
Abstract
Background:
Obesity is a significant public health concern linked to various health complications, including periodontitis. This study uniquely integrates multiple obesity indicators (body mass index (BMI), waist circumference (WC), and waist-to-hip ratio (WHR)) alongside clinical periodontal parameters and considers sociodemographic factors to provide a comprehensive analysis of the relationship between obesity and periodontitis.
Objectives:
To determine the association between BMI, WC, and WHR with periodontal clinical parameters, and to explore the role of sociodemographic and behavioral factors.
Design:
Transversal study.
Methods:
A total of 1000 adults (579 males and 421 females) with ⩾15 teeth were enrolled using systematic random sampling. Sociodemographic variables (age, sex, marital status, income, education level), behavioral factors (brushing frequency, smoking status), and anthropometric measurements (BMI, BP, WHR) were considered. Clinical periodontal parameters included probing pocket depth (PPD), bleeding on probing, clinical attachment loss (CAL), plaque index, and gingival index. Associations were assessed using multivariate regression models adjusted for age, sex, education, income, and oral hygiene habits.
Results:
The study population comprised 579 males and 421 females, predominantly aged 19–30 years. BMI classifications were 46.2% normal, 30.5% overweight, and 4.5% obese. Elevated BMI and WC were significantly associated with increased PPD and CAL (p < 0.001*). In univariate analysis, overweight (odds ratio (OR) = 2.28, p < 0.001*) and obesity (OR = 6.46, p < 0.001*) were significantly associated with periodontitis. In multivariate analysis, obesity remained significantly associated with periodontitis (adjusted OR = 3.42, p < 0.01*), as did WC (adjusted OR = 1.84, p < 0.01*). The WHR was associated with periodontitis in univariate but not in multivariate analysis.
Conclusion:
Obesity, as measured by BMI and central adiposity indicators, is independently positively associated with greater periodontitis severity. The findings highlight the importance of assessing obesity in estimating periodontal risk and structuring targeted interventions that consider both metabolic status and sociodemographic factors to optimize periodontal health benefits.
Introduction
Obesity is a health condition characterized by the excessive accumulation of body fat, which can negatively affect overall health, potentially shortening life expectancy and increasing the risk of various medical problems. According to a 2022 World Health Organization report, the prevalence of obesity has reached epidemic levels in most European countries. This means that 59% of adults and nearly one in three children are affected by this condition. 1
In the current medical landscape, adipose tissue is widely recognized as a dynamic metabolic and endocrine organ that plays a highly active role in the production and release of various hormones. These bioactive molecules, such as leptin, tumor necrosis factor α (TNF-α), interleukin-6 (IL-6), complement components, plasminogen activator inhibitor type 1, and proteins associated with the renin-angiotensin system, contribute to the regulation of food intake, insulin sensitivity, and inflammation. 2 Periodontitis is an inflammatory disease that causes significant damage to the gingiva, periodontal ligament, and alveolar bone. It is mediated by the involvement of pro-inflammatory cytokines such as IL-1β, IL-6, IL-10, IL-12, interferon-γ, and TNF-α.3,4
Scientific evidence supporting a bidirectional relationship between obesity and periodontitis, mediated by systemic inflammation and immune dysregulation, is growing.5–14 Central adiposity, assessed by waist circumference (WC) and waist-to-hip ratio (WHR), has shown significant associations with periodontal destruction, independent of body mass index (BMI).6–13 Additionally, recent studies have highlighted the important role of chemical control agents of dental biofilm, such as chlorhexidine, both in biofilm modulation and in their active participation in systemic inflammatory responses and periodontal tissue mediators. 15
In this context, we hypothesize that a higher BMI and central adiposity are significantly associated with greater periodontitis severity, independent of confounding factors, and that the association could be mediated by systemic inflammatory pathways modulated by both metabolic status and oral antimicrobial agents, such as chlorhexidine. The importance of the present study lies in a more precise and in-depth understanding of this bidirectional interaction, which will allow for the design of more targeted and comprehensive preventive and therapeutic strategies aimed at periodontal health and the control of systemic factors linked to obesity. Therefore, the primary objective is to evaluate the association between BMI, WC, and WHR with periodontal clinical parameters in adults, and as a secondary objective, to analyze the influence of sociodemographic factors on this association.
Methods
Study design
A descriptive cross-sectional research approach was used for this investigation.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki, 16 and the protocol was approved by the Ethics Committee of Maaruti College of Dental Sciences & Research Centre, Bangalore, India, via Ref number AECS/MDC/1484. Written informed consent to participate was obtained from all participants prior to enrollment in the study.
Study sample
A total of 1000 participants aged between 18 and 70 years were recruited, meeting the selection criteria during the recruitment period. The sample size was determined based on resource availability and participant accessibility. Subject recruitment considered the diversity of age and demographic characteristics within the accessible population, allowing for the inclusion of both younger and older individuals, which is important for the study’s objectives.
Sample technique
Systematic random sampling was used to select participants. The sampling frame included all subjects who successfully met the inclusion criteria during the study period. The sample size was not determined by a statistical formula but was instead based on resources and participant availability. Therefore, a selection interval proportional to the total accessible population was established. This method facilitated the even distribution of the selection process across the target population and reduced the risk of selection bias while maintaining the study’s operational feasibility.
Study setting
The outpatient Department of Periodontics, AECS Maaruti College of Dental Sciences and Research Centre, Bangalore.
Inclusion criteria
The research procedure included participants of both genders, aged between 18 and 70 years, the presence of at least 15 functional teeth, excluding third molars, absence of professional periodontal therapy in the last 6 months, ability to understand and sign written informed consent, willingness to undergo a complete periodontal examination, and anthropometric measurements.
Exclusion criteria
The research procedure excluded participants who were completely edentulous, were active smokers or had a history of tobacco use in the last 6 months, were pregnant or breastfeeding, had a previous diagnosis of a systemic condition (high blood pressure, diabetes mellitus, autoimmune diseases, neoplasia under active treatment), had used antibiotics, systemic anti-inflammatory drugs, or immunosuppressants in the 6 months prior to the study, had active acute or chronic systemic infections at the time of evaluation, and were unable to participate in all phases of the clinical evaluation or to provide informed consent.
Data collection methodology
The structured interview process involved completing a questionnaire to gather sociodemographic information. Anthropometric measurements included height (determined using a height scale) and weight (measured using a digital weighing scale). Waist and hip circumferences were assessed using a measuring tape. An Omron body fat monitor was used to determine body fat percentage and BMI. The following categories were defined for BMI: normal weight (BMI >18.6 and <24.9 kg/m2), overweight (BMI >25 and <30 kg/m2), and obese (BMI ⩾30 kg/m2). 17
In the assessment of periodontal health, the Plaque Index (PI) was meticulously measured for all participants using a standardized protocol. This index served as a crucial variable in our multivariate logistic regression models, helping to adjust for the impact of oral hygiene practices on the relationship between BMI and periodontal disease. The inclusion of the PI allows for a nuanced analysis of how oral hygiene mediates the effects of obesity on periodontal outcomes.
Each subject underwent a clinical periodontal examination to assess the PI, the gingival index (GI), the probing pocket depth (PPD), and the clinical attachment loss (CAL) for six selected teeth, excluding the third molars.18,19 The six teeth considered were chosen according to the protocol of Ramfjord 20 and Dowsett et al., 21 and they are: maxillary right first molar, maxillary left central incisor, maxillary left first bicuspid, mandibular left first molar, mandibular right central incisor, and mandibular right first bicuspid. Disease severity was assessed based on the percentage of periodontal sites. Calculations were performed to determine the proportion of sites within each oral cavity that met the PPD and CAL criteria. This involved dividing the total number of measured sites by those that met the specified criteria. Periodontitis was defined as the presence of four or more teeth with at least one site exhibiting a PPD of ⩾4 mm and a CAL of ⩾3 mm. 22 Finally, a sterile dental mirror and explorer were used to record the status of missing, filled, and decaying teeth. 23
Data analysis
For statistical analysis, the STATA V.15 program (Stata Corp, College Station, TX, USA) was used, considering a value of p ⩽ 0.05* as statistically significant. The normality of the data was examined using the Shapiro–Wilk test. Qualitative data were represented by absolute and relative frequency (%), while quantitative data were represented by mean ± standard deviation (SD). Analysis of variance (ANOVA) and Mann–Whitney U tests were used to compare quantitative variables. Univariate and bivariate analysis was also performed to explore the relationship between periodontitis and various indicators of obesity.
Results
Sociodemographic characteristics
An extensive analysis is presented in Figure 1, detailing the sociodemographic characteristics of the study cohort that investigated the relationship between body composition and periodontitis. The age distribution of the participants is detailed in Supplemental Tables 2 and 3. The majority of the study population (90.1%) were aged below 50 years, with significant representation across younger age groups: 103 participants (10.3%) were ⩽18 years, 401 (40.1%) were 19–25 years, 213 (21.3%) were 26–30 years, and 101 (10.1%) were 31–35 years. Participants aged above 50 accounted for 3.9% of the sample. The average age of the study participants was 22.54 ± 4.16 years. The skew toward younger age groups is reflective of the clinical setting and provides valuable insights into the early onset of obesity and periodontal issues. Marital status was evenly divided between single and married participants. Most individuals have an income of less than 2300 USD, suggesting a substantial portion from lower-income groups. Education levels were predominantly below the graduate level, with a significant proportion having educational backgrounds below high school education. Regarding oral hygiene habits, most participants (92%) brushed once a day. These sociodemographic insights provide a contextual foundation for interpreting the findings of this study, allowing the consideration of factors such as age, income, and education in the analysis of the correlation between body composition and periodontitis.

Sociodemographic characteristics.
Dental status among the study participants
Table 1 outlines the distribution of the participants based on the number of teeth affected by various dental problems, specifically decay, missing teeth, and filled teeth. The data provided a detailed snapshot of the prevalence of these issues within the study population. Most participants (58.20%) exhibited no decayed teeth (scored 0). As the number of decayed teeth increased, the percentage decreased, with 26.50% having two decayed teeth and only 0.20% having 10 decayed teeth. This finding suggests a generally low prevalence of decayed teeth in the study population. A substantial number of participants (86.40%) reported no missing teeth. The prevalence of missing teeth decreased with increasing counts, with 9.30% having 4 missing teeth and a notable proportion (80.30%) having 10 missing teeth. This indicates that most participants had a complete set of teeth, and a minor percentage experienced tooth loss. The distribution of filled teeth showed a pattern similar to that of decayed teeth, with 80.30% of the participants having no filled teeth. As the number of filled teeth increased, the percentage decreased, with a minimal representation in the categories of 8, 9, and 10 filled teeth. This finding suggests a limited occurrence of dental restorations in the study population.
Dental status among the study participants.

Overall, the results depicted a predominantly favorable oral health status, with a significant proportion of participants having no decayed, missing, or filled teeth. The data suggest that most of the study population maintained good oral health, although there was a subset with varying degrees of dental issues.
Measurements status
Supplemental Table 1 shows the three key metrics of BMI, WC, and WHR used to assess the participants’ body composition. The results revealed that 46.20% of the participants had a normal BMI, with 18.80% classified as underweight, 30.50% overweight, and 4.50% obese. Regarding WC, the majority (97.10%) exhibited a normal measurement, whereas only 2.90% had a high WC. Regarding the WHR, 33.90% had a normal ratio, whereas 66.10% had a high ratio. Notably, the prevalence of average WC suggests limited abdominal obesity. In contrast, a substantial proportion with a high WHR indicates a potential association between body fat distribution and periodontitis.
Comparison of BMI according to sociodemographic characteristics
Supplemental Table 2 outlines the findings investigating the correlation between BMI and diverse sociodemographic characteristics. Notably, a statistically significant difference in BMI was observed between the sexes, with males exhibiting a higher mean BMI than females (22.85 vs 22.12, t = 2.735, p = 0.006*). Age-related variations in BMI were evident, as indicated by a significant ANOVA result (F = 24.722, p < 0.001*), with a trend of increasing BMI as age advanced, reaching its peak in the age group above 50 years. Marital status was also associated with BMI, with single individuals having a lower mean BMI than married individuals (21.27 vs 23.88, t = −10.420, p < 0.001*). Moreover, an individual’s annual income is linked to BMI, with those earning higher incomes demonstrating a higher BMI (22.32 vs 24.35, t = −5.004, p < 0.001*). Education level significantly impacted BMI (F = 7.034, p < 0.001*), with a general trend of increasing BMI corresponding to higher education levels. Collectively, these findings underscore the multifaceted nature of the relationship between sociodemographic factors and BMI, shedding light on the potential correlations with periodontitis in the studied population.
Comparison of different parameters among samples according to BMI
Table 2 presents the findings of exploring the comparison between body composition and periodontitis. The investigation examined various oral health parameters across distinct BMI categories, classifying participants as normal weight, underweight, overweight, or obese. The results revealed statistically significant variances in PPD and CAL. Both PPD and CAL were notably higher in individuals classified as overweight or obese than in those with normal or underweight BMI, with p-values indicating statistical significance (PPD: p < 0.001*, CAL: p < 0.001*). The number of decayed teeth was significantly elevated in overweight participants (p = 0.020*), suggesting a potential association between higher BMI and increased severity of periodontal conditions. Additionally, the number of filled teeth was significantly higher in overweight individuals (p < 0.001*).
Comparison of different parameters among samples according to BMI.
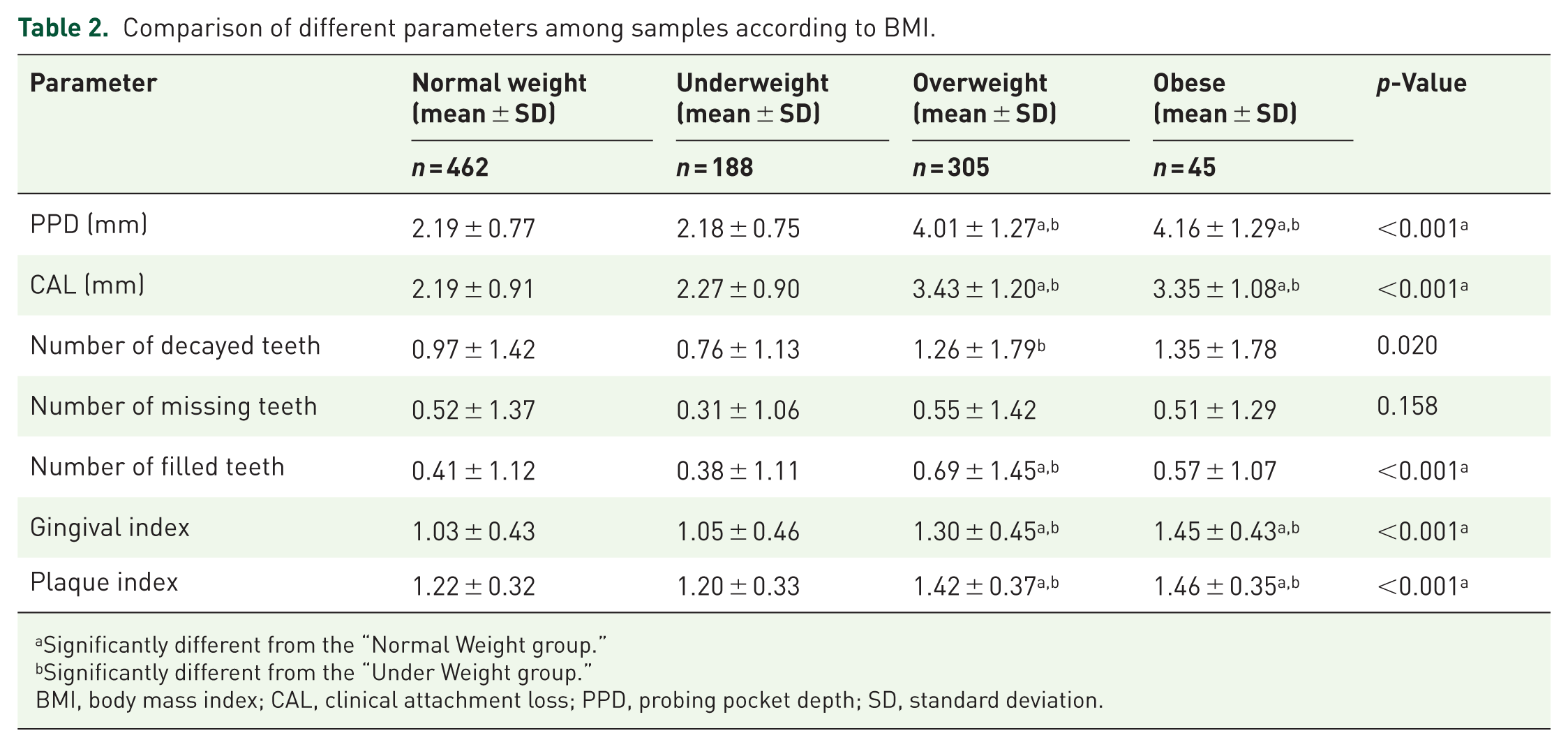
Significantly different from the “Normal Weight group.”
Significantly different from the “Under Weight group.”
BMI, body mass index; CAL, clinical attachment loss; PPD, probing pocket depth; SD, standard deviation.
GI and PI showed consistent increases with higher BMI categories (GI: p < 0.001*, PI: p < 0.001*), indicating a broader impact on oral health. Statistical analysis revealed significant disparities in the PI among the study groups. Participants with obesity and overweight conditions exhibited higher plaque scores compared to their normal-weight counterparts (p < 0.05). These findings suggest a notable association between increased plaque accumulation and higher BMI categories, potentially contributing to the elevated prevalence and severity of periodontitis observed in these groups.
Overall, these findings, supported by the mean and SD values, underscore the significance of considering body composition in understanding and addressing oral health disparities. These results suggest that individuals with a higher BMI may face an elevated risk of periodontal issues, emphasizing the need for tailored oral health interventions in populations with varying body compositions.
Comparison of WC and waist-hip ratio characteristics among samples
This research revealed significant differences between WC, WHR, and diverse dental parameters (Table 3). The Mann–Whitney test was used to compare individuals with normal and elevated values for these body composition metrics. It is particularly noteworthy that individuals with a greater WC exhibited a significant elevation in PPD (p < 0.001*) and CAL (p = 0.003*). Similarly, those with higher WHRs exhibited an elevated PPD (p = 0.022*) and CAL (p = 0.026*). Moreover, higher WC was significantly associated with an increased number of missing teeth (p < 0.001*), filled teeth (p < 0.001*), the GI (p < 0.001*), and the PI (p = 0.040*). Conversely, individuals with a higher WHR had a higher PI (p = 0.002*). These statistically supported findings underscore the connection between central adiposity and periodontal health and the importance of considering body composition in elucidating oral health disparities.
Comparison of WC and waist-hip ratio characteristics among samples.

Denotes significant difference.
CAL, clinical attachment loss; PPD, probing pocket depth; SD, standard deviation; WC, waist circumference.
Table 4 presents findings from both univariate and multivariate analyses exploring the association between periodontitis and various obesity indicators. In the univariate analysis, BMI exhibited a significant association with periodontitis, with odds ratios (OR) of 2.28 for overweight and 6.46 for obesity, both highly significant (p < 0.001*). However, in the multivariate analysis adjusted for age, P1I, and the number of missing teeth, the significance diminished for overweight (OR = 1.31, p > 0.05) and slightly reduced for obesity (OR = 3.42, p < 0.01*).
Univariate and multivariate association between periodontitis and obesity indicators.

The obesity indicator was tested separately in different multivariate logistic regression models. Adjusted for age, P1I, and the number of missing teeth. Normal weight (BMI >18.6 and <24.9 kg/m2), overweight (BMI >25 and <30 kg/m2), and (BMI ⩾30 kg/m2). High waist circumference >102 cm in males and >88 cm in females. High waist-hip ratio: >0.9 inches in males and >0.8 inches in females.
the value is statistically significant.
BMI, body mass index; CI, confidence interval; OR, odds ratio.
Similarly, WC demonstrated a significant univariate association with periodontitis (OR = 3.41, p < 0.001*), and this association remained significant in the multivariate analysis (adjusted OR = 1.84, p < 0.01*). For the WHR, the univariate analysis revealed a significant association (OR = 1.73, p < 0.01*), but in the multivariate model, after adjustments, the association lost significance (adjusted OR = 1.26, p > 0.05). Concerning the “Body Fat Percentage” category, the univariate analysis indicated a significant association (OR = 1.84, p < 0.01*), and this association persisted in the multivariate analysis with adjustments (adjusted OR = 1.76, p < 0.05*).
These results suggest that while BMI and WC maintain significant associations with periodontitis even after adjusting for confounding factors, the WHR loses significance in the multivariate model. After adjustments, the “Body Fat Percentage” category retains statistical significance, though slightly attenuated. These findings underscore the importance of considering multiple obesity indicators and adjusting for relevant covariates when examining their associations with periodontitis.
Discussion
In the present study, the findings indicate that obesity, assessed by BMI and indicators of central adiposity, is independently linked to greater severity of periodontitis, even after adjustment for key confounding factors, supporting its possible role as an important determinant of periodontal health.
The sociodemographic profile of the study population revealed a diverse group of 1000 participants with a slight male predominance and a notable concentration of individuals aged 19–30 years. The even distribution between single and married participants, coupled with a majority earning <2 lakhs, underscores socioeconomic diversity. The prevalence of education below the graduate level and a significant proportion with educational backgrounds below the 10th standard suggest potential links between lower educational attainment and the variables under investigation. Additionally, the majority reported brushing once a day (92%), highlighting a positive oral hygiene habit. These sociodemographic observations emphasize the importance of conducting a thorough analysis considering various factors, such as age, gender, socioeconomic status, education, and oral hygiene practices. This holistic approach is essential for interpreting the relationship between body composition and periodontitis, thereby enabling the development of targeted interventions tailored to specific demographic subgroups.
Previous studies have determined a positive association between periodontitis and some factors such as age, gender, occupation, and hypertension, while smoking showed a negative correlation. 24 The investigation revealed that individuals classified as overweight or obese showed elevated mean scores in both the PI and the GI compared to their counterparts with normal weight. 25 Furthermore, research concluded that there is a correlation between periodontitis and obesity as measured by BMI. 26 Collectively, these studies support the importance of considering sociodemographic factors such as age, income, education, and oral hygiene habits in analyzing the correlation between body composition and periodontitis. The findings of this study provide a positive picture of the oral health of the surveyed population. The data suggested that most participants encountered only a limited number of dental issues. The notably high percentage (58.20%) of individuals with no decayed teeth suggested a low prevalence of dental decay. As the number of decayed teeth increased, the percentage of decayed teeth decreased, indicating a diminishing trend in the prevalence of decay within the population. Additionally, a substantial number of participants (86.40%) reported having no missing teeth, with only a small percentage experiencing tooth loss, particularly in categories with higher counts of missing teeth. This indicates that the majority of participants maintained a complete set of teeth. Similarly, the distribution of filled teeth mirrors the pattern observed for decayed teeth, with 80.30% reporting no dental fillings and a decreasing percentage as the number of filled teeth increased. This finding implies a limited need for dental restorations in the study population. These findings collectively depicted a predominantly positive state of oral health, suggesting that most participants uphold good oral hygiene. However, a subset of individuals have diverse dental issues. Other studies have indicated a correlation between oral health status and obesity. 27
The normal-weight group had fewer individuals with periodontitis, whereas the obese group had a higher prevalence of severe periodontitis. In contrast to the normal-weight cohort, both the overweight and obese groups showed increased gingival crevicular fluid levels related to periodontal measures and inflammatory cytokines. Significant correlations were found between the clinical attachment level and periodontal pocket depth, as well as between BMI and WHR. 28
Although a possible correlation exists between periodontitis and obesity, as with other oral systemic diseases, some controversies remain. While some studies have reported a distinct correlation between periodontitis and obesity, others have suggested only moderate or no association between periodontitis and obesity. Unlike earlier studies, this investigation analyzed multiple obesity indicators and adjusted for confounders, providing a more nuanced understanding of the relationship between obesity and periodontal health. For instance, the study highlights the independent role of central adiposity metrics, such as WC, in exacerbating periodontitis, even after accounting for BMI. However, with few high-quality studies and variable reported findings, there is limited evidence of significant differences in clinical practice. Obesity is a risk factor for periodontal diseases. 29
This study investigated the relationship between periodontitis and body composition, utilizing BMI, WC, and WHR as key metrics. The results showed that 46.20% had a normal BMI, 18.80% were underweight, 30.50% were overweight, and 4.50% were obese. Regarding WC, 97.10% had a normal measurement, whereas 2.90% had a high measurement. For the WHR, 33.90% had a normal ratio, whereas 66.10% had a high ratio. Notably, individuals with BMI >25 kg/m² were three times more likely to have periodontitis than those with normal weight, suggesting a potential link between body fat distribution, especially a high WHR, and periodontal health. These findings are consistent with those of a study conducted on Japanese adults by Ekuni et al. 30 Numerous studies have consistently demonstrated a direct correlation between BMI, being overweight or obese, and the prevalence, extent, and severity of periodontitis. Global literature unequivocally establishes a link between periodontal disease and obesity. The predominant research approach in this regard is cross-sectional observational studies. Recent studies have suggested that factors such as excess weight, obesity, weight gain, and larger WC may contribute to the development or worsening of periodontitis. 31
Findings from a comprehensive analysis investigating the correlation between BMI and periodontitis consider diverse sociodemographic characteristics. Notably, a statistically significant difference in BMI was observed between the sexes, with males exhibiting a higher mean BMI than females (22.85 vs 22.12, t = 2.735, p = 0.006*). Age-related variations in BMI were evident, as indicated by a significant ANOVA result (F = 24.722, p < 0.001*), with a trend of increasing BMI as age advanced, reaching its peak in the age group above 50 years. Marital status was also associated with BMI, with single individuals having a lower mean BMI than married individuals (21.27 vs 23.88, t = −10.420, p < 0.001*). Moreover, an individual’s annual income is linked to BMI, with those earning higher incomes demonstrating a higher BMI (22.32 vs 24.35, t = −5.004, p < 0.001*). Education level significantly impacted BMI (F = 7.034, p < 0.001*), with a general trend of increasing BMI corresponding to higher education levels. Collectively, these findings underscore the multifaceted nature of the relationship between sociodemographic factors and BMI, shedding light on the potential correlations with periodontitis in the studied population. In Shandong, China, a recent cross-sectional study focused on adults to investigate the relationship between BMI and health-related quality of life. The results revealed sex-based variations in this correlation, emphasizing the significance of considering sex-specific factors when examining the influence of BMI on health-related quality of life. 32 In Indonesia, a cross-sectional study yielded congruent results highlighting a noteworthy positive association between obesity and periodontitis. The investigation further identified various risk factors: age, sex, profession, and hypertension. Notably, this study revealed a counterintuitive inverse correlation between smoking status and periodontitis. 24 In a study carried out recently in the United States, it was shown that obesity is associated with an increased risk of periodontal disease. The OR for this association was 1.35, with a 95% confidence range ranging from 1.05 to 1.75. 33 According to the findings of a study conducted in the United States on women who were either living with HIV or at risk for the virus, there was no significant correlation between BMI and periodontitis. Even when other criteria, such as age, race, and socioeconomic position, were considered, this lack of a link remained. 34
The results also provide insights into the correlation between body composition and periodontitis, examining oral health parameters across diverse BMI categories. Participants were categorized as normal weight, underweight, overweight, or obese. Significant differences were observed in PPD and CAL, with both metrics being significantly higher in individuals classified as overweight or obese than in those with normal or underweight BMI (PPD: p < 0.001*, CAL: p < 0.001*). Overweight participants exhibited a notably increased number of decayed teeth (p = 0.020*), suggesting a potential link between a higher BMI and heightened severity of periodontal conditions. Moreover, the number of filled teeth significantly increased in overweight individuals (p < 0.001*). Higher BMI categories were consistently associated with increased GI and PI values (GI: p < 0.001*; PI: p < 0.001*), indicating a more widespread impact on oral health. Overall, these findings, supported by the mean and SD values, underscore the significance of considering body composition to understand and address oral health disparities. These results suggest that individuals with a higher BMI may face an elevated risk of periodontal issues, emphasizing the need for tailored oral health interventions in populations with varying body composition. A cross-sectional study found that the gingival bleeding index and BMI were positively correlated. 35 Regular BMI assessment is recommended for patients to assess their susceptibility to periodontal disease. A thorough analysis of 15 observational studies highlighted a robust association between obesity and periodontitis. This underscores the importance of personalized treatment approaches based on BMI evaluations to effectively address periodontal health risks. 36 According to another study conducted in India, overweight individuals were found to be at a considerable risk of developing periodontitis. According to the findings of this study, there was a significant association between being overweight and the development of periodontal disease. This highlights the need to maintain regular oral hygiene habits in obese people. 32
The relationship between periodontitis and obesity is bidirectional, driven by systemic inflammation. Periodontal tissues release cytokines and chemokines, such as IL-6 and TNF-α, into the bloodstream, contributing to metabolic dysregulation and insulin resistance. This systemic inflammation can exacerbate obesity by promoting lipid dysregulation and impairing glucose metabolism. Conversely, obesity-associated chronic inflammation, mediated by adipokines, increases the severity of periodontal tissue destruction by enhancing local inflammatory responses. These findings underscore the need to consider both conditions together in clinical and public health strategies.
Certain research has highlighted that periodontitis, being a chronic inflammatory condition, promotes an environment of oxidative stress determined by an increase in the synthesis of reactive oxygen species and a reduction in systemic and local antioxidant capacity.37–39 This alteration of the redox state both contributes to periodontal tissue injury through lipid peroxidation, protein oxidation, and DNA compromise, and can also exacerbate the systemic inflammatory response.37,39 The prolonged persistence of the pro-oxidant-inflammatory state is associated with the deterioration of metabolic and cardiovascular conditions, highlighting the clinical importance of considering oxidative stress as a fundamental element in the interrelationship between periodontal health and the systemic state. 38 Our results, in line with existing evidence, support the hypothesis that obesity and central adiposity, by amplifying systemic inflammation, can aggravate this pathogenic mechanism.
The study underscores the importance of considering multiple obesity indicators and adjusting for relevant covariates to comprehensively understand their associations with periodontitis. Similarly, numerous studies have also reported an association between obesity and periodontitis, and the findings of the current study are consistent with these studies. A cross-sectional study conducted in 2019 found that BMI, WC, waist-hip ratio, and body fat percentage were significantly associated with periodontitis. 8 Similarly, a systematic review and meta-analysis published in 2022 reported a positive association between obesity and periodontitis. 33 Another systematic review published in 2018 found that obesity indicators such as BMI, WC, waist-hip ratio, and body fat percentage were significantly associated with measures of periodontitis. 40 A study published in 2023 found that BMI and WC were significantly associated with periodontitis in US adults. 41 Another study published in 2021 found a positive association between obesity indicators and chronic periodontitis. 42 Overall, the current study’s findings are consistent with previous studies that reported an association between obesity and periodontitis. The results underscore the importance of considering multiple obesity indicators and adjusting for relevant covariates when examining their associations with periodontitis.
In summary, this study underscores a significant association between obesity and the heightened occurrence of periodontal disease, coupled with an escalation in both the severity and extent of the ailment. These findings strongly suggest that adopting a well-rounded dietary approach, sustaining a healthy body weight, and actively participating in wholesome physical activities can play a pivotal role in mitigating the severity of periodontitis. This study implies that lifestyle modifications encompassing balanced nutrition and regular exercise could effectively reduce the frequency of periodontal disease and ameliorate its overall impact. This evidence highlights the interplay between lifestyle choices and oral health, emphasizing the potential for positive outcomes through holistic health practices. Therefore, maintaining normal body weight, incorporating nutritious dietary habits, and engaging in regular physical exercise have emerged as integral components in efforts to curtail the severity and breadth of periodontal disease. This nuanced understanding opens new avenues for comprehensive health interventions beyond traditional dental care, promoting a holistic approach to well-being that addresses systemic and oral health concerns.43–45
This study highlights significant findings linking body composition and periodontal health, emphasizing the importance of integrated care. Most participants exhibited favorable oral health; however, individuals with high BMI or central adiposity (e.g., elevated WHR) were at increased risk of chronic and recurring periodontal disease. Significant disparities in periodontal indicators such as PPD, CAL, and dental issues like missing and decayed teeth were observed across BMI groups and sociodemographic factors, including age, sex, marital status, income, and education. These results underscore the need for tailored oral health treatments based on body composition.
Furthermore, the bidirectional relationship between periodontitis and obesity highlights the importance of integrated care approaches. Collaborative efforts between dental and medical professionals can address shared inflammatory pathways, improving systemic and oral health outcomes. Designing interventions focused on body composition, particularly central adiposity, is essential to reduce the elevated risk of periodontal disease in affected populations. This research calls for holistic strategies to address oral health disparities across diverse communities.
Integrated health education should emphasize the link between body composition, especially BMI and central adiposity, and oral health. Tailored interventions, routine check-ups, and early detection for individuals with higher BMI can help prevent periodontal disease progression. Affordable oral health services for low-income groups and the integration of oral health into broader public health policies are essential. Further research is needed to explore the causal relationship between body composition and periodontitis, ensuring effective strategies to address disparities and improve overall health outcomes.
The findings highlight the PI as a significant mediator in the relationship between obesity and periodontitis. Higher plaque levels in overweight and obese individuals may reflect poorer oral hygiene practices, which could exacerbate the inflammatory pathways involved in periodontitis. These insights emphasize the need for targeted oral hygiene interventions as part of comprehensive obesity management strategies to mitigate periodontal disease risk.
This study faces several limitations that must be considered. First, the study participants comprise a high proportion of young adults, with the majority of patients under 50 years of age. This distribution particularly limits the generalization of the results to older populations, as periodontitis and obesity manifest differently in those age groups. Second, the cross-sectional design restricts the ability to establish causal relationships between the analyzed variables, limiting interpretation to links only. Third, although strict inclusion and exclusion criteria were established to reduce heterogeneity, this may generate selection bias, restricting the application of the findings to other populations with different sociodemographic or systemic characteristics. Likewise, no prior sample size calculation was conducted; the inclusion of participants was based on the availability of eligible individuals during the data collection period, which may influence the representativeness of the sample and potentially limit the generalizability of the findings to other populations. Fourth, the periodontal evaluation was performed considering the clinical parameters of only six teeth, following the Ramfjord protocol, and not through a full-mouth examination. Although this method has been validated and widely used in various epidemiological studies due to its efficiency and feasibility in large samples, we must keep in mind that it may underestimate or overestimate the prevalence and severity of periodontal disease compared to a complete analysis. This methodological strategy was established to optimize resources and recording time in a large sample; however, we recognize that obtaining full-mouth clinical parameters provides a more comprehensive view of periodontal status. Fifth, despite adjustment for key confounders, other variables, such as genetic predisposition or dietary habits, that could have influenced the findings were not considered. Additionally, systemic biomarkers of inflammation or oxidative stress were not integrated, limiting a deeper understanding of the potential pathophysiological mechanisms linking obesity with periodontitis. Finally, the lack of longitudinal follow-up limits the ability to analyze temporal changes and determine the directionality of the observed associations. Therefore, future multicenter studies are recommended, considering more diverse cohorts, broader age ranges, and the identification of systemic biomarkers, to validate these findings and ensure their generalizability.
Conclusion
The present study shows that obesity, assessed by BMI and indicators of central adiposity, is significantly associated with greater severity of periodontitis, even after adjusting for key confounding factors. However, due to the study design and the particularities of the population evaluated, these results should be interpreted with caution. The findings support the possible involvement of excess body fat as a factor influencing periodontal health, even though causal relationships cannot be determined. Longitudinal and multicenter studies involving diverse populations and integrating biological markers are essential to confirm these findings and provide a deeper understanding of the underlying mechanisms. Despite these limitations, our findings support the possibility that considering obesity indicators in periodontal risk assessment could promote more comprehensive preventive and therapeutic approaches.
Supplemental Material
sj-doc-1-taj-10.1177_20406223251383319 – Supplemental material for The impact of body mass index on periodontitis: a cross-sectional study
Supplemental material, sj-doc-1-taj-10.1177_20406223251383319 for The impact of body mass index on periodontitis: a cross-sectional study by Soumya Vishwanath, Vishwanath Gurumurthy, Ravinder S. Saini, Mario Alberto Alarcón-Sánchez, Sarah Monserrat Lomelí-Martínez, Artak Heboyan and Armen A. Muradyan in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-2-taj-10.1177_20406223251383319 – Supplemental material for The impact of body mass index on periodontitis: a cross-sectional study
Supplemental material, sj-docx-2-taj-10.1177_20406223251383319 for The impact of body mass index on periodontitis: a cross-sectional study by Soumya Vishwanath, Vishwanath Gurumurthy, Ravinder S. Saini, Mario Alberto Alarcón-Sánchez, Sarah Monserrat Lomelí-Martínez, Artak Heboyan and Armen A. Muradyan in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-3-taj-10.1177_20406223251383319 – Supplemental material for The impact of body mass index on periodontitis: a cross-sectional study
Supplemental material, sj-docx-3-taj-10.1177_20406223251383319 for The impact of body mass index on periodontitis: a cross-sectional study by Soumya Vishwanath, Vishwanath Gurumurthy, Ravinder S. Saini, Mario Alberto Alarcón-Sánchez, Sarah Monserrat Lomelí-Martínez, Artak Heboyan and Armen A. Muradyan in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-4-taj-10.1177_20406223251383319 – Supplemental material for The impact of body mass index on periodontitis: a cross-sectional study
Supplemental material, sj-docx-4-taj-10.1177_20406223251383319 for The impact of body mass index on periodontitis: a cross-sectional study by Soumya Vishwanath, Vishwanath Gurumurthy, Ravinder S. Saini, Mario Alberto Alarcón-Sánchez, Sarah Monserrat Lomelí-Martínez, Artak Heboyan and Armen A. Muradyan in Therapeutic Advances in Chronic Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.