repair. Paracrine signals such as cytokines, chemokines, and growth factors can promote cell proliferation, differentiation, and angiogenesis at the wound site, thereby accelerating wound healing and reducing scarring. 118 For example, transplantation of adipose-derived mesenchymal stem cells into wounds can release TGF-β3 and MMP1, inhibit the overproduction and accumulation of collagen, and make collagen arrangement more regular. Therefore, wounds exhibited smaller and softer scar tissue, better epithelization, and more subcutaneous tissue blood vessels. 119 In addition, adipose derived regenerative cells are composed of mesenchymal stem cells and mesenchymal blood vessels. When applied to a mouse acute trauma model, they can improve wound healing by promoting hemostasis and vascular regeneration. 120 Some studies have shown that the secretory proteome of human fetal mesenchymal stem cells (hfMSCs) has an anti-aging effect, and aging is also associated with wound healing. Therefore, the hfMSC secretory group (HFS) also has a certain role in promoting wound healing. Wang et al., used polylactic acid-coglycolic acid granules (PLGA) to encapsulate and protect HFS from degradation. When HFS-PLGA was used to treat skin wounds, it could inhibit inflammation and promote vascularization at the wound site, significantly promote wound healing and reduce the area of scars in diabetic rats. (Figure 5) 121 MSC-based media or exosomes have emerged as an important approach for scar-free skin repair. Pluripotent stem cells are another kind of cells that can promote wound healing, such as embryonic stem cells (ESC) and induced pluripotent stem cells (iPSC), can promote collagen synthesis and angiogenesis at the wound site when used, and there is no immune rejection, so it is also used in scar-free skin healing a wide range of applications. 122
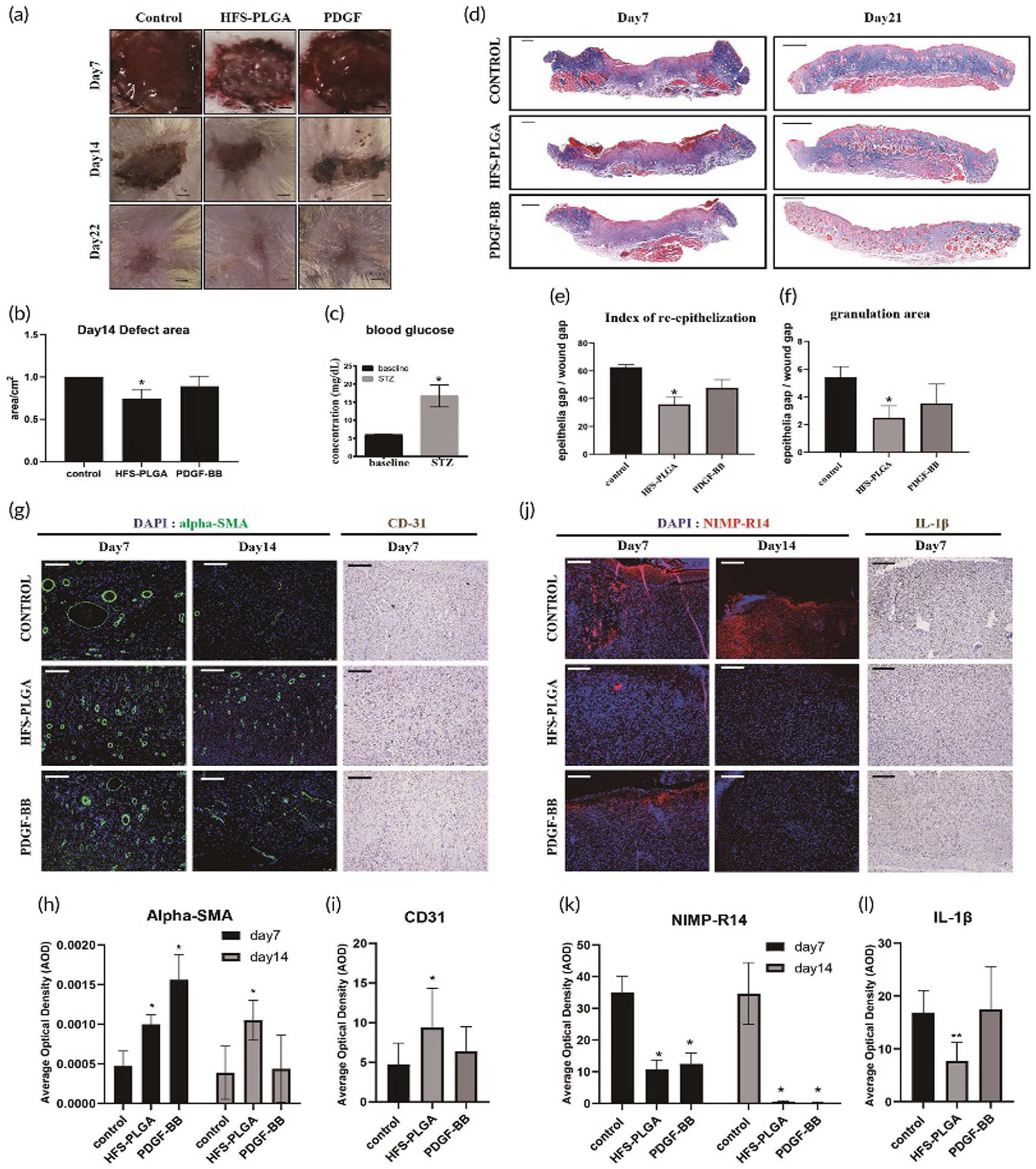
HFS-PLGA promotes rapid healing of streptozotocin (STZ) -induced dermal wound and reduces scar formation in diabetic rats. On day 7, HFS-PLGA promoted the regeneration of wound epithelial cells. Angiogenesis was accelerated on day 7 and 14, and granulation area and scar formation were reduced on day 22: (a) representative picture of dermal injure at 7,14,21 days post-surgery. Scalebar=1.5 mm, (b) semi-quantification result of the wound area. The relative wound area of all groups was measured using image J. ANNOVA test, N=4 *p< 0.05, (c) higher blood glucose indicates that the STZ induction is successful, (d) representative picture of Masson trichrome staining on wound tissue sections in all time points. Scalebar=1 mm, (e, f) semi-quantification data based on the color intensity of Masson trichrome staining. Quantitative data were measured using image J. N=4, Mann–WhitneyU test, *p< 0.05, (g) representative picture of immunofluorescent staining of Alpha-SMA and immunohistochemistry staining result of CD31 result in the wound bed. Scalebar=100μm, (h, i) semi-quantitative result of alpha-SMA and CD31 expression in the wound bed. N=4. ANNOVA test, *p< 0.05, (j) representative picture of immunofluorescent staining of NIMP-R14 and IL-1β in the wound bed, (k, l) the quantification results confirmed that HFS-PLGA particles suppress the NIMP-R14 and IL-1β at the Days 7 and 14 post-injury. N=4. ANNOVA test, *p< 0.05. 121
All in all, cell therapy, either directly transplanted or delivered in a scaffold, has shown good results in promoting scar-free healing and skin regeneration, but the precise functions of some cells are not well understood, and there are potential risks. Therefore, factors such as cell source and dose need to be further optimized.
Therapeutics based on mechanical regulation
The increased mechanical tension acts on the cells at the wound site through various chemical signals. 123 Therefore, it is possible to effectively reduce the production of scar tissue by interfering with these biochemical signals (Figure 6). 124 The technology of limiting fibrosis and reducing scar formation by offsetting the mechanical stress in the wound has been widely used (Table 2). For example, silicone therapy is a common method for treating the mechanical stress at the wound site, including the use of silicone gel sheet. The treatment of hypertrophic scars with silicone can provide mechanical support to the wound and reduce mechanical tension at the wound site. 125 Silicone can undergo a hydration reaction with the stratum corneum, and the treatment with silicone in wounds downregulates the expression of TGF-β1 and TGF-β2, thereby affecting fibrosis and collagen deposition, ultimately reducing scarring. 126 The results showed that the scar treated with silica gel sheet had PDGF and TGF- β1 are lower than the control group, and the scar area is significantly reduced, indicating that silica gel sheet may be a method to prevent scar formation. The expressions of PDGF and TGF-β1 in scar tissue treated with silicone for 4 months were lower than those in control, and the scar area was significantly reduced, suggesting that silicone may be a method to prevent scar formation. 127 From a molecular mechanistic point of view, Wnt/β-catenin signaling shows dichotomy of regeneration and fibrosis in skin repair, and wounds in mice lacking β-catenin shows impaired cell migration, adhesion. In addition, there is a link between Wnt/β-catenin signal and TGF-β1, for example, Wnt signal can promote the expression level of TGF-β1, and TGF-β1 can also react on Wnt signal to promote its signal transduction. 128 The Wnt/β-catenin pathway is usually only active in cells with strong cell division, such as intestinal epithelial cells and epidermal cells. The main characteristic of Wnt/β-catenin signaling pathway is the accumulation and translocation of β-catenin in the nucleus. 129 In the absence of Wnt signal, β-catenin in the cytoplasm will be phosphorylated, and then undergo ubiquitination and degradation. Under the stimulation of mechanical load and other conditions, Wnt can bind specifically to its receptor, the downstream signaling medium is repositioned to the cell membrane, and β-catenin rapidly accumulates in the cytoplasm and translocations to the nucleus. It binds to T cytokines in the nucleus and expresses target genes. 130
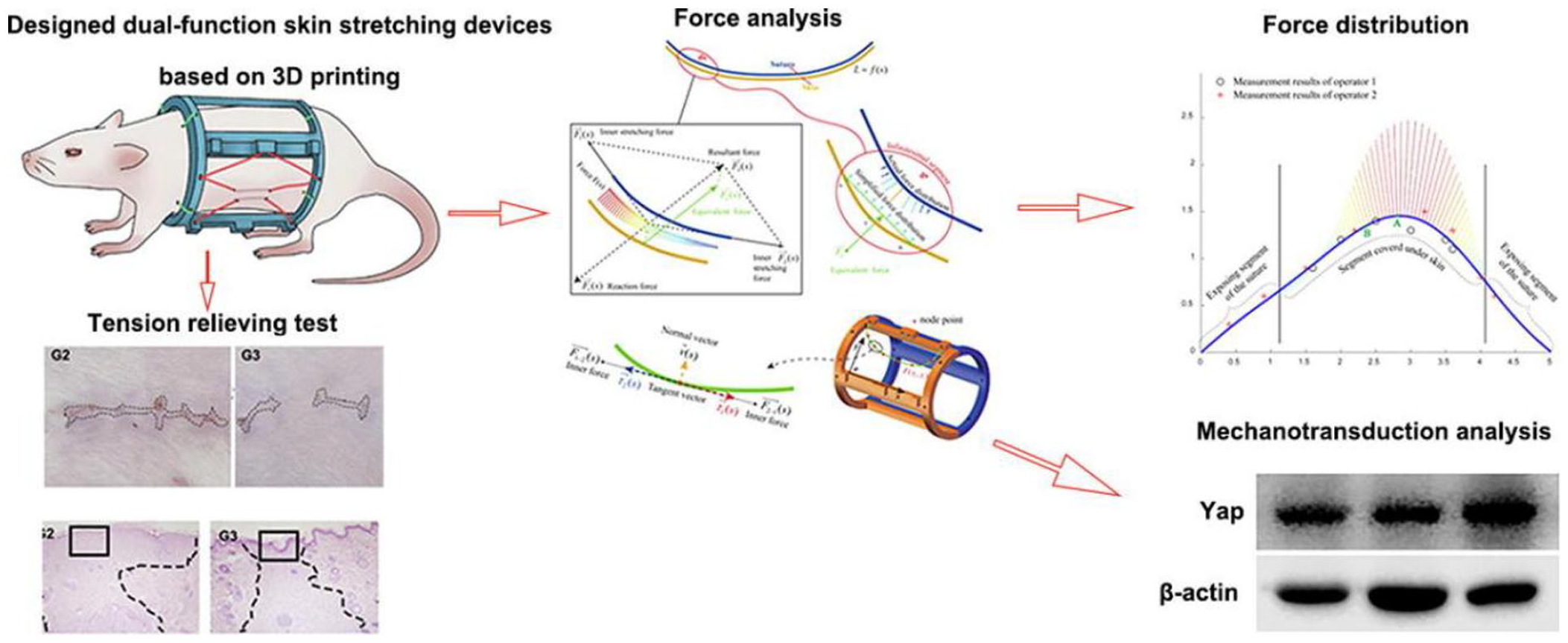
A device attached to the skin of rats to conduct tests on stretching and tension relief. In the skin stretching test, the mechanical load of the skin stretching outward can exert different forces on the skin and cause changes in the tissue characteristics of the skin epithelium. In the tension relief test, the edge of the wound can be pulled in the opposite direction to accelerate the wound closure and reduce the cross-sectional size of the scar. Western blot showed that the mechanical sensitive molecule YAP was related to the mechanical force applied on the skin. 131
Materials for regulating wound mechanical forces.
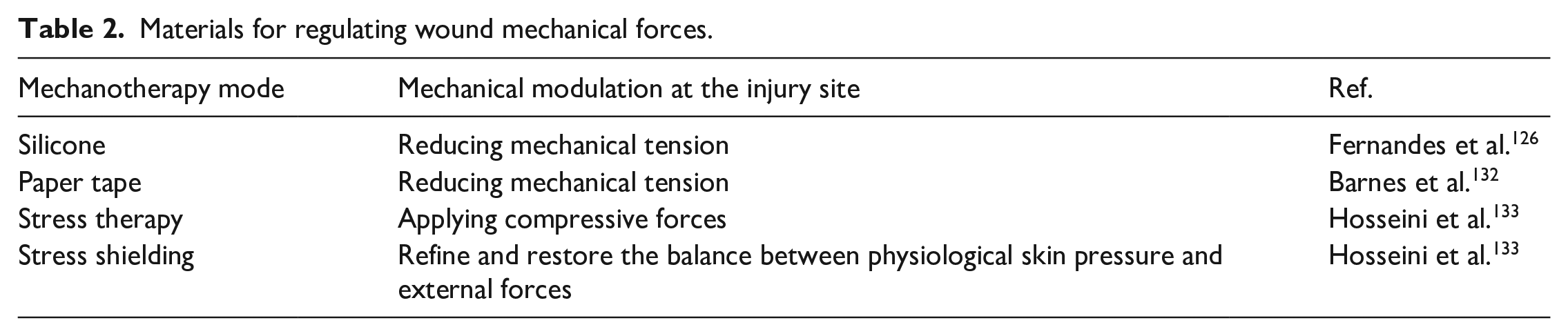
In addition, paper tape also plays a role in scarless by reducing the tension in the wound, it can reduce the volume of the scar and the chance of pathological scarring. 134 Stress therapy pressures the scar by reducing the perfusion pressure in the capillaries and promoting collagen matrix maturation, ultimately resulting in a flattening of the scar. Putting pressure on scar tissue can interrupt the fibrotic tissue, thereby achieving control of the remodeling of the scar, promoting increased softness. 132 Stress shielding can also attenuate the mechanical tension at the wound site, thereby reducing the production of skin scars, the size and appearance of the scar can be significantly changed. 133 Phosphatidylinositol 3-kinase (PI3K)/Akt signaling is involved in regulating cell proliferation, metabolism, and migration, as well as maintaining skin homeostasis. Phosphorylation of Akt is up-regulated when skin is damaged. 135 Fibroblasts at the wound by mechanically loading showed stronger Akt activation than those at an unloaded wound, suggesting a special association between mechanical force and PI3K/Akt signaling. 136 The PI3K/Akt signaling pathway can activate the mammalian target protein of rapamycin (mTOR), and then enhance the angiogenesis, inflammation and deposition of ECM in hyperplastic scars. The disturbance of PI3K/Akt signaling pathway in wound healing may lead to pathological results mainly characterized by excessive cell proliferation. 137 The inhibitor CUDC-907 was used to inhibit the PI3K/Akt/mTOR signaling pathway of keloid fibroblasts, and the results showed that the proliferation, migration and collagen accumulation of fibroblasts were significantly inhibited, and the expression of TGF-β1 was also reduced. Using CUDC-907 in a mouse model also reduced collagen accumulation and angiogenesis in scars. 137 In addition, Rho GTPases are involved in regulating the activities of various cells in vivo, such as skeleton remodeling, proliferation, movement and cell cycle progression of actin cells. Under mechanical loading, actin stress fibers can be recombined and coordinated through Rho signaling pathway. 138 The most typical Rho signaling pathway is RhoA and its downstream component RhoA-associated kinase (ROCK), which can mediate the function of myosin II and actin filaments and generate contractile force. The expression levels of Rho and ROCK in fibroblasts of scar tissue are significantly higher than those in surrounding tissues. 139 Haak et al. found that overexpression of myocardin-related transcription factor (MRTF) and serum response factors (SRF) was over-correlated with activation of Rho GTPases. Therefore, they used CCG-203971 (an inhibitor of MRTF/SRF) to act on fibroblasts in systemic sclerosis, which significantly reduced fibrosis markers. When tested on a mouse model, it can reduce skin thickness and collagen deposition at the site of skin injury in mice. Therefore, Rho inhibitors are one of the effective means to prevent fibrosis.139,140 In conclusion, minimizing the mechanical tension at the wound site through external interference measures is considered to be the best treatment goal for wound healing and regeneration.
Cell-free scaffold
Cell-free scaffolds play an irreplaceable role in creating a microenvironment conducive to cell proliferation and migration by mimicking the natural porous extracellular matrix in tissues. 141 Biomaterials play a decisive role in the performance of scaffolds, because their good biocompatibility, protection against bacterial infection and constant value can often reduce or eliminate rejection and promote perfect wound healing. In addition, the controlled biodegradation of the scaffold is also important, and the porous structure can promote cell migration and phenotype conversion. 142 Therefore, recent studies focus on several common types of scaffolds, mainly including porous scaffolds, hydrogel scaffolds, electrospinning scaffolds, 3D printed scaffolds, and microsphere scaffolds, etc.
Porous scaffolds are usually composed of biodegradable materials and exist in a variety of forms, such as sponges, foam, and mesh. They have a network of cross-linked pores with large porosity, which mimics ECM that can keep the wound in a beneficial microenvironment. The ideal porous scaffold needs to have a specific pore size, suitable porosity and large specific area so that nutrients and drugs can be evenly dispersed, and it should also have good biodegradability and prevent infection and mechanical damage. 143 A variety of porous materials have been used in skin tissue engineering, for example, a composite scaffold based on fibroin protein, sodium alginate and HA, which had a porosity of 92% and was characterized by elasticity and softness. 144 Interestingly, freeze-dried porous sponge scaffolds were prepared with nano silver particles, they had good water retention and swelling properties, and could absorb wound exudates and maintain a moist environment to promote wound contraction and tissue regeneration. 145 In addition, a porous cross-linked scaffold prepared using collagen and chitosan has strong stability and high porosity, promotes rapid wound healing and has good biocompatibility when used in mouse wound models. 146 In short, porous scaffolds have promoted cell adhesion, growth and migration in vitro, and increased wound re-epithelialization and extracellular matrix remodeling capacity in vivo.
Hydrogels are composed of hydrophilic polymers that are 3D cross-linked to form a grid-like material. Due to their structural similarity to natural ECM, high water content, good biological properties and the ability to absorb wound exudates, these characteristics make hydrogels an ideal scaffold material and play an important role in promoting acute and chronic wounds. 147 Hydrogels can be prepared by physical cross-linking and chemical cross-linking. Hydrogels prepared by physical cross-linking usually have self-healing properties, but are less stable. For example, Li et al. used COOH-modified gum Arabic, aluminum chloride, acrylic acid, and 1-vinyl − 3-butyl imidazole as raw materials to prepare hydrogels. 148 On the other hand, hydrogels formed by chemical crosslinking usually need to form covalent bonds under the effect of some catalysts, and their structure is more stable. For example, Liu et al. developed a hydrogel with injectable, self-healing and good stability based on HA. When applied to chronic diabetic wounds in mice, it can promote the transformation of macrophages to M2 type, reduce inflammatory response and accelerate wound healing. 149 In addition, Zhao et al. prepared a light-responsive intelligent hydrogel system by incorporating two-dimensional borocarbonitride nanosheets into methacrylated hyaluronic acid matrix to solve the problem of tumor recurrence and skin damage after melanoma surgery. 150 In short, hydrogels can be made from different materials through a variety of methods, so as to produce a variety of hydrogels to adapt to different locations of wounds, for example, self-healing hydrogels with anti-inflammatory properties can effectively treat chronic wounds, hydrogels with good biocompatibility and biodegradability can inhibit tumor recurrence and promote regeneration when activated by near infrared light, and hydrogels with good tissue adhesion and mechanical properties can be used to treat joint wounds and so on.
Electrospinning is the process of spinning with a polymer solution under the effect of high voltage static electricity. The electrospinning scaffold has many excellent features such as the similar structure and function to the natural ECM, the high specific surface area, porosity, diameter and permeability, and so on. Therefore, electrospinning scaffolds have been studied for wound healing.141,151 For example, Lee et al. developed a nanoparticle polylactic acid glycolate scaffold containing PDGF and bioactive antibiotics, which can significantly enhancing angiogenesis and accelerating the healing rate of diabetic wounds. 152 Ferreira et al. prepared a fiber scaffold by using gelatin/chitosan doped with wakame extract, which has good cytocompatibility and antimicrobial properties and promotes fibroblast adhesion, proliferation, and migration. 153 In addition, Yuan et al. constructed a dual-function nanofibers wound dressing using coaxial electrospinning technology can completely inhibit cancer growth while promoting the regeneration of skin wounds. 154
3D bioprinting is a rapidly developing technology that simulates the microenvironment of natural tissues by printing specific patterned structures with bioinks containing biological materials, drugs, and cytokines. 155 Recently, 3D bioprinted scaffolds that promote wound healing are increasingly used in skin tissue engineering. 156 For example, 3D bioprinted scaffolds loaded with VEGF could significantly inhibit the inflammatory response and promote the formation of new blood vessels, thus achieving rapid wound healing. 157 Domínguez-Robles et al. combined curcumin and lignin with polycaprolactone to create wound dressings by using semi-solid extrusion 3D printing, which can promote epithelial formation, reduce inflammatory response, provide a microenvironment conducive to the proliferation of fibroblasts, enhance the ability to generate new blood vessels, and promote wound regeneration. 158 Lu et al. used gelatin, sodium alginate, and quaternary ammonium chitosan as bio-inks to prepare a novel wound dressing through extrusion 3D printing technology. The wound dressing has good tensile properties, effective antioxidant and antibacterial properties, good cellular compatibility, and has great potential in promoting wound regeneration and healing. 159
With the continuous development of bioengineering technology, particles especially microsphere stents have been widely used and developed. Microsphere scaffolds have excellent mechanical properties, and can allow the controlled release of bioactive molecules, such as the antibiotics, drugs and gene therapy, into surrounding tissues to promote tissue regeneration. 143 For example, Lei et al. reported a microfluidic technique to fabricate chitosan microspheres in order to capture and locally deliver growth factors to promote wound healing. 160 Ouyang et al. used sodium alginate and cellulose as raw materials by reverse phase emulsion method. After self-assembly with ε-polylysine, the porous microspheres showed high porosity, liquid absorption capacity and strong antibacterial activity. 161 Wang et al. prepared a mixture of tannin-loaded microspheres using calcium alginate, fibroin peptide and Bletilla polysaccharide for rapid wound healing. The tannin-loaded microspheres could effectively shorten the inflammatory period and promote the rapid proliferation of fibroblasts. 162 In short, the microspheres can promote the rapid closure of wounds, induce epithelialization and angiogenesis, reduce the intensity of inflammatory response in the process of wound healing, and can also be effective antibacterial and reduce the area of scars after healing.
Natural polymers-based tissue-engineered skin substitutes
Skin substitutes made by mixing various biological and non-biological materials have made significant achievements in promoting skin wound healing. Various natural and synthetic polymers have been used to make wound dressings, mainly in the form of hydrogels, films, microspheres, scaffolds and sponges. 163 Especially in the past 5 years, great progress has been made in the field of skin tissue engineering substitutes. The wound dressing has good histocompatibility, low toxicity, and low inflammatory response, can keep the wound environment moist and promote cell proliferation and differentiation, and has a certain mechanical strength to prevent wound infection. 164 Meanwhile, wound dressings can also carry some drugs, cytokines, and other biological agents to accelerate healing and inhibit scarring. 163 Therefore, some natural polymers such as polysaccharides, proteoglycan, and proteins have been well developed in skin tissue engineering. Natural polymers for synthetic biomaterials are summarized in Table 3. 165 For instance, collagen is a macromolecular compound, has the highest content, the widest distribution and low immunity in mammals, so it has been widely used for wound healing. 166 Improved collagen hydrolysate powder and collagen glycosaminoglycan sponge can combine keratinocytes and fibroblasts to repair with the wound closed quickly, low inflammatory reaction, and smaller and softer scar.167,168 Some metal ions can be added to modify the material of gelatin substrate. For instance, zinc and curcumin can be added in 3D collagen scaffold for promoting angiogenesis and increase the expression of TGF-β3 to reduce scarring. Because zinc can promote keratinocyte migration, re-epithelialization, and act as a cofactor for MMPs, while curcumin can regulate inflammatory factors and inhibit the inflammatory response.169,170 The addition of AgNP and graphene oxide can give the gelatin scaffold antibacterial properties and the properties of destroying the bacterial film, preventing external infection events that occur after implantation. 171
Natural polymers used to make wound dressings.
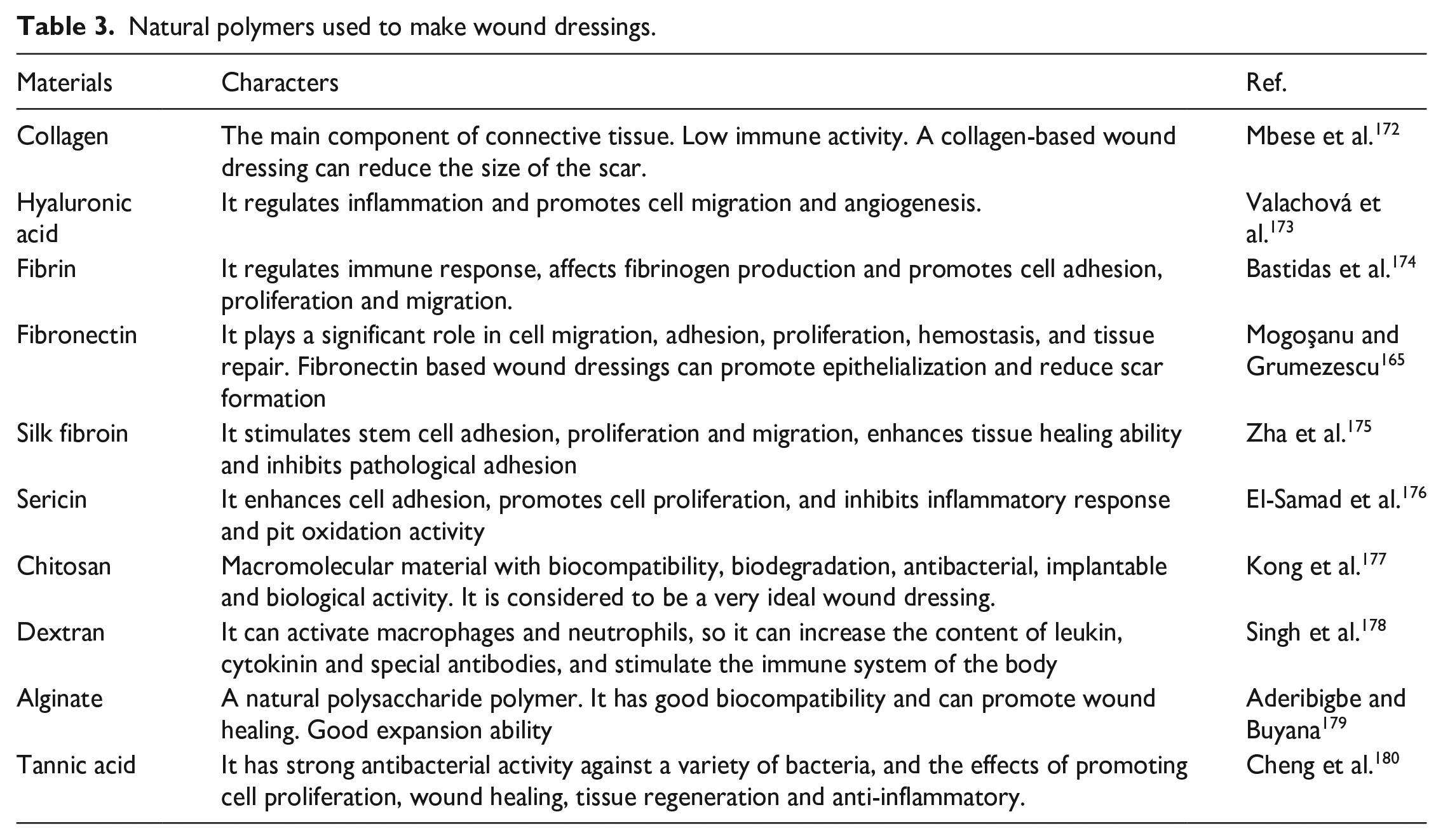
HA can regulate inflammation, promote cell migration and angiogenesis, so it is often used to promote wound healing and regeneration. 181 Wound dressings, consisting of a double layer of HA and an outer silicone membrane, showed faster epithelialization, a well-organized dermal matrix, even collagen distribution and less scarring. 182 HA hydrogel is usually combined with amniotic membrane-derived products to make wound dressings for thicker regenerated skin, more angiogenesis, and smaller scar area.183,184 Moreover, hydrogels can be used as delivery carriers. For example, a PLGA/gelatin/HA fiber membrane scaffold with adipose-derived stem cells accelerated wound healing by increasing the epithelialization rate and promoting the formation of robust dermis, angiogenesis, and macrophage polarization. 185 And a sodium hyaluronate-nanocellulose composite hydrogel loading platelet-rich plasma enhances granulation tissue formation, promotes neovascularization and collagen deposition, and accelerates epithelialization, playing an important role in promoting full-thickness skin wound healing. 186
Fibrin, composed of fibrinogen, is a natural polymer that plays an important role in tissue engineering and wound healing. Fibrin can interact with cells and other ECMs to promote cell adhesion, proliferation and migration. What’s more, it can be used as an effective signaling molecule, which can induce the expression level of related cytokines, thus affecting the activation of immune cells and the production of fibrinogen. 174 For example, human dermal fibroblasts can proliferate, migrate and attach in a natural macroporous interpenetrating polymer network hydrogel composed of polyethylene glycol and serum albumin, and the hydrogel can minimize inflammation and promote cell invasion, tissue remodeling, neovascularization, and ECM formation. 187 A fibrin-based hydrogel to deliver VEGF and platelet-derived growth factor beta was used to effectively promote diabetic wound closure, stimulate wound angiogenesis and improve wound healing. 188 What’s more, the addition of fibrin made the scaffold obtain higher tensile strength and lower elongation at break, strong mechanical strength and good pore size distribution. For example, a hybrid electrospun nanofiber scaffold consisting of polylactic acid-hydroxylactic acid copolymer/fibrin polymer and a fibroin/sulfated alginate porous hydrogel combined with plasma-polymerized polydimethylsiloxane film to address the challenges posed by pressure sores in clinical settings.174,189
Fibronectin can promote skin wound healing and regeneration, and it can interact with various cytokines to affect wound healing. 190 Chantre et al. had constructed a nanofiber scaffold using fibronectin. When this fiber scaffold was used in a full-thickness wound model in mice, it not only promoted wound healing and reduced scar formation, but also improved tissue repair and restored some skin accessories and adipose tissue. 191 The presence of fibronectin enables the matrix to enhance the adhesion and proliferation of fibroblasts. When fibrin matrix prepared by mixing fibronectin with plasma fibrinogen was used to treat wounds in mice, it enhanced angiogenesis, accelerated the wound healing process, and reduced scar area after healing. 192
Silk fibroin, a naturally occurring protein found in silk, has been shown to be a vital component in tissue regeneration. Numerous wound dressings utilizing silk fibroin have been created with the aim of limiting and avoiding scar formation. 193 For example, silk fibroin with microcarrier made higher epithelization, and inhibited fibrosis by downregulating the expression of FGF-2 and CTGF, thereby reducing the formation of scar. 194 A biodegradable polyglycolic acid/silk fibroin nanofiber scaffold containing deferoxamine can induce collagen deposition and vascular reconstruction, promote tissue mechanical property restoration, accelerate the rapid healing of diabetic wounds, and provide a promising treatment strategy for chronic wounds. 175 In addition, an allantoin-functionalized complex hydrogel by combining fibroin protein with sodium alginate promoted rapid wound healing by promoting re-epithelialization and vascularization and enhancing collagen accumulation at the wound site. 195 Sericin is another protein existing in silk, and its immunogenicity is lower than that of silk fibroin. Dressings utilizing sericin are extensively employed in tissue engineering applications as well. Sericin based hydrogel can promote the formation of new blood vessels by up regulating the expression of VEGF and EGF, and can down regulate TGF- β1 and TGF- β2 to inhibit the formation of scar tissue. Surprisingly, this hydrogel is capable of enlisting MSCs to the site of injury, facilitating the regeneration of skin appendages like sebaceous glands and hair follicles. 196 Sericin and carboxymethyl cellulose were used to prepare a multifunctional hydrogel. When used on diabetic wounds, it can effectively inhibit inflammatory response, promote angiogenesis and collagen accumulation, accelerate wound healing, reduce scar area after healing, and regenerated skin appendages such as hair follicles at the wound site. 176 A natural silk fibroin wound dressing by regulating the silkworm’s spinning behavior effectively accelerated wound healing and reduces scar area. 197
Chitosan is considered as an ideal wound dressing due to its biocompatibility, biodegradability, antibacterial, implantability and bioactive macromolecules. It has been found that it can promote the recruitment of inflammatory cells at the early stage, thus speeding up wound healing and reducing scar formation.198,199 The alkaline fibroblast growth factor and antibacterial peptides were slowly released from the microspheres, effectively inhibiting bacterial infection at the wound site, promoting blood vessel formation, reducing inflammation, ultimately accelerating wound healing and reducing scar formation. 200 In addition, methacrylic anhydride grafted onto chitosan and then introduced polydopamine to form hydrogel which can efficiently inhibit bacterial growth, suppress inflammation, promote neovascularization and re-epithelialization, accelerate wound healing speed, and reduce scar formation area. 201
Dextran is a polysaccharide that exhibits different biological functions through chemical modification of its hydroxyl groups. Dextran is mainly used in the form of hydrogels to treat skin lesions. 202 They are capable of promoting the transformation of M1-type macrophages into M2-type macrophages, thereby effectively diminishing the level of inflammatory response while stimulating the generation and epithelialization of new blood vessels. 203 For example, a dextran ethyl isocyanate ethylamine methacrylate hydrogel can significantly reduce the inflammatory reaction of the wound, promote the transformation of M2 macrophages, regenerate hair and other skin accessories, accelerate the wound healing process, and promote the perfect regeneration in the full-thickness wound models of mice and pigs. 204 Moreover, the mixed hydrogel based on β-glucan can promote the formation of type III collagen and the regeneration of hair follicles, regulate the production of VEGF and immune factors, inhibit the expression of fibroblast regulator En-1 in wound site, significantly accelerate wound healing, promote the formation of skin appendages and increase the expression of TGF-β3.205–207
Alginate is a natural polysaccharide polymer, mainly comes from brown algae and bacteria and can be crosslinked with divalent cations to form hydrogels. 179 Alginate also has good swelling capacity and biocompatibility, which can absorb wound exudates and limit wound infection. Wound dressings made of alginate can help stop bleeding and promote wound healing. 208 For example, the nanofiber membrane based on alginate/PVA showed high antioxidant activity and antibacterial properties, and had good biocompatibility, which accelerated the speed of wound healing and reduced the area of scar. 209 A sponge wound dressing with the properties of hemostasis, antibacterial, anti-inflammatory and promoting hair follicle regeneration and angiogenesis using alginate, chitosan and fucoidan polysaccharide as raw materials. 210 And a biodegradable scaffold based on gelatin/sulfated alginate was developed to address the problem of chronic non-healing skin wounds caused by diabetic foot ulcers, aiming to accelerate wound healing in diabetic mice. In vivo experiments showed that the mixed scaffold could make collagen distribution at the wound site more uniform, reduce immune cell infiltration, and effectively accelerate the wound healing process. 211
Through the utilization of tannic acid (TA) combined with dopamine, near-instantaneous hydrogen bonding mediated citrate gelation was achieved, ultimately resulting in the development of a bioadhesive with combined antibacterial activities, anti-inflammatory, and antioxidant, also known as 3A-TCMBAs. In vivo experiments conducted on a skin wound model infected on full-layers have demonstrated that the 3A-TCMBAs+NIR treatment can promote wound closure and deposition of collagen while also increasing the ratio of collagen I/III at the wound site, and inhibit proinflammatory cytokines, promote angiogenesis at the early stage, inhibit and trigger the degradation and remodel ECM in the later stage to achieve scarless wound healing (Figure 7). 212 A tannic acid-based hydrogel (PDH) was prepared by covalent crosslinking with polyvinyl alcohol (PVA) and chelating with Fe3+. Animal experiments showed that PDH could promote granulation tissue and neovascularization formation, reduce inflammatory reaction, accelerate wound healing, and decrease scar formation area. 180 In addition, TA can be incorporated into quaternized chitosan (QCS) to construct a wound dressing with antioxidant and antibacterial properties, which promoted wound hemostasis, inhibited inflammatory reactions, accelerated collagen accumulation, and facilitated wound healing while reducing scar area. 213
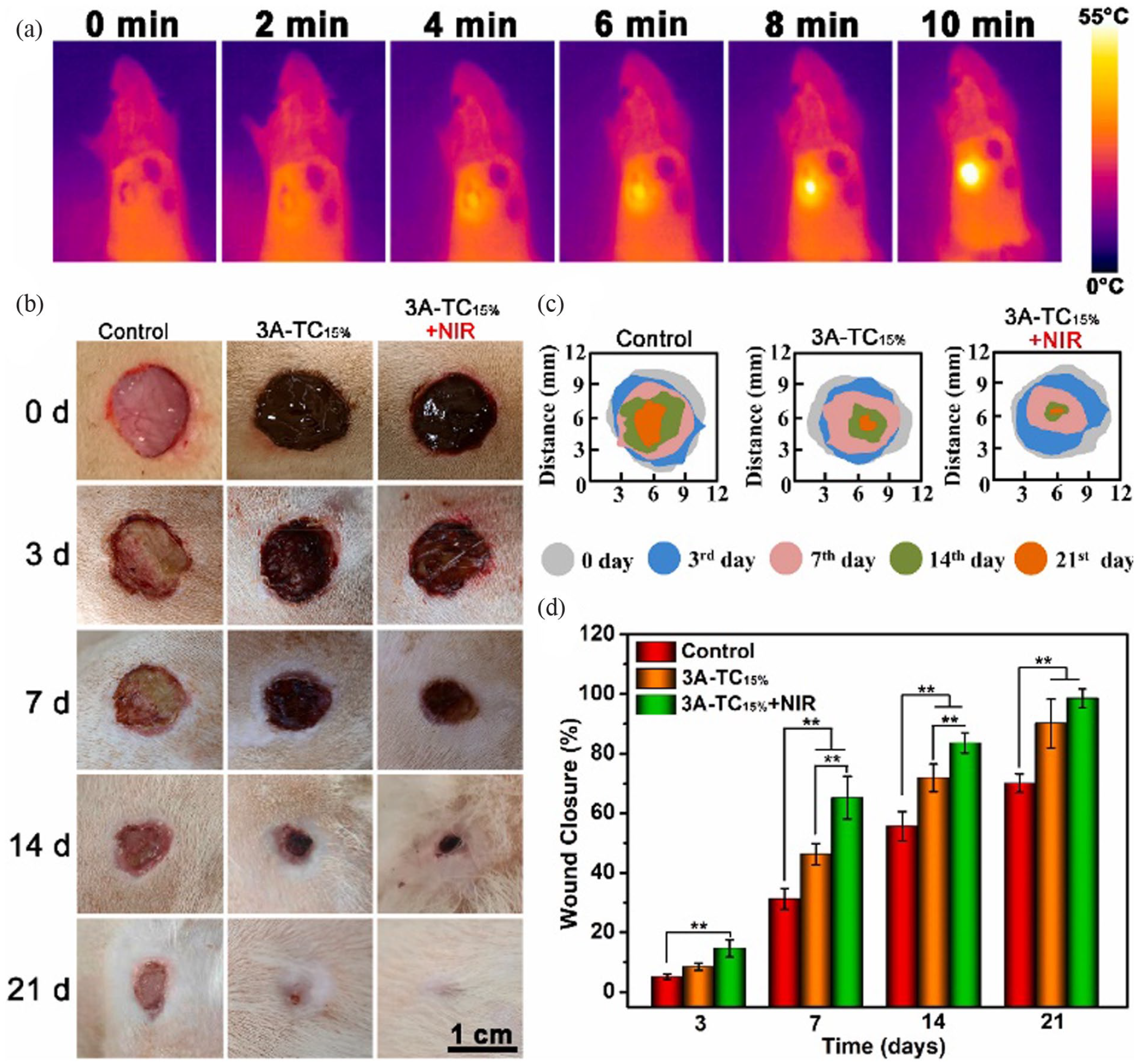
3A-TCMBA +NIR promotes closure of infected wounds and results in scarless healing: (a) photothermal temperature change of SD rats, (b) representative photographs of the wounds treated with samples, (c) schematic diagram of wound closure, and (d) quantitative statistical analysis of wounds closure. 212
Gene-based therapy
The purpose of gene therapy is to introduce some favorable growth factors into some cells involved in wound healing, make them express at a high level in the cells for a certain period of time, synthesize and release some proteins that promote wound healing locally, so as to promote wound healing toward regeneration and reducing the scar area after healing. It is a promising new treatment to promote rapid wound healing and reduce scar formation. Gene therapy includes gene amplification (adding genes to cells), gene silencing (inhibiting gene expression), and gene editing (modifying genes in cells). 214
Gene amplification is the most direct method of gene therapy, which can repair the abnormal cell function caused by gene deletion or defect. The purpose of gene amplification is to introduce DNA or mRNA into target cells so that specific proteins can be normally expressed in target cells, so as to restore the normal function of cells. 214 For example, Lou et al. developed a gene activated bilayer dermal equivalent (Ga-BDE) with good biocompatibility. They first designed a nanocomposite encoding VEGF’s Lifefectamine 2000/plasmid DNA, and then loaded the complex into a collagen-chitosan scaffold/silica gel membrane bilayer dermal equivalent to produce Ga-BDE. Treatment through the use of Ga-BDE in wounds, compared with the control group, the rat diabetes wound model showed faster wound healing, at the same time, the infiltration and transformation of macrophages were accelerated, angiogenesis was significantly enhanced, and better regeneration effect was obtained (Figure 8). 215 In another study, mineral-coated microparticles (MCM) were used as biomaterials for gene delivery because it can improve the transfection efficiency of plasmid DNA, the application of mRNA/MCM on the mouse wound model could improve the wound closure rate and the wound healing condition. 216 Han et al. have reported the role of human dermal fibroblasts (HDF) overexpressed with a granulocyte-chemotactic protein-2 (GCP-2) in wound healing. They first constructed minicircle DNA (mcDNA) containing GCP-2 and then delivered mcDNA into fibroblasts by using microperforation technology. The results showed that HDF overexpression of GCP-2 can enhance the ability of angiogenesis and activate the expression of some cytokines related to wound healing. Injection of HDF overexpressing GCP-2 at the wound site in a full-layer wound model promoted epithelialization, increased capillary density, accelerated wound healing and reduced scar formation area. 217 Additionally, Sun and his colleagues used chemically modified mRNA for gene delivery, and injecting the mRNA encoding vascular endothelial growth factor A into wounds of diabetic mice promoted epithelialization and accelerated wound healing. 218
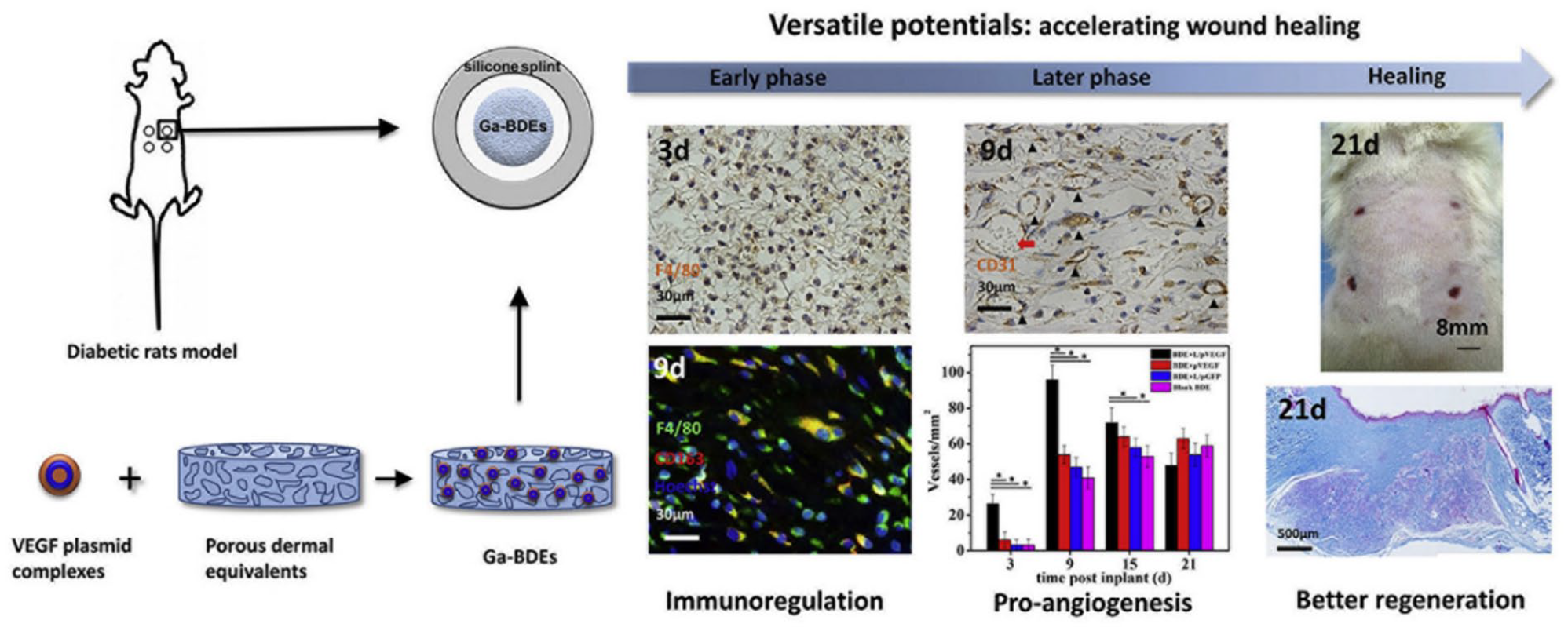
Ga-BDEs were constructed by using VEGF plasmid complex and porous dermal equivalent to treat diabetes wound model in mice. The use of Ga-BDEs can regulate immune response, accelerate the formation of vascular tissue, and promote wound healing and regeneration. 215
Gene silencing refers to the degradation or inhibition of translation by targeting specific pre-mRNA or mRNA, so as to achieve the goal of down-regulating gene expression, and finally reducing the synthesis of specific proteins to affect the function of cells. Gene silencing effect is usually mediated by nucleic acid aptamer, RNA interference (RNAi), microRNA (miRNA), small interfering RNA (siRNA), and antisense oligonucleotides (ASO). Gene silencing usually down-regulates gene expression by 70% instead of eliminating genes. 214 It is reported that FK506 binding protein-like (FKBPL) can inhibit wound angiogenesis. Therefore, inhibiting the synthesis of this protein by using siRNA targeting FKBPL can enhance angiogenesis, thereby speeding up wound healing. When the siRNA was delivered to the wound site, the wound showed stronger angiogenesis and faster wound healing. 219 In addition, siRNA such as HA-PEI@siRNA-29a can be delivered with hydrogels. The effectiveness of hydrogel in hastening wound healing and enhancing the expression of angiogenic factors while retarding proinflammatory factors has been validated through in vitro and in vivo investigations. 220 The overexpression of CTGF is a major cause of fibrosis and scarring. DegradaBALL (LEM-S401) loaded with siRNA showed persistent and effective CTGF silencing effect in both pulmonary fibrosis and skin fibrosis model cells. In addition, the use of LEM-S401 in the mouse wound model can promote the epidermal recovery and tissue remodeling, and can also effectively inhibit the formation of proliferative scars in the mouse model of skin fibrosis. 221 Tanaya et al. prepared a bi-functional hyaluronic-based hydrogel by loading an arginine-glycine aspartate (RGD) peptide and an anti-vascular endothelial growth factor-2 (VEGF-R2) DNA aptamer into a hydrogel which can promote cell adhesion and growth due to the presence of RGD, while the presence of anti-VEGF-R2 DNA aptamer enables the hydrogel to induce cell migration, improve cell viability and stimulate angiogenesis. 222 The microRNA-135a-3p acts as an inhibitor of angiogenesis by regulating p38 signaling in endothelial cells. Elevated levels of microRNA-135a-3p can inhibit proliferation and migration of endothelial cells at the site of injury, while inhibition of its expression yields the opposite effect. Therefore, delivery of a microRNA-135a-3p inhibitor to the wound site in diabetic mice can increase angiogenic rates, promote granulation tissue formation, improve wound closure rates, and reduce scar area post-healing. 223
Gene editing, also known as genome engineering, can modify specific target genes in the organism genome. 214 For example, based on CRISPR technology, Srifa et al. used Cas9 nuclease to edit specific sites of the genome in human mesenchymal stromal cells (hMSCs), and its targeting was achieved through single-guide RNAs. They used electroporation to deliver Cas9 nuclease and adeno-associated virus 6 to deliver homologous repair templates to achieve efficient and site-specific editing of hMSCs genome, thus producing platelet-derived growth factor beta and VEGFA-hypersecretingh MSC as wound healing agents. 224 The use of engineered hMSCs in the treatment of mouse wound models could improve the secretion of growth factors, accelerate the closure of wounds, and promote the formation of granulation tissue and blood vessels. 224
In short, gene therapy is an advanced treatment method that can promote rapid repair of damaged organs and tissues by altering genetic information within cells. In terms of skin wound healing, it can introduce specific genes to promote cell proliferation and differentiation, and inhibit the expression of some genes, so as to eliminate the factors that hinder wound healing. The use of gene therapy can achieve more accurate and personalized treatment for different types of skin injuries. It can selectively correct excessive scars caused by unhealed skin wounds or genetic defects at the root. At present, the main molecules that regulate gene expression are plasmid DNA and mRNA for intracellular gene overexpression, and siRNA and miRNA for gene silencing. In addition, gene editing tools based on palindromic sequences also play an important role in the development of gene therapy. Although gene or nucleic acid products can be easily applied to local wounds to promote rapid wound healing, their stability in wounds is difficult to be guaranteed and cannot be easy to be absorbed by cells.
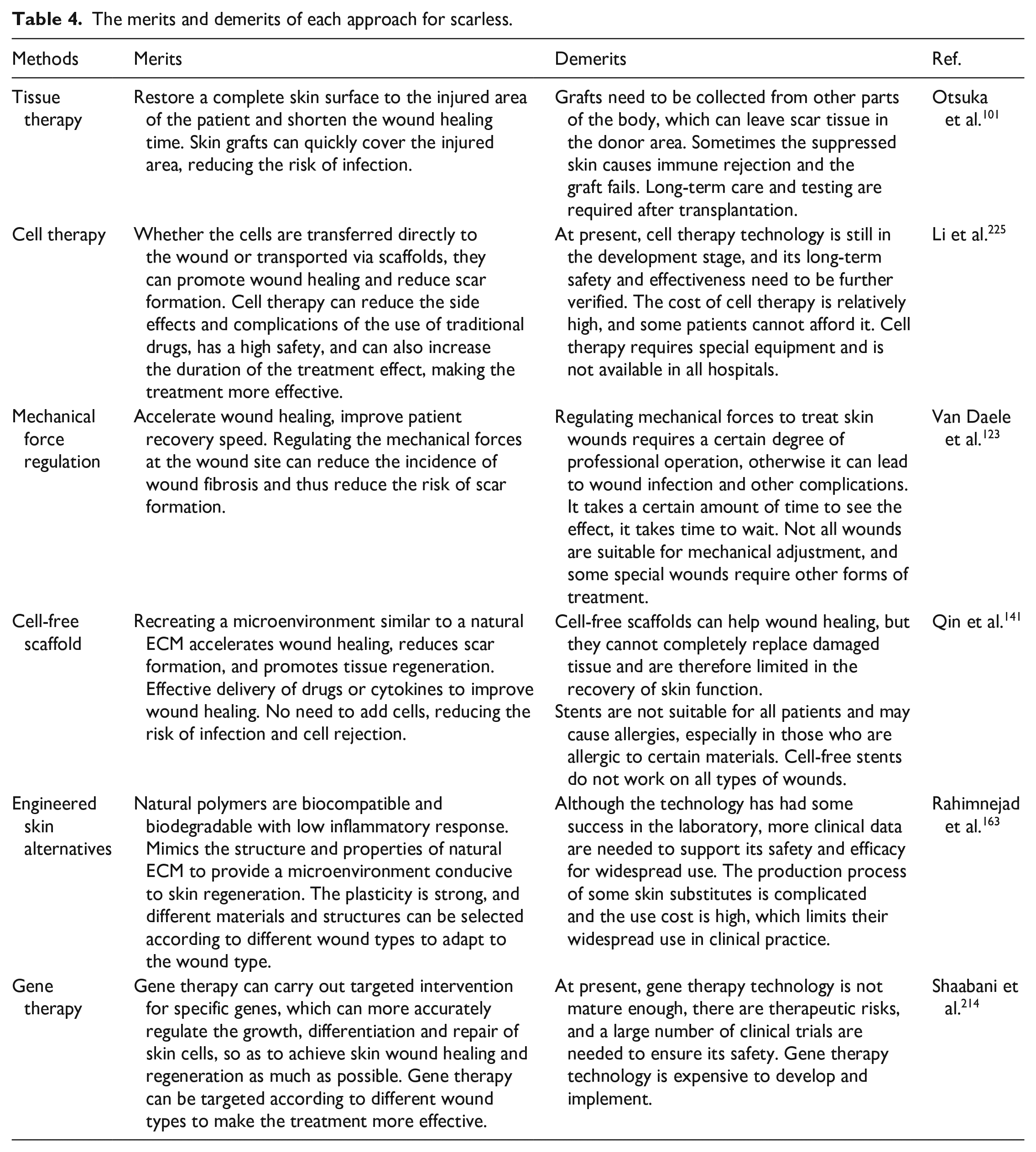
In conclusion, although these technologies reduce or prevent scar formation to some extent, they are not the most ideal methods. Thereby the merits and demerits of each approach are summarized in Table 4.
The merits and demerits of each approach for scarless.
Conclusions and outlooks
This review discusses the fundamental mechanisms involved in wound healing and scarring, while also presenting various approaches to prevent and minimize scarring during the wound healing process. Balancing wound healing and scarless skin repair, and regulating the order of time and space between them is difficult, and also the direction of future development. It may be possible to select appropriate stem cells (such as mesenchymal stem cells, epidermal stem cells and pluripotent stem cells, etc.), regulate inflammatory response (such as the phenotype transformation of pro-inflammatory cells and anti-inflammatory cells), regulate the progress of fibrosis (the transformation of fibroblasts and myofibroblasts), and regulate the role of mechanical force (change the mechanical force of the wound site through external force application), from both time and space levels, cells, factors and mechanical forces regulate the rapid completion of wound healing and the reduction or elimination of scars. By understanding the mechanism of scar tissue formation, many anti-scar treatments have been developed, such as: acellular tissue, cell-based strategies, wound dressings, modulation of mechanical forces, cell-free scaffold, and gene therapy. These techniques have achieved important achievements in promoting wound healing and reducing scar formation. However, so far there does not appear to be an approach that can be advocated for widespread use in scar-free regenerative repair of wounds, and the most difficult obstacle to achieving skin regenerative healing is regenerating tissue containing hair follicles, sweat glands and micro-vessels, and leaving no scar tissue after treatment.
Achieving scar-free wound healing has become a topic of concern, and the ideal treatment method should speed up wound healing, minimize scar formation, be safe, reliable, sustainable and affordable, and achieve personalized treatment. Since the emergence of 3D bioprinting technology, its development has been very rapid. It can connect various factors (biocompatible materials, cells and factors, etc.) in the treatment of wound healing, print biological materials with similar structure and properties to the natural extracellular matrix, and promote wound healing toward regeneration. In addition, 3D bioprinting technology can print biological materials directly on the wound, and can also be combined with sensors and imaging technology, which are beneficial to achieve regenerative healing of skin wounds. However, 3D bioprinting technology also has some shortcomings, the formation of the corresponding vascular system and the selection of cells and inks have not been perfectly solved. Nanomaterials can be utilized as drug carriers or therapeutic devices to play an important role in various stages of wound healing. The treatment methods based on nanomaterials have shown good antibacterial effects, which can effectively reduce the drug resistance of bacteria, shorten the duration of inflammation and thus shorten the wound healing time, and provide a very promising treatment method in the treatment of chronic wounds. At present, there are still some challenges in nano-based treatment methods, such as the problems between nanomaterials and biosafety, the heterogeneity of different wounds limits the regeneration potential of nanomaterials, and the optimization of manufacturing processes. Cell-free scaffolds have made great progress in the intervention of skin wound healing, but still have not reached the ideal state of regenerative therapy. Bioengineered scaffolds rely on the properties and structures of biomaterials, and the development of wound healing is closely related to biomaterials and skin biology. Therefore, the further exploration and development of wound healing mechanisms and the use of excellent biomaterials to manufacture scaffolds will provide a broader vision for reducing scars and achieving scar-free healing.
In addition, there is an urgent need to develop effective methods for delivering genes that protect them from degradation during delivery and promote their function within cells. Although great progress has been made in the development of effective delivery techniques in recent years, only a few gene therapies have met the requirements for clinical trials. Therefore, for gene therapy to be applied clinically, it must overcome uncertainties such as low transfection efficiency and long-term toxicity. Gene editing technology is a technology that changes the function and characteristics of cells by artificially intervening the expression or structure of genes, which can achieve the purpose of treating and preventing diseases at the cellular level, and has potential application prospects in realizing scar free wound healing. Gene editing technology can promote skin tissue regeneration and repair by altering various cell behaviors and cell-cell interactions during wound healing. For some genetic diseases that affect wound healing, such as hemophilia and lupus, coding can address these problems by repairing genetic defects. Gene editing technology has a broad application prospect in the realization of scar free skin wound healing. Although this technology is currently in the research stage and further clinical trials are needed to prove its efficacy and safety, in the future, as the technology continues to develop and mature, gene editing technology is expected to become one of the ways to achieve scar-free wound healing in the skin.
Achieving scarless skin regeneration is a highly challenging task, as the mechanisms underlying scar formation are complex and not yet fully understood. This requires further research to determine effective treatment methods. Moreover, individual variability and uncertainty also affect treatment outcomes, and current available techniques and treatments are still limited. Developing new treatment methods requires significant funding and research resources, while also requiring large-scale clinical trials to evaluate safety and efficacy. Additionally, there is a close relationship between scarless wound healing and clinical practice. The goal of clinical treatment is usually to heal the wound quickly and effectively, leaving minimal scars. In some cases, such as after surgery, poor healing processes may result in noticeable scars or hypertrophic scars. while scarring can affect a patient’s appearance, physical and mental health, and social and professional development. In summary, scarless wound healing of the skin is a complex issue that needs to be approached from various perspectives in terms of research and treatment. We look forward to the continuous development and application of more and more technologies to bring effective and safe treatments to the medical field.
Footnotes
Author contributions
Conceptualization, K.Z. (Kun Zhang) and B.C. (Bingjie Cai); writing—original draft preparation, S.Z. (Shengxi Zhou), M.X. (Mengbo Xie), J.S. (Jingjing Su) and B.C. (Bingjie Cai); writing—review and editing, K.Z. (Kun Zhang) and J.L. (Jingan Li); Funding acquisition, B.C. (Bingjie Cai) and J.L. (Jingan Li).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We sincerely thank the National Natural Science Foundation of China (U2004164) and Key Scientific and Technological Research Projects in the Program for Henan Province (232102311155).