
Abstract
The gastrointestinal (GI) tract has a diverse set of physiological functions, including peristalsis, immune defense, and nutrient absorptions. These functions are mediated by various intestinal cells such as epithelial cells, interstitial cells, smooth muscle cells, and neurocytes. The loss or dysfunction of specific cells directly results in GI disease, while supplementation of normal cells promotes gut healing. Gut bioengineering has been developing for this purpose to reconstruct the damaged tissues. Moreover, GI tract provides an accessible route for drug delivery, but the collateral damages induced by side effects cannot be ignored. Bioengineered intestinal tissues provide three-dimensional platforms that mimic the in vivo environment to study drug functions. Given the importance of gut bioengineering in current research, in this review, we summarize the advances in the technologies of gut bioengineering and their applications. We were able to identify several ground-breaking discoveries in our review, while more work is needed to promote the clinical translation of gut bioengineering.
Introduction
Functions of the gastrointestinal (GI) tract mainly include food digestion and absorption of nutrients for support of daily activities. These functions are mediated by a diverse set of cells in different layers of the GI wall. The GI wall consists of mucous, submucous, muscular, and serosal layers.1,2 In the small intestine, for example, the mucous layer contains absorptive enterocytes, goblet cells, enteroendocrine cells, Paneth cells, stem cells, lymphocytes, as well as a small number of smooth muscle cells. These cells have diverse functions including absorption of nutrients, secretion of digestive juice, immune defense, and maintaining gut microbiota homeostasis. The submucous layer consists of connective tissues where small blood vessels and lymph vessels nourish the mucous layer and facilitate lymphatic return. Smooth muscle cells comprise the muscular layer in a circular and longitudinal arrangement. This layer is innervated by the enteric nervous system and is responsible for intestinal motility. 3 The serosal layer consists of mesothelial and connective tissues that lubricate the surface, preventing intestinal adhesions. Hence, the complexity in the architecture and functions of the GI tract make its repair and regeneration difficult.
Gut bioengineering has developed from cell-free tissue scaffolds to the current use of constructing artificial GI tracts with native physiological function. 4 Gut diseases result from loss or dysfunction of one or more cell types. Reversing the abnormal status of pathogenic cells has been considered crucial to treatment of gut diseases. Therefore, it is important to know which cells to be used in gut bioengineering for a specific disease. Here, we summarize the current techniques of gut bioengineering and discuss some major concerns that were encountered from bench to bedside. Although gut bioengineering was mostly completed at the laboratory stage at the moment, it has been extensively applied in pharmaceutical research, serving as an ex vivo three-dimensional gut model to study drug-triggered host responses. We will also address this topic in our review.
The types of gut diseases determine the cells used in gut bioengineering
Currently, most gut diseases are treated with pharmacotherapy or surgical resection; however, these inevitably lead to some complications. For example, mesalazine and infliximab are recommended for treatment of inflammatory bowel disease (IBD), but these drugs can cause local and systemic toxicity, or are not effective.5,6 Surgical intervention is chosen to manage GI tumor or traumatic rupture of the GI tract; however, some severe postoperative complications may occur, reducing quality of life, such as gastroparesis, stricture, fistula, and even short bowel syndrome after wide resection. Hopefully, gut bioengineering will provide a new method in improving prognosis. IBD is manifested by exaggerated inflammatory responses in the intestinal epithelia, and basic research has revealed that restoration of normal gut microbiota can reduce epithelial inflammation and relieve disease activities.7,8 Based on this principle, the feces of healthy people are processed and then the normal gut microbiota is transplanted into the diseased colon in IBD patients. This is known as fecal microbiota transplantation (FMT). However, some patients are unresponsive to FMT, possibly due to the challenges in the selection of appropriate fecal composition 9 and irreversible inflammatory necrosis of the intestinal epithelia in severe disease. 10 Under such circumstances, direct replenishment of normal intestinal cells or gut tissues would be a permanent solution. The cells or tissues involved in the pathogenesis of the gut diseases would be considered as therapeutic targets. For example, ulcerative colitis is restricted to the mucosa and submucosa; therefore, we can use tubular tissues comprising all the cell types in these two layers to repair the damaged gut. However, Crohn’s disease involves transmural inflammation, requiring tubular tissues with restoration of both peristaltic and absorptive functions. 4 Gastroparesis 11 and colonic inertia 12 are resulted from the impairment of muscular layer. Maintaining the neuromuscular function by supplement of neurons and reconstruction of smooth muscle can restore motility. Table 1 lists the histological structures that need repair in common gut diseases.
Characteristics of common gut diseases and corresponding strategies of gut bioengineering in principle.
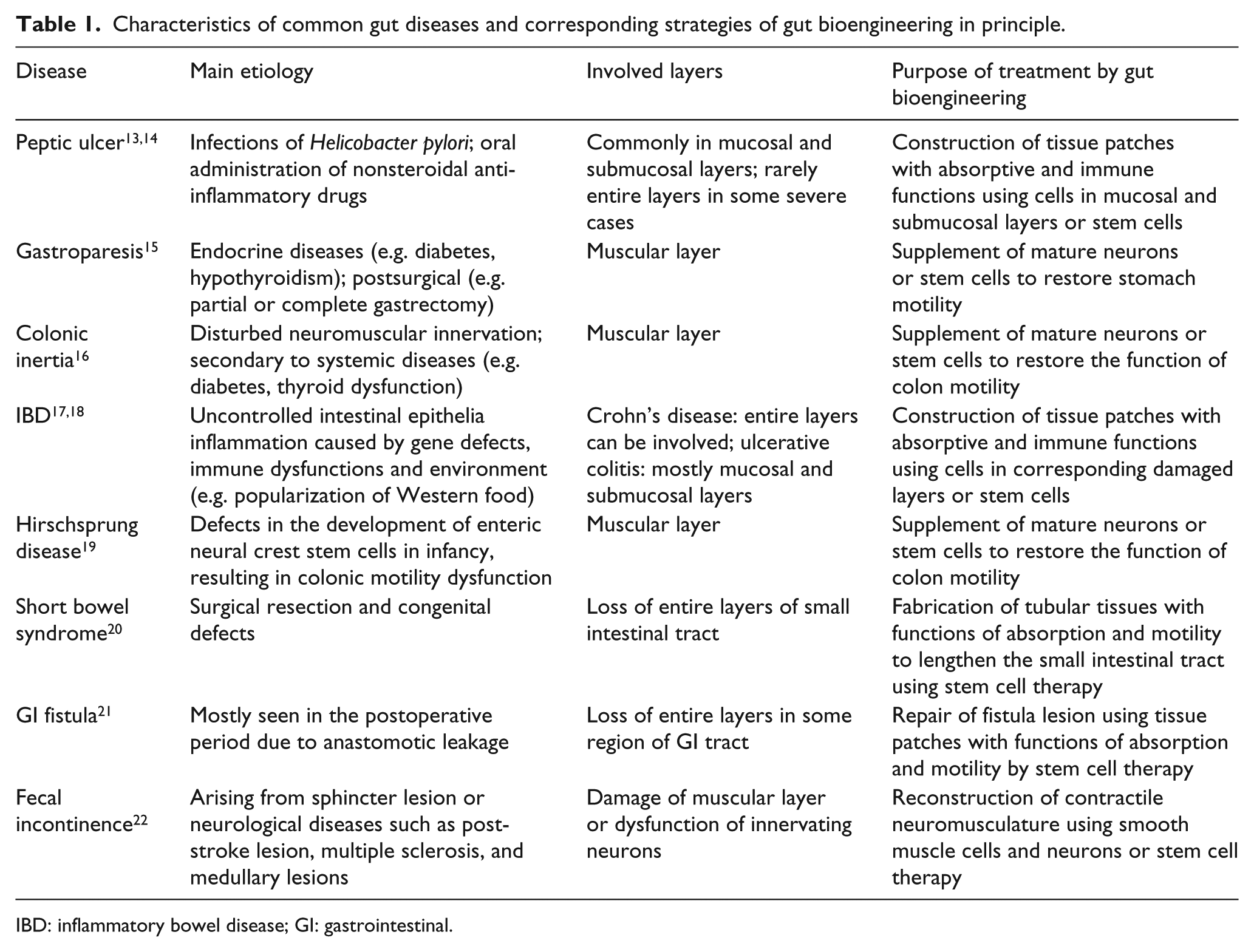
IBD: inflammatory bowel disease; GI: gastrointestinal.
Techniques of gut bioengineering
Cell-free scaffolds
Gut bioengineering is a branch of tissue engineering that restores gut anatomy and physiology. Since its emergence, gut bioengineering has developed from cell-free scaffolds to intestinal organoids based on advances in biomaterials and cell therapy4,23 (Figure 1). The cell-free scaffolds have a wide range of sources such as decellularized tissues, biologically derived hydrogels, and synthetic scaffolds. Syed et al. 24 generated decellularized intestinal submucosal scaffolds using two methods: perfusion/immersion and immersion/agitation. Their products showed improved biocompatibility and comparable mechanical strength to untreated tissues. Pahari et al. 25 elongated the length of bowel using the decellularized dermal matrix in rat models. They discovered the weight changes of treated experimental groups were similar to age-matched animal models, and the implanted scaffolds supported enterocyte infiltration, differentiation, and growth. Their findings revealed the cell recruitment ability of cell-free scaffolds; however, this process was time-consuming. Biologically derived hydrogels are another type of cell-free scaffold, featured by isolation from components of tissues or organisms such as collagen, hyaluronic acid, silk, xanthan gum, and fibrous protein.26,27 Our group previously reported enzyme-crosslinking fibrin gels that repaired the GI fistula in clinical practice. 28 To overcome the poor stability of fibrin gels in digestive juice, we further developed an anti-digestive hydrogel based on xanthan gum and verified its ability to induce expression of functional tight junction proteins of IEC-6 cells on surface culture. 29 This type of hydrogel allows convenient application by injection, and it is easy to fill in the irregular gut defects, but it still lacks certain biological activities. Synthetic scaffolds are the most widely used technique in repairing gut defects due to their tunable mechanics, porosity, shape, and degradation properties. 30 Our group previously used 3D-printing thermoplastic polyurethane scaffolds to maintain the continuity of the GI tract temporarily. We later examined the scaffolds’ efficacy on nutritional delivery in a clinical trial setting. 31 These scaffolds helped with rapid recovery from GI fistula, but regrettably we did not observe any tissues adhering to the scaffold. The defect was probably due to scaffold’s lack of porous structure. By using porous poly-ε-caprolactone meshes, Diemer et al. 32 found that such scaffolds were degradable and accompanied with ingrowth of epithelial and smooth muscle cells during treatment of esophageal damage in rabbits. Although their findings were encouraging, some rabbits presented with esophageal stenosis, suggesting a scarred tissue-repair program induced by the acellular scaffolds.

Techniques of gut bioengineering. (a) Three main types of tissue scaffolds: decellularized scaffolds, biologically derived hydrogels, and synthetic scaffolds. (b) Decellularized scaffolds promote healing of damaged gut based on their cell recruitment ability. (c) Specific cells can be laden by tissue scaffolds to repair injured gut. (d) Intestinal organoids that mimic gut anatomy and physiology are constructed to treat defects in intestinal tissues. (e) The application methods of intestinal organoids in gut repair. ESCs: embryonic stem cells; ISCs: intestinal stem cells; PSC: pluripotent stem cells.
Cell-laden scaffolds
Attempts are being made to construct artificial GI tracts by combining scaffolds and tissue-specific cells or stem cells. The properties of the scaffolds regulate the cell fate, including biocompatibility, porosity, stiffness, and surface topography. Decellularized matrix, 33 collagen-based scaffolds, 34 and chitosan-based hydrogels 35 have been tested for cell-laden potentials. These scaffolds are anchored with abundant amino groups that can support cell adhesion and are biocompatible to living tissues.26,36 For example, Cruz-Acuna et al. 37 decorated the PEG-4MAL hydrogel with protease-cleavable peptides containing terminal cysteines, which established an appropriate environment for growth and differentiation of human pluripotent stem cells (PSCs) to repair colonic injury. Zakhem et al. 38 constructed a tissue-engineered bowel by rolling innervated smooth muscle sheets around chitosan scaffolds and validated the contraction of the bowel following omentum implantation. The porosity of scaffolds is essential for water and nutrient exchange for seeded cells with an outer environment, 39 which provides space for cell spreading 40 and cell footholds.41,42 As for the stiffness, adequate strength is important for successful anastomosis; otherwise, the scaffolds would be ruptured and lead to leakage. Another role of stiffness is to regulate cell proliferation, differentiation, and functionalization 29 , 43 but the value in the achievement of the optimal status of intestinal cells needs to be precisely determined. In addition, Costello et al. 44 created scaffold topography in the shape of intestinal villi, which enabled cell differentiation along the villous axis. This 3D villus model was found to have strong physiological relevance to native tissues and act as an in vitro intestinal model. Altogether, even seeding cells is a good choice; the fate of cells is strongly associated with the above properties of scaffolds, which merit careful consideration.
Intestinal organoids
Although cell-laden strategies have added bioactivities to the scaffolds, there have been concerns about the phenotype alteration of specific cells during cell culture and failure of the subsequent cell transplantation.45–48 The intestinal organoid techniques can generate all layers of the gut architecture with gene and phenotype stabilities.49–52 The bottoms of intestinal crypts contain crypt base columnar (CBC) cells that are positive for G protein-coupled receptor 5 (lgr5) and are regarded as intestinal stem cells. The CBC cells are capable of self-renewal and differentiation into various intestinal epithelial cell types to maintain the integrity of the crypt-villus structure. 53 The differentiation ability is stronger providing the CBC cells are harvested from young donors. 54 Through biopsy and subsequent cell dissociation, crypts or single CBC cells are isolated from human GI tract and then cultured in Matrigel,55,56 which is commonly used to offer a physiological 3D environment for organoid culture. The CBC cells are differentiated when cultured in the specific medium, but they can maintain their location-specific identity (duodenum, jejunum, ileocolon) over a long period of time, or even when heterotopically transplanted into another part of the bowel.57–59 Apart from the CBC cells, the human ESCs and induced PSCs can be used to generate intestinal organoids as well by a temporal series of growth factor manipulations. 60 The underlying mechanisms are the selective roles of compounds in culture medium on activation or inhibition of Wnt, 61 Notch,62,63 epidermal growth factor (EGF), 64 bone morphogenetic protein (BMP),65,66 transforming growth factor-β (TGF-β), 67 as well as signal transducer and activator of transcription 3 (STAT3) 68 signaling pathways (Figure 2).

Regulation of intestinal organoid formation by different growth factors. (a) The biomolecule-signaling pathway-effect axis during construction of intestinal organoids. Arrows show activation of signaling pathway. Lines without arrowheads show inhibition of the signaling pathway. (b) Integration of several specific growth factors determines the differentiation direction of stem cells by regulating Wnt and Notch signaling pathways. For example, activation of Wnt and Notch signaling pathways causes self-renewal of stem cells. Inhibition of Wnt signaling pathway by IWP-2 leads to differentiation of enterocytes (VIL1+), while inhibition of Notch signaling pathway by DAPT leads to differentiation of other cell types such as goblet cells (MUC2+), enteroendocrine cells (CHGA+), and Paneth cells (DEFA5+) depending on the subsequent switch of Wnt signaling pathway. CHIR: CHIR99021; IL-2: interleukin-2; VPA: valproic acid.
The engineered intestinal organoids can grow into mature intestinal tissues in vivo when transplanted into bodies including the kidney capsule,37,69 peritoneal cavity, 70 mesentery, 71 injured colonic wounds,37,72 and even side-to-side small intestine anastomosis. 73 Liu et al. 74 compared the five locations for intestinal organoid incubation (omentum, intestinal mesentery, uterine horn membrane, abdominal wall, and subcutaneous space) and found that three vascularized membranes (omentum, mesentery, and uterine horn) produced the largest quantity and highest quality of intestinal organoids, and wrapping with omentum and mesentery may produce intestinal organoids that are most easily anastomosed with host intestine. 71 Besides, dynamic mechanical forces play a central role in intestinal organoid development and morphogenesis. Poling et al. 75 incorporated compressed nitinol springs in intestinal organoids and found that the strain-exposed tissues exhibited higher similarities to native human intestine, with regard to tissue size and complexity, and muscle tone. Overall, the technique of intestinal organoids provides new tools for gut repair and regeneration.
Challenges of gut bioengineering for clinical translation
Cell-free scaffolds
Acellular scaffolds are easily available and permitted for clinical applications; however, various factors limited the degree of applications. First, the pathological GI tract may lose its normal morphology and anatomy. Intestinal mucosal edema leads to stricture of the bowel lumen, and abdominal cavity adhesion causes irregular arrangement of the bowel. Therefore, the GI tract is fragile to the implanted scaffolds, especially when the scaffolds do not match well with the GI anatomy or during intestinal peristalsis. For example, we previously reported that a fistula patch could be used to close the enteroatmospheric fistula. 76 On the other hand, this approach can sometimes injure the surrounding mucosa and consequently causes bleeding if the patch does not fit the fistula shape. To overcome this issue, we fabricated patient-personalized scaffolds by further defining the intestinal lumen diameter and the angle at the lesion position using 3D-reconstructed intestinal images.31,77 Moreover, in vivo studies have found that wound infection or moderate inflammation occurs in some cases after scaffold implantation,78,79 which may lead to treatment failure. More importantly, the acellular scaffolds usually result in a scarred repair process due to the lack of bioactivity, which may cause severe complications such as intestinal stenosis and even obstruction. Therefore, we restrict application of the acellular scaffolds to small lesions of gut to prevent large scar formation.
Cell-laden scaffolds
Seeding the primary intestinal cells or cell lines improves the biological functions of scaffolds. However, these cells may undergo phenotypic transformation during development of intestinal tissues, ultimately impairing their specific functions. For example, smooth muscle phenotypes have been identified as myoblasts, immature myocytes, and mature smooth muscle myocytes.80,81 The mature smooth muscle myocytes represent the contractile phenotype and are important for GI tract motility, but they are transformed into synthetic, proliferative, and possibly migratory phenotypes when mature smooth muscle myocytes are isolated from in vivo environments and cultured.82,83 This directly reduces the contractile force of engineered smooth muscle layers. Chen et al. 49 demonstrated lower gene expression of intestinal epithelial cell markers for primary intestinal cells and cell lines compared with those of CBC cells after culture in Matrigel. This suggests that the functions of mature cells are impaired when cultured in vitro. Costello et al. 84 demonstrated the expression of functional protein genes in intestinal epithelial cells was decreased by the lack of physiological fluid shear, indicating the loss of physiological environment could lead to cellular function disorders. 85 Therefore, retaining the phenotypes of mature cells will still be a major challenge during in vitro culture.
Intestinal organoids
Transplanted intestinal organoids resemble the real histology of intestinal tissues with stable cellular phenotypes, allowing application of injection or direct anastomosis to the discontinuous GI tract.37,71 However, the intestinal organoids do not match well with the anatomy of the GI tract and may encounter failure during the anastomotic procedures. Shaffiey et al. 72 fabricated a Matrigel-coated tube-shaped PLGA scaffold, which was used to attach the intestinal stem cells. It displayed improved generation of intestinal organoids that exhibited an anatomically relevant shape and was easily transplanted for mucosal healing. Given its importance, more work needs to be undertaken on preparing scaffolds that can maintain the tubularized structure of intestinal organoids. Moreover, the donor source of stem cells merits consideration. Allotransplantation requires that stem cells are isolated from an HLA-matched donor and the recipients are treated with immunosuppressive therapy for prevention of graft rejection. The autotransplantation of engineered intestinal organoids does not come up against graft rejection problems; however, studies have shown that organoids developed from abnormal gut lesions (e.g. IBD and tumor) preserve the pathogenetic genes and tend to grow to be unhealthy tissues,86,87 limiting the use of autotransplantation. Gene editing using CRISPR/Cas9 offers the possibility of correcting the genetic errors and makes the intestinal stem cells qualified candidates for generation of autotransplantable organoids. For example, Schwank et al. 88 used the CRISPR/Cas9 editing system to amend the CFTR locus in the intestinal stem cells of cystic fibrosis patients, consequently restoring CFTR function in corrected organoids. Zafra et al. 89 further introduced a high-efficiency base editing method to re-engineer the sequences of BE3, BE4Gam, and xBE3 through codon optimization and incorporation of additional nuclear-localization sequences in intestinal organoids. The surgical procedures on implantations of intestinal organoids also deserve our discussion. Currently, the intestinal organoid transplantation is mainly depended on endoscopic injection 37 or surgical replacement. 90 These attempts have been done on various animal models such as mice, rats, dogs, and swine. 91 Of note, some cases demonstrated that surgical complications such as wound infections and hernia would cause the treatment failure and even death. In an updated study, Ladd et al. 92 compared the effects of intestinal organoid anastomosis using three surgical types and concluded that a single operation with a defunctionalized loop of small intestine may be an optimal approach. Undoubtedly, such efforts are important for clinical translation of intestinal organoids, and more work is needed for establishing standardized surgical methods.
Gut bioengineering for pharmaceutical research
Drugs administered orally are usually absorbed in the small intestine, but can simultaneously cause damage to the epithelia. The two sides must be evaluated before drugs are applied in clinic. Many preclinical models have therefore been established, including 2D monolayer culture in the Transwell plate, 3D monolayer culture, and 3D intestinal organoids. Compared with the conventional 2D culture, 3D cell models facilitate cell growth and polarization, which are much more similar to native intestine. For example, Yu et al. 93 showed a 3D monolayer culture platform by seeding Caco-2 cells onto the 3D collagen villus scaffolds and found that the drug permeability coefficient was 13 times higher than that in a 2D monolayer culture platform. Caco-2 cells can immediately polarize, differentiate into a columnar epithelium, and form undulating structures that are reminiscent of intestinal villi.94–96 However, Caco-2 cells were originally isolated from tumor samples, and they harbor multiple gene mutations. Human primary intestinal cells were alternatively used to construct the intestinal models. 97 For instance, Madden et al. 98 revealed the genetic similarity of a bioprinting 3D primary human intestinal model to the native human intestine. More excitingly, their model presented an intact mucosal layer that could visualize the mucosal injury and reflect drug toxicity during the co-culture of drugs. Intestinal organoids derived from human stem cells also express normal genes and exhibit critical physiological intestinal functions. Gunasekara et al. 99 described a method that a planar array of colonic organoids can measure enterotoxins by the responsive swelling extent and the rate of fluid movement across the organoid wall based on automated image assays. Moreover, the pharmacokinetic analysis can also be performed using intestinal models. For example, Onozato et al. 100 constructed PSC-derived intestinal organoids and identified the differential activities of drug efflux transporters and the differential expression of the drug-metabolizing enzyme cytochrome P450 in the presence of different drugs. More importantly, intestinal organoid models can be used in personalized medicine. Yan et al. 101 established a biobank of patient-derived gastric cancer organoids that maintained long-term similarity to the original tumors. They used the organoids to perform large-scale high-throughput drug screening that identified potential drugs targeted to different signaling pathways. However, traditional 3D models ignore the natural mechanical microenvironment of the normal gut that has trickling fluid flow and rhythmic peristaltic motions; thus, the gut-on-a-chip microdevices have emerged (Figure 3).102,103 Such a gut-on-a-chip can represent disease models for drug screening by adding specific interventions. For instance, Jalili-Firoozinezhad et al. 104 exposed the gut-on-a-chip to γ-radiation and demonstrated a series of pathological features, such as excessive oxidative stress in intestinal cells and disruption of intestinal barrier integrity, resembling radiation-induced gut injury. This disease model has potential in screening for novel radioprotective medical countermeasure drugs. In spite of the advances in drug screening models, in vivo drug studies are still indispensable because they can provide important systemic parameters such as drug distribution and clearance, while in vitro models representing a single organ cannot.

Existing cellular microdevices for drug screening and their features. (a) The traditional Transwell plate for 2D culture of Caco-2 cells. (b) The modified Transwell plate containing villus-shaped hydrogels for 3D culture of Caco-2 cells. (c) The 3D culture of intestinal organoids. (d) The Caco-2 cells can polarize and differentiate into a columnar epithelium with the appearance of intestinal villi when cultured on the mechanically relevant chip. (e) The modified gut-on-a-chip containing villus-shaped hydrogels for 3D culture of Caco-2 cells. (f) The various cells from intestinal organoids can polarize and assemble as the finger-like villi when cultured on the chip. Arrows in the same color represent the in vitro intestinal models before and after integration of microfluidic chip (the schematic diagram of microfluidic chip was from Kasendra et al.). 102
Real-time monitoring represents the future direction of rapid drug screening. Combined with this feature, existing cell models show greater convenience and efficiency in the definition of drug effects. For example, transepithelial electrical resistance (TEER) is a real-time quantitative method that indicates the integrity of tight junctions in the monolayers of intestinal epithelia. 105 The tight junctions are critical in the maintenance of gut homeostasis, serving as indicators of the efficacy and toxicity of tested drugs. The baseline of TEER is variable, affected by cell types, culture media, and detecting systems. 106 Besides, microinjection of fluorescein-isothiocyanate-labeled dextran into intestinal organoids will demonstrate different epithelial barrier dynamics after exposure to experimental compounds.107–109 The barrier dynamics here reflect the drug’s efficacy. Moreover, the intestinal cell models release some specific molecules if damaged, such as tetrathionate (S4O62−) and NO, which can be identified using the two-component regulatory system 110 or NorR-targeted genetic circuit, 111 respectively. These sensor genes along with fluorescence protein reporter are integrated into bacterial genes, allowing us to evaluate the level of cell models injury through fluorescence intensity; however, there is a short delay (~1 h) from the molecule sensing to fluorescent protein expression. The above real-time methods have expanded our tools to study the interactions between drugs and some aspects of gut function such as barrier functions and inflammation levels. In the next step, we advocate evaluating other gut functions such as brain-gut axis in a real-time manner by measuring neuron-firing activities or neurotransmitter concentrations. The innervated intestinal organoid models have been built by Workman et al. 112 They recapitulated normal enteric nerve system (ENS) development by combining PSC-derived neural crest cells and developing intestinal organoids. ENS-containing intestinal organoids grown in vivo formed neuroglial structures similar to a myenteric and submucosal plexus, had functional interstitial cells of Cajal, and showed contractile activities triggered by low-voltage stimulation. This innervated intestinal organoid would help to develop new pharmacotherapy to improve bowel motility and treat constipation.
Conclusion
In this article, we described the technology to conduct gut bioengineering, including acellular scaffolds, cell-laden scaffolds, and intestinal organoids. These techniques can be applied in gut repair and pharmaceutical research, but challenges persist for industrial production and clinical translation. For satisfactory gut repair, the scaffolds should possess the following characteristics: (1) biocompatibility and biodegradability; (2) bioactivity, especially loading specific cells with stable phenotypes and normal functions; (3) anatomical relevance for anastomosis; and (4) mechanical relevance for motility. The four characteristics are absent more or less in the current techniques and our future research will aim to improve the techniques in these aspects. Based on the specific microdevices, the in vitro cell models are properly used for drug screening because the models mimic the in vivo environment of the gut and detection is in real time.
Footnotes
Author contributions
J.H. performed the literature search and wrote the manuscript. J.H. drew the schematic diagrams and participated in the discussion. Y.R. edited and revised the manuscript. J.H., X.W., Z.L., and J.R. conceived this review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Nanjing Science and Technology Development Project (Grant no.201803051), Innovation Project of Military Medicine (Grant no. 16CXZ007), Key Project of Jiangsu Social Development (Grant no. BE2016752 and BE2017722), and National Major Scientific and Technological Special Project for “Significant New Drugs Development” (Grant no. 2018ZX09J18111-04).