
Abstract
Severe tracheal injuries that cannot be managed by mobilization and end-to-end anastomosis represent an unmet clinical need and an urgent challenge to face in surgical practice; within this scenario, decellularized scaffolds (eventually bioengineered) are currently a tempting option among tissue engineered substitutes. The success of a decellularized trachea is expression of a balanced approach in cells removal while preserving the extracellular matrix (ECM) architecture/mechanical properties. Revising the literature, many Authors report about different methods for acellular tracheal ECMs development; however, only few of them verified the devices effectiveness by an orthotopic implant in animal models of disease. To support translational medicine in this field, here we provide a systematic review on studies recurring to decellularized/bioengineered tracheas implantation. After describing the specific methodological aspects, orthotopic implant results are verified. Furtherly, the only three clinical cases of compassionate use of tissue engineered tracheas are reported with a focus on outcomes.
Introduction
Tracheal resection with end-to-end anastomosis (TRA) represents the treatment of choice for a variety of conditions that result in airway narrowing (e.g. congenital tracheal stenosis, traumatic injuries, chronic inflammatory diseases, neoplasms, or post-intubation injury) or in tracheal defects (e.g. tracheo-esophageal or tracheo-arterial fistulae, persistent tracheostomies, post-surgical defects) when primary closure is not possible.1–4 However, TRA is only possible when the tract to be excised is limited to 50% of the trachea in adults or 30% in children 5 ; for longer defects, in fact, re-approximation of the two tracheal stumps would not be possible because of an excessive anastomotic tension.
Currently, for patients affected by such long-segment tracheal lesions, the only established treatment option is represented by long-term airway stenting with either endotracheal stents, tracheostomy tubes or Montgomery T-tubes. However, such appliances cause a significant deterioration in quality of life and are fraught with complications such as infection, stent migration, mucous plugging or granulation tissue formation. 5 Moreover, for lesions of malignant etiology, airway stenting is only a palliative procedure.
Tracheal replacement, by the adoption of airway substitutes, has been proposed as an alternative approach to overcome the TRA technical limitations, thus avoiding long-term airway stenting and answering the patients’ clinical needs whether no other treatments are available. Briefly, the ideal tracheal substitute should possess all of the following characteristics: (1) lateral rigidity and longitudinal flexibility; (2) a luminal surface of ciliated respiratory epithelium; (3) an adequate airtight lumen; (4) biocompatibility with adjacent tissues, so that chronic inflammation, granulation tissue, infection and erosion do not occur; (5) a straightforward and reproducible method for construction/development and insertion and, possibly, (6) no need for long-term immunosuppression.5,6
Over the years, different approaches to tracheal replacement have been attempted in the pre-clinical and even in the clinical setting; however, all these procedures have some limitations and, currently, none of them has yet become an established treatment option. Synthetic materials, in the form of solid or porous prostheses, may lead to an increased risk of granulation tissue formation, infection onset up to possible erosion of adjacent organs. 7 Currently, only single case-reports, where the replaced airway segment was limited to the larynx and upper trachea are available.8,9
Aortic allografts are more biocompatible than synthetic prostheses; however, lack of specific vascularization is a significant limit, being responsible for their possible degeneration; moreover, absence of lateral rigidity needs to be compensated by a stent, which may likely trigger concomitant complications for the patient. The most consistent clinical experience with aortic allografts was published by Martinod et al. in 2018. 10 This single-center uncontrolled cohort study reported about 20 patients with end-stage tracheal lesions or proximal lung tumors requiring a pneumonectomy. After radical resection of the lesions through standard surgery, in 13/20 patients’ airway reconstruction occurred by positioning a human cryopreserved aortic allograft (not matched by the ABO and leukocyte antigen systems) combined with a custom-made stent to avoid collapse. Favorable outcomes were observed for all 13 patients; in fact, stent removal was possible for 9 patients, at a mean of 18.2 months from surgery. At a median follow-up of 3 years 11 months, 10/13 patients (76.9%) were alive; 8 of them (80%) breathed normally through newly formed airways after stent removal. Regenerated epithelium and cartilage were observed. Despite encouraging the results are limited to a single center, hence, further investigations are required.
Tracheal transplantation is an appealing treatment option; however, it is a complex procedure, which requires multiple operations and a relatively long period of immunosuppression. Moreover, a consistent clinical experience with tracheal transplantation has been reported only by a single center. 11 In their series, Delaere et al. 11 reported a two-step procedure wherein the donor trachea was first wrapped around the recipient radial forearm fascia to allow for graft revascularization, and then orthotopically transplanted using the radial flap pedicle for vascular anastomoses. However, this approach has several drawbacks. First, immunosuppression is needed for a variable amount of time (from 4 to 6 months in their series), and the authors are still uncertain about the correct timing for withdrawal from immunosuppression (before or after orthotopic implantation). Second, there’s not enough evidence yet about the rate of success of this procedure. In fact, graft necrosis after withdrawal of immunosuppression is of particular concern. Out of five reported patients, this complication occurred in one patient while the graft was still in heterotopic position, resulting in abortion of the orthotopic implantation procedure; and in two additional patients after orthotopic implantation, resulting in scarring and shrinkage of the graft with loss of patent airway lumen. Third, long-term follow-up is still lacking, as the longest period from successful orthotopic implantation to last follow-up (documented by computed tomography scan of the airway) was 2 years. Autologous, composite tissue flaps represent another ingenious strategy for developing a hollow structure displaying similar dimensions/biomechanical properties than that of native trachea. A free fascio-cutaneous flap, vascularized by radial vessels, is arranged to form a tubular structure; contextually, the positioning of autologous rib cartilage strips between the skin and the fascia is adopted to provide structural rigidity. This composite system can be anastomosed directly to the healthy tracheal stumps, and mammary vessels are recruited for vascular anastomosis. Again, clinical experience with this reconstructive approach is limited to one single center. Apart from being technically demanding, the major drawback of this procedure is the lack of a respiratory epithelium and mucociliary clearance. According to the same Authors, it is likely that the resulting bronchial secretions retention was probably fatal for those patients who underwent more extensive airway replacement procedures. 12 Finally, tissue engineering (TE) approaches are based on manufacturing a biocompatible supporting structure (scaffold) that allows and promotes the growth and differentiation of the recipient’s cells, thus leading to a functioning neo-trachea upon implantation. 13 This approach would allow to overcome all the limitations associated with other tracheal replacement procedures; however, to date, its widespread use is hampered by significant issues including inadequate reepithelization, poor mechanical properties, insufficient revascularization and unsatisfactory durability. 14
Focusing on tissue engineered tracheal grafts, two broad categories of scaffolds initially attracted researchers’ attention: synthetic structures created de novo by different methods (electrospinning, casting or 3D printing), trying to mimic the structural/ultrastructural and mechanical features of the native tissues; allogenic decellularized tracheas from cadaveric donors. In accordance with clinical and pre-clinical studies, synthetic devices seem to be less prone in supporting autologous cells’ colonization than the biologic scaffolds do15,16; possibly, this event is related to the preservation of naive tissue microanatomy as well as structural and signaling components, while depleting the extracellular matrix (ECM) of all allogeneic cellular elements that could elicit an immune response.
Through chemical + physical strategies or chemical and enzymatic treatments + physical strategies it is possible to prepare structures with specific morphological characteristics, preserving the extracellular matrix composition and angiogenic factors, free from consistent donor cells and major histocompatibility complex (MHC) class I and II molecules (assuring for low immunogenicity); however, there is still no consensus in the optimal protocol to adopt, triggering the debate.3,17–19 Controversies regard time required for scaffold preparation (time-consuming?) as well as recellularization by autologous mesenchymal stem cells differentiated into chondrocytes and/or airway cells (required? feasible?). In addition, also the “decellularization grade” is under investigation: a completely decellularized support may not guarantee for good mechanical properties after implant.20–23 Hence, many Authors moved their interest toward partially-decellularized supports (removal of immunogenic cells and immunoprivileged chondrocytes preservation) but lacking in orthotopic transplantation studies as well as in long-term follow-up do not permit a clear methodological evaluation of protocols quality and effectiveness, constituting a significant limit within this research field.3,17,22
Considering clinical interest in engineered tracheal grafts, orthotopic studies on animal models of disease represent a fundamental step for tissue engineered constructs validation.20,24,25 In addition, whether performed on large animals mimicking human anatomy, it is possible to face challenges associated with scale-up of in vitro procedures and give a better idea of the in vivo obstacles in a clinically relevant translational model. 25 The aim of this extensive literature review is to provide a broad overview on preclinical studies considering the development, characterization, and implantation outcomes of decellularized tracheal constructs, eventually bioengineered with cells. Comparing decellularization strategies, specific constructs characteristics and in vivo results may guide researchers and clinicians toward the identification of devices with fully satisfactory features, overcoming limitations of currently available approaches (Supplemental Material − S1).
Anatomy of trachea
To successfully develop an ideal and functional tracheal graft, native trachea characteristics, from anatomy to biomechanics, must be considered and matched. 26 The trachea is a vascularized hollow tubular structure, laterally rigid (to prevent collapse) and longitudinally flexible (to follow head/neck movements). 27 It starts at C6 level, following the laryngeal cricoid cartilage, up to the carina, at T4; hence it can be divided in two segments: cervical (C6-C7) and thoracic (T1-T4). Trachea length is of about 10–13 cm in adults (average length, 11.8 cm; a bit shorter in females), and it is characterized by a typical D-shaped cross-section structure of 16–20 incomplete, horseshoe-shaped cartilaginous rings (hyaline cartilage) interconnected by intercartilaginous membranes. Posteriorly, it is limited by a membranous wall; between the membranous wall and the esophagus, it is identifiable the trachealis muscle running longitudinally. Its contraction triggers bending and tensile stresses in the cartilage, modulating airway diameter.28–30 Typically, it is possible to identify about two cartilaginous rings/per centimeter of trachea; each tracheal ring has an average of 4 mm in height and of 3 mm in thickness. The external diameter is of about 2.3 cm in the coronal plane and 1.8 cm in the sagittal plane in men, while 2.0 and 1.4 cm in women, respectively.29,30
The tracheal luminal mucosa is lined by a pseudostratified columnar epithelium, characterized by ciliated, brush, basal, and secretory cells (i.e. globet cells) on a basement membrane (i.e. airway epithelium). The fundamental function of the airway epithelium is to provide a barrier to counteract infection against inhaled pathogens and move foreign particulates out of the trachea. Specifically, this function is mediated by the secretion of a protective layer of mucus by globet cells and the mucous glands located in the submucosa. The mucus, containing mucins involved in host-response defense, is moved along the airways through the movement of the cilia (mucociliary clearance).27,30 To date, engineering the respiratory epithelium without triggering events as tissue granulation and tracheal stenosis remains a significant challenge. 31
As for vascularization, the arteries supplying the trachea approach the organ wall laterally, in a segmental fashion, anastomosing with the segmental arteries above and below. In correspondence of the intercartilagineous ligaments, the tracheal arteries branch into anterior and posterior branches surrounding the trachea and anastomosing with contralateral side arteries. The cervical trachea is supplied by the tracheoesophageal branches of inferior thyroid arteries, which branch off the thyrocervical trunk from the subclavian arteries; while the thoracic segment and carina are supplied by the bronchial arteries, branching directly from the aorta. Keen awareness of this peculiar arterial architecture is fundamental in trachea surgery: specifically, to preserve the lateral blood supply and limit necrosis of the trachea within 1–2 cm of the anastomosis site is mandatory to prevent tissue ischemia.28,30
Considering tracheal cartilage extracellular matrix (ECM), it is typically characterized by collagen fibers entrapping a matrix core of hydrated proteoglycans (PGs): along with age, PGs content shows a decrease in turn associated with an average tensile modulus increase. In addition, from tissue surface to depth, tensile modulus decreases suggesting the variation in collagen fibrils orientation. At the surfaces, collagen fibrils are tightly woven displaying a parallel disposition, whereas, in the middle of the tissue, the fibrils are perpendicular to the luminal and abluminal surfaces. 28 As for mechanical behavior, Roberts et al., 28 working on human 100 µm thick strips of tracheal tissue, detected a decreasing tensile modulus (Young’s modulus) with depth: the calculated values ranged from 13.6 ± 1.5 MPa at the level of the abluminal superficial zone up to 4.6 ± 1.7 MPa in the middle zone. Moreover, stress-strain curves were linear for strains up to 10% with minimal residual strain. 28 Studies by Pauken et al. 32 and Trabelsi et al. 33 showed a tensile modulus of 3.33 MPa in the central part of the trachea, while an average tensile modulus of 4.4 MPa.
Decellularization strategies and tracheal grafts development
Decellularization
Tissues’ ECM can be isolated from resident cells by decellularization strategies to serve as a non-immunogenic bioscaffold.34–41 However, despite a higher cells’ removal is associated to a lower risk in immune and inflammatory responses, decellularization methods efficiency also strictly depends on maintenance of the structural/ultrastructural features and density of the target tissue. 16 To date there is no gold-standard among decellularization strategies; the preferred methods for tissues decellularization vary and can be tuned along with tissues and organs specific characteristics including size, species, shape, thickness, and ECM density. 40 Specifically, it is possible to recognize (i) chemical treatments (e.g. non-ionic/ionic/zwitterionic detergents; acids and bases; hypertonic and hypotonic solutions); (ii) enzymatic treatments (e.g. nucleases (DNase/RNase); trypsin); (iii) physical treatments (e.g. freeze-thawing cycles; freeze-drying; sonication; vacuum; hydrostatic pressure; perfusion; shaking).19,42 These strategies can be adopted alone or combined (preferentially) to effectively remove donor cells from allogeneic or xenogeneic tissues while preserving both the structural proteins (e.g. collagen, laminin, and fibronectin) and the ECM-entrapped signaling/bioactive molecules (e.g. growth factors). The resulting product can in turn be safely implanted in the recipient, influencing cell mitogenesis/chemotaxis, directing cell differentiation and prompting host tissue remodeling.16,43
Considering the trachea, cartilage density is a prerequisite for a functional graft but also represents an obstacle to detergents and enzymes penetration requiring intense efforts in research. 23 The main issue concerns in the identification of a balanced protocol which is expected to show efficiency in cells removal and “respectfulness” toward ECM architecture, to avoid that structural instability leading to airway obstruction up to collapse after implant.21,27,44,45 As documented by the numerous studies in the literature, the protocols developed for tracheal decellularization thus leading to ready-to-implant grafts can be classified in (i) Chemical + physical strategies (Table 1); (ii) Chemical and enzymatic treatments + physical strategies (Table 2). Together with soaking into enzymatic and/or chemical solutions, all the Authors facing tracheal decellularization highlighted the importance of imparting physical treatments. Mechanical agitation (i.e. shaking), according to intensity, promotes homogeneous exposure to the decellularizing media, cells rupture and detachment, as well as the removal of cellular remnants. Furtherly, different other physical treatments can be combined for results optimization.19,46
Development of tracheal grafts by “chemical treatments + physical strategies.”

dH2O: distilled water; DI H2O: deionized water; DNA: deoxyribonucleic acid; ECM: extracellular matrix; Et-OH: ethanol; F/T: freeze thawing; h: hour; HE: hematoxylin and eosin; NaCl: sodium chloride; NH4OH: ammonium hydroxide; NR: not reported; ON: overnight; PAA: peracetic acid; PBS: phosphate buffered saline; P/S: penicillin/streptomycin; PSS: physiological saline solution; rpm: revolution per minute; RT: room temperature; SDS: sodium dodecyl sulfate; SEM: scanning electron microscopy; v/v: volume/volume.
Development of tracheal grafts by “chemical and enzymatic treatments + physical strategies.”.

AA: antibiotic/antimycotic; BMSCs: bone marrow stem cells; CAM: chicken chorioallantoic membrane; Col-II: collagen type II; CTRL: control; DAPI: 4′,6-diamidino-2-phenylindole; dH2O: distilled water; DNA: deoxyribonucleic acid; DNase: deoxyribonuclease; ECM: extracellular matrix; EDTA: ethylenediaminetetraacetic acid; F/T: freeze thawing; GAG: glycosaminoglycans; Gent: gentamycin; h: hour; HE: hematoxylin-eosin staining; H2O: water; IF: immunofluorescence; IHC: immunohistochemistry; MgCl2: magnesium chloride; MHC: major histocompatibility complex; min: minutes; NaCl: sodium chloride; NR: not reported; PBS: phosphate buffered saline; PCR: polymerase chain reaction; P/S: penicillin/streptomycin; RNase: ribonuclease; rpm: revolutions per minute; RT: room temperature; SDC: Sodium deoxycholate; SDS: sodium dodecyl sulfate; SEM: scanning electron microscopy; SLES: sodium lauryl ether sulfate; UTS: ultimate tensile stress; VAD: vacuum-assisted decellularization; vs: versus; w: week; γ: gamma; ↓: reduced; ↑: higher.
As reported in Tables 1 and 2, sonication/ultrasonication, freeze-drying, freeze-thawing, vacuum, heat shock and hydrostatic pressure were broadly documented for tracheal grafts preparation. Sonication/ultrasonication are associated to the generation of acoustic cavitation bubbles inducing shear stress effect up to cell membranes rupture; in addition, the vibrations promote decellularizing agents’ penetration, also helping in cells debris removal. Unfortunately, high power or longer duration of the treatment could be associated to structural fibers disruption. 19 Freeze-drying or lyophilization is a method consisting in removal of ice-crystals by sublimation and desorption from a tissue/material previously frozen. As a result of intracellular ice crystals formation, this process is likely associated to cell membranes disruption and fragmentation of the genetic material up to cell lysis. During rehydration, the tissue tends to adsorb fluids more with possible ECM damage; furtherly, it requires to be matched with another process to remove cellular debris. 47 Freeze-thawing (thermal shock) is based on intracellular ice crystals formation, provoking cell membranes disintegration up to cell lysis and detachment from the ECM architecture. The cooling/thawing rate, the temperature ranges up to the number of cycles likely affect the method efficacy. Contextually, ice crystals may irreversibly damage ECM ultrastructure and further treatments are often desirable to remove cells remnants. However, it eases a uniform decellularization.19,46,48 A snap freezing is preferrable as it has no significant negative impact on the structure. 48 Vacuum facilitates the penetration of chemical agents within the tissue. It is not a decellularization approach itself, but it strongly supports the process in association with other agents. 48 Hydrostatic pressure imparts high pressure to the tissues thus provoking cells lysis; as an excessive pressure may induce ECM structure damage, a careful attention is required when recurring to this strategy. 48 Osmotic shock is based on treatment with hypotonic and hypertonic solutions; it provokes cellular lysis but, as cells residues are released within the matrix, further supportive treatments are required. 49
Chemical + physical strategies
Chemical treatments adopt detergents/chemicals to induce cellular bonds disruption up to cellular components removal. Considering tracheal tissue, the resort to chemicals alone (no enzymes) was attempted by Dang et al.,3,17 Kutten et al., 20 Liu et al., 22 Wood et al., 50 Hung et al., 51 and Tan et al. 52 Specifically, the solutions consisted in detergents (sodium dodecyl sulfate (SDS) (ionic) and Triton X-100 (non-ionic)), hypertonic solutions (sodium chloride (NaCl)), acids (peracetic acid), bases (ammonium hydroxide (NH4OH)) and organic solvents (ethanol), alone or combined within more complex protocols. Regarding the physical treatments, agitation (broadly recommended by the Authors) was also eventually associated with sonication/ultrasonication,3,17,51 freeze-drying, 51 freeze-thawing,20,50 and vacuum. 20
A tight comparison between the different approaches (Table 1), highlighting similarities and differences, can guide toward a critical analysis and conscious interpretation of in vivo results. Hung et al., 51 similarly to Dang et al.3,17 reported about rabbit tracheas yared; despite effectiveness in epithelium and submucosa cells removal, the cartilaginous component often maintained chondrocytes within the lacunae.
Chemical and enzymatic treatments + physical strategies
Seeking for a satisfactory decellularization grade of the tracheal tissue, a major part of the Authors recurred to miscellaneous approaches where chemical and enzymatic treatments were combined to physical strategies. The enzymes used included the DNase-I,1,19,53–57,60 eventually mixed with the RNase58–60 or trypsin. 18
As reported in Table 2, the nucleases (DNase, RNase) were preferentially associated with SDC1,53–58,60 (also combined with Triton X-100 in Maughan et al. 59 ). The choice of sodium lauryl ether sulfate (SLES) (a novel anionic detergent with a structure like that of SDS) combined with DNase-I was also experienced for the first time. 19
Comparing the different methods (Table 2), it stands out that the favorite SDC % was set to 4%,1,18,53–57 mainly for an exposure time of 3–4 h.1,53–57 Lower percentages were reported by Batioglu-Karaaltin et al., 58 Maughan et al., 59 and Sun et al. 60 who preferred a complex solution (0.2–0.25% w/w SDC + 0.2–0.25% w/w Triton X-100). As expected, to balance the reduced detergents concentration, the time of exposure was extended up to 24 h. A further consideration may concern the consequentiality of the different phases: all the Authors proceeded with detergent first, followed by nucleases treatment.1,18,19,53,55–60 Differently, Jang et al., 54 after storing the samples in milliQ water (4°C/48 h), incubated the rabbit tracheas in a single solution consisting in 2000 kU DNase-I in 4% SDC+1 mol/lNaCl for 4 h; while Ohno et al. 61 distinguished for a decellularization strategy based on nuclease + chelant instead of detergents. Briefly, the tissues were washed with saline containing 40,000 U/L DNase-I + 20 mM MgCl2 (2 weeks) and then soaked in saline with 2 mM EDTA (2 weeks), followed by washing with saline (1 week).
Regarding the physical strategies adopted to boost acellular grafts preparation, immersion in active solutions under agitation was combined with other techniques including the impartment of osmotic and heat shock, hydrostatic pressure, up to ultrasonic bath and vacuum recur. Osmotic shock in distilled water was mainly applied prior to begin with decellularization1,19,53–57 or, eventually, after a first freezing (heat shock). 58 For Villalba-Caloca et al., 18 Zhang et al., 19 Maughan et al., 59 and Sun et al. 60 it was an intermediate phase; while, for Zhou et al., 56 immersion in deionized water was both the first step in decellularization and the last step of each cycle, specifically consisting in 4% SDC (25°C/4 h), 50 kU/mL of DNase-I in 1 M NaCl (37°C/3 h). Together with osmotic and temperature shock, other physical processes included constant agitation, 59 high-hydrostatic pressure, 61 ultrasonic bath, 18 and vacuum. 60
To date, the approaches based on detergents and enzymes are the preferred ones for trachea decellularization, showing to be effective in cells removal while better preserving the ECM structure and biomechanical characteristics 47 ; however, as reported in Table 2, the number of cycles (range: 1–20 cycles), the time required to obtain the graft (range: 23 h-12 weeks) as well as the decellularization grade (complete? partial?) are still under discussion. Both partial and complete decellularizations were performed.
Verification of decellularization grade
Decellularized tracheal grafts characterization is mandatory before orthotopic implant. Several factors including native tissue cells density, matrix thickness, lipid content, species of origin (small or large animals) may influence decellularization efficiency; hence, a protocol previously proved to be effective requires to be validated whether applied to a tissue with different characteristics. 42 The major concerns of all decellularization protocols remain immunogenicity and ECM alteration: cellular material removal while retaining scaffold functionality are the goal to pursue. 62
Immunogenicity
No decellularization protocol can completely remove cellular materials, so much so that also commercially available biologic scaffolds show presence of small quantities of DNA remnants. 46 Those cells residues may remain entrapped within the ECM ultrastructure in turn affecting in vitro cytocompatibility and/or in vivo immunogenicity.23,63–65 Thus, quantitative verification of cell residues, including double-stranded DNA (dsDNA), is paramount for biologic scaffolds characterization and for effectiveness forecast46,62; specifically, <50 ng of dsDNA per mg of tissue (dry weight) and less than 200 base pair of DNA in length is the minimal criterion that satisfies the intent of decellularization.16,66,67
In addition to cellular leavings, eventual immunogenic response can be also triggered by antigens; typically, these include the superficial epitopes α-Gal and the major histocompatibility complexes (MHC). 62 Currently, no tissue treatment has proven ability in masking or inactivating them; however, their reduction must be sought before implantation in the recipient to avoid immune rejection. 64 While α-Gal is the main mediator of hyperacute rejection and it must be considered in case of xenotransplants, the MHC molecules (MHC-I, II) represent the most critical intermediary of chronic rejection, being potent mediators of both innate and adaptive immune responses in allografts and xenografts. Both α-Gal and MHC molecules may trigger those mechanisms ultimately leading to graft degeneration and failure. 68
Considering decellularization of trachea, DNA quantification,19,22,60,61 tissue sections staining by histology,18,20,22,51,55,57,58,60,61 immunohistochemistry,19,55,60 fluorescence (i.e. vital staining/DAPI)1,3,17–19,60 but also SEM19,22,59 and polymerase chain reaction (PCR) studies 58 were performed to discriminate whether the protocol adopted was suitable to achieve a satisfactory tissue decellularization grade. Occasionally, morphometric studies considering the number of residual cells were also associated with, for completeness.57,60 Specifically, Ohno et al., 61 Sun et al., 60 and Zhang et al., 19 resorting to chemical and enzymatic treatments + physical strategies (Table 2) based on DNase-I/EDTA + pressure (pig trachea, 1 cycle/5 weeks), Triton X-100/SDC/DNase-I/RNase + vacuum assisted decellularization (VAD) (rabbit trachea, 1 cycle/56 or 64 h) and SLES/DNase-I + shaking (rabbit trachea, 1 cycle 18 h), achieved a “complete” (threshold: DNA < 50 ng/mg) decellularization of the segments, with a residual DNA amount of 30.9 ± 7.2, 29.65 ± 3.63–38.29 ± 4.08, and 40 ng/mg, respectively; cartilage and epithelium were both considered. Within the same group (i.e. Table 2), despite not providing DNA quantification data but other verification studies, complete decellularization was also reported by Batioglu-Karaaltin et al., 58 showing a 90% acellular cartilage and acellular epithelium (methods: histological analyses and PCR for Sox2); Ershadi et al., 55 proving the presence of few residual chondrocytes only (no reported data for the epithelium) (methods: histological analyses and MHC I/II detection by immunohistochemistry); Maughan et al., 59 revealing no cells in both cartilage and epithelium (methods: SEM analyses); Villalba-Caloca et al., 18 showing few but well preserved chondrocytes and complete epithelium loss (methods: histological analyses and DAPI).
Together with complete decellularization discussed above, experimental studies referring about a partial decellularization of the trachea in ECM-bioscaffolds preparation were also numerous: interestingly, both chemical + physical strategies (Table 1)3,17,20,22,51,chemical and enzymatic treatments + physical strategies (Table 2)18,60 may lead to uncomplete cells removal. Liu et al. 22 (mouse trachea), adopting SDS/Triton X-100 + shaking, quantified the DNA content in tissue samples after 1 cycle/3 days thus verifying that genetic material remained above the “ideal” limit (~1300 ng/mg vs 50 ng/mg). Epithelium and submucosa were removed while chondrocytes decreased but remained nucleated. As for the others, different characterization methods were preferred (histology, fluorescence) all ascertaining that residual cells were still identifiable within the cartilaginous matrix.
Developing a full-thickness acellular trachea represents a challenge in TE. Epithelium removal or acellular epithelium set-up is often reported after few decellularization cycles; however, within the same protocol, cartilage tissue tends to preserve chondrocytes. This evidence often leads researchers to increase decellularization cycles number or prefer more “aggressive” protocols with the risk of affecting ECM integrity. In consideration of this, partial decellularization was regarded as a possible chance: the trachea is characterized by a three-layered structure; hence, there might be a certain variability in antigenic properties among them. The mucosa and the connective tissue mainly show cells presence and removing them likely reduces trachea antigenicity. 69 Conversely, cartilage, lacking in blood vessels and with lacunae/chondrocytes dispersed within a dense collagen-proteoglycans ECM, results an “immune privileged” component, not eliciting severe immune-reaction in the recipient.51,57
Having residual donor cells in the tissue to graft is less favorable whether considering safety. It descends that intense efforts are required in decellularization processes set-up, in order to guarantee for chondrocytes removal before translation to medicine of such strategies. 51
ECM structural characteristics maintenance
Among the main challenges possibly associated with decellularization, the significant compromission of the tissue mechanical properties stands out. Thus, determining the resulting tracheal biomechanics (descending from ECM morphological/structural features) is essential when describing preparation of decellularized tracheal grafts, as this feature may predict eventual risk for collapse.
Considering that native-like substitutes are regarded as ideal, 21 cartilage integrity maintenance is fundamental to this purpose. Strong of this, many Authors highlighted the possible advantages descending from partial decellularization, 22 idea that clashes with eventual immune-related issues, as discussed above. Whether in presence of a fully decellularized tissue, Villalba-Caloca et al. 18 suggested that a preliminarily recellularization with chondrocytes in vitro, leading to a complete recellularization, may be the solving-approach to avoid structural integrity loss and fibrosis at the anastomosis site. Despite Authors’ awareness on decellularized trachea mechanics importance, only Hung et al. 51 and Batioglu-Karaaltin et al. 58 reported numerical data about these evaluations after rabbit tracheas decellularization by chemical + physical strategies 51 or chemical and enzymatic treatments + physical strategies. 58 Hung et al. 51 reported a maximum strength under compression of 327.8 ± 125.30 kPa and a Young’s Modulus of 1.54 ± 0.655 MPa; while Batioglu-Karaaltin et al. 58 achieved a tensile strength of 3937.6 ± 57, 3577.6 ± 108,and 1760.8 ± 21 kPa for upper, middle and lower tracts of the segment. In both studies no significant differences were detected versus the native control.
Tissues ultrastructure/microstructure have mechanical implications also correlating with macroscopic behavior and functions.70,71 In addition, the microenvironment also plays a pivotal regulative role toward mechanosensitive cellular activities (i.e. adhesion, migration, solute transport, mechanotransduction), 72 in turn exerting a fundamental role whether considering scaffold repopulation. According to these evidences, the arrangement of the acellular trachea ultrastructure, monitored by SEM, was advised by some Authors.19,60 Zhang et al. 19 determined the impact of SLES on tissue structure, highlighting that 2% SLES destroyed the mucosa and the collagen fiber in the submucosa, although the basement membrane remained intact in some groups. In 0.5%−0.05% SLES adventitial surfaces was showed to remain intact. Sun et al. 60 described cells density variation along with decellularization protocol phases modulation; the arrangement of the collagen fibers at the basement membrane was also disclosed, unraveling absence of structural alteration descending from vacuum (physical method assisting decellularization).
ECM is a highly dynamic and complex meshwork of proteins 73 ; specifically, considering trachea, key ECM proteins whose preservation is fundamental to achieve biomechanical support and matrix micromechanics maintenance are GAGs, type II collagen, laminin, fibronectin22,74 (Figure 1).

Macroscopic (a–c), microscopic (d–n) and ultrastructural appearance (o–t) of native and decellularized tracheal segments from pig. Specifically, two protocols were here considered, based on SDS and Tergitol™, respectively. Both methods consisted in: soaking in MilliQ water (24 h/+ 4°C); DNAse + NaCl 1M (3 h /RT under stirring); trypsin + EDTA in PBS (1 h/37°C); SDS or Tergitol™ + NH4OH in PBS (96 h/4°C under stirring); MilliQ water (72 h/4°C). According to samples gross appearance (a–c), decellularization conferred to the tracheal segments the typical white color. Inside the lumen, the respiratory epithelium was clearly identifiable as a continuous layer. Considering the lumen patency, a slight modification was observed in the SDS-treated segments; a possible stiffness reduction may be specifically ascribed to the detergent used. Histological analyses of the cartilaginous tissue allowed to prove cells removal and extracellular matrix (ECM) microscopic appearance after decellularization. As preliminarily showed by hematoxylin and eosin (H&E) staining (d–f), empty lacunae were identified in both the treated samples versus the native tissue (control); contextually, ECM appeared preserved in integrity, as showed by Masson’s Trichrome (collagen) (g–k) and Alcian Blue (glycosaminoglycans) stainings (l–n), furtherly confirming chondrocytes removal. Scale bars: 100 µm. Scanning Electron Microscopy (SEM) analysis of the native and decellularized tracheas, allowed to highlight and compare the specific ultrastructural features of the tissue; the outer and inner layers were considered (o-t). The protocol based on Tergitol™ leads to smoother surfaces than SDS which determines the exposure of the collagenic component appearing as a network; this may suggest a more “aggressive” behavior of the detergent with possible superficial erosion of the ECM.
GAGs are a family of linear, negatively charged carbohydrates with a repeating disaccharide unit; according to the repeating disaccharide structure and sulfation level, the GAGs include: heparan sulfate, chondroitin sulfate, keratan sulfate and hyaluronic acid. The GAGs residing within the ECM are implied in cells-ECM interactions and tissue biomechanical properties maintenance; controlling hydration and swelling pressure, the GAGs permit tissues to absorb compressional forces. In particular, the sulfation patterns play crucial roles in ionic interactions with growth factors/cell surface receptors/enzymes/cytokines/chemokines/proteins that are associated with biological processes (development, disease, cell growth and differentiation). 73 GAGs adequate content avoids tracheal stenosis after transplantation. 75 Type II collagen belongs to collagens family that are fibrous proteins typically characterized by long, stiff, triple-stranded helical structure, made up of three α chains wound around each other; proline, hydroxyproline and glycine residues are highly represented in the strands. Specifically, type II collagen is fibrillar-like; it is formed by three polypeptide chains interacting together to form a right-handed helical structure. 76 Considering the airways cartilage, it represents 95% of total collagen. Despite being directly associated to tissue mechanics, it also facilitates chondrocyte synthesis of ECM. GAGs and type II collagen and are both important for cartilage matrix homeostasis. 77 Fibronectin is a large adhesive glycoprotein; it consists of a dimer made of two subunits linked by disulfide bonding; laminins are large cross-shaped flexible complex of three polypeptide chains held together by disulfide bonding. 78 Fibronectin and laminins both preside at cell attachment and vascularization. 77 Histological verification of GAGs, type II collagen, laminin, fibronectin presence and distribution were widely reported by Authors facing trachea decellularization,1,18,19,22,57,60 consisting in a fundamental methodological approach to evaluate and compare methods effectiveness. In addition to histology, Zhang et al., 19 Zhong et al. 57 and Sun et al. 60 also adopted immunofluorescence with a focus on collagen type II19,57,60 and laminin. 60 Consistently, together with histological characterization based on “staining intensity,” proteins content was quantified.1,19,57,60
Among the Authors embracing the chemical + physical strategies, Liu et al. 22 referred that decellularized tracheas were similar to the native sections regarding collagen and GAGs intensities at histology. Moreover, according to mass spectrometry data, key ECM proteins were all confirmed to be maintained. As for the Authors supporting the chemical and enzymatic treatments + physical strategies, Sun et al. 60 showed the maintenance of tracheal structural integrity (Masson’s trichrome staining), but reduction in proteoglycans (Alcian blue staining) versus native tissue. While total collagen content was not affected by VAD treatment, the GAGs were significantly reduced (range: 7.22 ± 0.19 - 5.09 ± 0.57 µg/mg; p < 0.01) compared to the native tissue (11.32 ± 0.52 µg/mg). Immunohistochemical analyses highlighted that Col-II and laminin and b-FGF were still preserved in the mucosa and submucosa (laminin, b-FGF) and cartilage (Col-II). Differently, Villalba-Caloca et al. 18 after 7 or 15 decellularization cycles highlighted a paler tissue with separated collagen fibers. Destruction of the trachea gross structure was also evidenced by Zhang et al. 19 by HE. This event occurred after trachea treatment with 2% SLES (1 cycle, 18 h); the data were corroborated by Masson’s trichrome staining. Conversely, collagen was reserved after 0.05%–1% SLES treatment. A gradual decline was also observed in GAGs levels within the cartilaginous compartment, along with SLES concentration. IHC technique was adopted for Col-II content verification, after decellularization. The protein was mainly located in the cartilage and, intriguingly, 0.25%, 0.1%, and 0.05% SLES groups displayed nearly normal levels in Col-II. The Authors identified slightly reduced Col-II levels without differences in total collagen amount comparing decellularized and native tissues. Zhong et al. 57 did not show significant differences in type II collagen at both immunofluorescence and ELISA (29.36 ± 0.93 µg/g dry weight vs 33.00 ± 2.04 µg/g; p < 0.05) after 7 decellularization cycles.
The decellularization process inevitably triggers the risk of ECM proteins depletion that may consequently determine the in vivo adverse outcome of the implant, due to tissue poor mechanical properties. According to our knowledge, decellularized tracheas approached by chemical and enzymatic treatments + physical strategies are likely more prone to this risk, even though chemicals concentration and cycles number/extent in chemical treatment + physical strategies have a significant role.
Supportive strategies for trachea strengthen
To reduce the ECM structural alteration, with higher tissue strengthen thus compensating for the GAGs loss that may descend from decellularization, multiple exogenous cross-linkers have been reported in literature, classified as (i) chemical crosslinking agents and (ii) natural crosslinking agents. The chemical crosslinking agents include, for instance, glutaraldehyde (GA), carbodiimide (1-ethyl-3-(3-dimethyl aminopropyl)- carbodiimide (EDC)), epoxy compounds, six methylene diisocyanate, glycerin and alginate; the natural crosslinking agents, superior in terms of lower cytotoxicity and anti-calcification ability, include genipin (GP), nordihydroguaiaretic acid (NDGA), tannic acid and procyanidins (PC). 79
Recurring to tissue crosslinking after decellularization descends from the need to identify an ideal method for stabilization of mechanical integrity and natural compliance of collagen-based scaffolds.75,80 However, referring to trachea, caution must be observed. Stiffening of the airway ECM is a core pathological change sufficient to drive excessive bronchoconstriction, even in the absence of inflammatory signals. 81
According to our knowledge, the adoption of the synthetic fixative GA (0.5% w/v, for 7 days at 4°C, pH = 7.4) 18 or the natural crosslinker genipin (1% w/v) 57 was reported for decellularized tracheas preparation, before orthotopic implant.
GA is undoubtedly one of the most widely used crosslinkers for proteins; it reacts with the amino groups leading to a more tightly crosslinked ECM network with a significantly improved tensile strength and pliability and reduced antigenicity of the tissue. GA crosslinking can also make scaffolds non-resorbable and non-susceptible resisting to matrix metalloproteinase. However, it does not protect against elastase that may sustain the onset of an inflammatory environment. 82 In addition, the GA toxicity and GA-induced calcification may determine a final failure of the implant promoting the adoption of detoxifying strategies and specific treatments to increase the biocompatibility/durability/effectiveness of the scaffolds. 83
Genipin is an iridoid compound with several hydroxyl and carboxyl active groups. It derives from the geniposide which is extracted from the fruit of Gardenia jasminoides Elli. Reacting with the free lysine, hydroxyl lysine and arginine amino groups it can lead to annular crosslinking, which is more stable than the reticular crosslinking formed by GA. Furthermore, genipin-crosslinked ECMs are associated to a lower inflammatory response than GA and less substance release during preservation.79,83 Unfortunately, the dark blue aspect of genipin-treated samples together with the high costs mainly related to its production, may discourage from its adoption.
Comparing the acellular, crosslinked tracheas characteristics/outcomes, Zhong et al. 57 highlighted the genipin-based method effectiveness in graft preparation. No structural variations were observed, except for denser elastic fibers after the treatment. The animals (rabbits) implanted with the developed substitutes were stable after surgery without showing difficulties in breathing and/or inflammatory reactions. Conversely, an unfavorable result was associated to Villalba-Caloca et al. 18 experience. The Authors, approaching the acellular trachea crosslinking by GA (i.e. 7 decellularization cycles + GA for 7 days), obtained tissue substitutes not different in outcomes from the other groups considered within the study (15 cycles decellularized tracheas; 15 cycles decellularized tracheas + surgical wire reinforcement; 7 cycles decellularized tracheas; 7 cycles decellularized tracheas + cryopreservation). Focusing on macroscopic/microscopic findings after decellularization, all samples showed necrotic changes and decreased length. Additionally, the rings were pale with epithelium total loss and separated collagen fibers. The survival time of the implanted animals (swines) was the higher for samples crosslinked with GA (13.33 ± 1.97 days) than the others, but post-mortem findings revealed scattered areas of preserved epithelium in the submucosa, cartilage degeneration signs together with disorganized collagen fibers and chronic inflammation evidences. Considering no substantial difference among groups, no specific correlation with GA treatment can be assumed but neither excluded. Possibly, the ECM crosslinking, together with the lower number of decellularization cycles (7 instead of 15) assured for better mechanical features of the grafts and, in turn, to their longer in vivo permanence.
Sterilization and disinfection methods
Non-sterile conditions, occurring while harvesting xenogenic tissues and/or during manipulation phases associated to decellularization, could influence the levels of ECM-derived tissues bioburden. Thus, particular attention must be paid whether the decellularized scaffolds are prepared for in vitro biological assays and/or in vivo experiments, as heterotopic and orthotopic implant.
Sterilization is the process of killing all microorganisms, while disinfection is the process of killing or removing all kinds of pathogenic microorganisms except bacterial spores. 84 To date, systematic methods for decellularized ECMs sterilization/disinfection have not been reported and few studies regard effects of these approaches on decellularized ECMs. 84 A sterile/disinfected ECM is required to be non-toxic while maintaining physical, chemical and biological properties. Among sterilization methods, irradiation (gamma (γ)- and beta (β)- irradiation), ethylene oxide (EO), peracetic acid (PAA) (under specific conditions), hydrogen peroxide low-temperature plasma (HPLP) have been adopted; whereas, disinfection methods include PAA (under specific conditions), peroxide, alcohol, UV, supercritical carbon dioxide (ScCO2).
Along with composition (types of proteins), structure/size (thickness of the specimen) and function (end use destination) of the decellularized ECMs, the sterilization/disinfection approaches must be modulated. However, revising the literature, it’s clear that different strategies have been applied to the same tissue/organ, without any specific reference criterion. 84
According to our knowledge, the sterilization and disinfection methods for acellular trachea preparation, in the perspective of an orthotopic implant, mainly included: treatment with antibiotic (e.g. penicillin, streptomycin, gentamicin),3,17,51 eventually added in antimycotic (e.g. fungizone)19,54–58,60; soaking in PAA/ethanol 50 ; γ-irradiation (25 kGy; 10 kGy)18,59; immersion in PAA/ethanol + γ-irradiation (20 kGy). 20
Antibiotics are often used to sterilize decellularized ECMs. They can act according to several mechanisms depending on the molecule considered. In particular, the following molecules can be recognized: β-lactams (e.g. penicillin) and polypeptide antibiotics (vancomycin); aminoglycosides (e.g. streptomycin and gentamicin); macrolide antibiotics (e.g. erythromycin and azithromycin) and lincosamides (e.g. clindamycin); quinolones (e.g. ofloxacin); amphotericin B. Despite not showing effect on mechanical properties, structure and components of decellularized ECM, the antimicrobial spectrum of each antibiotic is limited (even in combination) (e.g. mycoplasma). Moreover, possible toxic effects toward cells cannot be excluded.
PAA (CH3C(O)OOH) belongs to the organic peroxides; it is a commonly used disinfectant, but it can guarantee for sterilization under certain conditions, depending on concentration/exposure time. Its decomposition products include acetic acid, water and oxygen that are “safe,” thus PAA is not toxic; moreover, it has a wide spectrum of microbial activity (comparable to chlorine). 85 Unfortunately, it has strong oxidation and acidity which may affect the physical and chemical properties of some matrices. 84
Ethanol disinfects the substrates (not sterilize) by protein denaturation and microorganisms’ enzyme system destruction. It is broadly used as it does not affect ECM structure in a significant manner but it can reduce collagen content.
Irradiation is not linked to eventual residual toxicity but it may affect physical and chemical properties of the ECM-derived scaffolds as well as bioactivity. In particular, γ-irradiation, commonly performed at 25 kGy (Sterility Assurance Level of 10−6) could reduce the mechanical strength of collagen-containing tissues also increasing the resistance toward enzymatic degradation. 86
Tissue substitute disinfection/sterilization is essential to be successful; hence, to avoid the risk of failure in surgery, intense efforts are still required for the establishment of a rigorous methodological approach beyond effective decellularization.
Cell repopulation
Cell-free ECM, still preserving native tissue structure and adequate mechanical features, is the product resulting from optimal decellularization. Thus, the scaffold is expected to support re-population that may preliminarily occur in vitro or post-implantation by the patient’s own cells migration. However, considering that autologous cells migration with consistent ECM deposition may take long time, this phase is particularly delicate for scaffold survival as collapse and loss of function may likely occur.
Whether approaching a pre-implant seeding, several aspects need to be considered including the most adequate cell source to choose (stem cells, differentiated cells), technical difficulties regarding cells isolation and expansion, seeding and culturing methods; the long times that these procedures take are also a significant drawback. Focusing on the different cell populations used for preliminary colonization of the tracheal scaffolds intended for orthotopic implant, experience is reported with: mouse EGV-4T cells; mouse iPS-MEF-Ng-492B-4 or mouse iPS-Hep-FB/Ng/gfp-103C-1 cells 56 ; adipose MSCs50,58; bone marrow MSCs 19 also with bone marrow mononuclear cells 51 ; nasal epithelial cells sheets 17 ; endothelial cells induced from differentiated bone marrow cells 60 ; chondrocytes from bone marrow MSCs and epithelial cells 53 ; amniotic MSCs then differentiated toward chondrogenic lineage. 1 The seeding side is also distinguished, with chondrocytes/derived chondrocytes and epithelial cells or MSCs seeded externally or internally, respectively (Tables 3–6). It is easily inferable that seeding chondrocytes externally may promote cartilaginous matrix strengthness, possibly affected by decellularization; whereas, seeding epithelial cells onto the luminal side before implant may promote and guide epithelialization. In addition, the adoption of systems like bioreactors may be essential to guarantee for optimal cells distribution and adhesion. Within this complex scenario, some authors demonstrated that cell-free scaffolds may be successful too; hence, any paradigm still exists, and different approaches are reported with different success degree, that may be dependent form several critical factors including the animal species, the defect type/length. 62
Orthotopic implant of tracheal grafts in mice and rats.

CT: computed tomography; d: day; GFP: Green Fluorescent Protein; IF: immunofluorescent/immunofluorescence; IHC: immunohistochemistry; iPS: induced pluripotent stem cells; K: keratin; M: macrophages; MRI: magnetic resonance imaging; n: number; NR: not reported; PET/PU:PGA: electrospun polyethylene terephthalate/polyurethane:polyglycolic acid; w: week; >: higher; ↑: increased; ┼: death.
Orthotopic implant of tracheal grafts in rabbits.
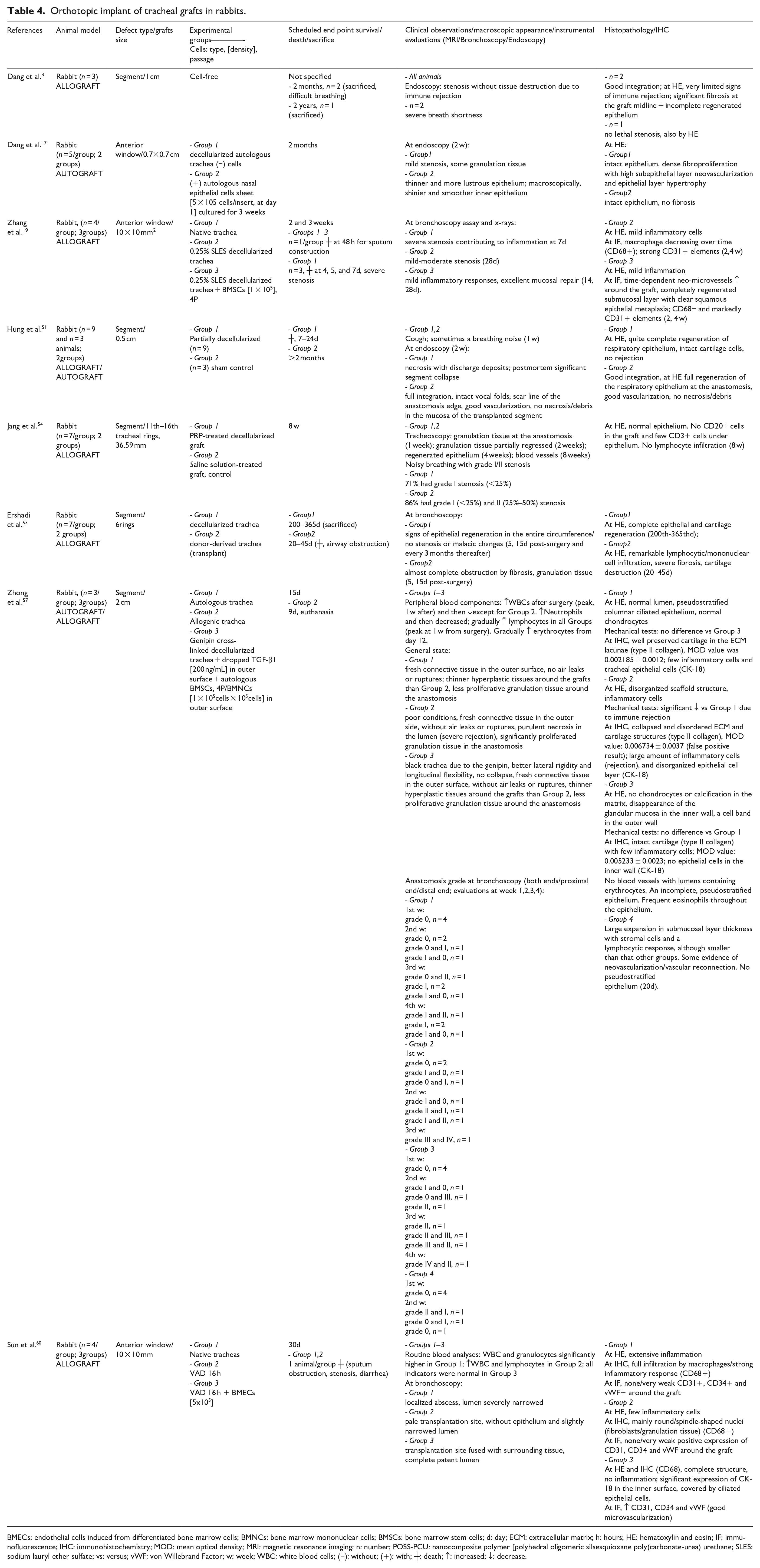
BMECs: endothelial cells induced from differentiated bone marrow cells; BMNCs: bone marrow mononuclear cells; BMSCs: bone marrow stem cells; d: day; ECM: extracellular matrix; h: hours; HE: hematoxylin and eosin; IF: immunofluorescence; IHC: immunohistochemistry; MOD: mean optical density; MRI: magnetic resonance imaging; n: number; POSS-PCU: nanocomposite polymer [polyhedral oligomeric silsesquioxane poly(carbonate-urea) urethane; SLES: sodium lauryl ether sulfate; vs: versus; vWF: von Willebrand Factor; w: week; WBC: white blood cells; (−): without; (+): with; ┼: death; ↑: increased; ↓: decrease.
Orthotopic implant of tracheal grafts in pig.

BMMSCs: bone marrow mesenchymal stem cells; HE: hematoxylin and eosin; IHC: immunohistochemistry; n: number; w: week; Ø: diameter; ↓: reduction; ↑: high; >: greater.
Orthotopic implant of tracheal grafts in dogs and fetal lambs.

d: day; ECM: extracellular matrix; GAG: glycosaminoglycans; GFP: Green Fluorescent Protein; h: hour; HE: hematoxylin and eosin; min: minutes; MSC: mesenchymal stem cells; n: number; ↑: increased; ↓: reduced; Ø: diameter; ┼: death.
In particular, while considering trachea, achieving a successful re-epithelialization of de-epithelialized tracheal constructs still remains a significant challenge for tracheal graft success. 87
The specific outcomes referring to tracheal scaffolds seeding are reported in the paragraphs below.
Vascularization of the tracheal graft
A critical issue when resorting to tissue engineering approaches is that of restoring graft/organ vascularization. The establishment of an adequate blood supply is essential to support any graft survival, being responsible for nutrients supply to seeded cells and/or to native/endogenous cells growing into the engineered tissue.
Unlike other organs, the trachea does not possess a discrete vascular pedicle to be used for anastomosis, but it shows a finely segmental blood supply, as described above. After positioning the tissue engineered tracheal scaffold in the recipient, vascular connections supporting cells growth and tissue integration are relatively slow to be established. In fact, whether no specific measure is adopted to provide vascularization, neo-angiogenesis from the graft edges in contact with the recipient blood vessels is the only mechanism supposed to occur. The evidence for this principle finds confirmation in the studies conducted by Delaere et al. 11 Looking for tracheal repair optimization, the researchers refined a two-step procedure for ideal trachea allograft development consisting in (a) tracheal segment heterotopic implant (recipient forearm, under immunosuppressive therapy), to trigger its revascularization and re-epithelization, followed by (b) graft orthotopic anastomosis, recurring to the radial vascular pedicle as blood source. Interestingly, while waiting for revascularization (first phase), the authors noticed a high risk of necrosis for the grafts portions that were more distant from recipient tissues. The time necessary for full revascularization was 2 months; however, smart strategies to use in order to boost the ingrowth of recipient blood vessels may include engraving the allograft intercartilagineous ligaments or covering the luminal surface of the graft with the recipient’s tissues. 11 According to these evidences, it descends that any non-vascularized tracheal scaffold, whether orthotopically transplanted, is at high risk of necrosis, since angiogenesis may take several months to occur. In addition, also the graft size is an important feature to consider: longer and circumferential scaffolds are at higher risk of necrosis than the smaller or patch-like ones. Beside heterotopic revascularization, characterized by long times and a certain procedural complexity, another strategy to allow tracheal graft revascularization consists in its wrapping with an autologous tissue flap while occurring positioning, whether locally available.
Interestingly, among the studies included in this review, no author addressed the issue of revascularization by first heterotopic revascularization; in addition, only in two studies the graft was wrapped with an autologous tissue at the time of orthotopic positioning.57,88 In particular, Zhong et al., 57 considering tracheal transplantation procedure in rabbits, mentioned that “the anastomosis was fixed with the remaining tracheal fascia and surrounding muscle”; however, it is unclear whether this strategy was adopted to provide a reinforcement to the anastomosis or promote re-vascularization. Elliott et al., 88 in their first report of tracheal replacement with a stem-cell seeded graft on a human patient, mobilized and transposed the omentum between the heart and trachea, to minimize the risk for fistulae and to increase vascularity. 88 This was not possible for their next patient who underwent tracheal replacement with a stem-cell seeded graft in 2012: the patient had insufficient omentum to form a wrap around the conduit due to previous abdominal surgery. 89
Orthotopic implant
Research in Tissue Engineering pursues for a scaffold that, mimicking ECM features, can accommodate cells, be instructive and promote an effective tissue regeneration. However, to provide for a reliable bench-to-bedside translation of the “device,” in vivo verification is mandatory. Heterotopic positioning of the scaffold (synthetic and biologic) may guarantee for preliminary data about its specific characteristics40,41,90–92 but, in the perspective of a future use of the graft in clinical practice, orthotopic implant is fundamental: mimicking the clinical situation, the device is expected to elicit a functional response up to physiologic healing.20,93
The choice of the animal model for tracheal replacement research is of paramount importance; an adequate species is expected to meet human biology, immunology, metabolism and physiology as likely as possible. Thus, it is easily inferable that large animal models display specific features, also including tracheal diameters and wall tissue thickness, that are nearest to that encountered in clinical practice representing a better reference for surgeons, than small animal models. However, practical aspects come often into play, including availability, required housing and care, experience, expertise and costs. 94 In the 18 experimental studies included in this review, the reported animal models adopted consisted in mouse (n = 3), rat (n = 1), rabbit (n = 9), pig (n = 3), fetal lamb (n = 1), and dog (n = 1); while three studies were conducted on humans (compassionate treatments).
Considering the experimental setting specific characteristics, also the type/length of the tracheal defect to be repaired was highly variable (even within the same species). The repair of a circumferential tracheal segment was approached in 14 preclinical studies, thus requiring a conduit-shaped tracheal substitute to be interposed and a termino-terminal anastomosis with native tracheal edges to be performed; while, in four studies, an anterior window defect was created and then repaired with a patch-like tracheal graft. As for the length parameter, this was clearly not comparable between the different animal species; however, even between studies using the same animal model there was a significant variability. In studies performed on rabbits, for instance, the length of the excised tracheal segment varied from 0.5 cm 51 to more than 3 cm 54 (Tables 3–6).
Most Authors evaluated the outcomes of partially/completely decellularized tracheas but bioengineered scaffolds implantation (seeded with cells prior to implant, boosting regeneration) was also performed1,17,19,50,53,56–58,60 considering the behavior and contributory role of nasal/tracheal epithelial cells, adipose MSCs, iPS cells to graft integration (Tables 3–6).
Specific in vivo outcomes, referred to the different species, are discussed here below.
Mice and rats
Tracheal acellular allografts implanted in mice (C57BL/6) were obtained by chemical + physical strategies. According to our knowledge, after the first study developed by Kutten et al., 20 7 years passed for the subsequent adoption of mice as an animal model of tracheal disease, probably do to surgery-related difficulties. The methods described, free from enzymes presence, allowed to set up only segmental, partially decellularized substitutes still showing chondrocytes within the lacunae; no repopulation of the samples was performed before graft positioning.20,22,52
Focusing on Kutten et al. 20 preclinical outcomes, all the animals survived up to the scheduled endpoints (1, 4, and 8 weeks); however, it was observed that tracheal segments (implant size: 5–6 rings) treated by Triton X-100/vacuum lead to a moderate concentric narrowing at 8 weeks from surgery. In spite of that, the decellularized tracheas were effective in sustaining re-cellularization by epithelial cells, with a resurfacing of the lumen by the end of the first week post-transplantation. Specifically, an early proliferation of keratin (K)−5+/K-14+ basal cells and an epithelium with motile cilia and a certain beat frequency were observed. Conversely, the cartilaginous portion remained acellular. A segmental defect of 3–4 mm was later approached by both Liu et al. 22 and Tan et al. 52 The Authors highlighted comparable results in terms of survival rate (41.67% and 44%, respectively) after implantation of a segment prepared by a protocol including Triton X-100 and SDS under shaking. Respiratory distress onset (within the first week from surgery) lead to early euthanasia in most animals 22 ; additionally, high percentage of CD68+ cells was also detected, despite a certain macrophages’ infiltration was possibly amenable to tracheal repair. 52 Considering the mice that survived, patency of the grafts was evident at micro-CT. Following the histopathological analyses, luminal K5+ basal cells and K14+ cells (higher than native trachea) were detected, together with ciliated epithelial cell and restored CD31 positive endothelial cells. Additionally, increased chondrocytes viability was also evidenced. 22
The only research study considering acellular rat tracheas then orthotopically implanted in F344/NJc1-rnu/rnu rats (segment length: 5 rings), preferred to adopt chemical and enzymatic treatments + physical strategies for donor cells removal (i.e. SDC+DNase). 56 Differently from the studies above, here the regenerative contribution eventually associated with cells was also verified. Particularly, the decellularized graft group was compared with others also including mouse EGV-4T cells; mouse iPS-MEF-Ng-492B-4 or mouse iPS-Hep-FB/Ng/gfp-103C-1 cells. Each group had two or three animals, suggesting an explorative analysis by the Authors. Despite the scheduled end-point was fixed at 56 days, only the animals of the control group reached it. All the others died or were sacrificed earlier, with a shorter survival in the +iPS-MEF-Ng-492B-4 group (28 days). Except for the control group, all the animals were affected by dyspnea and wheezing, eventually associated with body-weight loss. At histopathological analysis, the samples showed a certain stenosis. In the decellularized tissue, the scaffold lumen and submucosa were fully covered/infiltrated with cells; granulation tissue presence was also identified. No cilia were recognizable on the epithelium; similar features occurred in the samples seeded with EGV-4T cells. The IPS-cells conditioning did not lead to teratoma formation, colonic cellular proliferation or granulation tissue in the tracheal lumen. A ciliated epithelium was identifiable.
Rabbits
Since 2014, the rabbit stands out as the species of choice for studies considering the effectiveness of decellularized grafts in trachea reconstruction. Both segmental3,51,54,55,57–59 and window-like defects17,19,60 were approached; the injuries extension ranged from 0.5 to 3.6 cm in length for segments and 0.7–10 mm × 0.7–10 mm for the anterior holes. Additionally, both decellularized tracheas3,51,54,55,59 and bioengineered tracheas (+ cells)17,19,57,58,60 were assessed for their in vivo outcomes. In vivo re-population was always adopted when focusing on window-like defects (Table 4).
Hung et al. 51 looked at the repair of tracheal defects (0.5 cm) through partially decellularized scaffolds obtained by SDS + sonication. All the operated animals (n = 9) died within 7–24 days from surgery, with the segments showing structure collapse at the post-mortem endoscopy. Interestingly, despite the worst outcome associated with the treated group versus the sham control group, cough and sometimes a breathing noise during the first week were typically observed in the whole cohort, thus suggesting that these clinical symptoms may also correlate with the type of surgery performed instead of the graft type (fully/partially decellularized graft; decellularization approach; pre-implant bioengineering). Survival over 2 weeks was associated to respiratory-epithelium regeneration which, as for Dang et al., 3 seems to be a prerogative for a good outcome; a mature epithelium acts as a barrier defense and provides for mucociliary clearance. Similarly to Hung et al., 51 also Dang et al. 3 engrafted the segments prepared by SDS + sonication. Surgery was performed on three rabbits only (gap: 1 cm): n = 1/3 animals survived for 2 years prior to be sacrificed while n = 2/3 animals were euthanized after 2 months from graft positioning, due to respiratory difficulties. Despite good integration of the segments with poor evidences of immune rejection, the post-mortem histopathologic analysis recognized a significant fibrosis (without stenosis), also accompanied by an incomplete regenerated epithelium. Although Dang et al. 3 were able to provide for a longer animals’ survival (2 months) than Hung et al. 51 (7–24 days), in both the cases the protocol based on SDS + sonication did not lead to fully satisfactory results in vivo, even if the low number of the samples size is an important aspect to consider as it may affect the results overall significance. SDC and DNase-I under shaking was the preferred choice to prepare tracheal grafts by Ershadi et al. 55 ; the Authors assessed promising in vivo outcomes for their decellularized trachea segments. The operated rabbits were sacrificed at 200 and 365 days, differently from the ones implanted with donor-derived tissues, who died prematurely for airway obstruction (20–45 days). The bronchoscopy, furtherly supported by post-mortem histopathologic analyses, clearly evidenced a circumferential epithelial regeneration associated with tracheal patency and absence of malacic modifications in the acellular group; differently, fibrosis, inflammation with lymphocytic and mononuclear cell infiltration up to cartilage destruction were visible in the transplant-group. Less encouraging results, in terms of animals’ survival, were that displayed by Maughan et al. 59 who combined Triton X-100 and SDC + osmotic shock + exposure to enzymes (DNase-I + RNase) for grafts preparation. Despite submucosal thickness, stromal cells and a lymphocytic response were smaller than that of the other groups, with also some evidence of neovascularization/vascular reconnection, no pseudostratified epithelium was detected.
Among the Authors considering the positioning of acellular segments only (36.59 mm), Jang et al. 54 distinguished for a particular approach based on grafts conditioning by platelet-rich-plasma (PRP). PRP products are particularly interesting in the field of tissue engineering for beneficial effects in tissues repair, mainly ascribable to growth factors and cytokines release in situ.91,95,96 Initially, granulation tissue was identified at the grafts’ margins (week 1) of the whole cohort, with a regression associated with epithelium and blood vessels regeneration (week 4 and 8). In addition, noisy breathing was also present, possibly associated with a certain stenosis degree that was more severe in the animals implanted with the PRP-free grafts. Interestingly, the healing effect in the PRP-treated rabbits was better than that showed by the animals included in the control group (PRP-free); histological and immunohistochemical analyses confirmed the presence of a normal epithelium with no CD20 and only few CD3 positive elements in the PRP-treated group.
Among cells here included in bioengineered tracheas, adipose MSCs, BMSCs, nasal epithelial cells and bone marrow derived epithelial cells were experimented. In general, in accordance with evidences gathered from other species, grafts bioengineering resulted in better clinical outcomes than cells-free scaffolds; additionally, cell seeding always occurred in studies considering window-like scaffolds implantation (Table 4). Batioglu-Karaaltin et al. 58 processed tubular segments developed by a protocol based on Triton X-100, SDC, RNase A and DNase-I. Hence, the contribution of autologous adipose MSCs was verified versus decellularized grafts only. Autologous cells exerted a fundamental role after segments positioning, aiding angiogenesis and proper tissue regeneration. Differently from not pre-seeded grafts, ciliated pseudostratified epithelium, goblet cells as well as mature chondrocytes with complete substitute integration were detected in bioengineered implants at 90 days from positioning in vivo. Interestingly, as documented by both MRI and histopathology, pre-implant MSCs seeding also discouraged the occurrence of a severe stenosis, without signs of separation, granulation, necrosis, ulceration and infection. The promising impact attributable to grafts repopulation before surgery was furtherly validated by control-groups excluding seeding or including allogenic-trachea implantation. 57 In this latter case, poor general conditions, external fibroconnective tissue formation, evidences of rejections and proliferative granulation tissue were recognized. Intriguingly, in accordance with Go et al., 53 decellularized tracheas + autologous bone marrow MSCs-derived chondrocytes (externally) and autologous epithelial cells (internally) provided for healthy functional grafts, thus suggesting this specific approach as instructive for future investigations on trachea substitutes development. No collapse or rupture of the grafts with only thin adherences occurred. 57 The recovery of window-like tracheal defects was discussed by Dang et al. 17 The Authors approached a 0.7 × 0.7 cm tracheal hole in rabbits by means of an autologous implant developed by SDS and sonication, with/without autologous nasal epithelial cells. Within this experimental setting, excluding the risk of eventual immune response triggering tracheal stenosis, the Authors aimed to specifically evaluate a feasible strategy for decellularized trachea re-epithelization. At endoscopy, performed after 2 weeks from surgery, the repopulated grafts showed a thinner and more lustrous epithelium (later detected also macroscopically) than cell-free implants; these latter distinguished for a mild stenosis of the tracheal lumen at the surgery site and outgrowth of granulation tissue within the luminal surface. According to histopathological analyses, based on HE, in both groups was identified an intact epithelium; however, bioengineered substitutes were not associated to fibrosis, differently from the decellularized patch also showing dense fibroproliferation with high neovascularization in the subepithelial layer and hypertrophy of the epithelial layer. Finally, Sun et al. 60 and Zhang et al. 19 also verified cells contribution to graft integration/effectiveness: endothelial cells derived from BMSCs and BMSCs were considered, respectively. In both cases, bioengineered scaffolds assured for better outcomes than that guaranteed by the acellular supports that, as highlighted by routine blood analyses, also correlated with a certain increase in white blood cells and lymphocytes. 60 Specifically, adequate graft integration, a completely patent lumen 60 and optimal mucosal repair 19 were visible at bronchoscopy when pre-implant seeding occurred. Histopathological analyses identified presence of ciliated epithelial cells without inflammatory elements; in addition, the expression of CD31 and CD34 suggested a good microvascularization of the specimens. Differently, a slight narrowing/mild-moderate stenosis occurred in cells-free scaffolds also not displaying epithelial coverage.19,60
Pigs
According to our knowledge, only three Authors approached orthotopic implant of decellularized/bioengineered tracheas in pig (Table 5). Two studies reported about segmental injuries treatment (range 10–12 rings)18,53, one research paper considered the recovery of a window-like defect (15 × 15 mm). 61
Pioneering, Go et al. 53 compared decellularized tracheas (SDC and DNase-I under shaking) outcomes with that displayed by three differently bioengineered tracheal grafts that included acellular trachea conditioned by: external seeding of autologous bone marrow MSCs-derived chondrocytes; internal seeding of autologous epithelial cells; external seeding of autologous bone marrow MSCs-derived chondrocytes and internal seeding of autologous epithelial cells. The scheduled end-point was fixed at 60 days; however, except for the MSCs-derived chondrocytes + epithelial cells group, all the other animals died earlier, with a mean survival of 11 days in cells-free grafts, 29 days in presence of MSCs-derived chondrocytes and 34 days in presence of epithelial cells. Thus, cells exert a contributory role in terms of survival rate of the animals; however, a certain stenosis was detected in the whole cohort, according to this descending order: +epithelial cells >cells-free tracheas > + MSCs-derived chondrocytes. Histopathological analysis of the explants showed presence of bacterial/fungal contamination in the acellular group and in the tracheal ECM + MSCs-derived chondrocytes group. Less/slight inflammatory signs, suggesting a good graft integration, were observed in the animals implanted with segments repopulated with epithelial cells with/without MSCs-derived chondrocytes.
Villalba-Caloca et al. 18 approached decellularization by 7 or 15 cycles of a protocol based on Trypsin-EDTA, SDC and DNase-I. All animals survived surgery but not the study time, scheduled at 4 weeks; euthanasia occurred before the third post-implant week. At histopathological analyses, the whole cohort displayed disorganized collagen fibers; considering the group implanted with scaffolds prepared by 15 cycles, necrosis and bacteria were also detected in tissue full-thickness. The same was observed in presence of an external surgical steel wire; here, the typical histopathologic findings included lymphocytes and calcifications in the lamina propria and adventitia with hemorrhagic evidences like in the submucosa and necrosis. Regarding the scaffolds prepared by 7 decellularization cycles, all of them showed scattered areas of preserved epithelium; cartilage degeneration and chronic inflammation with also histiocytes in the perichondrium. Cartilage and lamina propria were characterized by granulation tissue, congestion, hemorrhage, fibroblasts, calcifications, necrosis and bacteria.
Differently from the studies mentioned above, Ohno et al. 61 focused on a window-like defect. Like Villalba-Caloca et al., 18 no cells seeding occurred and decellularized and fresh tracheas were compared for in vivo outcomes at 11 weeks from graft positioning. Experimental data, based on histopathology, showed lumen maintenance (mild narrowing) with a certain longitudinal compression. Macroscopically, the tissue engraftment without presence of inflammatory signs and a certain spread of the mucosal membrane were evident, as later confirmed by the histopathologic analysis. CD3 positive elements were detected at the graft margins but less than that observed in the fresh-trachea implanted group, which also displayed a greater stenosis with internal contortion.
Others
Two unusual animal species were considered in the whole panorama of studies addressing tracheal reconstruction by acellular allogenic grafts (Table 6). Dog-derived tracheas were decellularized by Wood et al. 50 adopting a chemical + physical strategy (for protocol details see Table 1). Specifically, regeneration driven by adipose MSCs dispersed in fibrin glue (n = 4) was figured out versus a control group (n = 1) implanted with the acellular graft + fibrin glue, without cells. Despite an intact surgical anastomosis suggesting the surgical technique adequacy, all the implanted dogs (segment length, 2.5 cm) were sacrificed due to malacic and compromised tracheas, leading to airway distress at about 1 week postoperatively. Unfortunately, the neat contribution of cells was not clearly identifiable here.
Rabbit tracheal matrices, decellularized by chemical and enzymatic treatments + physical strategies, were implanted in fetal lambs for the replacement of 9–12 rings. 1 The study experimental design allowed to verify the contribution in regeneration guaranteed by cells seeding over SDC-DNase-I derived scaffolds. Segments bioengineering resulted in better clinical outcomes characterized by full epithelization of the lumen; as reported by the authors, engineered grafts showed a significant increase in diameter in vivo, differently from acellular grafts. Moreover, engineered constructs exhibited full epithelialization, versus the acellular counterpart. Histological analyses considering ECM features detected increased and stable levels of α-elastin and GAGs, respectively.
From the bench-to-the-bedside: Transplantation of decellularized tracheas in humans
Clinical transplantation of a decellularized and bioengineered tracheal allograft is a procedure still considered as compassionate. To date, only three cases were reported in the literature: one adult and two pediatric patients. Regarding treatment success, good outcomes were observed in an adult (first case)97,98 and in a young boy (second case),88,99 respectively. As firmly supported by Elliott et al., 88 urgent need is to convert one-off, compassionate-use successes into more widely applicable clinical treatments.
2008: The first implant of a tissue engineered trachea in human
The first transplantation of a tissue engineered trachea in human was reported in 2008 97 and a 5 year followup was also communicated. 98 The clinical case refers to a 30-year old woman who was diagnosed with post-tuberculosis chronic tracheitis and secondary severe bronchomalacia of the left main bronchus. A near occlusive 3 cm tracheal stenosis was well treated by resection and end-to-end anastomosis, however, the Dumon stent placed in the bronchus was not well tolerated with consequent recurrent pneumonitis, cough and mucous retention leading to its removal. Further worsening of patient’s conditions occurred and carinal total pneumonectomy appeared as the only conventional option to perform. As this procedure is commonly associated with high mortality rates as well as perioperative and long-term morbidity, the complete resection of the left bronchus associated with bioengineered human trachea replacement was pursued. Bioengineerization consisted in the donor-derived trachea decellularization followed by repopulation with recipient cells; specifically, the airway matrix was seeded with epithelial cells and bone marrow MSCs differentiated into chondrocytes.
According to the methods section, 97 a tracheal segment of 7 cm in length, obtained by a 51-years old female donor died because of cerebral hemorrhage, was processed through a combined protocol including chemical and enzymatic treatments + physical strategies. After tissue rinse in a PBS solution added in 1% streptomycin and 1% amphotericin B, 25 cycles occurred of a decellularization protocol that was previously set-up. Briefly, the method consisted in 7 h in distilled water + incubation in 4% SDC and 2000 kU deoxyribonuclease I in 1 mmol/L sodium chloride. 100 The segment was then reduce to 5 cm intraoperatively, to fit the defect. The 25 cycles were claimed to be adequate to assure epithelial and glandular cells removal; only few and mainly anuclear chondrocytes remained. 101 Tissue architecture was reported as maintained. HLA-A, HLA-B and HLA-C antigens were referred as removed although low levels of focal MHC class II positive elements were still identifiable in limited areas.
According to the study results section, 97 lung function resulted normal after 2 months; serological analysis showed absence of anti-donor HLA antibodies at 14 days, 1 month, and 2 months. Moreover, the segment was indistinguishable from adjacent normal bronchial mucosa at still 4 days from surgery suggesting its engraftment. The presence of a rich microvascularization was showed by laser-doppler. At 14 days, the mucus detected on the graft surface was free from inflammatory cells. The segment was recognized as healthy and strong along the follow-up (14 days, 1, 2, and 3 months). Cytological analysis of the luminal surface confirmed the presence of epithelial cells at 4 days; viable chondrocytes were also identifiable. The patient was followed-up approximately every 3 months using a multidetector CT scan and bronchoscopic assessment. Every 6 months, biopsy samples were obtained for histological, immunohistochemical and electron microscopy assessment. By 12 months after surgery, a progressive cicatricial stenosis was identified in correspondence of the anastomosis site requiring endoluminal stenting; however, the tissue engineered trachea was referred as open, well vascularized and recellularized with normal cilia function and mucus clearance. Also, lung function and cough reflex were reported as normal. No teratoma formation or anti-donor antibodies were developed; the patient was referred as able to conduct a normal social and working life by the Authors. 98
On 4 March 2019, at the invitation of the Lancet editors, the journal published a clinical update letter by Laureano Molins, who was involved with other colleagues in the patient management. 102 Here it was reported that “3 weeks after the transplantation, it was necessary to stent the transplanted bronchus because of a homograft collapse.” At 9 months after transplantation, the patient started a followup in a new institution and no further news were available from her. Later, in February 2014, the patient was admitted to the Department of Thoracic Surgery again showing evidences of acute respiratory failure and total atelectasis of the left lung; the bronchoscopy highlighted an 80% bronchial collapse. The patient referred that in the previous 5 years, she underwent positioning of multiple bronchial stents (mainly bioabsorbable). In that occasion, a silicone stent was placed in turn leading to lung re expansion. Since then the patient experienced the need of multiple fibreoptic and interventional rigid bronchoscopies (total number: 18) to assure a certain bronchus patency. The left lung showed a very poor function (20% of that expected), and the patient experienced repeated bronchial obstructions, causing multiple lung infections in turn requiring several interventional bronchoscopies. As consequence of this, in July, 2016 a transternal left pneumonectomy was done; the patient was discharged after eighth days from surgery as the postoperative course was uneventful. At 30 months after pneumonectomy, the patient was fully recovered. 102
In 2022, Schneider et al. 103 also reported that in May 2018 the Lancet received an e-mail by Antoni Castells, the new director of the Hospital Clinic Barcelona where the first implant of a tissue engineered trachea in human occurred. Here, it was claimed that “three weeks after the airway transplantation procedure, it was necessary to stent the transplanted bronchus, due to an homograft collapse.” In the light of this, the graft could not have had “a normal appearance and mechanical properties at 4 months.” In addition, discrepancies were also recognized about lung function improvement. 103
Following the 2008 paper, 97 Schneider referred that other patients experienced transplantation of cadaveric trachea graft 104 Schneider et al. 103 reported that “the collapse of decellularized cadaveric tracheas contributed to the death of several patients, including a 19 year old woman [. . .] and a 15 year old girl.”
On the basis of the above discordances, Schneider et al. 103 asked for retraction of the 2008 paper 97 ; however, at the moment, the manuscript has not been retracted. 105
2010 and 2016: The second and the third implant of a tissue engineered trachea in human, two pediatric patients
The second case considering the positioning of a tissue engineered trachea in human occurred in 2010 in a 12-year-old child. The boy, born with a long-segment congenital tracheal stenosis and pulmonary sling, was approached by autologous patch tracheoplasty at 6 days old followed by the positioning of a balloon-expandable stainless-steel stents to counteract patch collapse and scarring as well as severe bilateral bronchomalacia. Despite a significant clinical improvement, at 3 years old the child showed aorta erosion by the stent, requiring an emergency repair by a bovine pericardial patch. The impacted stents and trachea were excised and replaced by a tracheal homograft that was replaced 1 week later by another stented homograft, due to mediastinitis. After 3 months of hospitalization, the patient showed an excellent recovery; because of recurrent stenosis, occasional interventions were required for further stents positioning. At 10 years old the patient suffered a second hemorrhage: instrumental analyses (bronchoscopy and CT scan) identified erosion of tracheal stents with a new aortotracheal fistula thus requiring urgent reconstruction. After excluding tracheal allografting (as implying lifelong immunosuppression) an autologous stem-cell-based tracheal replacement was planned. A donor-derived trachea was obtained by a 30-year-old deceased woman (segment length 7 cm); the tissue was decellularized with distilled water + 4% SDC + 2000 kU deoxyribonuclease I (see paragraph 7.1) 101 and then repopulated with the recipient’s cells after a short course of granulocyte colony stimulating factor (G-CSF). Specifically, BMSCs were isolated preoperatively and seeded onto the scaffold in the operating room; contextually, patches of autologous epithelium, removed from the excised trachea, were placed as free grafts at regular intervals within the lumen of the acellular trachea. In the meanwhile, topical human recombinant erythropoietin (hrEPO) and TGFβ were adopted to promote angiogenesis and support chondrogenesis, respectively. To support the graft patency, an absorbable polydioxanone (PDO) tracheal stent was sutured in place. Considering the clinical outcomes, graft revascularization occurred within 1 week after surgery but epithelium restoration was not detected until 1 year; despite any further medical intervention was required, no biomechanical strength was highlighted focally until 18 months. A normal chest CT scan and ventilation-perfusion scan were observed at 18 months after surgery. At 2 years follow-up, the patient had a functional airway and returned to school. 88 At 42 months from surgery, proximal transplant biopsy highlighted the presence of a complete epithelial layer characterized by a mix of squamoid and respiratory type epithelium with also few ciliated cells; a complete mucosal layer was also detected at bronchoscopy together with a widely patent airway. No evidence of rejection/lymphocyte-associated epithelial damage was observed, in presence of normal submucosal T cells. Ki67 was normal while caspase 3 was negative in both pre and posttransplant specimens. No anti-donor HLA antibodies were identified at serological examination. Routine endoscopy showed ciliated epithelial cells with a normal ciliary beat frequency. 99
After failure of the conventional reconstructive approaches (tracheoplasty with a lateral costal cartilage graft repair at 2 months of age; pericardial patch tracheoplasty at 4 years of age) characterized by malacia, failed balloon dilatations, recurrent granulation tissue formation and re-stenosis up to tracheostomy, a girl born with a single left lung and long-segment congenital tracheal stenosis was treated by a stem cell-seeded, decellularized tracheal graft, at 15 years old. This case represented the third case in clinical practice of tissue engineered trachea implantation in a compassionate use case. Briefly, according to the previous experience reported by Elliott et al., 88 a tracheal segment derived from a human cadaveric donor, matched for normal tracheal diameter, was decellularized by detergent enzymatic processing, under vacuum pressure; Good Manufacturing Practice (GMP)-compliant production processes were adopted. Hence, autologous MSCs from bone marrow aspirate and respiratory epithelial cells from mucosal biopsies were used and seeded/cultured onto the scaffold, prior to be implanted in the patient, taking advantage by a bioreactor. Regarding tracheal replacement surgery, resection occurred and the segment was placed in situ; because of previous abdominal surgeries, it was not possible to proceed with omental flap positioning. Unfortunately, while early results were encouraging, a sudden airway obstruction occurred (intrathoracic bleed?), thus leading to patient death, 3 weeks after surgery. 89
Conclusions and final considerations
To date, the development of a tissue engineered/bioengineered tracheal graft followed by its transplant represents a potential treatment of last resort in case of significant compromission of tracheal tissue integrity and function.
Decellularization is regarded by several authors a promising and vanguard technique to prepare an adequate scaffold; however, the ideal method for generating a fully functional graft has yet to be elucidated. Approached techniques, despite assuring for non-immunogenic substitutes due to mismatched MHC absence, may not preserve tracheal ECM architecture thus leading to collapse/stenotic fibrosis of the implant. Control over the mechanical properties of the decellularized tissue remains among the most significant challenges in trachea tissue engineering. To date, migration and hemorrhage after any tracheal substitute placement accounts for 68% of graft-related mortality in all clinical cases. 4 Thus, unfortunate clinical evidences suggest two key-points to keep in mind when developing a new tracheal tissue engineered device: the graft must not be so soft, avoiding collapse and stent positioning for patency (which can lead to a host further complications); it must not be so stiff/sharp, avoiding migration and perforation of the nearby vascular structures. 4 Often, obtaining a mechanically unsuitable decellularized scaffold descends from a not fully suitable decellularization protocol. Drawbacks include ECM structural alteration or loss of some important ECM components due to overexposure to enzymes and/or chemicals. Recurring to crosslinkers for matrix strengthen can lead to unproper rigidity. 106 The protein composition/ECM stiffness likely affects the resident cells behavior including spreading and motility, changes in morphology and cytoskeletal dynamics, apoptosis, signal transduction, and ECM remodeling; the same occurs in pathological conditions.107,108 That may partly justify the small rate of success in preclinical studies. Considering tracheal tissue organization and specific characteristics, applying a different protocol for cartilage tissue and mucosa/submucosa decellularization would be appealing. Ideally, un-coupling mucosa/submucosa from cartilage by stripping, to perform specific ECM respectful decellularization protocols, prior to re-coupling the two layers and proceed with grafting, may be a new and interesting approach to be considered in the future.
Together with mechanical properties maintenance, working on “protocol effectiveness” also implies the identification of a method addressing other challenging features including: (i) reasonable decellularization times; (ii) no cytotoxicity; (iii) graft integration with proper vascularization. To date, combining chemical and enzymatic treatments + physical strategies seem to be the preferred choice for tracheal decellularization; however, despite consensus in the main direction to follow, protocols crucial specificities are difficult to be established also due to not comparable set-up in preclinical studies. Different species and defects’ types/extensions, low samples size, not uniform animals’ number per group, distinct instrumental and/or histopathologic analyses together with biological variability can be encountered as aspects leading to significant bias. Additionally, with a focus on the detergents adopted, many Authors recurred to Triton X-100 (an octylphenol ethoxylate) that has been recently placed into Annex XIV of the European Union REACH (Registration, Evaluation, Authorisation and Restriction of Chemicals) regulation, due to endocrine toxicity of its degradation derivatives. Since the 4th January 2021 it cannot be used or placed on the market unless an exemption certificate is held. Other detergents can be effective to prepare acellular scaffolds, however, to assure for a “safe” decellularized device, more rigorous technical approaches, likely based on high performance liquid chromatography (HPLC) and mass spectrometry, should be routinely adopted to confirm chemical residues absence. In case of trapped detergents within the ECM network, eventual desorption even in long time, may trigger cytotoxic events with inflammation and poor function of the device.
A further reflection concerns possible bioengineerization of the biological construct. An ideal scaffold is expected not only supporting cells growth, but also promoting tissue regeneration. 109 However, dense arrangement of collagen fibers, typical of cartilage ECM, may hinder cells invasion and graft integration.110,111 This may also occur in case of adequate donor cells removal following numerous decellularization cycles. Consequently, referring to trachea, structural collapse with degradation of the matrix, separation in the anastomosis region, infection up to death is possible. 112 To counteract cell invasion difficulties within cartilage tissues many methods have been applied from cutting cartilage into sheets, 113 to mincing it into fragments. 114 However, these approaches alter tissue 3D, which is fundamental in trachea grafting. Within this scenario, recurring to laser micropatterning may represent a safe, inexpensive and interesting strategy stimulating cellular infiltration, thus triggering graft remodeling and reconstitution.110,111,115,116 Like other cartilaginous tissues (e.g. temporomandibular joint disks, 110 articular cartilage 111 ) also trachea was recently approached by lasering. Superficial pores of 200–300 µm in depth109,115 showed to be effective in supporting de novo synthesis of a robust cartilage matrix after cellular invasion. There are two possible reasons for this: the porous structure increases the cell contact area, which is conductive for cell spreading; lasering introduces a certain surface rough that is advantageous for cells to adhere. 112 Moreover, the treatment is respectful of tissue integrity without destroying it and keeping original advantages of a shape-preserving graft.109,115 Despite research is still required, especially on the most proper equilibrium between decellularization grade and pores depth (depending on the output power and pulse width), laser micropatterning seems promising and further work on it needs to be encouraged. Intriguingly, lasering may also act as a supporting step in decellularization. 109
Contextually, identification of the most proper cells to use (one single population? differentiated cells? stem cells? alone or in co-culture) and consciousness about the extended times (and costs) required for isolation, expansion, pre-seeding are not elements to ignore. Certainly, the early regeneration of epithelium in transplanted tissue is among the most important elements to focus on while approaching tracheal reconstruction. 54
In regards of all the issues discussed above, it descends that intense research is required prior to introduce tissue engineered tracheal substitutes among commonly adopted procedures in case of severe airway compromission. Only solid studies favoring the cooperation of different expertise/figures (anatomists, biologists, engineers, veterinary, surgeons) within preclinical studies conducted on large animals, may led to “biological devices” with low morbidity, increased mechanical properties, good integration in the defect site and acceptable costs to healthcare providers. To date, there is no standard large animal model to adequately evaluate candidate tracheal replacement strategies/grafts for future clinical application; unfortunately, their use is severely affected by practical issues (costs, housing, and procedural difficulties) in turn promoting the use of other species, as rabbits. Establishment of a standard large animal model for tracheal repair is strongly recommended, also supporting data from rodent models progressively leading to results that can be successfully translated to the clinical setting. 117 In parallel, surgical procedure for tracheal graft implantation is not free from issues; for instance, positioning of a muscular flap to induce graft vascularization and survival is a peculiar step for surgery success, despite not broadly described in the literature (Figure 2).

Development of functional tracheal substitutes is an intriguing challenge corresponding to an unmet clinical need. Tissue engineered grafts and, in particular, decellularized/engineered allografts may be promising; however, identification of the most suitable fabrication approach (chemical + physical treatments or chemical + enzymatic + physical treatments) is still debated. Currently, paucity of preclinical studies represents a possible limitation to successful clinical outcomes.
In the panorama of tissue engineering-based tracheal substitutes, beside synthetic grafts and shape-preserving decellularized allografts (these latter representing the focus of this review article), composite scaffolds are also under investigation; merging the advantages of both the synthetic and the biological matrices they are a promising future option also for trachea reconstruction. The synthetic scaffold can be customized with structural and mechanical characteristics similar to the native trachea, whereas the possible lacking biochemical cues, that are fundamental for graft regeneration, are provided by the ECM (not exclusively from trachea). The biological component plays a critical role modulating epithelial cells migration, proliferation, and differentiation.118–121 As representative of this encouraging strategy for trachea, Xu et al. 121 fabricated electrospun nanofibrous membranes composed of decellularized Wharton’s Jelly matrix/poly(ε-caprolactone) (PCL) (ratios: 8:2, 5:5, and 2:8). Homogeneous cartilage regeneration was observed in presence of the higher matrix content and derived 3D, tubular, trachea-shaped devices also revealed efficient in circumferential tracheal lesion repair in rabbit. Additionally, Huo et al., 120 reported the efficient fabrication of a “cartilage-vascularized fibrous tissue-integrated trachea,” recurring to 3D-bioprinting and new photocrosslinkable tissue-specific bioinks loaded with chondrocytes/fibroblasts. The inks were made of [methacryloyl-modified gelatin, chondroitin sulfate, and cartilage acellular matrix] (the first) and [methacrylate-modified hyaluronic acid, 8-arm-polyethylene glycol-succinic acid ester and methacryloyl-modified derm acellular matrix] (the second). The tubular ring-to-ring alternant structure showed as a promising alternative for clinical trachea reconstruction. Mimicking target tissue ECM composition and structure is fundamental for optimal scaffolds development as these characteristics are required to guide cellular differentiation and tissue remodeling. In particular, considering the critical long-segment tracheal injuries scenario, recurring to stem cells for tracheal cartilage regeneration may be promising 121 and furtherly explored, possibly also combining this cells source with the more complex composite scaffolds described above.
Despite considerable logistical and technical obstacles still requiring significant efforts in research and surgery while approaching trachea reconstruction, airway tissue engineering may represent a solid therapy in future clinical practice. Aiming to strongly support researchers and clinicians in the trachea challenging “mission,” we are firmly convinced about the potential residing in Body Donation Programs.122–127 In accordance with previous evidences we gathered, donated bodies may represent a precious supporting resource, displaying a twofold meaning: they may serve surgeons, thus allowing for surgical technique improvement and clinical setting simulation; but, additionally, they may also represent a precious source of human tissues for the establishment of a biobank of organs (i) to be included in “research and development” studies; (ii) ready to be decellularized for subsequent implant in patients; and (iii) supporting the institution of an acellular tissues/organs deposit for bioengineerization and devices customization, toward the development of a personalized medicine.
Supplemental Material
sj-docx-1-tej-10.1177_20417314231151826 – Supplemental material for Preclinical and clinical orthotopic transplantation of decellularized/engineered tracheal scaffolds: A systematic literature review
Supplemental material, sj-docx-1-tej-10.1177_20417314231151826 for Preclinical and clinical orthotopic transplantation of decellularized/engineered tracheal scaffolds: A systematic literature review by Elena Stocco, Silvia Barbon, Marco Mammana, Giovanni Zambello, Martina Contran, Pier Paolo Parnigotto, Veronica Macchi, Maria Teresa Conconi, Federico Rea, Raffaele De Caro and Andrea Porzionato in Journal of Tissue Engineering
Footnotes
Acknowledgements
The Authors would like to thank Dr. Giulia Zivelonghi for her kind help in literature revision.
Authors’ Contributions
All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be published. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the ‘Consorzio per la Ricerca Sanitaria’ (CORIS) of the Veneto Region, Italy (L.i.f.e.L.a.b. Program), grant number DGR1017, 17 July 2018.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.