
Abstract
Visual illusions serve as a window into the altered perceptual experiences of individuals with psychiatric disorders. One such is the induced Roelofs effect, where the perceived position of a small stimulus is shifted toward the midline of a distractor frame surrounding the stimulus, as the shift is more pronounced in individuals with schizophrenia. The present work extends the induced Roelofs effect assessment to bipolar disorder. Healthy controls, patients with bipolar disorder, and patients with schizophrenia were shown a dot stimulus placed inside a frame whose horizontal position could vary, and they were asked to determine whether the dot position was to their left or to their right. The induced Roelofs effect was minimal in healthy controls, large in schizophrenia, and intermediate in bipolar disorder. No association between the effect size and psychotic symptomatology or cognitive abilities was found. Yet, a nonlinear, concave association was found between the total pharmacological load and the illusion size. The results suggest that the illusion is related to alterations in sensory processing, which are common to both bipolar disorder and schizophrenia, hence showing their potential utility in clinical evaluations, which currently tend to overlook the sensory domain.
Keywords
How to Cite this Article
Esposito, D., Bertolasi, J., Escelsior, A., Amadeo, M. B., Inuggi, A., Perucco, M., Alvano, A., Marcenaro, M., Zizzi, A., Pereira Da Silva, B., Serafini, G., Amore, M., & Gori M. (2026). Differentiating bipolar disorder from schizophrenia: The role of the induced Roelofs illusion. i-Perception, 17(2), 1–22. https://doi.org/10.1177/20416695251394612
Introduction
Sensory perception plays a crucial role in shaping our understanding of the world around us. Our senses continually provide information that the brain processes to create a rich and dynamic perceptual experience. Pivotally, the perceptual experience the brain generates is not a hard copy of the physical stimuli eliciting the nervous system in each moment, but rather an interpretation influenced by assumptions, expectations, prior experiences, and structural peculiarities of the sensory hardware. This can lead to percepts that diverge from physical reality. Among the most common expressions of such phenomenon are perceptual illusions. Far from being just captivating demonstrations of the brain's susceptibility to misinterpretation, their scientific relevance in the study of the brain is undeniable as the susceptibility to illusions can reveal the mechanisms by which the brain constructs and interprets sensory information (Axelrod et al., 2017; Schwarzkopf et al., 2011).
In psychiatry, where endogenous perceptual aberrations such as hallucinations and delusions are distinctive phenomena (Butler et al., 2008), there has been growing interest in the study of exogenous perceptual aberrations like visual illusions (Notredame et al., 2014; Silverstein & Keane, 2011). The condition whose susceptivity to perceptual illusions has been investigated the most is schizophrenia (SZ), with several literature reviews on the topic published in the last 20 years (see Costa et al., 2023; King et al., 2017; Notredame et al., 2014, for some examples). As these reviews show, despite several contradictory findings (especially concerning the Ebbinghaus and the Ponzo illusions), patients with SZ seem overall less susceptible to surround-contrast illusions and depth-inversion illusions, whereas they seem more susceptible to the Müller-Lyer illusion.
One point that has been raised is whether the different susceptivity to visual illusions is a marker of SZ per se, an endophenotypic marker of psychoses (Notredame et al., 2014), or else a marker of psychotic or psychotic-like symptomatologies (Sperandio et al., 2023). Recognizing the specificity of such illusions could greatly benefit the diagnosis formulation, as many patients exhibit a combination of symptoms that can be associated with more than one pathology. This is the case of SZ and bipolar disorder (BD; Lake, 2010; Möller, 2003; Pearlson, 2015). The two disorders’ symptomatology overlap is such that they can be seen as portions of a psychosis continuum (Maier et al., 2006; Möller, 2003) where SZ lies at one extreme and BD lies in an intermediate stage. Concerning the sensitivity to perceptual illusions in BD, the current literature on the topic is limited and (again) conflictual. For example, Yang et al. (2013a) compared the sensitivity of healthy participants, patients with BD, and patients with SZ to illusions based on visual context in terms of brightness, size, contrast, orientation, and motion. They found weaker contextual contrast illusion in participants with SZ than in healthy controls (HCs), while no clear group-related differences between controls and patients with BD emerged in any domain assessed; yet, they found that patients with BD with worse manic symptoms were more likely to have a weaker contrast illusion, and that motion and orientation illusions correlated with the severity of psychotic symptoms irrespective of pathology. Schallmo et al. (2015) found instead an intermediate sensitivity to the context-induced contrast illusion that did not extend to their unaffected biological relatives. Despite their differences, these studies suggest that the reduced sensitivity to context-induced contrast illusion may reflect specific symptom dimensions shared among the two populations, even though with different degrees of severity. This hypothesis is supported by studies on nonpsychotic populations showing that the presence of psychotic-like symptoms is associated with an alteration in the susceptivity to visual illusions, especially those involving perceptual context (Sperandio et al., 2023).
It is important to notice that the current literature on visual illusions in psychosis used mostly contextual conflicts such as central versus peripheral visual field, for example, Ponzo, Ebbinghaus, or surround contrast illusions (Costa et al., 2023; King et al., 2017; Notredame et al., 2014; Yang et al., 2013b), or involving world-related expectations, for example, depth-inversion illusions (Costa et al., 2023; Keane et al., 2016). However, as one of the core symptoms of psychoses is the disruption of the sense of self (Nelson et al., 2014), investigating illusions which involve such sense, even in its minimal, sensorimotor aspects (Blanke, 2012; Salomon, 2017), may reveal different susceptibilities related to its degree of disturbance. One such illusion is the induced Roelofs effect (Bridgeman et al., 1997; Roelofs, 1959). In this illusion, observers tend to mislocalize the position of a target object with respect to their visual midline when the target is displayed within an off-centered rectangular frame. In a series of studies (Bridgeman et al., 2018; Dassonville et al., 2004; Dassonville & Bala, 2004), Dassonville and colleagues investigated the mechanisms underlying the illusion, and they found strong evidence suggesting that the frame acts upon the mental construct of the visual midline, which can be intended as an aspect of the minimal self, or sensorimotor self (Blanke, 2012; Salomon, 2017; Sherick et al., 1976). Chen et al. (2011) investigated the susceptibility to the induced Roelofs effect in patients with SZ in both purely visual judgments and in immediate and delayed visuomotor tasks (reaching-to-touch), finding a larger effect compared to HCs in all the tasks. They interpreted the result in terms of hyperresponsiveness to sensory information and stronger influence of instantaneous evidence over the sensory self.
Recognizing the induced Roelofs effect as an illusion that involves the perception of the self, a core aspect of psychoses, we hypothesized that the illusion could be weaker in patients with less pronounced or absent disturbance in the sense of self, such as those with BD. Specifically, in light of the abovementioned hypothesis of psychosis continuum placing BD at an intermediate psychotic severity compared to SZ (Maier et al., 2006; Möller, 2003), we hypothesized that patients with BD would experience the induced Roelofs illusion more prominently than HCs but less than patients with SZ. Additionally, we investigated whether the interindividual differences in induced Roelofs effect size were associated with other clinical and cognitive abilities regardless of the diagnosed pathology. Finally, we checked the effect of pharmacological load on the sensitivity to the illusion. Investigating the susceptibility of patients with SZ and BD to the perceptual illusion, along with correlations with pharmacological treatment, psychotic symptomatology, and cognitive skills, may offer insights into the root cause of the disease and provide useful information to better discern between conditions whose distinction is hard in clinical practice.
Materials and Methods
Participants
The study enrolled 21 patients diagnosed with BD and nine participants diagnosed with SZ, along with 15 HCs (refer to Table 1 for summary of demographic and clinical data). The sample size was based on the amount of suitable and available participants in a timeframe of 3 years. Given the low number of participants with SZ, we conducted a sensitivity power analysis (Lakens, 2022) with software G*Power (Faul et al., 2007) to estimate the minimum significant effect size we could aim for, and we compared the obtained estimate with the effect reported by Chen et al. (2011), which was a Cohen's f2 = .66. For a repeated-measures analysis of variance with nine participants, two repeated measures, correlation between repeated measures fixed at .5 (G*Power's default), significance level at .05, and expected power at 0.8, we estimated a minimum Cohen's f2 = .53, suggesting that nine participants with SZ are enough to find an effect as large as the one reported in Chen et al. (2011).
Demographic and clinical characteristics of participants.
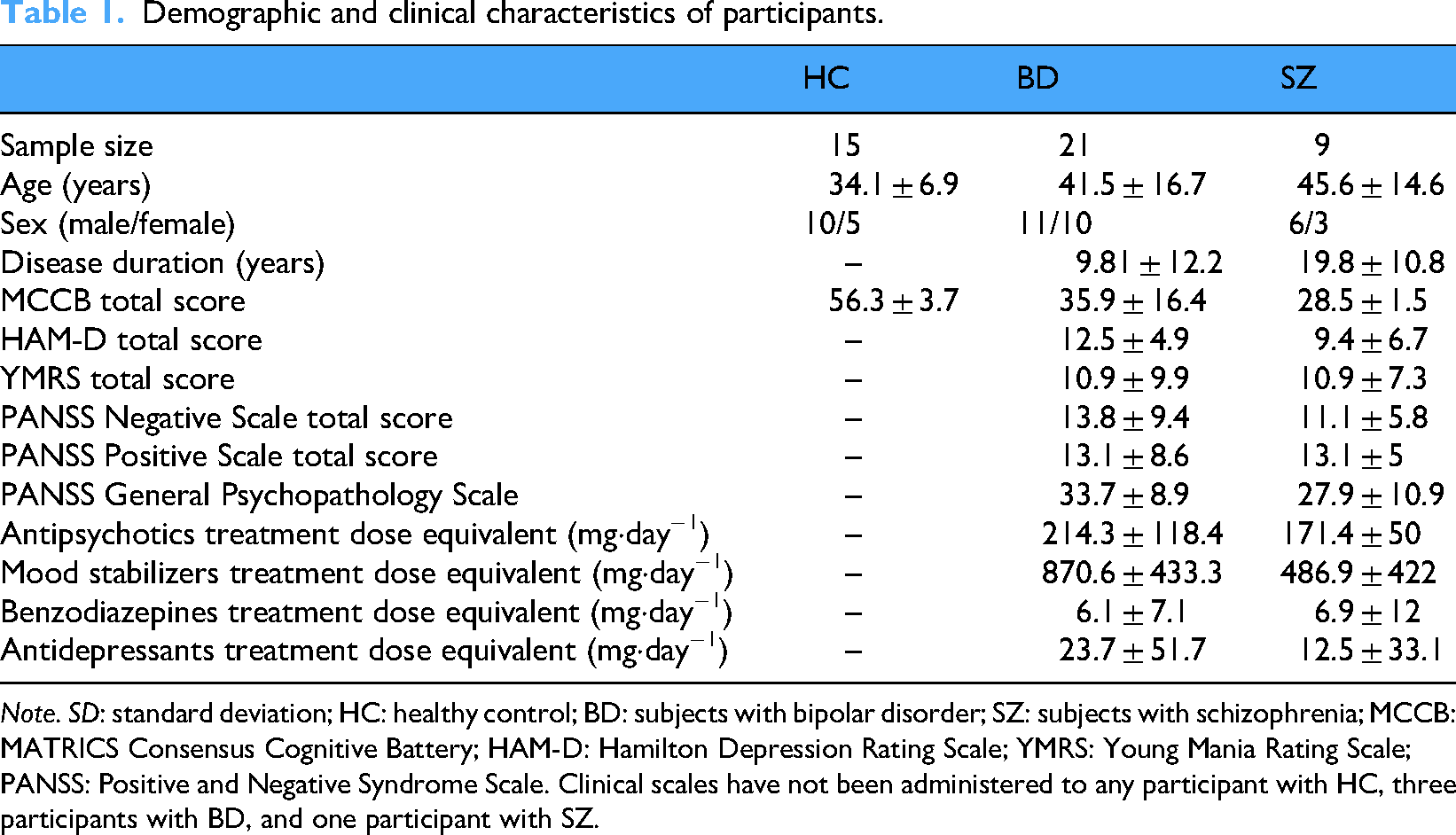
Note. SD: standard deviation; HC: healthy control; BD: subjects with bipolar disorder; SZ: subjects with schizophrenia; MCCB: MATRICS Consensus Cognitive Battery; HAM-D: Hamilton Depression Rating Scale; YMRS: Young Mania Rating Scale; PANSS: Positive and Negative Syndrome Scale. Clinical scales have not been administered to any participant with HC, three participants with BD, and one participant with SZ.
All patients enrolled were hospitalized at the Psychiatric Unit of San Martino Hospital in Genoa, and received a diagnosis of SZ or BD according to the Diagnostic and Statistical Manual of Mental Disorders 5-TR criteria (American Psychiatric Association, 2022), while HCs were drawn from local contacts, and had no personal or family history of psychiatric, neurological, or cognitive disorders. All participants were Italian native speakers. Participants were administered a battery of psychopathological scales to assess their symptomatology at the moment of testing and a neuropsychological battery to assess their cognitive performance. The psychopathological assessment used the following scales: Hamilton Depression Rating Scale (HAM-D; Hamilton, 1960); Young Mania Rating Scale (YMRS; Young et al., 1978); and Positive and Negative Syndrome Scale (PANSS; Kay et al., 1987). The neuropsychological assessment used the MATRICS Consensus Cognitive Battery (MCCB; Kern et al., 2008; Nuechterlein et al., 2008). All the assessment tools listed above were administered by a professional evaluator. The research protocol was approved by the local ethics committee (Comitato Etico Regionale ASL3 Liguria) and conducted in line with the Declaration of Helsinki, and all subjects gave written informed consent. The study was performed following the relevant ethical guidelines and regulations.
Psychopathological and Neuropsychological Assessments
Psychopathological Assessment
To explore symptomatology of patients at the moment of testing, clinicians administered different psychopathological scales: HAM-D (Hamilton, 1960), YMRS (Young et al., 1978), and PANSS (Kay et al., 1987). The HAM-D is a clinician-administered assessment tool widely used to measure the severity of depressive symptoms. It consists of 21 items covering a range of symptoms such as mood, guilt, sleep disturbances, and suicidal thoughts. Clinicians rate each item on a scale of 0 to 4 or 0 to 2 based on the patient's reported experiences during the evaluation. Higher scores reflect more severe depressive symptoms. The HAM-D scale showed acceptable internal consistency in a sample of 278 patients with SZ (Cronbach's alpha between .72 and .79) (Schennach et al., 2012). The YMRS is a diagnostic scale designed to evaluate the severity of manic symptoms. It consists of 11 items that assess various aspects of mania, including elevated mood, increased energy, irritability, and disruptive behavior. Each item is scored on a scale ranging from 0 to 4 or 0 to 8, with higher scores indicating more severe manic symptoms. The YMRS scale demonstrated acceptable internal consistency (Cronbach's alpha = .72) (Mohammadi et al., 2018). The PANSS is a standardized assessment tool typically used in psychiatry to evaluate the severity of symptoms in individuals with SZ. It comprises 30 items that assess various aspects of psychotic disorders. These items are divided into three subscales: positive subscale (including positive symptoms such as hallucinations and delusions), negative subscale (including negative symptoms such as blunted affect and social withdrawal), and general psychopathology (including anxiety, depression, and disorientation). Each item is rated on a scale from 1 to 7, with higher scores indicating more severe symptomatology. The PANSS scale showed acceptable internal consistency in a sample of 500 patients with SZ (Cronbach's alpha between .70 and .85) (Van Den Oord et al., 2006).
Neuropsychological Assessment
To assess cognitive functioning in patients, clinicians utilized the MCCB (Kern et al., 2008; Nuechterlein et al., 2008). The MCCB is a standardized tool designed to evaluate key cognitive domains relevant to SZ and related disorders. It comprises 10 subtests that measure seven cognitive domains: speed of processing, attention/vigilance, working memory, verbal learning, visual learning, reasoning and problem-solving, and social cognition. Each subtest is scored individually, and the results are standardized to T scores, with a mean of 50 and a standard deviation (SD) of 10. These scores are then combined to provide an overall composite score reflecting global cognitive functioning. The MCCB has demonstrated good internal consistency for one-factor model in a sample of 183 community-dwelling outpatients diagnosed with SZ or schizoaffective disorder (Cronbach's alpha = .76) (Burton et al., 2013). The MCCB is widely used in both clinical and research settings to assess cognitive deficits and track changes over time in individuals with SZ.
Stimuli and Setting
The experimental sessions were conducted in a dimly lit room. The apparatus consisted of a 60 Hz, 19″ HP monitor (model L1940T, aspect ratio 5:4, dimensions 29.4 cm × 29.4 cm, resolution 1280 × 1024 pixels) to deliver the visual stimuli, a keyboard to collect the participant responses, and a chinrest, placed at 57 cm from the monitor and aligned it to keep the participants’ head midline aligned with the monitor midline (Figure 1). The target stimulus consisted of a black spot with a diameter of 0.15°, placed within a black frame measuring 20° horizontally and 10° vertically. Visual stimuli were generated and controlled by MATLAB (The MathWorks Inc., 2022) with the Psychophysics toolbox (Brainard, 1997; Kleiner et al., 2007; Pelli, 1997).

Experimental setting. Participants were seated in a dimly lit room, with the head position controlled by the chinrest and at 57 cm from the screen.
Design
The experimental session consisted of two blocks: a preliminary assessment of the participants’ left–right discrimination abilities and the actual induced Roelofs effect assessment. In both blocks, the trial structure was the following: participants were shown the stimulus for 1 s, then they were required to discriminate the position of the dot with respect to their perceived head midline using a two-alternatives-forced-choice response pattern (left or right), regardless of the frame position. Participants could answer only after the stimulus offset. No feedback regarding response accuracy was provided. The next trial started after the current trial's response collection. Successive trials were temporally separated by an intertrial interval sampled randomly in the range [1, 1.5] s. The two blocks differed only in the number of trials and in the positioning of the dot and frame. The specificities of the two blocks are described in the following subsections.
Preliminary Left–Right Discrimination Abilities Assessment
For the preliminary assessment, the frame appeared always in the center of the screen, that is, 0° from the monitor midline, and the dot position was determined adaptively by a QUEST routine on a trial-by-trial basis. QUEST is an adaptive algorithm that uses a Bayesian approach to set the dot position using all the information available from previous trials (Watson & Pelli, 1983). The dot position ranged from −2° to 2° (positive numbers on the right). The preliminary assessment consisted of 40 trials, lasting approximately 2 min, breaks excluded. Following standard psychophysical procedures, the just noticeable difference (JND) was used as an index of discrimination ability. The JND was computed as the SD of the Gaussian cumulative distribution fitted on the proportion of “right” responses with respect to the dot position.
Induced Roelofs Effect Assessment
For the actual assessment, the frame could appear with a shift of −3.2°, −1.6°, 0°, +1.6°, or +3.2° relative to the monitor midline (positive number ipsilateral to the dot shift), and the dot could appear in two positions only on the left or on the right of the monitor midline. Refer to Figure 2 for a visual representation of the stimuli used. The dot distance from the monitor midline corresponded to the participant's JND, so as to expect that the participant would give around 65%–70% correct answers when the frame was in the center (.68 is the probability that a value drawn from a cumulative normal distribution centered at 0 is smaller than the normal distribution's upper SD). Each combination of dot and frame shift (five frame shifts by two dot shifts) was presented 20 times, for a total of 200 trials. The stimulus for each trial was selected according to the method of constant stimuli. The induced Roelofs effect assessment lasted approximately 13 min, with breaks excluded.

Set of stimuli used in the study. As the induced Roelofs effect emerges as the influence of the frame displacement on the dot displacement judgment, regardless of the direction, the study considered only the relative shift of the frame with respect to the dot and ignored the absolute shift direction.
Procedure
The participants were first introduced to the task verbally. They received the following instructions: (translation from Italian) You will see two shapes appear on the screen, a dot and a frame. These may appear shifted a little to the right or a little to the left in an unrelated manner. Your task is to judge the position of the dot with respect to yourself while ignoring the frame. You will have to judge whether the dot appears to your right or left, therefore to the right or left of your nose. Concentrate solely on the dot and ignore the frame. To answer LEFT, press the left arrow key on the keyboard; to answer RIGHT, press the right arrow key on the keyboard. For example, if the dot is on your left, press the LEFT arrow key; If the dot is on your RIGHT, press the RIGHT arrow key. Wait for the shapes to disappear before responding, and once the shapes have disappeared, try to respond as quickly as possible.
During the whole experimental session, the experimenter sat close to the participants, yet out of sight, to control their posture and be ready to provide support as needed. If the participant had difficulty in pressing the arrow keys for answering, the participant was asked to respond verbally, and the experimenter keyed the responses into the computer manually. The whole experimental session lasted about 15–20 min, breaks included.
Data Analysis
The data analysis aimed to test the difference in induced Roelofs effect size among HCs, individuals with BD, and individuals with SZ. Further exploratory analyses investigated the specific association between the induced Roelofs effect sizes and cognitive functions, clinical scales, or pharmacological load. All the analyses were performed using R Statistical software (v4.3.1; R Core Team, 2021).
Induced Roelofs Effect Size Assessment
The link between induced Roelofs effect size and diagnosis was quantified as the variation in the proportion of correct responses as a function of the frame shift relative to the dot. To do so, the analysis used generalized linear mixed effects model (GLMM) fitting (Breslow & Clayton, 1993; Jiang, 2007; Stroup, 2012). The fitted models were binomial GLMM with logit link function, corresponding to multiple logistic regression (Menard, 2002). The models’ outcome variable was the proportion of correct responses. A first baseline model fitted the frame shift (“frame” factor) on each individual was used to perform outlier detection. The baseline model was, in Wilkinson’s (1959) notation,
The outliers were identified as the data points whose Pearson residuals from the model fit were larger than 2. Those data points were excluded from the full model fitting procedure.
The full model's predictor variables were the frame shift (“frame”), the experimental group (“diagnosis”), the participant's age (“age”), and their JND estimated from the preliminary assessment (“JND”). The factor “diagnosis” was encoded using orthogonal polynomial contrasts, which treated the three levels of the factor “diagnosis” as equally spaced and orthogonal values of two continuous variables encoding a linear and a quadratic trend (Freedman, 2009), ordered in the increasing order of psychotic symptoms severity. This encoding was chosen to test the “psychosis continuum hypothesis” (Möller, 2003). Therefore, the model searched for the presence of linear (“diagnosis.L”) and/or quadratic (“diagnosis.Q”) trends between diagnosis and response variables. The factors “JND” and “age” were z-standardized prior to model fitting to avoid convergence issues. The fitted model was, in Wilkinson’s (1959) notation,
Association With MCCB Subscales
The association between induced Roelofs effect size and cognitive functions was investigated by correlating the induced Roelofs effect sizes estimated individually with the scores obtained from the subscales of the MCCB. The subscales are: processing speed, attention, working memory, verbal learning, visual learning, and social cognition. The Shapiro–Wilk test was used to assess the MCCB subscale scores distributions’ normality. From our analysis, three out of nine subscale distributions were significantly non-Gaussian. Therefore, the association between the induced Roelofs effect size and the MCCB scores was assessed using Kendall's tau-b, a nonparametric estimate that is typically preferred to Spearman's correlation when the data set under investigation includes ties (Kendall, 1938). The correlation was assessed on all groups together, in line with the psychosis continuum hypothesis (Möller, 2003). In such a framework, one would expect to find the values from control participants closer to one side of the data distribution, those from participants diagnosed with SZ closer to the other side, and those from participants diagnosed with BD in between.
In addition to the correlation analysis, the induced Roelofs effect size and the MCCB data sets underwent a simple supervised classification routine to investigate if the induced Roelofs effect size assessment can provide clinicians with useful information to support the diagnosis formulation. A naïve Bayes classifier (Devroye et al., 1996) was trained on the MCCB subscales alone first and then on the MCCB subscales together with the induced Roelofs effect size estimates, using the participants’ diagnoses as target classes. The naïve Bayes classifier uses the Bayes formula to obtain the probability that the participant under investigation has a given diagnosis conditional to the scores of that participant in the features set of interest. According to Bayes’ theorem (Bayes, 1763), the conditional probability of the data belonging to a certain class given a set of features, 
Association With the PANSS Scores
The association between induced Roelofs effect size and the severity of psychotic symptoms was investigated by correlating the induced Roelofs effect sizes estimated individually with the PANSS total score and PANSS subscales scores (PANSS-P, PANSS-N, PANSS-G). The correlation analysis followed the same procedure used for assessing the correlation between induced Roelofs effect size and MCCB scores. The correlation was assessed on all the patients regardless of their diagnosis. The Shapiro–Wilk test was significant for all variables. Therefore, the association between the induced Roelofs effect size and the PANSS scales was assessed using Kendall's tau-b.
Association With Pharmacological Load
The association between the induced Roelofs effect and the pharmacological load was investigated using Conway-Maxwell (COM)–Poisson regression, which assumes the response variable comes from a COM–Poisson distribution (Conway & Maxwell, 1962). The COM–Poisson distribution is a generalization of the Poisson distribution that can model count data that is both underdispersed (positive mean-variance ratio, ν > 1) and overdispersed (negative mean-variance ratio, ν < 1). The COM–Poisson distribution makes this possible by adding to the Poisson probability mass function
Results
Induced Roelofs Effect Size in SZ and BD
The study quantified the association between induced Roelofs effect size and the psychiatric disorders under investigation by fitting a binomial GLMM with logit link function, corresponding to logistic regression, on the proportion of correct responses in the left–right discrimination task. We anticipate here that the model found an increase in the induced Roelofs effect size stepping from HC to BD to SZ (Figure 3). Table 2 reports the model's fixed-effects estimates and their significance. The coefficient values are on the log-odds scale. The model's total explanatory power is substantial (conditional R2 = .726), and the part related to the fixed effects alone (marginal R2) is .546. The model's intercept, that is, the average log-odds of correct responses, is 0.589 (95% CI [0.472, 0.705], p < .001), corresponding to a probability of correct response of 0.643 (95% CI [0.616, 0.669]), in line with the probability of correct response one would expect when the stimulus administered is around the participant's JND. The coefficients “diagnosis.L” (0.059, 95% CI [−0.169, 0.287], p = .612) and “diagnosis.Q” (0.060, 95% CI [−0.128, 0.247], p = .533) were not significant. Together with the intercept estimate, these results confirmed that the personalized dot shift based on the preliminary assessment of the participants’ abilities standardized the task's perceptual difficulty successfully in all groups. The “frame” coefficient was significant (1.021, 95% CI [0.801, 1.240], p < .001), showing that the paradigm on average could induce the induced Roelofs effect. Concerning the interaction effect of the diagnosis on the induced Roelofs effect size, the coefficient “frame:diagnosis.L” was significant (1.044, 95% CI [0.612, 1.476], p < .001), while the coefficient “frame:diagnosis.Q” was not significant (−0.0387, 95% CI [−0.392, 0.314], p = .830), meaning that the effect size in the bipolar group lied between that of the control group and that of the schizophrenic group (Figure 3).

(A) Scatter plot of the raw proportion of correct responses per degree of frame shift, and the corresponding binomial GLMM fit. A negative value corresponds to a frame shift to the same side of the dot, a positive value corresponds to a frame shift opposite to the dot side. (B) Scatter plot and box plot of the individual induced Roelofs effect size estimates. GLMM = generalized linear mixed effects model.
Estimates of the fixed-effect coefficients from the binomial GLMM used to assess the relationship between the induced Roelofs effect size and psychosis severity.

Note. Each coefficient corresponds to the variation of log-odds ratio related to the given factor value. “Diagnosis.L” = the presence of a linear trend in the psychosis severity; “Diagnosis.Q” = a quadratic one; SE = standard error of the coefficient estimate; z = Wald z statistic; GLMM = generalized linear mixed effects model; JND = just noticeable difference.
The asterisks indicate the significance level: *p < .05, **p < .01, ***p < .001.
Induced Roelofs Effect Size and MCCB
The study assessed the relationship between individual induced Roelofs effect sizes and scores obtained in the subscales of the MCCB using two methods: Kendall's tau-b correlation coefficient estimation, and performance comparison of naïve Bayes classifiers using MCCB with and without the induced Roelofs effect size as input feature.
Kendall's tau-b coefficient did not reach significance for any of the MCCB subscales, τelaboration speed = −.16, p = .241, τattention = −.10, p = .524, τworking memory = −.10, p = .464, τverbal learning = −.18, p = .172, τvisual learning = −.26, p = .063, τproblem solving = −.02, p = .905, τsocial cognition = −.12, p = .413, τtotal = −.12, p = .466, N = 28 (Figure 4), that is, it failed to identify an association between the induced Roelofs effect size and any of the MCCB subscales.

(A) Scatter plot of MATRICS subscales and total scores versus induced Roelofs effect size. (B) Correlogram results. Negative correlation between Roelofs coefficients and MATRICS subscales and total scores. All the MCCB scores reveal nonsignificant correlations with Roelofs effect (marked with an X).
The LOOCV on the naïve Bayes classifiers based on the MCCB scores returned acc = 0.643 and k = 0.429. The LOOCV of the model including also the induced Roelofs effect size returned acc = 0.821 and k = 0.718. This means that the classification based on MCCB alone performed worse than the classification based on MCCB and induced Roelofs effect size together. Additionally, the classifiers’ confusion matrices inspection (Table 3) shows that the classifier based on MCCB alone performed well in discerning between control and patients but not between diagnoses, and that the induced Roelofs effect size contributed to the classification performance by improving the patients diagnosis discrimination.
Confusion matrices for the naïve Bayes classifiers with and without induced Roelofs effect size as a feature.

Note. Each column in the matrices represents the predicted values, while each row represents the actual values. As can be observed, using the induced Roelofs effect estimates, the classification of subjects with BD and SZ improves. In fact, if we only consider the contribution of the MCCB, nine subjects are classified as “Bipolar” and five are mistakenly classified as “Schizophrenic.” With the contribution of the induced Roelofs effect, only two subjects are mistakenly classified as belonging to the “Schizophrenic” category, while 11 are correctly classified as “Bipolar.” In the case of the classification of patients with SZ, we see how the contribution of the induced Roelofs effect increases the accuracy of the classification from two to five subjects. BD = bipolar disorder; SZ = schizophrenia.
Induced Roelofs Effect Size and PANSS Scores
The study assessed the relationship between individual induced Roelofs effect sizes and the PANSS total and subscales scores using Kendall's tau-b correlation coefficient estimation.
Kendall's tau-b coefficient did not reach significance for any of the PANSS scores τPANSS Positive = −.03, p = .848, τPANSS Negative = −.18, p = .221, τPANSS General = −.06, p = .657, τPANSS Total = −.11, p = .427, N = 30 (Figure 5), that is, it failed to identify an association between the induced Roelofs effect size and severity of psychotic symptoms.
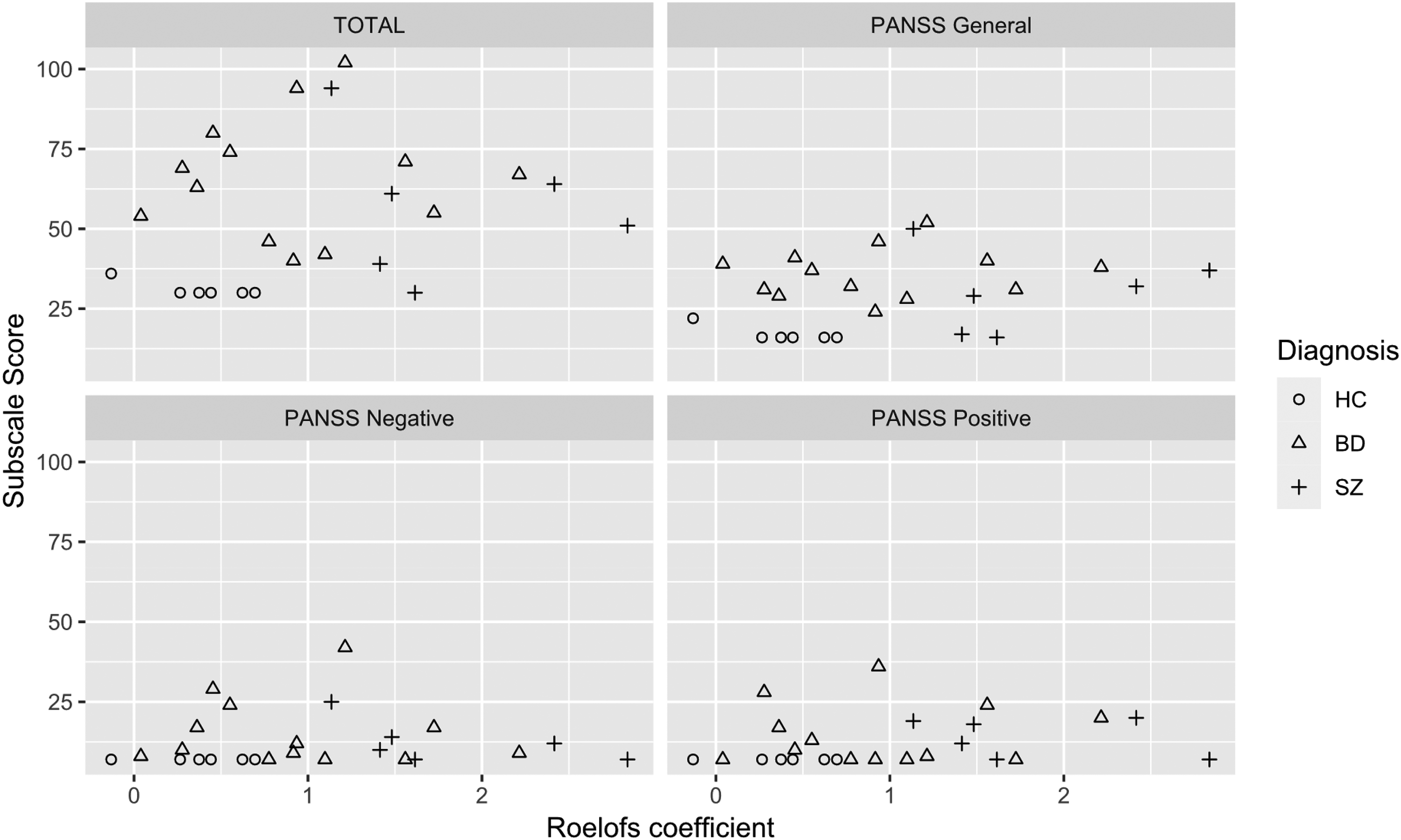
(A) Scatter plot of PANSS scales versus induced Roelofs effect size. (B) Correlogram results. Positive correlation between induced Roelofs coefficients and PANSS total and subscales scores. All the scores reveal nonsignificant correlations with the induced Roelofs effect (marked with an X). PANSS = Positive and Negative Syndrome Scale.
Induced Roelofs Effect Size and Pharmacological Load
The study assessed the relationship between individual induced Roelofs effect sizes and pharmacological load using COM–Poisson model comparisons. The procedure was conducted on each drug type and on the total pharmacological load. The AIC comparison is reported in Table 4, whereas the summary of the estimated coefficients for each model fitted is reported in Table 1S of the Supplementary materials. The intercepts-only model (no relationship with induced Roelofs effect size) was the best model for all the individual drug types, whereas the total pharmacological load was best described by the model with induced Roelofs effect size as a predictor of both λ and ν. This means that the study failed to identify any relationship between the individual induced Roelofs effect size and the load of a specific drug class, yet it identified an association between induced Roelofs effect size and the total pharmacological load. In particular, the induced Roelofs effect size was positively associated with both log(λ) (

Scatter plot of induced Roelofs effect versus pharmacological load for each drug class and corresponding fitted value of the best COM–Poisson regression models. On the x-axis, individual induced Roelofs effect size estimates; on the y-axis, the pharmacological load of each pharmacological class.
AIC per each predictor set and drug class.
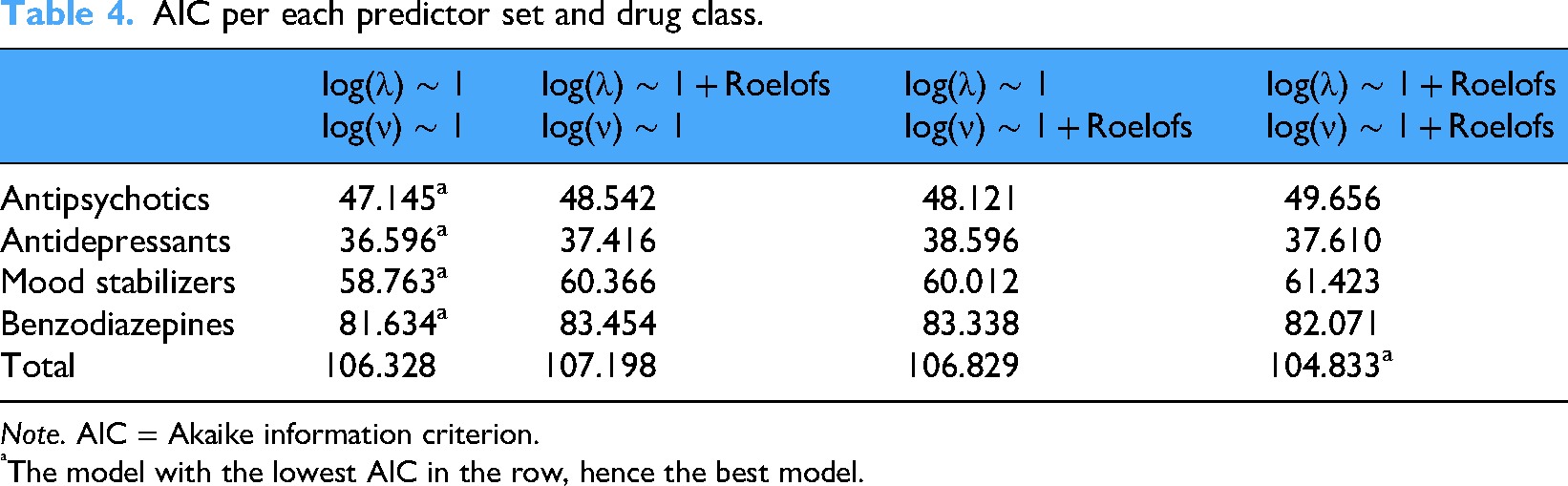
Note. AIC = Akaike information criterion.
The model with the lowest AIC in the row, hence the best model.
Discussion
The present research investigated the induced Roelofs effect in patients with SZ, BD, and in HCs searching for an association between the size of such effect and psychosis severity. According to the psychosis continuum hypothesis (Lake, 2010; Möller, 2003; Pearlson, 2015), the study hypothesized that the induced Roelofs effect size would be smaller in HC, larger in SZ, and intermediate in the BD. Concerning our results, the population with SZ showed the largest induced Roelofs effect. This finding replicates the findings of Chen et al. (2011), who previously found larger induced Roelofs effect size in patients with SZ than in the typical population. Dassonville and colleagues (Bridgeman et al., 2018; Dassonville et al., 2004; Dassonville & Bala, 2004) interpreted the induced Roelofs effect as a shift of the egocentric visual midline construct induced by the perceptual context. While on the one hand this interpretation is in line with the literature on SZ reporting hyperresponsiveness to perceptual information (Chen et al., 2011; Freedman et al., 1987), on the other hand, the effect of perceptual context does not seem to generalize to other similar mental constructs, such as the visual vertical (or horizontal). Indeed, several studies investigated the balance between verticality and perceptual context using variegate methodologies, such as the rod-and-frame test (Shanker, 1980) and different parameterizations of the surround suppression test (Grzeczkowski et al., 2018; Seymour & Kaliuzhna, 2022; Tibber et al., 2013; Yang et al., 2013b), and none of them found significant differences between SZ and controls (Grzeczkowski et al., 2018). The difference between induced Roelofs illusion and the abovementioned tilt illusions may stem from the fact that the regulation of the balance between egocentric mental constructs and perceptual context differs depending on the constructs investigated. Notwithstanding that, it is also possible that such differences may arise from methodological issues. For example, Grzeczkowski et al. (2018) used only two trials to estimate the strength of illusions, which could affect the reliability of their findings. This highlights the importance of considering methodological differences, as emphasized by Wincza et al. (2024). They noted that the magnitude of visual illusions, such as the vertical–horizontal illusion, can differ significantly depending on the method used. Specifically, they reported opposite age-related trends in the susceptibility to some visual illusions when using adjustment-like methods compared to forced-choices. This suggests that the choice of method can influence the observed effect and should be carefully considered when designing experiments and when comparing them. Future studies are needed to clarify the specificities of such processes, also in light of the evidence on the typical population suggesting the existence of a common factor underlying induced Roelofs effect and rod-and-frame illusion (Walter et al., 2009). The population with BD showed an intermediate induced Roelofs effect. This is particularly interesting because it is to our knowledge the first assessment of the induced Roelofs effect in BD and the first study on this population reporting abnormal susceptivity to a static visual illusion different from surround contrast suppression (Schallmo et al., 2015; Yang et al., 2013b). The intermediate induced Roelofs effect size of patients with BD also suggests that an exaggerated induced Roelofs effect is not an endophenotype of SZ and stands in favor of the psychosis continuum hypothesis associating DB and SZ (Möller, 2003). That said, the psychosis correlates reflected by the induced Roelofs effect remain unknown: the study did not find significant correlations between the effect and any of the PANSS or MCCB total and subscales scores. Combining this result with the result from the classification analysis (the patient diagnosis discrimination improvement found by combining the MCCB subscales with the induced Roelofs effect estimates), we conclude that no state-of-the-art clinical dimension or cognitive domain of the psychotic spectrum assessed in this study is related to the effect. This is a relevant finding which shows how including the assessment of perceptual alterations in the clinical evaluation process can be fruitful. Indeed, efforts to identify reliable and standardized perceptual markers of psychosis have been made already (Silverstein & Keane, 2011) and are currently ongoing (Schallmo et al., 2023). That said, our results are only preliminary, as the number of participants is limited. Future replications of this study, conducted with a larger pool of samples and clinicians from different centers, are necessary to confirm our findings.
The lack of correlation between induced Roelofs effect size and psychopathological scales or cognitive tests opens to the matter of what psychosis correlates underlie the susceptibility to the effect. We believe that a good candidate is the systemizing trait, that is, the ability and predilection for analyzing, understanding and building complex systems (Walter et al., 2009). Indeed, Walter and colleagues showed that in the typical population a larger induced Roelofs effect size is associated with poorer systemizing (Walter et al., 2009). At the same time, poor systemizing has been proposed as a core dimension of schizotypal traits (Möller, 2003). Therefore, conceptually speaking, our results would close the loop between induced Roelofs effect size, schizotypal traits, and systemizing traits. Notwithstanding, the evidence about schizotypal traits and systemizing is to date limited and contrasted (Andersen, 2022; Larson et al., 2015; Russell-Smith et al., 2013). Brosnan et al. (2010) found that, in a sample of female undergraduates, systemizing loaded negatively on a factor that included psychosis-related traits such as paranoia, thought insertion, and strange experiences, suggesting an inverse association between positive schizotypy (unusual perceptual experiences, odd beliefs, and cognitive disorganization) and systemizing in this population. A similar pattern was found by Larson et al. (2015): less systemizing in a sample of people with autism spectrum disorder and co-occurring psychosis than in a sample without co-occurring psychosis. Russell-Smith et al. (2013), instead, did not find significant associations between systemizing and positive schizotypy in a large sample of healthy participants, thus providing evidence contrasting the positive schizotypy—poor systemizing association. Andersen (2022) posited that the poor systemizing in high positive schizotypy may be explained as large weighting of top-down priors and low weighting of sensory inputs, which is in line with the results of Lányi et al. (2024) reporting larger Müller-Lyer illusion in individuals with high positive schizotypy. Such interpretation seems in contrast to our finding showing an apparent overweighting of contextual sensory information (the frame) over the prior (the visual midline). However, although both the Müller-Lyer illusion and the induced Roelofs effect involve higher-level perceptual processing, they differ in the type of information weighting they require. The Müller-Lyer illusion is primarily explained by priors related to the object geometry (Amir & Firestone, 2025; Gregory, 1997). In contrast, the induced Roelofs effect depends on the integration of egocentric and allocentric spatial reference frames, where egocentric information reflects an internalized prior and allocentric information derives from the current sensory input (Dassonville et al., 2004). This distinction indicates that, although both illusions require balancing prior knowledge and sensory evidence, they operate within different representational domains, object-centered for Müller-Lyer and spatial-frame-centered for Roelofs, which may account for their divergent associations with systemizing traits. Supporting this domain specificity, Axelrod et al. (2017) demonstrated that behavioral judgments show notable similarity across geometrical illusions but not between geometrical and nongeometrical illusions, suggesting shared mechanisms within the geometric class that differ from other perceptual distortions. Future effort is necessary to unravel the association between induced Roelofs effect, schizotypy, and systemizing in both the nonclinical (Andersen, 2022) and the clinical population, where expecting a larger effect is reasonable.
The individual induced Roelofs effect size was associated with the total pharmacological load, but not with the load of individual pharmacological class. This finding is in line with the literature, as it is known that the impact of single drugs on cognitive or behavioral tasks may vary and might not reach statistical significance on their own; however, significant effects emerge when considering the cumulative effect of multiple drugs (Johnson et al., 2008). The COM–Poisson regression revealed that the induced Roelofs effect size was positively associated with the mean parameter (log(λ)) and negatively associated with the dispersion parameter (log(ν)). This means that as Roelofs effect size increases, the expected pharmacological load tends to increase, while the variability around that expectation decreases. Because the COM–Poisson distribution combines these two parameters in a nonlinear way, the result is a concave, “rise-and-fall” pattern: patients with intermediate Roelofs effect sizes tend to have higher pharmacological loads, while those with either low or high effect sizes tend to have lower loads (Figure 6). An explanation of this concave, “rise-and-fall” relationship is defined by the compensatory mechanism that comes into play. From the literature, to achieve optimal therapeutic outcomes, the pharmacological load is decided according to the compensatory responses to medications (Pacchiarotti et al., 2013), which may explain the “raise.” However, the prolonged use of medications in patients with long-lasting disease course (Sramek et al., 1990) can increase the tolerance to medications (Kosten & Ziedonis, 1997; Margolese et al., 2004; Mueser et al., 1990, 1995), and potentially explaining the “fall.” Another reason may be that the effect found reflects the heterogeneity in the patient groups’ pharmacological load, which is higher in the BD group than in the SZ group, that is, the effect may be spurious. That said, the sample size is too small to correct the association between induced Roelofs effect size and pharmacological load according to the abovementioned confounding effects, therefore verifying such interpretation will require dedicated investigations.
Aside from the small number of participants, the study is also limited by their heterogeneity in terms of population (e.g., BD-I and BD-II pooled together), pathology onset, symptomatology, and medication. Moreover, even if no association between induced Roelofs effect and attention score in the MCCB scale has been found and the percentage of correct responses with central frame corresponds to the expected value, we cannot exclude that some differences in the illusion may have arisen due to different attention levels during the experimental sessions. Repeating the study using an eye-tracker would help better understand if participants comply with the instructions and maintain an adequate attention level through the experimental session.
To conclude, the present research found that the induced Roelofs effect size increases with psychosis severity (small effect in HCs, intermediate in BD, large in SZ). Additional explorations failed to relate the interindividual effect size to the participants’ cognitive performance (as revealed by scores of the MCCB total and subscales), to the patients’ psychotic symptomatology (as revealed by PANSS total and subscales scores), or to specific pharmacological treatments. However, the study found an association with the overall amount of pharmacological load. Additionally, the study used naïve Bayes classification to show how the patients’ diagnoses discrimination improved combining the MCCB scores with the induced Roelofs effect estimates compared to the discrimination based on the MCCB scores alone. This finding supports the speculation that the induced Roelofs effect size underlies a process related to psychosis that is missing from the current clinical and cognitive state-of-the-art assessments. Such insights underscore the intricate interplay between perceptual illusions and psychiatric disorders, as well as the value of integrating perceptual and cognitive information to refine diagnostic processes and contribute to a more nuanced understanding of the complex interplay between psychiatric conditions, medications, and individual characteristics. Future work should first aim to consolidate the findings presented here by increasing the sample size, uniform the sample characteristics. Second, it should focus on investigating the relationship between the induced Roelofs illusion and other similar perceptual illusions like the rod-and-frame. Third, it should delve deeper into what psychosis domain is reflected into the sensitivity to the induced Roelofs illusion. All these future efforts would help clarify the fragmented evidence concerning perceptual illusions and psychoses.
Supplemental Material
sj-docx-1-ipe-10.1177_20416695251394612 - Supplemental material for Differentiating bipolar disorder from schizophrenia: The role of the induced Roelofs illusion
Supplemental material, sj-docx-1-ipe-10.1177_20416695251394612 for Differentiating bipolar disorder from schizophrenia: The role of the induced Roelofs illusion by Davide Esposito, Jessica Bertolasi, Andrea Escelsior, Maria Bianca Amadeo, Alberto Inuggi, Margherita Perucco, Ambra Alvano, Martina Marcenaro, Alessio Zizzi, Beatriz Pereira Da Silva, Gianluca Serafini, Mario Amore and Monica Gori in i-Perception
Footnotes
Acknowledgements
The authors want to thank the patients who kindly participated in the research. The authors also sincerely thank all the healthcare workers, nurses, and doctors of the Psychiatry Unit at the IRCCS Ospedale Policlinico San Martino.
Ethical Considerations
The research protocol was approved by the local ethics committee (Comitato Etico Regionale ASL3 Liguria) and conducted in line with the Declaration of Helsinki. The study was performed following the relevant ethical guidelines and regulations.
Consent to Participate
All subjects gave written informed consent to participate in the study.
Consent for Publication
All subjects gave written informed consent to publish their data.
Author Contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was developed within the framework of the Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health (DINOGMI) and of the Unit for Visually Impaired People (U-VIP). It has been partially supported by the MYSpace project (PI Monica Gori), which has received funding from the European Research Council (ERC) under the European Union's Horizon 2020 research and innovation program (grant agreement No 948349). Furthermore, this works was also partially supported by #NEXTGENERATIONEU (NGEU) and funded by the Italian Ministry of University and Research (MUR), National Recovery and Resilience Plan (NRPP), project MNESYS (PE0000006) - A Multiscale integrated approach to the study of the nervous system in health and disease (DN. 1553 11.10.2022).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.