
Abstract
Background:
Rheumatoid arthritis (RA) is a chronic autoimmune disease that requires long-term pharmacotherapy and self-management. Disease knowledge and medication adherence are essential for achieving optimal outcomes, but remain under-researched in low-resource settings such as Nepal.
Objective:
This study aimed to assess the factors associated with disease knowledge and medication adherence among RA patients attending a private rheumatology clinic in Nepal.
Design:
Cross-sectional study.
Methods:
A hospital-based cross-sectional study was conducted from March to September 2023 among 428 RA patients who had been on a disease-modifying anti-rheumatic drugs (DMARDs) regimen for at least 3 months prior to the start of the study. Disease knowledge was assessed using the Rheumatoid Arthritis Knowledge Assessment Scale, and medication adherence was measured using the General Medication Adherence Scale. Pearson’s χ² test and multivariate logistic regression analyses were employed to examine the associations between levels of the disease knowledge, medication adherence, and related variables, using a 95% confidence interval and a 5% level of significance.
Results:
A total of 82.2% of RA patients had poor knowledge of the disease, and 62.2% demonstrated low medication adherence. Poor disease knowledge was significantly associated with older age, illiteracy, being a homemaker or unemployed, functional disability, higher disease activity, lower income, and absence of a family history of RA. Low medication adherence was significantly associated with male gender, being a homemaker or unemployed, rural residence, longer disease duration, presence of the comorbidities, obesity, higher disease activity, functional disability, and the use of multiple DMARDs.
Conclusion:
The findings highlight a critical gap in the disease knowledge and medication adherence among RA patients in Nepal, emphasizing the urgent need for targeted educational and adherence-enhancing interventions. Tailored strategies focusing on older adults, individuals with low literacy, and rural populations are essential to improve health outcomes and support effective RA management in resource-constrained settings.
Plain language summary
Rheumatoid arthritis (RA) is a long-term disease that causes joint pain, swelling, and progressive joint damage. People with RA need to take DMARD medications regularly and manage their condition through self-care. However, in countries like Nepal, many patients may not fully understand their disease or follow their treatment plans properly. This study looked at 428 people with RA who were receiving care at a private clinic in Nepal. It aimed to find out what factors are linked to how much patients know about RA and how well they stick to their medication routines. Researchers used two questionnaires to measure patients’ disease knowledge and how well they followed their treatment. The results showed that over 80% of patients had poor knowledge about RA, and more than 60% were not taking their medications as prescribed. Poor knowledge was more common among older adults, people with little or no education, those who were unemployed, had lower income, more severe disease, or no family history of RA. Poor medication adherence was linked to being male, unemployed, living in rural areas, having other health conditions, being overweight, and using multiple medications. These findings show that many RA patients in Nepal lack important knowledge and struggle to take their medications properly. The study highlights the need for education programs and support systems, especially for people who are older, less educated, or live in rural areas. Improving these areas can help patients manage RA better and live healthier lives.
Keywords
Introduction
Rheumatoid arthritis (RA) is a chronic, systemic autoimmune disorder primarily characterized by persistent synovial inflammation, which leads to joint pain, deformity, functional disability, increased morbidity, reduced health-related quality of life, and premature mortality. 1 Globally, RA affects approximately 0.5%–1% of the population, although prevalence rates vary considerably across geographic regions. 2 The disease predominantly affects middle-aged individuals and older adult women. 3 In low- and middle-income countries (LMICs) such as Nepal, musculoskeletal conditions are increasingly recognized as a major public health concern. A national survey reported a 17% prevalence of joint pain in the general population, 4 while a study conducted in a mountainous region of Nepal found that 4.3% of males and 7.1% of females were affected by RA, highlighting a notable sex-based disparity in disease burden. 5
Over the past decade, significant advancements have been made in the treatment of RA, particularly with the introduction of novel biological therapies. Evidence suggests that early diagnosis and intensive treatment using both conventional and biological disease-modifying anti-rheumatic drugs (DMARDs) can effectively alleviate symptoms and slow disease progression. 6 However, the medication adherence among RA patients remains suboptimal, with reported rates ranging from 16.4% to 76.9%.3,7,8 Medication nonadherence remains a significant global health concern, particularly among individuals with chronic diseases. In RA, poor adherence is associated with increased disease activity, accelerated joint damage, greater disability, reduced quality of life, and the need for more complex and costly therapeutic regimens, raising the risk of adverse drug events and drug interactions.1–9 These consequences contribute to the rising economic burden on patients and healthcare systems.
Patient knowledge plays a vital role in shaping health behaviors, enhancing medication adherence, and influencing health outcomes. Individuals with a comprehensive understanding of RA and its long-term implications are more likely to adhere to their prescriptions and engage in shared decision-making with healthcare professionals. 10 Such patients often experience better disease control, higher remission rates, improved physical functioning, slower disease progression, and a reduced likelihood of requiring more aggressive treatments. 11 In contrast, limited knowledge of disease can perpetuate misconceptions, nonadherence, and poorer clinical outcomes.
Several socio-demographic and clinical variables, including age, educational level, income, disease duration, and presence of comorbid conditions, have been reported to influence both disease knowledge and adherence in RA patients.10–12 Moreover, patients’ beliefs and perceptions about medication, health literacy, physician–patient relationship, and access to healthcare services play critical roles in shaping adherence behavior, particularly in LMICs.10,12,13
Despite the increasing burden of RA and the recognized importance of disease knowledge and medication adherence in effective disease management, research in the context of Nepal remains scarce. A comprehensive understanding of these elements is crucial to addressing existing literature gaps and guiding healthcare professionals and policymakers in developing context-specific interventions that enhance patient education and promote sustained adherence. Such efforts can ultimately optimize treatment outcomes and reduce the healthcare burden. Hence, this study aims to explore the factors associated with disease knowledge and medication adherence among RA patients attending a private rheumatology clinic in Kathmandu, Nepal.
Materials and methods
This study was conducted and reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. 14
Study design, setting, and population
A prospective, observational cross-sectional study was conducted over a 6-month period from March to September 2023 at the National Center for Rheumatic Diseases, located in Ratopul, Kathmandu. It is the first specialized clinic in Nepal dealing with the diagnosis and management of rheumatic diseases, which includes conditions affecting joints and connective tissues, autoimmune diseases such as RA, Gout, Lupus, Scleroderma, and other degenerative diseases such as Osteoarthritis and Ankylosing spondylitis. 15
Inclusion criteria
Adults (⩾18 years) with a confirmed diagnosis of RA, stable on a DMARD regimen for at least 3 months, attending regular follow-up visits, and willing to provide informed consent.
Exclusion criteria
Patients not on DMARDs; those with overlapping rheumatic or autoimmune syndromes; those unwilling to participate; individuals with psychiatric illness; or terminally ill patients unable to be interviewed.
Sample size and sampling techniques
The sample size was calculated using the single population proportion formula: n = Z²pq/d², 16 assuming a 95% confidence interval (CI), a 50% estimated proportion (p) due to the unknown prevalence of disease knowledge and medication adherence in the study area, and a 5% margin of error (d). After accounting for a 10% non-response rate, the final calculated sample size was 428. A convenience sampling technique was employed to recruit study participants.
Data collection
Data were collected through face-to-face interviews using a pre-tested, semi-structured questionnaire (see Supplemental File 1). Trained graduate clinical pharmacy student conducted the interviews after obtaining written informed consent from eligible participants. The data collector received 3 days of training, which covered the study objectives, data collection procedures, sampling methods, ethical considerations, and data entry techniques.
The questionnaire was originally developed in English, translated into Nepali, and then back-translated into English to ensure translation validity. All interviews were conducted in the Nepali language. The Nepali version of the questionnaire was pretested among 43 participants (10% of the total sample), who were not included in the main study but shared similar characteristics. The tool demonstrated good internal consistency, with a Cronbach’s alpha of 0.85 in the pilot study.
Outcome measures
Rheumatoid Arthritis Knowledge Assessment Scale
Patient knowledge regarding RA was assessed using a modified version of the Rheumatoid Arthritis Knowledge Assessment Scale (RAKAS) developed and validated by Naqvi et al. 17 in a South Asian context. The scale consists of 13 items covering essential aspects of RA, including disease awareness, symptoms, risk factors, complications, genetic predisposition, diagnostic tools, treatment duration, and the role of physical therapy.
Each item was scored as either correct or incorrect, with some questions allowing partial credit based on the degree of knowledge. For example, in the item assessing general awareness of RA, responses were graded as: “Yes, completely aware” (2 points), “Yes, to some extent” (1 point), and “No” (0 points). The remaining items were scored as 1 for correct and 0 for incorrect or “don’t know” responses. The total knowledge ranged from 0 to 15, with higher scores indicating greater knowledge of RA. Knowledge levels were categorized as good knowledge for scores ⩾11 (⩾70% of the total score) and poor knowledge for scores <11 (<70% of the total score).
General Medication Adherence Scale
Medication adherence was assessed using the General Medication Adherence Scale (GMAS), a validated instrument designed to evaluate both behavioral and cost-related factors influencing medication-taking practices among patients with chronic illnesses. The Nepali version of the GMAS, developed through rigorous translation, cultural adaptation, and psychometric validation by Shrestha et al., 18 was employed to ensure contextual and linguistic appropriateness for the local population.
The scale consists of 11 items addressing multiple dimensions of adherence, including forgetfulness, intentional discontinuation, regimen complexity, adverse effects, disease progression, and financial constraints. Each item is rated on a 4-point Likert scale (Always = 0, Mostly = 1, Sometimes = 2, Never = 3), yielding a total score ranging from 0 to 33, where higher scores reflect better adherence. Although the original scale categorizes adherence into high (30–33), moderate (27–29), and low (<27) levels, in this study, participants were classified into either high or low adherence groups based on the distribution of scores within the sample.
Explanatory variables
Health Assessment Questionnaire Disability Index
The Health Assessment Questionnaire Disability Index (HAQ-DI) is a widely used tool in both clinical research and routine clinical practice to assess physical disability in patients with RA. It was developed to evaluate the degree of difficulty patients experience in performing day-to-day activities related to physical function. 19 The HAQ-DI consists of 20 items across 8 categories: dressing and grooming, arising, eating, walking, hygiene, reach, grip, and common daily activities. Each item is scored on a 4-point Likert scale ranging from 0 (no difficulty) to 3 (unable to do), with the highest score in each category taken to calculate the final score. The overall HAQ-DI score is the average of the eight category scores, ranging from 0 (no disability) to 3 (completely disabled). In this study, functional disability was defined as an HAQ-DI score ⩾1, consistent with previous literature indicating this threshold as clinically significant.
Disease Activity Score 28-erythrocyte sedimentation rate
The Disease Activity Score 28-erythrocyte sedimentation rate (DAS28-ESR) is a widely used clinical tool for assessing disease activity in patients with RA, derived from a simplified version of the original DAS44. 20 The DAS28 includes four components: the number of tender joints (TJC28), the number of swollen joints (SJC28), the ESR, and the patient’s global health assessment using a visual analog scale (VAS, 0–100). The DAS28-ESR is calculated using the following validated formula:

The total DAS28 score ranges from 0 to 9.4, where higher values indicate greater disease activity. In this study, disease activity was categorized into three groups: remission/low disease activity (DAS28 ⩽ 3.2), moderate disease activity (3.2 < DAS28 ⩽ 5.1), and high disease activity (DAS28 > 5.1).20,21
Other variables included were age (categorized as ⩽50 and >50 years), gender (male/female), marital status (ever married/never married), religion (Hindu, Buddhism, Islam, and Christianity), ethnicity (advantaged/disadvantaged), and educational status (illiterate/literate). The current occupation of participants was categorized as unemployed, professional workers, and homemakers. Residence was recorded as either urban or rural.
Clinical variables included duration of illness (⩽5/>5 years), presence of comorbidities (yes/no), and body mass index, categorized as normal weight, overweight, and obese. Socioeconomic status was assessed based on annual household income in Nepalese Rupees (NPR), categorized as <300,000; 300,000–500,000; and ⩾500,000. Substance use was categorized into none, smoking, and alcohol use. Family history of RA was recorded as yes or no. Medication use was evaluated by the number of DMARDs taken, categorized as ⩽2, 3, and ⩾3.
Statistical analysis
Data were cleaned and analyzed using SAS version 9.4 (SAS Institute Inc., 2013), Cary, NC, USA. 22 Descriptive statistics were computed to summarize the characteristics of the study population. Bivariate analyses were conducted to examine associations between explanatory variables and outcomes: the Chi-square test was applied for categorical variables with sufficient expected counts, Fisher’s exact test was used when expected cell counts were <5, and the likelihood ratio test was used when appropriate for sparse data.
Multicollinearity among independent variables was assessed using the Variance Inflation Factor (VIF), with all variables exhibiting VIF values below 2.5, indicating no significant multicollinearity. Accordingly, all independent variables listed in Table 1 were included in multivariable logistic regression models to adjust for potential confounding. Both unadjusted and adjusted odds ratios (ORs) with 95% CIs are presented in Tables 2 and 3 for poor disease knowledge and low medication adherence. A p-value of less than 0.05 was considered statistically significant.
Baseline characteristics and bivariate analyses by disease knowledge and medication adherence (n = 428).

RA: rheumatoid arthritis; n: frequency; %: percentage; BMI: body mass index; DMARDs: disease-modifying anti-rheumatic drugs; DAS-28: Disease Activity Score-28; HAQ-DI: Health Assessment Questionnaire Disability Index; NPR: Nepalese Rupees.
Chi square test.
Fisher’s exact test.
Likelihood ratio.
Unadjusted and adjusted ORs for factors associated with level of disease knowledge.
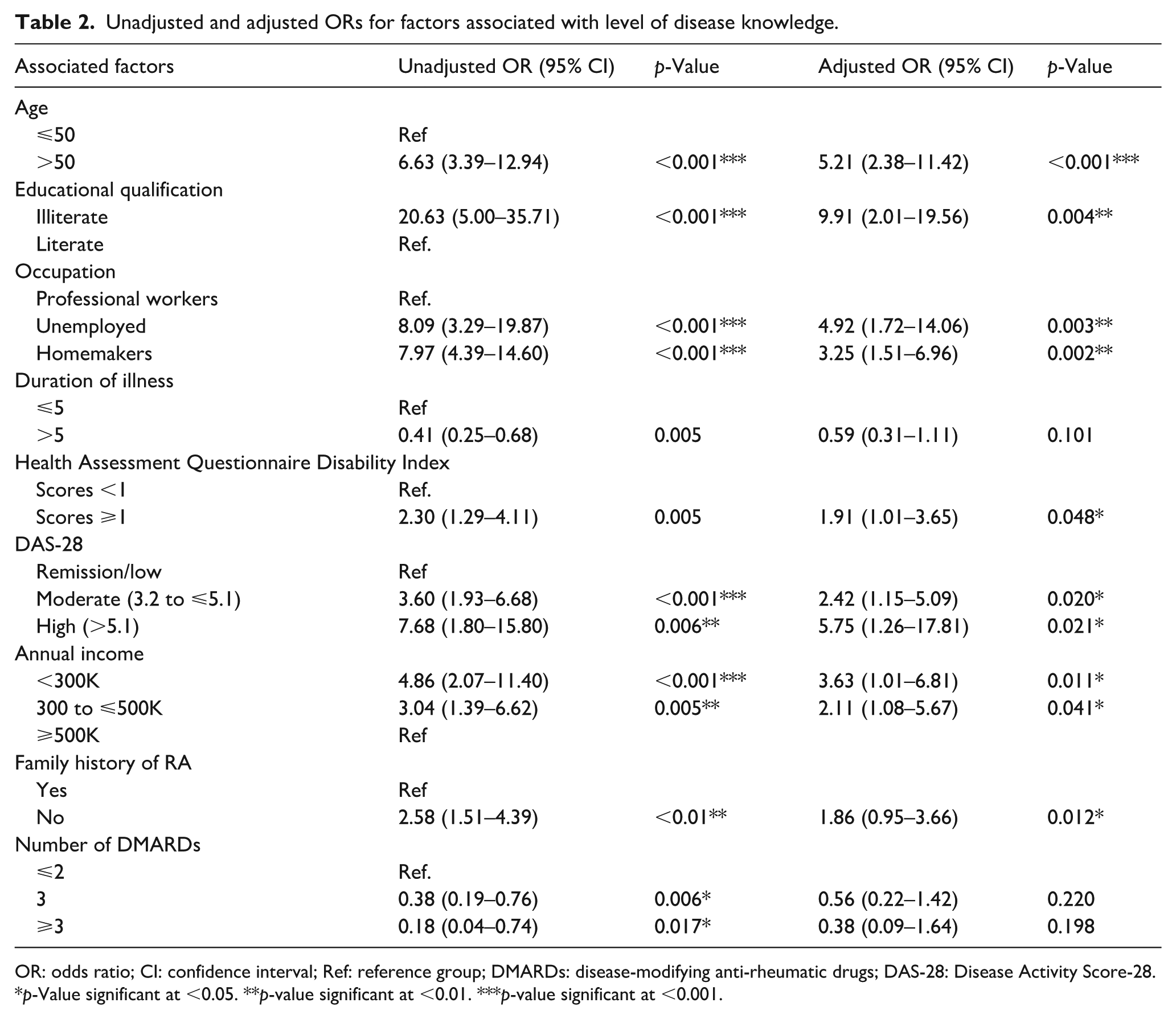
OR: odds ratio; CI: confidence interval; Ref: reference group; DMARDs: disease-modifying anti-rheumatic drugs; DAS-28: Disease Activity Score-28.
p-Value significant at <0.05. **p-value significant at <0.01. ***p-value significant at <0.001.
Unadjusted and adjusted ORs for factors associated with level of medication adherence.
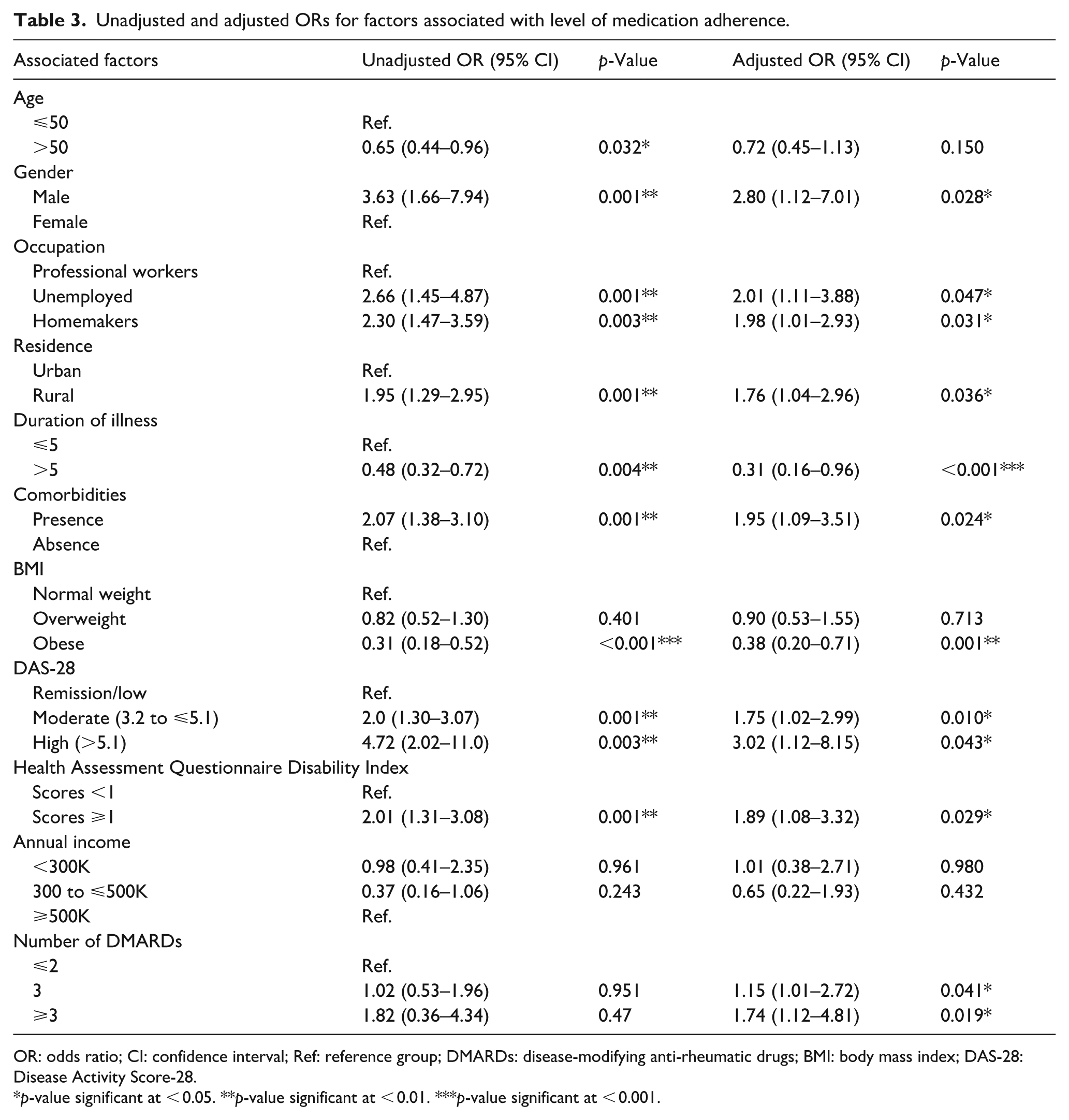
OR: odds ratio; CI: confidence interval; Ref: reference group; DMARDs: disease-modifying anti-rheumatic drugs; BMI: body mass index; DAS-28: Disease Activity Score-28.
p-value significant at < 0.05. **p-value significant at < 0.01. ***p-value significant at < 0.001.
Ethical consideration
The study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Institutional Review Committee (IRC) of CiST College (Ref. No: 65/079/080). Written informed consent was obtained from all participants prior to data collection. For individuals with limited literacy, the consent form was explained verbally in Nepali in the presence of an impartial witness, who signed to validate the process, while participants provided consent through a thumbprint. They were informed about the voluntary nature of their participation, confidentiality safeguards, and their right to refuse or withdraw from the study at any time without any consequences. Anonymity was ensured by assigning unique identification codes, and personal identifiers were securely stored separately from the research dataset.
Results
Table 1 presents the baseline characteristics and bivariate analyses of disease knowledge and medication adherence among RA patients (n = 428). More than half of the participants were aged 50 years or younger (54.2%), and the majority were female (88.6%), ever married (82.2%), and Hindu (73.6%). Regarding ethnicity, 52.3% belonged to advantaged groups, while 47.6% were from disadvantaged backgrounds. Nearly three-fourths were literate (70.1%). In terms of occupation, 52.6% were homemakers, 29.7% were professional workers and 17.7% were unemployed. Most participants resided in urban areas (60.9%) and had a disease duration of 5 years or less (62.6%). Approaching 60.0% had no comorbidities and were of normal weight (45.8%), with 33.9% overweight and 20.3% obese. Functional disability (HAQ-DI ≥ 1) was observed in 36.7%, while 47.7% had moderate-to-high disease activity (DAS-28 > 3.2). Regarding annual income, 54.7% earned NPR 300–500K, and 37.8% earned less than NPR 300K. Most participants had no history of substance use (45.1%), no family history of RA (77.3%), and were taking two or fewer DMARDs (88.1%).
Bivariate analyses identified several statistically significant associations between various factors and both disease knowledge and medication adherence. Poor disease knowledge was significantly associated with age over 50 years, illiteracy, unemployment or homemaker status, longer disease duration, greater functional disability, higher disease activity, lower income, absence of a family history of RA, and use of fewer DMARDs. Similarly, low medication adherence was significantly associated with male gender, age over 50 years, unemployed or home makers, rural residents, longer disease duration, presence of comorbidities, obesity, higher disease activity, greater functional disability, lower income, and use of multiple DMARDs. No significant associations were observed for marital status, religion, ethnicity, or substance use with either disease knowledge or medication adherence.
Table 2 presents the unadjusted and adjusted logistic regression analyses of factors associated with disease knowledge among RA patients. After adjusting for potential confounders, several variables were significantly associated with poor disease knowledge. Patients aged over 50 years were more than five times (AOR:5.21; 95% CI: 2.38-11.42) as likely to have poor disease knowledge compared to those aged 50 years or younger. Illiterate individuals had nearly tenfold (AOR: 9.91; 95% CI:2.01-19.56) higher odds of poor knowledge than literate patients. In terms of occupation, unemployed individuals (AOR:4.92; 95% CI:1.72-14.06) and homemakers (AOR:3.25; 95% CI:1.51-6.96) were more likely to have poor disease knowledge than those engaged in professional work. Patients with greater functional disability (HAQ-DI score ≥ 1) (AOR:1.91; 95% CI: 1.01-3.65), had higher odds of poor knowledge. Similarly, patients with moderate (DAS 28 3.2-5.1; AOR: 2.42; 95% CI: 1.15-5.09) and high disease activity (DAS 28> 5.1; AOR:5.75; 95% CI: 1.26-17.81) were significantly more likely to have poor knowledge than their counterparts.
Patients earning less than 300K (AOR:3.63; 95% CI: 1.01-6.81) and NRs 300-500 K (AOR: 2.11; 95% CI: 1.08 -5.67) had higher odds of poor knowledge compared with those earning ≥ 500K. Absence, of a family history of RA was also associated with higher odds of poor knowledge (AOR: 1.86; 95% CI: 0.95-3.66), although this association did not reach statistical significance. Although patients taking ≤ 2 DMARDs were more likely to have poor knowledge, this association was not statistically significant after adjustment.
Table 3 presents the unadjusted and adjusted logistic regression analyses of factors associated with medication adherence among RA patients. Male patients were nearly three times (AOR: 2.80; CI: 1.12-7.01) more likely to exhibit low medication adherence compared with females. Occupational status remained significant, with unemployed individuals (AOR: 2.01; 95% CI: 1.11-3.88) and homemakers (AOR: 1.98; 95% CI: 1.01-2.93) showing higher odds of low adherence than those in professional occupations.Patients residing in rural areas had significantly higher odds (AOR: 1.76; 95% CI: 1.04-2.96) of low adherence than urban residents. Longer disease duration (> 5 years) was associated with lower medication adherence (AOR: 0.31; 95% CI: 0.16-0.96). The presence of comorbidities (AOR: 1.95; 95% CI: 1.09-3.51) was significantly associated with low adherence, while obesity (AOR: 0.38; 95% CI: 0.20-0.71) was also independently associated with poorer adherence.
Patients with moderate (AOR: 1.75; 95% CI: 1,02-2.99) and high disease activity (AOR: 3.02; 95% CI: 1.12-8.15) were more likely to report low adherence compared to those in remission or with low disease activity. Higher functional disability (HAQ-DI ≥ 1) was another significant factor, with these patients nearly twice as likely to have low adherence (AOR: 1.89; 95% CI: 1.08-3.32). Although income was significant in bivariate analyses, it did not remain statistically significant in the adjusted model. However, patients receiving ≥ 3 DMARDS were significantly more likely to demonstrate low medication adherence compared with those receiving ≤ 2 DMARDs (AOR: 1.74; 95% CI: 1.12-4.81).
Discussion
This study provides valuable insights into the multifactorial determinants of disease knowledge and medication adherence among patients with RA attending a private rheumatology clinic in Nepal. It identifies critical gaps in patient knowledge and adherence, with poor disease knowledge significantly associated with older age, illiteracy, homemaker or unemployed status, functional disability, higher disease activity, lower income, and absence of a family history of RA. Similarly, low medication adherence was significantly associated with male gender, homemaker or unemployed status, rural residence, longer disease duration, comorbidities, obesity, higher disease activity, functional disability, and the use of multiple DMARDs. Details of the DMARD regimens used by participants are presented in Supplemental File 2.
The high proportion of patients with poor disease knowledge and low medication adherence aligns with findings from other resource-constrained settings, where barriers such as low educational attainment, limited health literacy, and weak healthcare infrastructure impede effective management of chronic diseases.8,13,23 In contrast, a study from Saudi Arabia reported better patient knowledge, likely due to broader access to healthcare education and support systems. 24
Older age was significantly associated with poorer disease knowledge, potentially due to cognitive decline, lower health literacy, and limited engagement with digital or formal health education resources. 10 Illiteracy emerged as a strong predictor, consistent with evidence from Pakistan highlighting the crucial role of education in shaping RA awareness among South Asian populations. 17 Individuals who are illiterate may struggle to understand complex medical instructions and their condition, underscoring the need for tailored communication strategies designed for low-literacy audiences.
Occupational status also influenced both disease knowledge and medication adherence. Professional workers demonstrated better disease understanding and adherence, possibly due to higher education levels, improved access to healthcare, and greater autonomy in health-related decisions. In contrast, homemakers and unemployed individuals, who often face financial dependence and limited exposure to healthcare facilities, were significantly more likely to report poorer outcomes. 7
Disease severity further contributed to gaps in knowledge and medication adherence. Patients with higher disease activity and greater functional limitations were more likely to have inadequate knowledge and poor adherence, consistent with findings from previous studies.1,2,25,26 Physical impairment and chronic symptoms may lead to psychological distress, reduce motivation, and hinder participation in health education or self-management activities, thereby perpetuating a cycle of poor engagement and worsening health outcomes.
Lower income and the absence of a family history of RA were independently associated with poor disease knowledge. Socioeconomic disadvantages can limit access to medical services and educational resources, while lacking familial experience with RA may reduce opportunities for informal knowledge-sharing and firsthand insight into disease management.23,27 Interestingly, although unadjusted analyses showed better knowledge among patients using multiple DMARDs, possibly due to more frequent healthcare interactions, this association did not persist after adjustment, suggesting potential confounding by disease severity.
Medication adherence is a cornerstone of effective RA management. In this study, nearly half of the participants demonstrated low adherence to DMARD therapy. This finding is comparable to results from Australia, where adherence rates were around 50%, particularly among older patients, those with middle income, and shorter disease duration. 11 However, other studies have found no significant associations between adherence and factors such as age, employment status, disease duration, or disease activity, 3 highlighting the contextual variability in determinants of medication adherence.
In this study, female patients demonstrated higher adherence, possibly reflecting greater health consciousness and caregiving roles, which are often associated with more consistent health behaviors and compliance with long-term therapies. 11 Rural residence emerged as a significant barrier to adherence, likely due to disparities in healthcare infrastructure, limited access to specialized care, and reduced exposure to educational interventions in rural areas.
A noteworthy finding was the significant association between longer disease duration and poor medication adherence, which may reflect treatment fatigue, reduced motivation, or a perceived decline in medication efficacy over time.11,28
The negative impact of comorbidities and obesity on medication adherence underscores the complexities of managing multimorbidity. Patients with multiple health conditions often face polypharmacy, increased risk of drug–drug interactions or adverse effects, and greater psychological and financial burdens, all of which may contribute to intentional nonadherence. In addition, patients on multiple DMARDs were more likely to be nonadherent, possibly due to complex treatment regimens, fear of side effects, and high out-of-pocket costs an especially significant issue in LMICs like Nepal.
To the best of our knowledge, this study is among the few in Nepal to comprehensively assess disease knowledge and medication adherence in RA patients. The use of validated, culturally adapted tools and a relatively large sample strengthens the findings. However, several limitations should be acknowledged. The cross-sectional design limits causal inference, and potential confounders such as comorbidities, concurrent treatments, psychosocial factors, and patient–provider communication were not fully addressed. Convenience sampling from a single private urban center may introduce selection bias, and reliance on self-reported adherence could underestimate nonadherence. Unmeasured contextual or cultural factors may also have influenced outcomes. Future longitudinal, multicenter studies with broader adjustment for confounders are warranted.
Conclusion
The study demonstrates that socio-demographic and clinical factors significantly influence the disease knowledge and medication adherence among RA patients in Nepal. The findings underscore the need for targeted, multidisciplinary strategies centered on patient education, health literacy, and improved access to care to address disparities among vulnerable subgroups such as older adults, individuals with limited literacy, and rural residents. Integrating these approaches into routine RA management can support better adherence and encourage patients, ultimately improving clinical outcomes in resource-constrained settings.
Supplemental Material
sj-docx-1-taj-10.1177_20406223251408617 – Supplemental material for Factors associated with disease knowledge and medication adherence among rheumatoid arthritis patients attending a private rheumatology clinic: A cross-sectional study
Supplemental material, sj-docx-1-taj-10.1177_20406223251408617 for Factors associated with disease knowledge and medication adherence among rheumatoid arthritis patients attending a private rheumatology clinic: A cross-sectional study by Sabina Sankhi, Nirmal Raj Marasine and Sujita Khadka in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-2-taj-10.1177_20406223251408617 – Supplemental material for Factors associated with disease knowledge and medication adherence among rheumatoid arthritis patients attending a private rheumatology clinic: A cross-sectional study
Supplemental material, sj-docx-2-taj-10.1177_20406223251408617 for Factors associated with disease knowledge and medication adherence among rheumatoid arthritis patients attending a private rheumatology clinic: A cross-sectional study by Sabina Sankhi, Nirmal Raj Marasine and Sujita Khadka in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-3-taj-10.1177_20406223251408617 – Supplemental material for Factors associated with disease knowledge and medication adherence among rheumatoid arthritis patients attending a private rheumatology clinic: A cross-sectional study
Supplemental material, sj-docx-3-taj-10.1177_20406223251408617 for Factors associated with disease knowledge and medication adherence among rheumatoid arthritis patients attending a private rheumatology clinic: A cross-sectional study by Sabina Sankhi, Nirmal Raj Marasine and Sujita Khadka in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
The authors would like to acknowledge the CiST College for providing the opportunity to conduct this study, the doctors and staff of the National Center for Rheumatic Diseases for their invaluable support during data collection, and all the participants for their time and willingness to be part of this research.
Ethical considerations and consent to participate
The study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Institutional Review Committee (IRC) of CiST College (Ref. No: 65/079/080). Written informed consent was obtained from all participants prior to data collection. For individuals with limited literacy, the consent form was explained verbally in Nepali in the presence of an impartial witness, who signed to validate the process, while participants provided consent through a thumbprint. They were informed about the voluntary nature of their participation, confidentiality safeguards, and their right to refuse or withdraw from the study at any time without any consequences. Anonymity was ensured by assigning unique identification codes, and personal identifiers were securely stored separately from the research dataset.
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The raw data used to support the findings of this study are made available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.