
Abstract
Dental pulp represents a promising and easily accessible source of mesenchymal stem cells for clinical applications. Many studies have investigated the use of human dental pulp stem cells and stem cells isolated from the dental pulp of human exfoliated deciduous teeth for bone tissue engineering in vivo. However, the type of scaffold used to support the proliferation and differentiation of dental stem cells, the animal model, the type of bone defect created, and the methods for evaluation of results were extremely heterogeneous among these studies conducted. With this issue in mind, the main objective of this study is to present and summarize, through a systematic review of the literature, in vivo studies in which the efficacy of human dental pulp stem cells and stem cells from human exfoliated deciduous teeth (SHED) for bone regeneration was evaluated. The article search was conducted in PubMed/MEDLINE and Web of Science databases. Original research articles assessing potential of human dental pulp stem cells and SHED for in vivo bone tissue engineering, published from 1984 to November 2017, were selected and evaluated in this review according to the following eligibility criteria: published in English, assessing dental stem cells of human origin and evaluating in vivo bone tissue formation in animal models or in humans. From the initial 1576 potentially relevant articles identified, 128 were excluded due to the fact that they were duplicates and 1392 were considered ineligible as they did not meet the inclusion criteria. As a result, 56 articles remained and were fully analyzed in this systematic review. The results obtained in this systematic review open new avenues to perform bone tissue engineering for patients with bone defects and emphasize the importance of using human dental pulp stem cells and SHED to repair actual bone defects in an appropriate animal model.
Keywords
Introduction
Tissue engineering is a multidisciplinary field based on combination of cells and/or proteins with biomaterials to generate a new tissue. Some factors are very important to succeed in tissue engineering: the choice of stem cell source, the strategies used to isolate and expand the specific cells, the choice of the biomaterial to be used as a scaffold, and the correct association between them. 1 To bone regeneration, it is necessary that the chosen biomaterial allows the cells to migrate, proliferate, and differentiate into bone cells in order to regenerate the bone tissue defect, but also it is necessary that local angiogenesis occurs to provide the necessary nutrients and environment factors for the correct development of the bone tissue. 2
Reconstruction of maxillofacial critical bone defects represents a major challenge in the areas of dentistry and medicine and they are the main objective pursued by several research groups. With this aim in mind, mesenchymal stem cells (MSCs) are being investigated as an appropriate type of stem cells to be used in bone tissue engineering due to their ability to differentiate in both osteoblasts and endothelial cells supporting hematopoiesis. 3 This type of stem cell, despite being classically isolated from bone marrow 4 (bone marrow stromal cells (BMSCs)), can also be obtained from several neonatal and adult tissues, including dental pulp, 5 orbicularis oris muscle, 6 and fat. 7 Many studies are focusing on the isolation of MSCs from more accessible sources aiming for a safer clinical application of these cells for tissue engineering purposes.8–10 In this context, the dental pulp is currently being proposed as one of the most promising source of MSCs for tissue engineering. The advantages that the use of MSCs isolated from dental pulp tissue (dental pulp stem cells (DPSCs)) represent are related to their accessibility and great proliferative and multilineage differentiation potential.5,11,12
Human dental pulp stem cells (hDPSCs) were first isolated and characterized by Gronthos et al. 13 They are extremely proliferative and capable of osteogenic, 11 dentinogenic, 13 adipogenic, 12 chondrogenic, 12 and neurogenic 12 differentiation. A number of studies were conducted in which hDPSCs were used in combination or not with several types of scaffolds and transplanted to repair a number of bone defects in animal models and in human clinical trials.14–16 In particular, a study conducted by Miura et al. 17 was the first study to successfully isolate stem cells from the dental pulp of human exfoliated deciduous teeth (SHED) and to use them associated with a scaffold for bone tissue engineering purposes in vivo. With regard to the method of isolation of both stem cells from human exfoliated deciduous teeth (SHED) and hDPSCs, the main difference between SHED and hDPSC is related to the fact that hDPSCs are isolated from the dental pulp of permanent teeth or isolated from deciduous teeth without exfoliation while SHED are obtained from the dental pulp of exfoliated deciduous teeth.13,17 As a result, SHED represent a more immature than permanent teeth DPSC subpopulation. SHED have higher proliferation rate and differentiation capability in comparison with permanent DPSCs and, considering the ease to obtain deciduous teeth exfoliated of children, the clinical use of SHED may be particularly advantageous. 17 The main objective of this research is, therefore, to present and summarize, through a systematic review of the literature, in vivo studies in which the efficacy of hDPSCs and SHED for bone regeneration was evaluated. Furthermore, this study aimed to assess the influence of host-related factors (animal model and defect type) and the scaffold used on the efficiency of hDPSCs for bone regeneration.
Methodology
An electronic customized search of scientific articles published between 1984 and November 2017 using PubMed/MEDLINE and Web of Science databases was conducted. The following key words were used separately and in combination: stem cells, dental pulp, isolation, human DPSCs, SHED, MSCs, mesenchymal stromal cells, deciduous tooth, deciduous teeth, tooth exfoliation, inflamed pulp, in vivo differentiation, stem cell transplantation, MSC transplantation, cell transplantation, cell differentiation, regeneration, tissue engineering, tissue regeneration, bone tissue engineering, bone transplantation, tissue-engineered bone, bone regeneration, osteogenesis, osteoblast, osteoporosis, scaffold, tissue scaffolds, mandible.
The application of the inclusion and exclusion criteria for each article was conducted by two independent researchers (A.L.J. and C.C.G.P.) through the screening of titles and abstracts. Disagreements were resolved by discussion by a third reviewer (D.F.B.). Duplicate articles were excluded from the analysis. Furthermore, articles written in languages other than English, in vitro studies, review manuscripts, studies that evaluated the regeneration of tissues other than bone, studies that used only MSCs isolated from other human tissues, studies that used only non-human MSCs, and studies in which stem cells were not used were also identified and removed through the application of the exclusion criteria. In order to select the manuscripts that were included in this systematic review, an inclusion criteria were applied and only the manuscripts that described in vivo studies in which hDPSCs and SHED were used for bone tissue engineering purposes were elected for complete evaluation. After this, the selected articles were reviewed and classified according to the type of scaffold used, the in vivo experimental model chosen, the type of defect created, the method of evaluating bone regeneration, the time elapsed of evaluation after transplantation, and the results of bone tissue engineering obtained.
Results
The initial search resulted in 1576 articles. Among them, 128 articles were excluded because they were duplicates, 67 articles written in languages other than English, 408 in vitro studies, 213 review manuscripts, 114 studies that evaluated the regeneration of tissues other than bone, 201 studies that used only MSCs isolated from other human tissues, 329 studies that used only non-human MSCs, and 60 studies in which stem cells were not used were also removed from the analysis (Figure 1).

Flow diagram presenting the results of the literature search and the strategy used to select manuscripts that performed in vivo studies on the use of hDPSCs for bone tissue engineering.
After application of both exclusion and inclusion criteria, a total of 56 studies17–72 were selected and formed the basis of this systematic review. A list of the experimental model, type of scaffold, bone defect created, and the time and the methodology employed by the articles selected are presented in Table 1.
List of in vivo studies in which the potential of hDPSCs for bone tissue engineering was evaluated and the experimental model, type of scaffold, bone defect created, and the time and methodology employed by each of them.
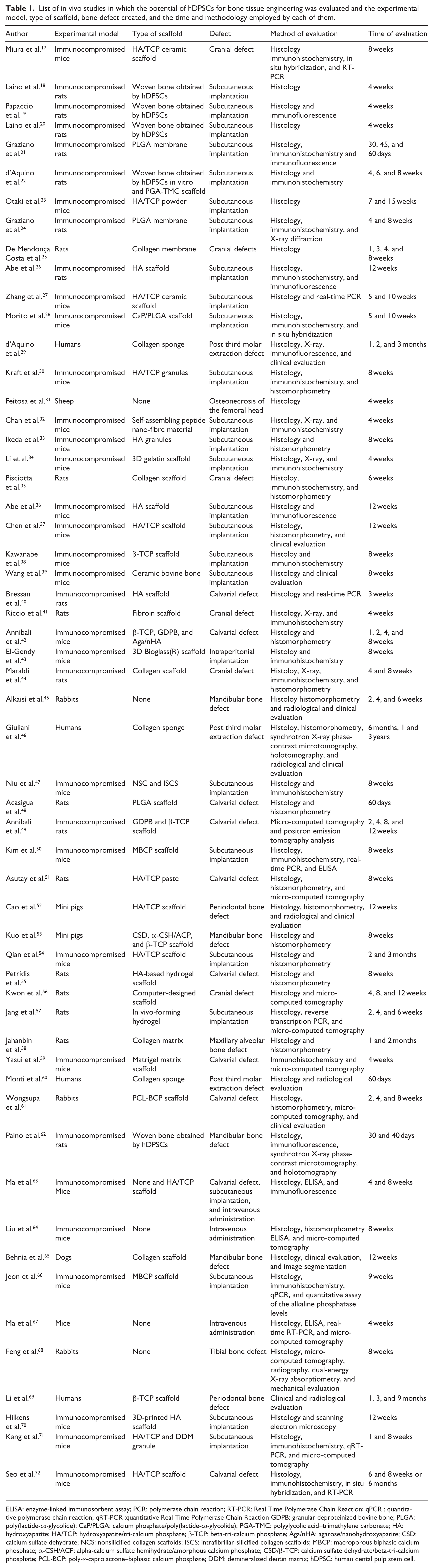
ELISA: enzyme-linked immunosorbent assay; PCR: polymerase chain reaction; RT-PCR: Real Time Polymerase Chain Reaction; qPCR : quantitative polymerase chain reaction; qRT-PCR :quantitative Real Time Polymerase Chain Reaction GDPB: granular deproteinized bovine bone; PLGA: poly(lactide-co-glycolide); CaP/PLGA: calcium phosphate/poly(lactide-co-glycolide); PGA-TMC: polyglycolic acid–trimethylene carbonate; HA: hydroxyapatite; HA/TCP: hydroxyapatite/tri-calcium phosphate; β-TCP: beta-tri-calcium phosphate; Aga/nHA: agarose/nanohydroxyapatite; CSD: calcium sulfate dehydrate; NCS: nonsilicified collagen scaffolds; ISCS: intrafibrillar-silicified collagen scaffolds; MBCP: macroporous biphasic calcium phosphate; α-CSH/ACP: alpha-calcium sulfate hemihydrate/amorphous calcium phosphate; CSD/β-TCP: calcium sulfate dehydrate/beta-tri-calcium phosphate; PCL-BCP: poly-ε-caprolactone–biphasic calcium phosphate; DDM: demineralized dentin matrix; hDPSC: human dental pulp stem cell.
In vivo model
Fifty-two17–28,30–45,47–59,61–68,70–72 out of 56 studies17–72 using hDPSCs and SHED for bone tissue engineering were performed on animal models and only four of these 56 selected manuscripts evaluated the potential of hDPSCs for bone tissue engineering in humans.29,46,60,69 Among the studies that used animal models, 20 manuscripts used rats,18–22,24–26,35,40,41,44,48,49,51,55–58,62 24 manuscripts used mice,17,23,27,28,30,32–34,36–39,42,43,47,50,54,59,63,64,66,67,70–72 3 manuscripts used rabbits,45,61,68 2 manuscripts used mini pigs,52,53 one manuscript used sheep, 31 and one manuscript used dogs. 65 The use of these different experimental models for bone tissue engineering in the articles reviewed is graphically represented in Figure 2.

Representative graph of the different experimental models employed to assess the bone tissue engineering potential of hDPSCs and SHED in the articles reviewed. It is important to note the high prevalence of studies in which the rat and mouse was chosen as the experimental model, in contrast with the low amount of studies in which an animal model with a greater similarity to human bone (as the pig, sheep, and dog model) was chosen. The prevalence of studies conducted in humans is also low among the articles reviewed.
The experimental designs
Among the 52 manuscripts that used animal models,17–28,30–45,47–59,61–68,70–72 the authors tested the ectopic bone formation using hDPSC in 27 studies,18–24,26–28,30,32–34,36–39,43,47,50,54,57,63,66,70,71 in 26 studies they created local bone defects to test the efficacy of the use of hDPSC and SHED for bone tissue engineering,17,25,29,31,35,40–42,44–46,48,49,51–53,55,56,58–62,63,65,68,69,72 and in three studies63,64,67 SHED were intravenously administered.
In order to assess ectopic bone formation, the authors implanted hDPSCs and SHED associated with scaffolds subcutaneously in 26 studies18–24,26–28,30,32–34,36–39,47,50,54,57,63,66,70,71 and in one manuscript, the authors implanted hDPSCs intraperitoneally associated with a scaffold. 43 All 27 manuscri-pts18–24,26–28,30,32–34,36–39,43,47,50,54,57,63,66,70,71 showed the ectopic bone formation when hDPSC or SHED were used for bone tissue engineering.
To study the local bone formation using hDPSCs and SHED, cranial defects were created in rats on 11 manuscri-pts,25,35,40,41,44,48,49,51,55,56 in mice on 4 manuscripts,17,42,59,72 and in only one manuscript they were made on rabbits. 61 Furthermore, 10 studies created maxillary and mandibular bone defects29,45,46,52,53,58,60,62,65,69 to assess the potential of hDPSCs for bone tissue engineering. In 3 out of these 10 studies, the researchers used the alveolar bone to test the tissue engineering strategies after extraction of third molars of maxillary 60 and mandibular29,46 regions in humans. In addition, one study transplanted hDPSCs to periodontal defect areas in patients undertaking periodontal treatment. 69 Six studies were conducted in different animal models. Among these studies, one used rats and created the bone defect in the anterior part of the maxilla, 58 one used rat and created the defect in the left side of mandible, 62 one used rabbits and created the defect between the first premolar and the mental foramen, 45 one used mini pigs to create the defects in the mesial region of the maxilla and mandibular first molars, 52 one used mini pigs and created the defect in front of the mandibular angle, 53 and one used dogs and created the defect on each side of the inferior mandibular border. 65 Furthermore, one study evaluated the potential of hDPSCs for bone tissue engineering in rabbits tibia submitted to distraction osteogenesis 68 and one study investigated the osteogenic potential of hDPSCs in an ovine model of induced osteonecrosis of femoral head. 31 Finally, the therapeutic potential of SHED intravenously administered for the treatment of osteoporosis was assessed in three studies conducted in a mice model of the disease.63,64,67 The use of different sites of hDPSCs and SHED transplantation for bone regeneration purposes in the articles reviewed is graphically represented in Figure 3.
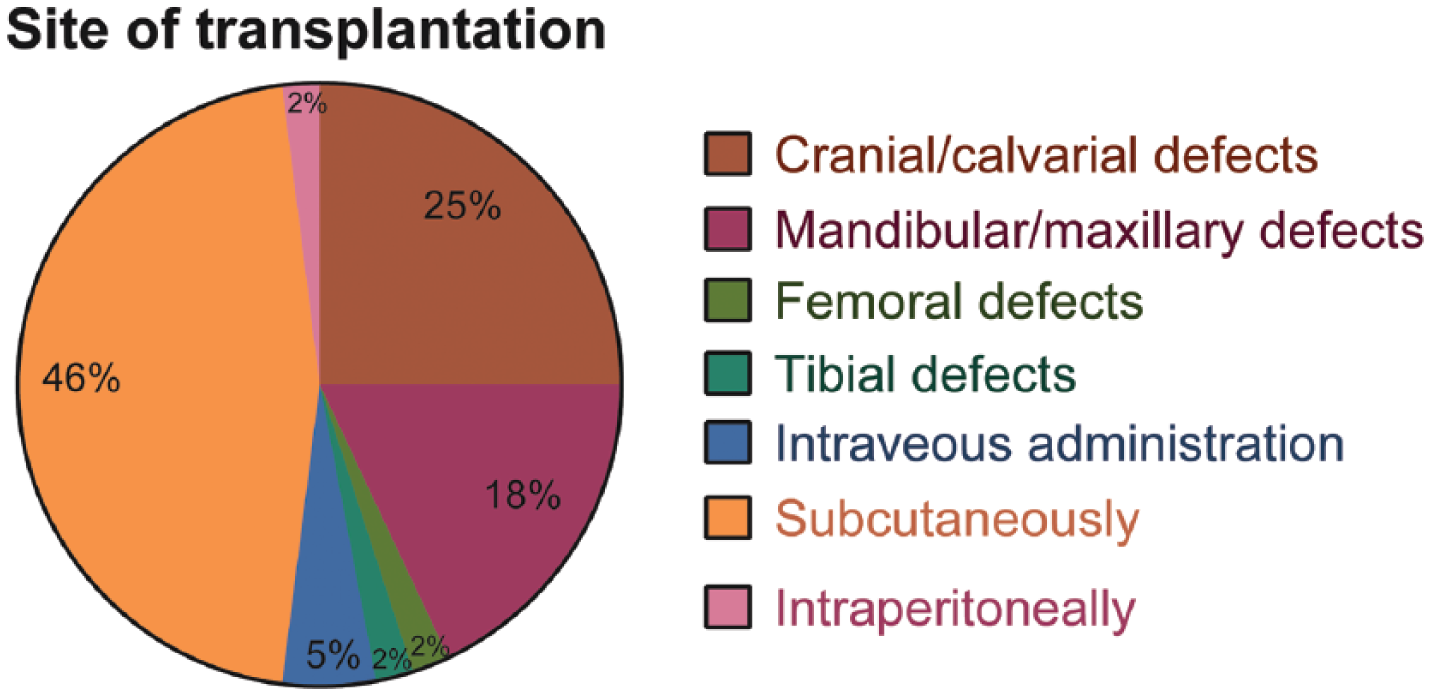
Representative graph of the different sites of transplantation used to assess the bone tissue engineering potential of hDPSCs and SHED in the articles reviewed. It is imperative to note the high prevalence of studies in which dental stem cells were subcutaneously and intraperitoneally transplanted to assess ectopic bone formation. The amount of studies in which dental stem cells were used to repair actual bone defects were only around half of the articles reviewed.
It is important to note that while most studies evaluated the potential of hDPSCs to produce ectopic bone when implanted subcutaneously or intraperitoneally,18–24,26–28,30,32–34,36–39,43,47,50,54,57,63,66,70,71 the majority of the recent in vivo studies published applied hDPSCs to repair local bone defects.17,25,29,31,35,40–42,44–46,48,49,51–53,55,56,58–62,63,65,68,69,72 In Figure 4, the prevalence of articles in which dental stem cells were employed to assess ectopic bone formation per year is graphically represented and summarizes the change observed in the literature.

The prevalence of studies in which the potential of hDPSCs and SHED to produce ectopic bone when implanted subcutaneously or intraperitoneally was evaluated per year. It is important to note that in the majority of the studies conducted recently, dental stem cells were used to repair actual bone defects, in contrast with the high prevalence of studies that employed dental stem cells to produce ectopic bone observed in previous years.
The scaffold
The scaffolds were used to seed the hDPSCs for bone tissue engineering in the bone defect sites. Different types of scaffolds were used in these studies that were summarized in this systematic review. The most common scaffolds used were collagen sponge or collagen membrane (observed in 8 studies),25,29,35,44,46,58,60,65 and hydroxyapatite/tri-calcium phosphate (HA/TCP) granules or HA/TCP ceramic (observed in 11 studies).17,23,27,30,37,51,52,54,63,71,72 Furthermore, six studies used scaffolds composed only by HA,26,33,36,40,55,70 five studies used scaffolds composed by beta-tri-calcium phosphate (β-TCP),38,42,49,53,69 three studies used PLGA membranes,21,24,48 two studies used granular deproteinized bovine bone (GDPB) scaffolds,42,49 and two studies used macroporous biphasic calcium phosphate (MBCP) scaffolds.50,66 The other types of scaffolds were used only once and are listed in Table 1.
In 11 manuscripts, scaffolds were not used to deliver hDPSC to the defect site18–20,22,31,45,62–64,67,68 for bone tissue engineering applications. Among them, five studies transplanted the woven bone produced by hDPSCs in rats18–20,22,62 (subcutaneously18–20,22 and to bone defects sites 62 ) and, in three studies, undifferentiated hDPSCs were directly injected to the defect site in sheep 31 and rabbits.45,68 Finally, in three studies, SHED were intravenously injected in mice for the treatment of osteoporosis.63,64,67 The use of these different types of scaffolds for bone tissue engineering purposes in the articles reviewed is graphically represented in Figure 5.

Representative graph of the different types of scaffolds employed in combination with hDPSCs or SHED in the articles reviewed. It is important to note that despite the fact that HA/TCP scaffolds were used by the majority of the articles reviewed, the number of papers in which collagen, HA, and β-TCP scaffolds were used is also significative. In 26% of the studies reviewed, however, other types of scaffolds were used for bone tissue engineering purposes, showing a great heterogeneity among the studies in this regard. In addition, a considerable amount of articles did not use a scaffold to deliver dental stem cells to the site of transplantation.
The method of evaluation
The most common methods used to evaluate the bone tissue engineering potential of hDPSCs were histology, immunohistochemistry, and histomorphometry. Histology was applied to obtain results regarding bone regeneration in 53 out of the 56 articles analyzed,17–48,50–58,60–68,70–72 while immunohistochemistry was used in 20 studies17,21,22,24,26,28,30,32,34,35,38,41,43,44,47,50,59,66,71,72 and histomorphometry was applied in 16 articles.30,35,37,42,44–46,48,51–55,58,61,64 Other methods included immunofluorescence (7 studies),19,21,26,29,36,62,63 micro-computed tomography (10 studies),49,51,56,57,59,61,65,68,69,71 real-time polymerase chain reaction (9 studies)17,27,40,50,57,66,67,71,72 and radiological (10 studies)29,32,34,41,45,46,52,60,68,69 and clinical (10 studies)29,37,39,45,46,52,61,65,69 evaluation. The other methods of evaluation that were used in the articles selected are shown in Table 1.
Outcomes
The results obtained and the methods employed by the articles reviewed were analyzed individually and divided according to the site of transplantation of dental stem cells for in vivo bone tissue engineering purposes. Table 2 summarizes the results obtained in the studies selected in this systematic review.
List of in vivo studies in which the potential of hDPSCs for bone tissue engineering was evaluated, the site of transplantation and the results obtained.

BMP-2: bone morphogenetic protein-2; vWF: von Willebrand factor; VEGF: vascular endothelial growth factor; TRAP: tartrate-resistant acid phosphatase; FABP-4: fatty acid–binding protein 4; PECAM-1: platelet endothelial cell adhesion molecule 1; HLA-1: human leukocyte antigen 1; Runx2: runt-related transcription factor 2; GFP: green fluorescent protein; HA: hydroxyapatite; HA-TCP: hydroxyapatite–tri-calcium phosphate; DPSC: dental pulp stem cell; hDPSC: human dental pulp stem cell; SHED: stem cells from human exfoliated deciduous teeth; MBCP: macroporous biphasic calcium phosphate; PCR: polymerase chain reaction; DDM: demineralized dentin matrix; PLGA: poly(lactide-co-glycolide); PCL-BCP: poly-ε-caprolactone–biphasic calcium phosphate; α-CSH: alpha-calcium sulfate hemihydrate; ACP: amorphous calcium phosphate; CSD: calcium sulfate dehydrate; β-TCP: beta-tri-calcium phosphate; ELISA: enzyme-linked immunosorbent assay.
Subcutaneous and intraperitonial implantation of hDPSCs
Among the 27 articles that assessed ectopic bone formation,18–24,26–28,30,32–34,36–39,43,47,50,54,57,63,66,70,71 no evidence of bone tissue formation could be found in only one study which used HA/TCP ceramic scaffolds to deliver hDPSCs to a mouse model. 27 Most common histological findings included the positivity for alizarin red staining22,43,47 and the observation of a lamellar bone formation with osteocytes entrapped within the lacunae and lamellae and osteoblasts on the bone surface.18–21,23,30,37,50,66 In addition, the expression of human leukocyte antigen 1 (HLA-1),19,21,24 collagen-I,21,32,38,43,72 bone alkaline phosphatase,21,22,24,30,50,66,72 bone sialoprotein,21,22,24,34,72 osteocalcin,21,22,24,28,32,34,36,38,43,47,66 osteonectin,21,22,24,32 osteopontin,32,34,50 platelet endothelial cell adhesion molecule 1 (PECAM-1),22,24 Runx2, 28 and von Willebrand factor22,24 in the newly formed bone were commonly observed by immunohistochemistry and immunofluorescence staining. Gene expression analysis by RT-PCR has also shown upregulation of the collagen-I, 50 bone sialoprotein,50,71,72 Runx2,27,50,66,67 osteocalcin,27,50,57,66,67,71,72 osteopontin,56,66,71 osteonectin,56,71 and alkaline phosphatase 67 mRNA levels. In most studies, the implants were retrieved at 4, 8, or 12 weeks after transplantation.
Cranial bone defect
The first study to use SHED for bone tissue engineering purposes was conducted by Miura et al. 17 This study was able to demonstrate that SHED, despite not been able to differentiate directly into osteoblasts, were able to induce recipient murine cells to differentiate into osteoblasts and osteocytes when transplanted to the brain of immunocompromised mice associated with HA/TCP scaffolds. 17 A more recent study conducted by Ma et al. 63 demonstrated that the transplantation of SHED associated with HA/TCP scaffold was able to regenerate the calvarial bone defects of mice. The tissue regenerated, however, contained a large amount of bone-like structures and bone-marrow-like components of human origin as demonstrated by the presence of human mitochondria-positive cells arranged on the mineralized matrix. 63 Other studies have shown that the transplantation of hDPSCs in combination with collagen and fibroin scaffolds resulted in significant bone regeneration after 4–8 months in rat cranial defects.25,35,41 The use of hDPSCs seeded on hydroxyapatite-based hydrogel scaffolds also resulted in superior healing compared to both untreated and scaffold-treated defects in rat calvarial bone defects, although complete healing could not be observed in any group of animals. 55 Furthermore, when hDPSCs were seeded on poly(lactide-co-glycolide) (PLGA) scaffolds, a greater bone neoformation was observed in the hDPSC-seeded scaffold group maintained 13 days in osteogenic medium before transplantation in rat calvarial bone defects. 48 In addition, the transplantation of both hDPSCs and SHED associated with HA/TCP scaffolds resulted in a greater regeneration of calvarial bone defects in rats 51 and mice 72 when compared to the control group (scaffold alone). The bone mineral density values in the group treated with hDPSCs associated with the HA/TCP scaffolds were also significantly higher than in the untreated control group. 51 A study conducted by Yasui et al. 59 demonstrated that LNGFRLow + THY-1High + hDPSCs associated with matrigel matrix scaffolds promoted greater central and peripheral would healing and new bone formation compared to the group transplanted with the scaffold alone when transplanted into immunocompromised mice to treat calvarial bone defects. 59 Transplantation of hDPSCs seeded on circular computer-designed Poly L-lactide-co-glycolide-co-epsilon-caprolactone (PLGC) scaffolds resulted in extensive bone-like ingrowths when compared to the control group in which computer-designed PLGC scaffolds were transplanted without hDPSCs. 56 Furthermore, no significant increases in the bone regeneration volumes were detected in the group treated with the scaffold alone. However, in the group treated with hDPSCs associated with the computer-designed PLGC scaffold, bone regeneration increased from 0% to 35%, 46%, and 53% at 4, 8, and 12 weeks, respectively. 56 Finally, a study by Wongsupa et al. 61 has shown that transplantation of hDPSCs seeded on poly-ε-caprolactone–biphasic calcium phosphate (PCL-BCP) scaffolds in combination with the modified melt stretching and multilayer deposition technique resulted in higher bone regeneration in the middle of the defects at 4 and 8 weeks when compared to the control group (scaffold alone) in a rabbit model of calvarial bone defects. However, bone regeneration in the group that received autogenous bone transplantation was superior, at all time points, to the groups of scaffolds seeded with hDPSCs and scaffold alone. When hDPSCs were transplanted in combination with GDPB, β-TCP, or Aga/nHA scaffold, however, little to no difference was observed between the group transplanted with the scaffold alone and the group treated with the scaffold seeded with hDPSCs. 42
Mandibular and maxillary bone defect
In a total of 10 studies, dental stem cells were transplanted for mandibular and maxillary bone defect reconstruction.29,45,46,52,53,58,60,62,65,69 In three of the four human studies selected for this systematic review, hDPSCs were used in combination with collagen scaffolds to repair bone defects created at the site of extracted maxillary and mandibular third molars.29,46,60 In one study, however, hDPSCs were transplanted in combination with a β-TCP scaffold to repair a periodontal bone defect in patients undertaking periodontal treatment. 69 In general, results from these studies demonstrated that a greater bone neoformation is achieved when hDPSCs are transplanted to the bone defect site associated with collagen or β-TCP scaffolds compared to control (scaffold alone).29,46,60,69
A study conducted by d’Aquino et al., 29 for instance, demonstrated that the sites that received the transplantation of hDPSCs seeded on collagen scaffolds presented a high rate of mineralization 1 month after transplantation. Furthermore, it was observed vertical bone regeneration in the site transplanted with hDPSCs seeded on collagen scaffolds but not in the site transplanted with the collagen scaffold alone at 2 months after transplantation. Three months after transplantation, it was confirmed that the bone defect in the site that received the combination of collagen scaffold and hDPSCs was completely regenerated and the cortical bone level was much higher in this site than in the site that was transplanted with the collagen scaffold alone. 29 An increase of clinical attachment was further observed in the site transplanted with hDPSCs seeded on collagen scaffolds compared to the site transplanted with the scaffold alone. Histological analysis also revealed that the tissue regenerated in the site that received the combination of hDPSCs and collagen scaffolds consisted of a well organized and well vascularized bone with a lamellar architecture surrounding the Haversian canals. In the site that received only the collagen scaffold, however, a more immature bone was formed, with fibrous bone entrapped among new lamellae, incomplete and large Haversian canals and evidence of bone reabsorption. Immunofluorescence analysis also revealed that the site that was transplanted with hDPSCs seeded on collagen scaffolds expressed higher levels of BMP-2 and VEGF when compared to the site transplanted with the scaffold alone. The results of the study conducted by d’Aquino et al. 29 were further investigated by Giuliani et al., 46 in a secondary report of the same experiment containing the results of a 3-year follow up. Results from this study demonstrated that the bone tissue regenerated in the sites that received hDPSCs seeded on collagen scaffolds was uniformly vascularized and compact. Furthermore, the bone tissue regenerated in these sites was larger in volume and had a better vertical bone height compared to the sites transplanted with the scaffold alone. In addition, a study conducted by Monti et al. 60 showed that 6 days after transplantation, the sites that were transplanted with hDPSCs seeded on collagen scaffolds presented stronger radio-opacity when compared to the sites transplanted with the scaffold alone. It was also observed a greater regeneration of a well-differentiated bone tissue with Haversian system formation in the sites that received the transplantation of hDPSCs associated with collagen scaffolds. Finally, a study conducted by Li et al. 69 demonstrated that the transplantation of hDPSCs associated with β-TCP scaffolds greatly improved the clinical symptoms of periodontitis on patients and exerted a repair effect on periodontal hard tissue defects caused by the condition.
The other six studies selected for this systematic review in which hDPSCs were used to repair maxillary and mandibular bone defects were conducted by Alkaisi et al., 45 Behnia et al., 65 Cao et al., 52 Kuo et al., 53 Jahanbin et al., 58 and Paino et al. 62 Alkaisi et al. 45 created a bone defect between the first premolar and the mental foramen in a rabbit model and investigated the potential for bone neoformation of SHED. No scaffold was used associated with SHED in this study. Radiological evaluation showed that at 2 weeks postoperatively, in the group that received the SHED transplantation, radiopacity had partially bridged the gap between the distracted bones and a greater bony union was observed at the center of the surgical area when compared to the groups treated with the scaffold alone. Furthermore, the tissue regenerated in the group that was transplanted with SHED has shown bony continuity with greater radiodensity when compared to the group treated with the scaffold alone, 4 weeks after transplantation. At 6 weeks postoperatively, greater radiodensity in the distraction gap and clear corticalization with a marrow cavity was observed in the group that received SHED transplantation. Histomorphometric findings also revealed that the total amount of bone regenerated in the groups that received SHED transplantation was significantly greater when compared to the groups treated with the scaffold alone across all measurement points and the percentage of remaining fibrous tissue was significantly lower in the group that received SHED transplantation. In a study conducted by Behnia et al., 65 dogs had bone defects created on each side of their inferior mandibular border. In this study, no difference could be noted between the site that received the transplantation of SHED associated with a collagen scaffold and the site that was only transplanted with the collagen scaffold alone. The bone tissue regenerated in both sites was compact in both lingual and floor parts of the defect, in the middle part of the defect a lamellar and woven bone with limited connective was produced, and in the lateral cortex of mandible the defect site was restored with connective tissue. 65 Cao et al. 52 created a bone defect in the mesial region of the maxilla and mandibular first molars in a miniature swine model in order to assess the bone tissue engineering potential of hDPSCs disassociated or seeded on HA-TCP scaffolds. Results from this study indicated that at 12 weeks postoperatively, the transplantation of hDPSCs disassociated or associated with HA-TCP scaffolds promoted the regeneration of a bone tissue higher and larger in volume when compared to the control group (scaffold alone). Kuo et al. 53 created bone defects in the front of the mandibular corner in a miniature swine model in order to evaluate the bone tissue engineering potential of hDPSCs seeded on various resorbable calcium sulfate/calcium phosphate scaffolds. This study has shown that at 8 weeks postoperatively, the sites treated with hDPSCs seeded on alpha-calcium sulfate hemihydrates (α-CSH)/ACP scaffolds presented less unhealed cavities when compared to the sites transplanted with hDPSCs seeded on calcium sulfate dehydrate (CSD) and CSD/β-TCP scaffolds. In contrast, some new bone but many unhealed cavities were observed in the empty control group. Furthermore, the ratio of new bone formation was significantly lower in the group treated with hDPSCs seeded on CSD/β-TCP scaffolds when compared to the sites treated with hDPSCs seeded on α-CSH/ACP and CSD scaffolds. Jahanbin et al. 58 created bone defects in the anterior part of the maxilla in a rat model to evaluate the potential for bone tissue regeneration of hDPSCs seeded on collagen scaffolds. This study demonstrated that maximum fetal bone neoformation was achieved in the group that received iliac bone graft 2 months after transplantation. However, there were no significant differences for bone neoformation between iliac bone graft and stem cell plus collagen scaffold groups at 1 or 2 months after transplantation. Finally, Paino et al. 62 created bone defects in the left mandible of rats in order to investigate whether a woven bone obtained by hDPSCs in vitro can be efficiently grafted to repair bone defects in a rat model. The results obtained demonstrated that woven bone, after transplantation, was remodeled to a bone tissue highly vascularized containing small clusters of mineralized bone. The bone tissue transplanted also integrated with the surrounding tissue, giving rise to a lamellar bone tissue with Haversian canals and osteocytes visible.
Intravenous administration
In three of the studies analyzed, SHED were intravenously administered for the treatment of osteoporosis in a mice model of the disease.63,64,67 In a study by Ma et al., 63 SHED, when intravenously administered, were able to increase the bone mineral density and to recover the trabecular bone structures in the long bones in a mice model of osteoporosis. Furthermore, a study conducted by Liu et al. 64 demonstrated that the systematic transplantation of SHED was able to increase the bone volume, the trabecular thickness, the trabecular number, the bone mineral density, the connectivity density, and the trabecular bone area and to decrease the trabecular space and structure model index in a mice model of ovariectomy-induced osteoporosis. SHED transplantation also resulted in an increase in the cortical bone parameters, including total cross-sectional area, cortical bone area, cortical bone fraction, and cortical thickness. Furthermore, histological analysis revealed that the trabecular bone volume in the SHED-treated group was markedly elevated compared with the control group. 64 Finally, Ma et al. 67 showed that the intravenous administration of SHED successfully recovered the bone mineral density and trabecular bone structures in a mice model of osteoporosis. The bone regenerated also expressed higher levels of the osteoblast-specific genes Runx2, alkaline phosphatase, and osteocalcin in the group transplanted with SHED when compared to the control group. Enzyme-linked immunosorbent assay (ELISA) results from the studies conducted by both Liu et al. 64 and Ma et al. 67 demonstrated that SHED systemic transplantation markedly reduced the serum concentration of the bone resorption markers receptor activator of nuclear factor kappa-B ligand (RANKL) and C-terminal telopeptides of type I collagen (CTX) and up-regulated the level of osteoprotegerin (OPG) compared with the control group. It is believed, however, that the reduction in bone loss observed after SHED intravenous transplantation is mainly due to their immunomodulatory properties.
Discussion
Currently, the gold standard for alveolar bone repair is to perform an autologous bone transplantation, in which the bone is removed from the patient and transplanted in order to fill the bone defect. 73 However, there are some problems related with this method that should be taken into consideration. For example, in cleft lip and palate patients, the amount of bone material removed from the donor site may not be enough to fill the alveolar cleft in case of wide fissures. 74 Furthermore, bone absorption, pain in the donor site area, infection and secretory disorders may also occur.75–77 Due to these complications, bone tissue bioengineering has been pointed out as a promising strategy for the reconstruction of critical orofacial defects, and the MSCs are currently being considered the main candidates for bone tissue engineering applications. 74 Bone marrow has been considered as one of the main sources of MSCs. However, the process of obtaining BMSCs requires a painful surgical incision. 4
Taking all these problems into consideration, several groups are trying to isolate of MSCs from more accessible sources and to use them in bone tissue engineering applications.8–10 One of the most promising source of MSCs for reconstruction of bone defects currently investigated is the dental pulp. 9 DPSCs can be easily isolated from deciduous and permanent teeth, expanded in vitro and used, in combination or not with a scaffold, for the repair of bone defects.14–16 The use of hDPSCs and SHED is particularly advantageous for bone reconstruction in cleft lip and palate patients. Due to the great benefits that the use of DPSCs can generate for the treatment of bone injuries and bone congenital malformations several in vitro studies have been conducted to investigate the potential use of dental pulp stem cells for bone tissue engineering applications.78–80 However, there is a limited number of clinical trials in humans in which the potential of hDPSCs and SHED for bone tissue engineering is evaluated. Furthermore, the methodologies applied for the evaluation of the potential of hDPSCs for bone regeneration vary considerably between distinct studies.
A variety of animal models were used in the studies analyzed in this systematic review, including mice,17,23,27,28,30,32–34,36–39,42,43,47,50,54,59,63,64,66,67,70–72 rats,18–22,24–26,35,40,41,44,48,49,51,55–58,62 rabbits,45,61,68 sheep 31 and mini pigs.52,53 Most studies evaluated in this systematic review were conducted in mice or rats. However, it is known that the swine and the ovine model represents the models with the highest similarity to human. 81 Future studies should put their focus on the use of animal models that have a greater similarity to human. In only four studies29,46,60,69 out of fifty-six analyzed,17–72 hDPSCs were used to treat bone defects in humans. It is imperative to conduct more human studies to reach a safer and more efficient use of hDPSCs for bone tissue engineering.
The type of defect created is also a factor of influence on bone regeneration. While the great majority of studies evaluated ectopic bone formation, an increasing number of studies are focusing on the use of hDPSCs to repair the site of bone defects in locus as evidenced in Figure 4. This change is extremely positive because the bone formation process occurs in a distinct manner when hDPSCs are implanted subcutaneously in comparison with the bone formation process in a bone defect site. As a consequence of the lack of all mechanical and chemical influences that the bone usually receives in an area of bone regeneration, subcutaneous implantation of hDPSCs hardly simulates clinical conditions. 82 Furthermore, in one of the studies analyzed in this systematic review, the process of ectopic bone formation completely failed. 27 Studies in which hDPSCs were transplanted to actual cranial, maxillary, and mandibular bone detects had better outcomes in general. However, in a study conducted by Annibali et al. 42 using a mice model in which calvarial bone defects were created, it was not possible to observe any difference in bone regeneration between the animals transplanted with the scaffold alone and the animals transplanted with the combination of the scaffold and hDPSCs. In addition, Behnia et al., 65 conducted a study in which dogs had bone defects created on each side of their inferior mandibular border. One side was transplanted with a combination of SHED and a collagen scaffold and the other side was transplanted with the collagen scaffold alone. No difference could be noted between the side that received the transplantation of SHED associated with a collagen scaffold and the side that was transplanted with the collagen scaffold alone and, as a result, the ability of SHED to contribute to the regeneration of mandibular bone defects in vivo in this dog experimental model could not be demonstrated. 65
Finally, the type of scaffold used to support the proliferation and differentiation of dental stem cells can also play a crucial role in the process of bone tissue regeneration. For instance, Zhang et al. 27 did not observe ectopic bone formation in vivo when hDPSCs were seeded on HA/TCP scaffolds. A study by Kuo et al., 53 however, was able to demonstrate that the use of α-CSH/ACP scaffolds in combination with hDPSCs promoted a more efficient bone regeneration when compared to hDPSCs seeded on CSD and CSD/β-TCP scaffolds. This study also demonstrated that the ratio of new bone formation was significantly lower in the group treated with hDPSCs seeded on CSD/β-TCP scaffolds when compared to the sites treated with hDPSCs seeded on α-CSH/ACP and CSD scaffolds. Furthermore, a study conducted by Acasigua et al. 48 has shown that a superior bone regeneration is reached when hDPSCs seeded on PLGA scaffolds are maintained in osteogenic induction medium for 13 days before transplantation. Finally, a study conducted by Kang et al. 71 demonstrated that both HA-TCP and demineralized dentin matrix (DDM) scaffolds had similar effects on the ability of hDPSCs to produce ectopic bone in a mice experimental model. hDPSCs, when used in combination with both scaffolds, showed great ectopic bone formation efficacy in vivo when compared with the control group (scaffold alone). 71 Three of the four human studies evaluated in this systematic review used collagen scaffolds as cell carries and reported successful bone formation for the repair of the bone defect produced after the process of extraction of third molars.29,46,60
Final considerations
Most of the studies analyzed in this systematic review reported positive results when they used hDPSC for bone tissue engineering. While most studies evaluated the potential of hDPSCs to produce ectopic bone when transplanted subcutaneously other evaluated their bone tissue engineering potential in actual bone defects using, in most cases, rats and mice as animal models. This emphasizes, therefore, the importance of a change of attitude regarding the use of hDPSCs to repair actual bone defects in an animal model with a greater similarity to human.
Footnotes
Acknowledgements
Supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) and Programa de Desenvolvimento Institucional do Sistema Único de Saúde (PROADI – SUS). To Instituto de Ensino e Pesquisa - Hospital Sírio Libanês, for provide us all support to develop stem cells and tissue engineering researches.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.