
Abstract
Dysfunction in the olfactory system of a person can have adverse effects on their health and quality of life. It can even increase mortality among individuals. Olfactory dysfunction is related to many factors, including post-viral upper respiratory infection, head trauma, and neurodegenerative disorders. Although some clinical therapies such as steroids and olfactory training are already available, their effectiveness is limited and controversial. Recent research in the field of therapeutic nanoparticles and stem cells has shown the regeneration of dysfunctional olfactory systems. Thus, we are motivated to highlight these regenerative approaches. For this, we first introduce the anatomical characteristics of the olfactory pathway, then detail various pathological factors related to olfactory dysfunctions and current treatments, and then finally discuss the recent regenerative endeavors, with particular focus on nanoparticle-based drug delivery systems and stem cells. This review offers insights into the development of future therapeutic approaches to restore and regenerate dysfunctional olfactory systems.
Introduction
Olfactory dysfunction, estimated to affect 3%–20% of the population, significantly affects the health and quality of life of the afflicted individual,1,2 and increases the likelihood of mortality among individuals up to four times. 3 This is mainly related to the body’s weakened defense (immune) system and the inability to sense dangerous signals (e.g. fires, hazardous chemical vapors, gas leaks, and decayed food).4–6 The principal causes of olfactory dysfunction are sinonasal diseases, viral infections, head injuries, and neurodegenerative diseases.
The olfactory system has several unique characteristics. One notable feature is that the cells (mainly olfactory sensory neurons (OSNs)) are always exposed to various harmful substances while in direct contact with external air that enters the nasal cavity 7 ; as such, the OSNs are easily damaged. More importantly, OSNs can also regenerate throughout the lifetime of a person 8 ; this fact allows the possibility of regenerative approaches to treat olfactory dysfunction. While treatment varies depending on the etiology of the olfactory dysfunction, medications such as oral/intranasal steroids, surgery, and olfactory training are clinically used. However, as the success of these various treatment modalities is not guaranteed, it is currently challenging to treat patients with olfactory dysfunctions. Recent efforts in the field have yielded promising outcomes in the treatment of anosmia using stem cell therapies.
Thus, we are motivated to highlight recent studies that endeavored to regenerate the dysfunctional olfactory system. For this, we first introduce the anatomical characteristics of the olfactory pathway, then detail the various pathological factors related to olfactory dysfunction and current clinical options, and then finally discuss the recent emerging therapeutic approaches, particularly with respect to nanoparticle-based delivery systems and stem cells. We also added the availability of the combinatory approach of nanoparticles with stem cells to potentiate regenerative functions. This review offers insights into the development of future therapeutic approaches to restore and regenerate the dysfunctional olfactory system.
Anatomy of the olfactory system and the dysfunctions: A brief overview
Figure 1 shows the anatomical structure of the olfactory pathway. The olfactory nerve is the first of the 12 cranial nerves and specifically carries olfactory sensory information (sense of smell). The olfactory epithelium (OE), a mucosal membrane that lines the roof and sides of the nasal cavity, contains the olfactory receptor cells. When an odorant passes through the nasal vestibule and contacts the OE, the perception of smell begins. The OE consists of the pseudostratified columellar neuroepithelium and basal cells which reside in the deep layers of the OE, and function as stem cells with multipotency. 9 These basal cells can give rise to new olfactory sensory neurons. 10

Anatomy of the olfactory system, and the tissue structure and cells comprising of.
Olfactory neurons reside superficially to basal cells. Each olfactory neuron expresses a single olfactory receptor. One odor is capable of activating multiple receptor types to varying degrees. The binding of an odorant to olfactory receptors results in signal transmission via the olfactory nerves to the olfactory bulb. Efferent neurons of the olfactory bulb form the olfactory tract. The axons from the olfactory bulb cells project information to the thalamus, hypothalamus, and dorsolateral frontal cortex, which ultimately results in the sense of smell. 11
Clinically, olfactory dysfunction results from many underlying diseases such as sinonasal diseases, post-infectious disorders, and post-traumatic disorders.12–14 Other etiologies such as congenital, idiopathic, toxic, or neurodegenerative disease-associated problems are related, but less prevalent; however, they must not be ruled out. Depending on the site of olfactory nerve injury, olfactory dysfunction is categorized as follows: (i) direct damage to the olfactory nerve epithelium or subepithelial tissue, and (ii) degeneration and damage to the olfactory nerve axons or olfactory bulb. 15
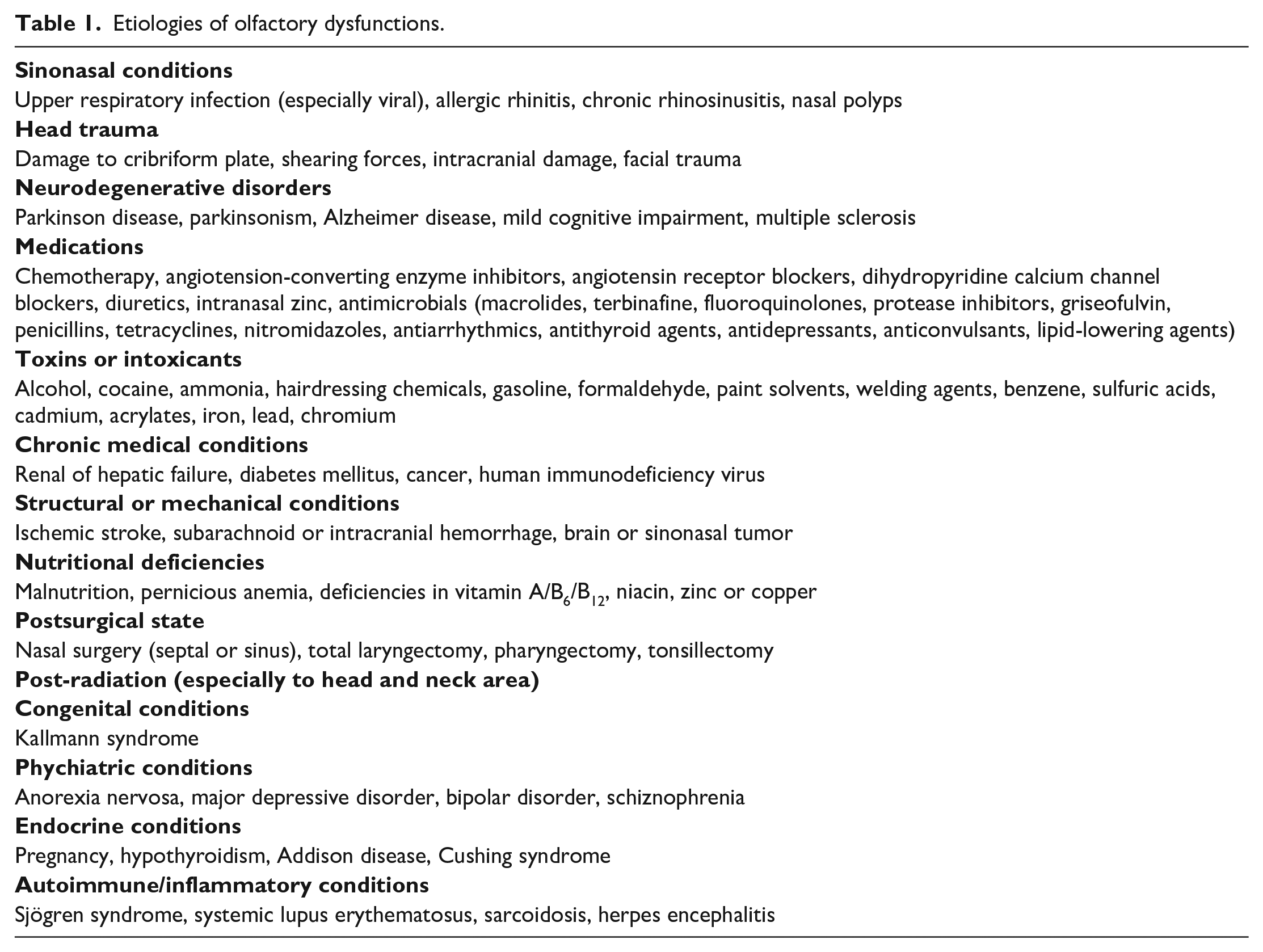
Table 1 summarizes the common etiology of olfactory dysfunction. Most etiologies are attributed to common conductive or traumatic processes (such as, sinonasal disease and head trauma) and common sensorineural processes (such as, upper respiratory infection and age-related loss), and congenital disorders. 16 Regardless of the specific etiology, neurogenic exhaustion is likely a common feature of many acquired anosmia in which the normal replacement of damaged or senescent OSNs from progenitor basal cells is overwhelmed. 17
Etiologies of olfactory dysfunctions.
Current clinical treatments and therapeutic molecules and their limitations
Clinical treatment options
For patients with chronic rhinosinusitis, functional endoscopic sinus surgery was shown to improve some of the olfactory functions, ameliorating ventilation, and decreasing inflammation in the olfactory cleft area 18 ; a spontaneous recovery in 32%–66% of the patients was observed in post-URI anosmia. 19 On the other hand, post-traumatic olfactory disorders showed a much lower recovery rate, due to scarring in the cribriform plate area, accompanied by shearing injuries and intracranial lesions. 20 Olfactory training is also recommended to gain some olfactory functions in post-traumatic anosmia/hyposmia 21 and in chronic rhinosinusitis.22,23 Exposure to certain odors may modulate the regenerative capacity of olfactory receptor neurons.24,25 In this study, patients with post infection anosmia showed brain remodeling during functional magnetic resonance imaging following 12 weeks of olfactory training. 26 Patients with hyposmia, who have neurodegenerative disorders like Parkinson’s disease, may also benefit from olfactory training. 27
Clinical therapies based on oral or systemic steroids have often been proven to be effective for sinonasal disorders, although the duration and dose of steroids remain to be optimized.28,29 Topical steroids have also been shown to be effective in allergic rhinitis combined with antihistamines.30,31 In a double-blind, randomized, placebo-controlled study, the effect of fluticasone nasal spray on patients with olfactory dysfunction was evaluated. Eighty-three percent of the patients had improved smell after systemic treatment, with no difference observed in the topical versus placebo groups. 32 Although the administration of steroids was proven to be effective in many animal models,33,34 studies in humans showed variable outcomes and often had limited efficacy.35,36 In patients with post-traumatic olfactory dysfunction, the treatment effect of steroids was known to occur only in 12%–16% of the patients. 37 More importantly, the side effects of steroids such as osteonecrosis and iatrogenic Cushing syndrome (adrenal insufficiency) have been raised as significant considerations.38,39 Other side effects of steroids include cataracts, gastritis, hyperglycemia, hypertension, delayed wound healing, and bacterial/fungal/viral infection.
Other medications such as statins and vitamins have been used in clinical settings, in addition to steroids. A recent study has revealed that vitamin A plays a role in the regeneration of olfactory receptor neurons. 40 In post-traumatic and post-infectious anosmic patients, topical treatment with vitamin A increased the olfactory function in 37% of anosmic patients, while 23% improvement was shown in the control group. 40
Candidates of therapeutic molecules studied in vivo
Some of the candidate small molecules and proteins, albeit not clinically proven, have been tested in dysfunctional olfactory in vivo models.
Statin, a β-hydroxy β-methylglutaryl-CoA (HMG-CoA) reductase inhibitor with putative neuroprotective properties, has shown effects on the nervous system. 41 Kim et al. 42 showed that the statin treatment group had an increased expression of olfactory marker protein (OMP) and thickness of OE, compared to the control group. Furthermore, a significantly higher pass rate in a food-finding test was shown in the treatment group compared to that in the control group. 42
Valproic acid (VPA), a histone deacetylase (HDAC) inhibitor, has shown some neuro-regenerative properties in rodents with spinal cord injury. 43 Ogawa et al. 44 investigated the effects of VPA on olfactory sensory neuron regeneration. In a mice model of OE degeneration induced by methimazole injection, daily administration of VPA increased epithelial thickness, the proliferation of OMP positive cells, and the expression of growth-associated protein-43 (GAP43), which is a nervous tissue-specific cytoplasmic protein in the OE, suggesting that VPA stimulates proliferation and differentiation of olfactory precursor cells, which in turn promotes regeneration of the olfactory system. 44
Treatment with growth factors is also a potential tool to improve olfactory dysfunction by restoring homeostasis and normal neurogenesis, as growth factors stimulate cellular growth, proliferation, and regeneration. 45 In young and aged mice, intranasal administration of basic fibroblast growth factor (bFGF) significantly increased the proliferation of GAP43-positive cells, although there was no significant change in the number of OMP positive cells and mature olfactory receptor neurons. 46 Nota et al. 47 examined the effect of bFGF on the injured OE of mice. In a murine anosmia model, intranasal treatment with bFGF and hydrogel increased the thickness of the OE and the number of mature OSNs expressing OMP. 47 With hydrogel, sustained release of bFGF could be achieved.
Platelet-rich plasma (PRP) is a small amount of blood from a subject that is separated into its components via centrifugation. It is a biocompatible physiological material and contains many growth factors, including platelet-derived growth factor (PDGF), transforming growth factor-β (TGF-β), epidermal growth factor (EGF), vascular endothelial growth factor (VEGF), insulin-like growth factor (IGF), and numerous neurotrophic factors such as the neurotrophin-3, angiopoietin-1 (Ang1), and glial cell line-derived neurotrophic factor (GDNF).48–52 A recent study demonstrated the effectiveness of PRP on anosmia in a mouse model, showing that PRP treatment induced significant functional and histological improvements. 53 However, this study had some limitations; the authors only investigated the histopathological findings with hematoxylin and eosin staining.
These studies in in vivo anosmia models revealed some of the important roles that small molecules and proteins play in various biological pathways in restoring the functions of OE, highlighting their potential use as candidate molecules for the treatment of olfactory dysfunction in the future. Despite their therapeutic effectiveness, the potential dose-dependent human toxicity and side effects of small molecules and proteins, particularly when administered systematically, must be resolved, which might be alleviated by utilizing adequate delivery systems.
Nanoparticle-based intranasal drug delivery system
Nanoparticles have been extensively studied as drug delivery systems in diverse fields, including for the treatment of tumors, neurodegenerative disorders, and cardiovascular diseases.54,55 Nanoparticles have recently been studied for applications in olfactory disorders. Like in the other areas, the treatment of olfactory system disorders requires the nanoparticles to satisfy several prerequisites: biocompatibility and the capacity to load large amounts of cargo molecules and subsequently release them in a controllable manner. Furthermore, the nanoparticles are tailored to exert specific functions; for example, surface modification is required to target cells or cellular components, which depends on the administration route (oral, intravenous, or intranasal delivery), and the composition needs to be properly chosen (polymers, inorganics, or composites) to allow controlled drug release profiles (diffusion, swelling, erosion, or degradation). Sometimes, the nanoparticles are equipped with more advanced properties such as stimuli-responsiveness and imaging/diagnostic capacity. Authors are guided to refer to some of the key reviews in this nanoparticle development area.56–58 Among other delivery routes, intranasal delivery has been the most widely studied route for the use of nanoparticles in the treatment of olfactory system disorders.
Overcoming mucus clearance and the therapeutic efficacy in vitro and in vivo
Above all, the mucus layer is considered a unique characteristic of the olfactory system; thus, “mucociliary clearance” has remained a major physiological barrier that the nanoparticles with drugs need to overcome in the olfactory pathway. 59 This protection mechanism of the respiratory system operates efficiently and rapidly eliminates noxious substances (particles and microorganisms) trapped in the 10–15 μm thick mucus layer. As such, this system greatly limits the residence time of therapeutic substances administered into the nasal cavity.
Two strategies made with nanoparticles are used to address the mucociliary clearance issue: (i) mucoadhesive and (ii) mucus-penetrating, as depicted schematically in Figure 2. The mucus layer has different physicochemical properties depending on the organ. The nasal mucus is slightly acidic (pH 5.5–6.5) and is negatively charged because of the presence of high amount of mucins.60,61 Therefore, mucoadhesive nanoparticles are often developed to have a positively-charged surface to maximize nanoparticle adhesion to the nasal mucus based on their electrostatic attraction with mucins. Moreover, the surface can be tailored to be hydrophobic to enable hydrophobic interaction with mucin hydrophobic domains. 62 For this reason, chitosan has been widely studied as a mucoadhesive nanoparticle for intranasal drug delivery. It is not only biocompatible, biodegradable, mucoadhesive, and positively charged in the slightly acidic pH of nasal mucus, but is also an efficient permeation enhancer that can transiently open the tight junctions between epithelial cells in mucosal tissues.63–65

(a) Schematic illustrating the mucoadhesive and mucus-penetrating strategy with developed nanoparticles. Mucoadhesive nanoparticles (b) are good at catching the surface of mucous membrane whereas the mucus-penetrating nanoparticles (c) transport more effectively through the mucus layer.
Several studies have reported mucoadhesive nanocarriers based on chitosan derivatives (Figure 3(a)). Trimethyl chitosan (TMC), for example, is a water-soluble, permanently positively charged chitosan derivative that has been used to encapsulate the analgesic neurotransmitter leucine-enkephalin (Leu-Enk). Trimethyl chitosan nanoparticles could increase the permeability of the peptide across porcine nasal mucosa 35 times, leading to a significant increase in the antinociceptive effect. 66 Liposomes coated with a chitosan derivative have also been proposed for nasal delivery. Liposomes loaded with ghrelin were prepared by the lipid film-rehydration-extrusion technique, followed by coating with N-([2-hydroxy-3-trimethylammonium] propyl) chitosan chloride (HTCC). The chitosan-coated liposomes bound mucin more efficiently than the uncoated anionic liposomes and improved permeation. 67 Clementino et al.68,69 developed hybrid chitosan–lipid nanocapsules for drug (statin) delivery. The nanocapsules with sizes of 200 nm and that were positively charged, were administered intranasally to rats and showed a higher intake rate than free-standing drugs. Another study developed a mucin-controlled drug release system from mucoadhesive phenylboronic acid-rich nanoparticles (PBNPs) that specifically adhered to mucin (Figure 3(b)). 70

Exemplar studies on the development of mucoadhesive or mucus-penetrating nanoparticles. (a) Mucoadhesive nanoparticles based on chitosan-coating for binding to negative-charged mucus layer. (b) Mucoadhesive nanoparticles based on phenylboronic acid-rich nanoparticles (PBNP) for adhesion to mucin and mucin-controlled drug release. (c) Mucus-penetrating nanoparticles by low molecular weight PEG coating. (d) Mucus-penetrating nanoparticles based on NAC-coating by reducing mucus viscosity.
On the other hand, the mucus-penetrating nanoparticles had their surface modified to reduce mucoadhesion (Figure 3(c)). Mucus is a dense molecular network with a mesh spacing (20–500 nm) that prevents the diffusion of larger particles through it.71,72 Thus, the use of sufficiently small nanoparticles coated with proper polymers that minimize interactions with mucins, may increase their penetration through the mucus layer. Polyethylene glycol (PEG) is often used to coat the surfaces of polymeric nanoparticles. For example, the presence of PEG on the surface of PLA nanoparticles at high density was shown to enhance nanoparticle transportation within the nasal mucosa when administered intranasally to rats. 73 Furthermore, nanoparticles of 100 and 200 nm coated with low MW PEG were also shown to penetrate the mucus of individuals suffering from chronic rhinosinusitis effectively. 74 The unique characteristics of nanoparticles, such as, the small size (<200 nm) and negatively charged surface (ζ potential between −15 and −30 mV), makes them favorable for drug delivery across the nasal mucosa (and even to brain transport), and superior to naked drug delivery. When poly (lactic-co-glycolic acid) (PLGA)/PEG nanostructured particles loaded with resveratrol (RSV) were used to treat a mouse nasal polyp model, polyp formation was inhibited, and epithelial integrity was increased. 75 The lipid was also combined with PEG to coat the PLGA nanoparticles as an effective mucus-penetrating nanocarrier of the drug. Although the work was actually aimed at nose-to-brain delivery, the highlighted point was that the dose fraction accumulated in the liver and spleen was significantly reduced, confirming a higher safety of the nasal treatment via a mucus-penetrating approach. 76
Another approach for designing mucus-penetrating nanoparticles is in conjugation with a mucolytic agent to disrupt the mucus barrier (Figure 3(d)). N-acetyl-L-cysteine (NAC), a potent mucolytic agent, remarkably enhanced nasal absorption of large molecular weight compounds, in combination with nonionic surfactants. 77 NAC can disrupt the mucus structure by substituting the free thiol (sulfhydryl) group for the disulfide bonds connecting with mucin proteins, resulting in its clinical use in bronchopulmonary diseases to reduce both the viscosity and tenacity of mucus, as well as to facilitate its removal.77,78
Discussion and outlook on nanoparticle-based therapies
Along with the design of nanoparticles to be mucoadhesive or mucus-penetrating, other properties might be helpful in future developments. Some of the intrinsic properties of the newly developed nanoparticles, such as enzymatic activity, require special attention to treat olfactory injuries. The enzymatic activity involves catalase-, superoxide dismutase-, oxidase, and peroxidase-like properties; thus, the nanoparticles developed to have these properties can play roles similar to those of the body’s natural antioxidant enzymes.79,80 For example, nanoparticles such as cerium oxide (CeO2), copper oxide, and polyoxometalate (POM), have been shown to exert some of those properties in vitro and in vivo and were thus highly effective in scavenging reactive oxygen species (ROS) under oxidative stress conditions (e.g. inflamed tissues such as osteoarthritis, skin infection, and spinal cord injury).81–84 Acute injuries and infections in the olfactory system mostly entail severe inflammation with excessively generated ROS; thus, using such enzymatic nanoparticles would help attenuate local inflammation, possibly contributing to olfactory tissue recovery; this, however, requires further investigation. Furthermore, when the enzymatic nanoparticles are modified to be mucoadhesive or mucus-penetrating and to deliver drugs, their therapeutic functions in inflamed olfactory tissues could be synergized and potentiated, which constitutes a potential future research area.
While we focused on nanoparticle delivery to the site of olfactory injuries, nasal delivery often reaches the brain region, and thus, olfactory dysfunction is closely linked to brain diseases. Recently, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has been shown to significantly influence the respiratory and central nervous systems, leading to anosmia and several neurological diseases.85,86 Olfactory dysfunctions caused by sensorineural or traumatic etiologies are difficult to treat clinically. Although researchers and medical companies are focusing on developing drugs for anosmia and SARS-CoV-2-induced anosmia, there are few reports on the use of nanoparticles to treat anosmia. As a key mechanism of sensorineural/traumatic anosmia, the disruption of the olfactory neurons is considered 87 ; therefore, strategies for drug delivery from intranasal to brain are thought to be a promising treatment option.69,88,89 As listed in Table 2, some of the nanocarrier systems developed for nose-to-brain delivery are also based on mucoadhesive or mucus-penetrating polymeric nanoparticles, with compositions such as lipids, fatty acids, PEG, PEG-PLGA, and Pluronic F127.69,90,91 The olfactory sensory neurons directly cross-talk with the brain and central nervous system, so nanoparticle-based therapeutics through the route of nose-to-brain would be a promising therapeutic strategy to address olfactory dysfunction.
Nanocarriers with mucoadhesive or mucus-penetrating property developed for the intranasal drug delivery.

FTA: farnesylthiosalicylic acid; SLN: solid lipid nanoparticles.
Stem cell-based transplantation therapies
Stem cells have self-renewal potential and multi-lineage differentiation properties and have therefore been used for therapeutic purposes in regenerative medicine. In particular, multipotent adult stem cells including hematopoietic stem cells (HSCs), mesenchymal stem/stromal cells (MSCs), and fetal tissue-derived stem cells, can be specialized more toward tissue- and lineage-specific cell types; thus, a wide range of clinical trials have been performed for over 60 years. 109 Although these stem cells have beneficial effects in regenerative medicine in vitro, several pathophysiological conditions such as hypoxia, restricted nutrient supply, oxidative stress, and inflammation, suppress the therapeutic efficacy in vivo. Thus, to enhance stem cell functions against pathophysiological conditions, recent studies on stem cell-based therapy have adopted new technologies such as virus-mediated transduction of stem cells, gene-editing tools, optogenetics, chemogenetics, extracellular vesicles (EVs), and application of nanoparticles.109–111
Therapeutic evidences of stem cell transplantation to olfactory dysfunctions
Various cell transplantation treatments have recently been studied for the restoration of dysfunctional olfactory system (Table 3). Transplanted stem cells are more likely to secrete beneficial substances (proteins such as growth factors or exosomes) that help the survival and regeneration of target cells, rather than directly differentiating to provide new cell sources.112,113 Among other secretome molecules, neurotrophic factors enhance neuronal survival, regulate progenitor cell proliferation, and promote neurogenesis.114–116 For example, nerve growth factor (NGF) is known to transport to OE, and its presence in OE can modulate neuronal turnover.117,118 Additionally, brain-derived neurotrophic factor (BDNF) has been implicated in generating and differentiating new olfactory receptor neurons. 119 The upregulation of neurotrophic factors by the stem cells transplanted to the olfactory injury sites would thus be a promising approach for increasing the healing capacity of dysfunctional olfactory systems.
Stem cell therapies used to treat olfactory dysfunctions.
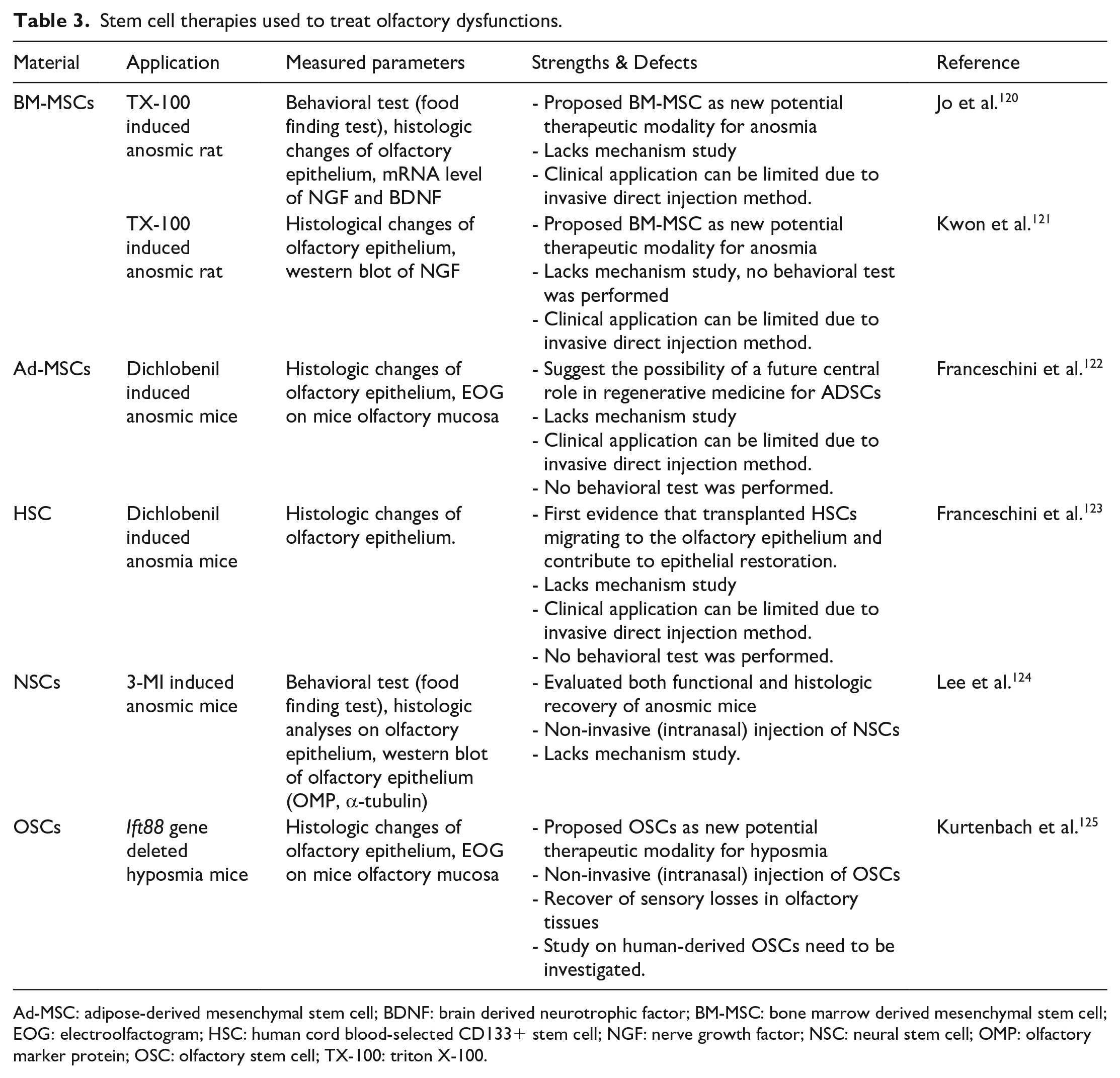
Ad-MSC: adipose-derived mesenchymal stem cell; BDNF: brain derived neurotrophic factor; BM-MSC: bone marrow derived mesenchymal stem cell; EOG: electroolfactogram; HSC: human cord blood-selected CD133+ stem cell; NGF: nerve growth factor; NSC: neural stem cell; OMP: olfactory marker protein; OSC: olfactory stem cell; TX-100: triton X-100.
Tissue healing, including those in the olfactory system such as repairing endothelial cells and sensory neurons, entails neo-blood vessel formation and angiogenesis. MSCs are known to induce and secrete angiogenic cytokines. 126 Therefore, MSCs are an effective therapeutic cell source for the treatment of anosmia. In a recent representative study, bone marrow-derived MSCs (BM-MSCs), adipose tissue-derived MSCs (Ad-MSCs), and HSCs were transplanted into an OE degeneration rat model (Figure 4(a)). 120 The intranasal injection of BM-MSCs could augment the thickness and cellular composition of the OE to the normal level. In addition, the restoration rate of olfactory functions due to the BM-MSC injection was significantly enhanced compared to that of the control group. 120 This study also found a close relationship between the restoration of olfactory functions and the activated neurotrophic factors, including NGF and BDNF. In another study, in a rat anosmia model, the transplantation of BM-MSCs promoted the morphological restoration of the olfactory mucosa when compared to the contralateral control side. 121 Franceschini et al. 122 transplanted Ad-MSCs into immunodeficient mice with permanent damage in the dorsomedial olfactory region induced by dichlobenil inoculation (Figure 4(b)). The transplanted cells integrated into the lesioned OE and clusters of differentiated cells were observed in the epithelium. 122 In particular, there was a marked increase in the thickness of the OE and the expression of OMP in the Ad-MSC transplanted group compared to the control group.
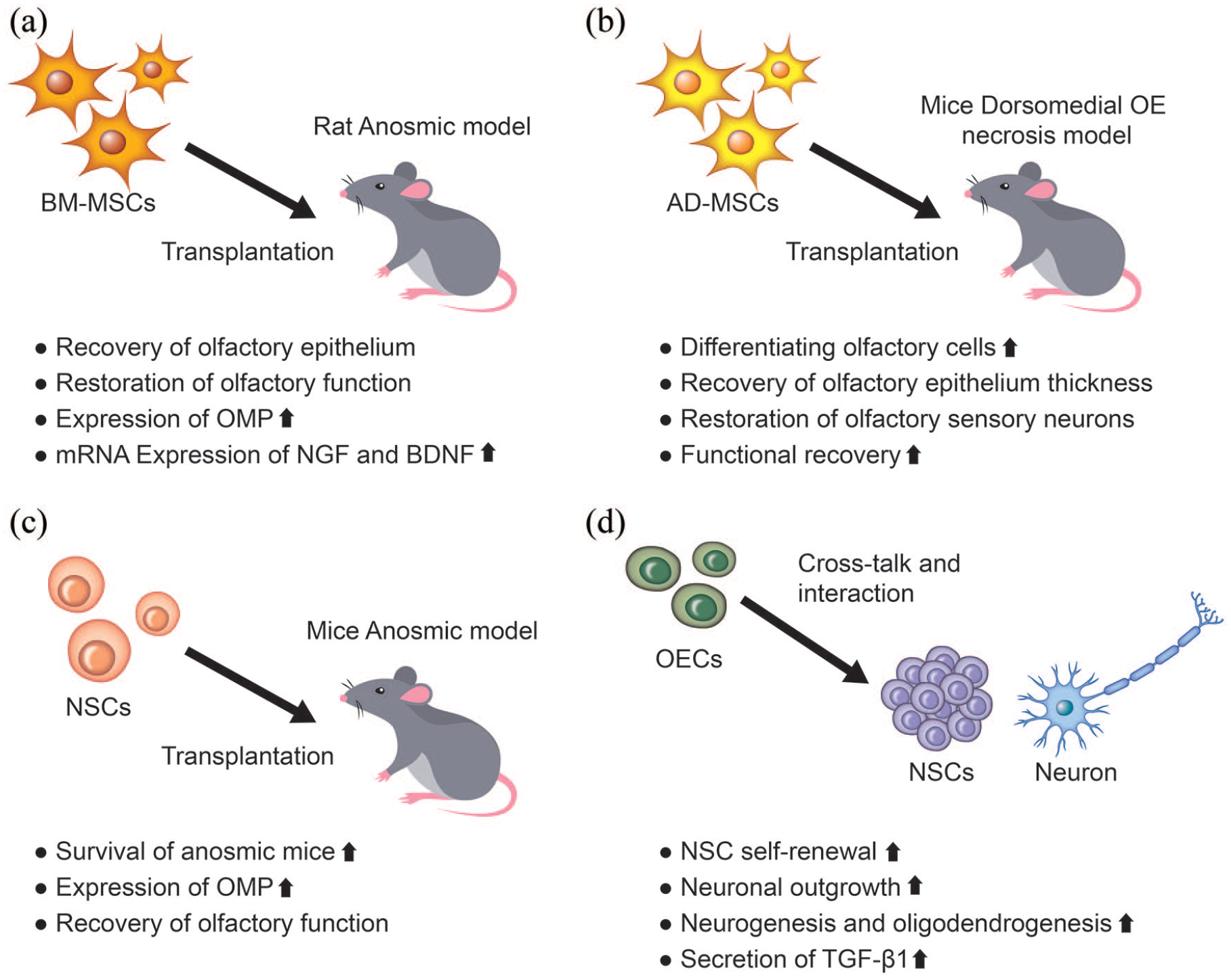
Application of stem cell transplantation in olfactory dysfunction and the regenerative effects of cell-based therapeutics.
Other types of stem cells have also shown therapeutic efficacy in restoring olfactory dysfunction. One study has shown that HSCs transplanted into injured OE of NOD-SCID mice resulted in improved neuronal recovery, with an increased expression of GAP43. 123 Lee et al. 124 investigated neural stem cells (NSCs) as a potential treatment for olfactory dysfunction (Figure 4(c)). The olfactory bulb-derived NSCs recovered olfactory function and the expression of OMP in a murine OE-injured model. Compared to the control, NSC-treated mice showed a better recovery of olfactory function in terms of the food-finding test and the expression of OMP. 124 Olfactory ensheathing cells (OECs) are a unique glial cell type that ensheathe olfactory axons into large bundles as they traverse from the lamina propria to the nerve fiber layer of the olfactory bulb. They express guidance cues and extracellular matrix molecules to assist in the growth and provide directional and tropic support to the primary neurons to reach the olfactory bulb (Figure 4(d)). 127 A recent study revealed that OECs secrete transforming growth factor β1 (TGF-β1), which can increase their phagocytic activity by regulating integrin/milk fat globule-epidermal growth factor (EGF) factor 8 (MFG-E8) protein signaling pathway. 128
Discussion and outlook of stem cell-based therapies
As noted, stem cell transplantation to the dysfunctional olfactory system is effective with convincing evidence. However, a couple of issues remain that need to be addressed. First, the cells considered as the stem cells of the olfactory nerve epithelium have not been accurately identified in the molecular biology context, which makes it difficult to determine the differentiated fate of transplanted stem cells and their possible specific roles. Second, it is also unclear what kinds of biochemical factors are essentially involved in the differentiation of stem cells into olfactory-specific cells, complicating the identification of the decisive role of secreted molecules from the transplanted cells. In addition, the effects of injection route, injection dose, number of administrations, and source of stem cells used for olfactory dysfunction, have not been well examined, requiring more systematic studies in the area. Given that these issues are addressed in the future, we may identify the fate of stem cells transplanted (whether they are differentiated or not, and if so, what fraction and which lineage cells would be) and the mechanisms underlying the differentiation into specific cell types that are needed for the recovery of dysfunctional olfactory tissues.
As the surrounding matrix influences stem cell properties, such as survival and differentiation capacity, it is highly recommended to use biomaterials and scaffolds for stem cell delivery. Many hydrogels and 3D scaffold systems for the delivery of stem cells have been developed with tunable physico-mechano-chemical properties such as stiffness, dynamic mechanical properties (e.g. stress relaxation), ligand type, and density.129–132 Depending on these extracellular matrix properties, the biological fate of stem cells can be modulated. For example, when MSCs were cultured in stress-relaxing hydrogels, their differentiation into osteogenic or chondrogenic lineage was significantly enhanced compared to those in non-stress-relaxing hydrogels,133,134 implying the importance of dynamic mechanical properties of hydrogels in cell fate determination. In addition, the ligand type of 3D scaffolds primarily determined the lineage differentiation of NSCs,135–137 demonstrating the difference in initial cellular perception of the extracellular matrix ligand governing the intracellular signaling that leads to altered cell fate. Therefore, future studies on stem cell delivery to the olfactory system are needed that use the hydrogels and 3D scaffolds that are designed to specifically stimulate the cells to induce secretome and/or differentiate to the cells helpful for the recovery of dysfunctional olfactory tissues.
Although here we focused on the delivery of stem cells, their secretome such as extracellular vesicles (EVs), are considered to be of utmost importance as an alternative to stem cells because of their merits over living cells, including delivery to target specific cell types, less immune responses, stabilization in the body, and the ability to contain drugs.111,138 Some of the applications of EVs to dysfunctional tissues such as kidney diseases, cardiovascular diseases, bone defects, fibrosis, stroke, and spinal cord injuries, have shown the therapeutic efficacy of EVs to levels comparable to those treated with conventional stem cell delivery approaches.111,138–140 The applications of stem cell-based therapies for the dysfunctional olfactory system are still in infancy; thus, future strategies need to harness the new technologies that progress in scaffold development and EV biogenesis, in order to potentiate the cellular capacity for regenerating the dysfunctional olfactory tissues.
Footnotes
Authorship
Shin Hyuk Yoo and Hae-Won Kim contributed to the concept of the work, data acquisition, and drafting of the manuscript and revised the article critically for important intellectual content. Jun Hee Lee designed the study, drafted the manuscript, procured funding, and supervised the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present research was supported by the research fund of Dankook University in 2020.