
Abstract
Background:
Metabolic associated fatty liver disease (MAFLD) stands as the leading cause of chronic liver disease globally. Notably, individuals with metabolic risk factors, such as diabetes and obesity, exhibit a staggering prevalence of MAFLD, with estimates reaching up to 70%. However, despite its widespread occurrence, there’s a noticeable gap in understanding and awareness about MAFLD among these high-risk groups.
Objectives:
The main objective of this study was to assess the awareness and prevalence of MAFLD among diabetic patients who regularly receive secondary care focusing particularly on how multiethnic backgrounds and associated lifestyle preferences influence these health outcomes.
Design:
Cross-sectional study.
Methods:
Patients with type 2 diabetes (T2D) who regularly attend Lambeth Diabetes Intermediate Care Team clinics were invited to undergo MAFLD screening using FibroScan. Those who agreed to participate were provided with structured questionnaires on diet, physical activity, and MAFLD knowledge by a hepatologist. For each participant, anthropometric data, medical history, liver stiffness measurement, and controlled attenuation parameter (CAP) were documented. Steatosis was identified with a CAP value of ⩾275 dB/m, and advanced fibrosis was flagged at values of ⩾8 kPa.
Results:
The FibroScan data was valid in 96.4% (215), 53.5% (115/215) had steatosis and 26.2% (58/215) had liver fibrosis in this multiethnic high-risk group. Awareness of MAFLD was notably low at 30.9%. Alarmingly, 69% of patients diagnosed with liver fibrosis were unfamiliar with the condition. Additionally, understanding of MAFLD showed variation among different ethnic groups with highest levels were demonstrated in the Caucasian/White population (46%). Majority (96%) of these subjects were receiving specific lifestyle advice from healthcare professionals due to metabolic conditions and comorbidities. However, most patients preferred diets that were rich in carbohydrates (65.8%) and only 43% subjects performed moderate exercise daily highlighting lack of understanding regarding MAFLD and lifestyle management.
Conclusion:
There’s a pressing need for increased awareness of MAFLD, especially in multiethnic high-risk groups. Additionally, the development of cost-effective strategies to stratify risk is essential to address this growing health concern.
Plain language summary
Metabolic associated fatty liver disease (MAFLD) or more commonly fatty liver disease is the leading cause of chronic liver disease globally, particularly affecting individuals with diabetes and obesity. This study focuses on patients with type 2 diabetes in South London who regularly receive secondary care, examining the awareness and prevalence of MAFLD, especially across different ethnic groups. Participants, all with Type 2 Diabetes, attended clinics run by the Diabetes Intermediate Care Team where they underwent MAFLD screening using Fibroscan. This tool measures liver stiffness (fibrosis) and fat levels. In addition to the scans, participants answered questions about their diet, physical activity, and knowledge of MAFLD. Key findings include a low overall awareness of MAFLD, with only about 30.9% of patients aware of the disease. Among those diagnosed with liver fibrosis, 69% were unfamiliar with the condition, indicating a significant awareness gap. Interestingly, awareness levels varied among ethnic groups, with Caucasian/white patients showing the highest awareness at 46%. Despite receiving lifestyle advice from health professionals, many participants preferred carbohydrate-rich diets and only a minority engaged in daily moderate exercise. This behaviour highlights a general lack of understanding about MAFLD and its management through lifestyle changes. The study concludes that there is a critical need to raise awareness about MAFLD among high-risk, multi-ethnic groups in South London. It also highlights the necessity for developing cost-effective strategies to better identify and manage this growing health concern.
Keywords
Introduction
According to British Liver trust, every day over 40 people die from liver disease in the UK. 1 Liver disease is the third leading cause of premature death in the UK 2 and 90% of liver disease is preventable. 3 About three quarters of people are currently diagnosed at a late stage when it is too late for lifestyle changes or intervention. Outcomes can vary greatly depending on income and location. 1
The nomenclature for nonalcoholic fatty liver disease has been recently updated to metabolic associated fatty liver disease (MAFLD) which is defined as having excessive fat in the liver and association with metabolic disorders such as such as obesity, type 2 diabetes (T2D), insulin resistance, and hyperlipidemia. 4 Numerous studies have highlighted the critical role of systemic metabolic dysregulation in the development of MAFLD and have proposed targeted metabolic interventions as effective treatment strategies.5–7 Additional pathways, not solely linked to metabolic syndrome, also play significant roles in the development of fatty liver disease. 8 Moreover, the distribution of body fat, particularly obesity-associated visceral adiposity and conditions such as lipodystrophy, are critical determinants in the onset and progression of fatty liver disease. 9 MAFLD encompasses a spectrum of disorders that range from steatosis through to steatohepatitis, cirrhosis, and hepatocellular carcinoma (HCC). 10 It is estimated that the number of MAFLD-related deaths will increase 178% by the year 2030, 11 but there is a lack of awareness among high-risk patients, primary care physicians, and other healthcare workers. 12
A recent international survey revealed major deficiencies in our MAFLD referral pathways, insufficient screening of comorbidities, and limited availability of nonpharmacological interventions. In addition, monitoring practices were found to be mal-aligned with current guidelines. 13 Given the lack of approved MAFLD treatments, our focus should be early screening of high-risk populations, lifestyle modification as a preventative strategy, and a broader focus on health optimization. It is critical to screen patients who are already in our healthcare system with other preexisting conditions such as metabolic syndrome to achieve an early diagnosis of MAFLD.
Urban areas like London, with a diverse ethnic makeup, present a unique challenge in public health management, as certain ethnic groups may have a predisposition to metabolic disorders and MAFLD. The diabetes population in London, like in many urbanized areas, comprises individuals from a myriad of ethnic backgrounds. Notably, several studies have indicated that people of South Asian, African, and Hispanic descent are at an elevated risk of developing type 2 diabetes mellitus (T2DM) and associated complications. 14 Ethnic polarity, or the variance in disease susceptibility across different ethnicities, coupled with a lack of awareness and understanding of these health disparities, exacerbates the risk of MAFLD in these populations. The disparities may be attributed to a combination of genetic factors, lifestyle choices, cultural dietary practices, and access to health information and care. 15
At King’s College Hospital, we care for some of the most deprived communities in the country and there is significant ethnic diversity across our catchment area. For example, the proportion of patients who are classified as black and ethnic minority ranges from 19% in Bromley to over 40% in Lambeth. The aim of this study was to evaluate the awareness of MAFLD in diabetic population who regularly attend to secondary care, as well as to evaluate the prevalence of steatosis and advanced fibrosis. The study also took into account factors such as multiethnicities and related lifestyle preferences. Addressing the challenge of MAFLD in the high-risk diabetes population necessitates a comprehensive understanding of ethnic disparities and proactive measures to raise awareness. Only through such informed strategies can we hope to curtail the alarming rise of MAFLD among most vulnerable populations.
Methods
The project was carried out in Akerman Health Centre, which is part of Lambeth Diabetes Intermediate Care team between October 2021 and April 2023. Patients with T2D, who were under regular follow up at the Lambeth Diabetes Intermediate Care Team clinics, were invited to participate in a MAFLD awareness-screening program. The cross-sectional study included males and nonpregnant, nonlactating females aged 18–80 years with a body mass index (BMI) greater than 18 kg/m2 who were willing and able to comply with the study requirements. Exclusion criteria encompass any condition deemed by investigators as a risk to participants or study integrity, severe psychiatric disorders impairing consent, illiterate individuals to ensure that all participants could fully understand through their own reading, and comprehension the lifestyle questionnaires and specific contraindications to FibroScan such as severe obesity that hinders device application, nonfasting state, the presence of electronic medical implants, recent surgeries in the assessment area, or an inability to lie flat during the procedure. These guidelines are designed to ensure participant safety and the reliability of study results. The main reasons cited by patients for declining to participate included time constraints and not having fasted prior to their appointment. Verbal consent was taken by the patients due to the nonintrusive nature of the study that involved assessing existing conditions without introducing new interventions, thereby posing minimal risk to participants. This method was also chosen for its practicality and efficiency, ensuring inclusivity for participants of diverse backgrounds and literacy levels, and facilitating a quicker consent process in a busy clinical environment, thus minimizing disruptions to routine care. Assessment was carried out using transient elastography (FibroScan- Echosens) on verbal consent and a total of n = 223 patients participated in the service development project. This project was part of a service evaluation and so a UK NHS Research Ethics Committee review was not required. We guaranteed that the data was anonymized for the statistical analysis. Despite the classification of our project as a service evaluation, we took significant measures to ensure the ethical handling of patient data and safeguard the interests and safety of the participants involved. The sample size was determined based on the practical considerations of the service capacity and the availability of participants during the pilot phase. This approach is common in service development studies where the focus is on process optimization and preliminary data collection to inform future larger-scale research. As part of the standard care at the diabetes clinic, all patients routinely receive personalized advice on nutrition and exercise delivered by qualified professionals, including diabetic nurses and nutritionists. The subjects understanding of MAFLD and lifestyle preferences were assessed using questionnaires (Supplemental Appendix A). We developed a new questionnaire specifically tailored to our research objectives, which, due to its novel approach, was not pretested in the traditional manner before being implemented. The development of the questionnaire involved a rigorous process, including a comprehensive review of relevant literature and consultation with experts in the field of lifestyle medicine, to ensure its content validity. Anthropometric measures such as height, weight, BMI, medical history, liver stiffness measurements (LSM), and controlled attenuation parameter (CAP) were recorded for each patient. Patients included in the study had been fasting for at least 3 hours. For the FibroScan, a certified personnel conducted a minimum of 10 valid readings per patient, and measurements were accepted only if the interquartile range (IQR) was less than 30%, in accordance with established guidelines. The presence of steatosis was defined as a CAP ⩾275 dB/m, mild fibrosis ⩾7–7.9 kPa, and advanced fibrosis ⩾8 kPa. The EASL Clinical Practice Guidelines on noninvasive tests for evaluation of liver disease 2021 recommends referral of subjects with >8 kPa as of intermediate high-risk and require further evaluation. 16 Subjects identified with advanced fibrosis based on the FibroScan were linked with tertiary care and an appointment was booked within 10 days at the liver outpatients Liver-NASH clinic at King’s College Hospital for further investigations. Patient with confirmed advanced fibrosis were enrolled into a liver cancer surveillance program.
Statistical analysis
Statistical analysis was done using IBM Statistical Package for Social Sciences software package version 26.0 (IBM, Armonk, NY, USA). Categorical (qualitative) data were described using numbers and percentages. Quantitative data were described using median and IQR for nonparametric data and mean ± standard deviation for parametric data after testing normality using Kolmogorov–Smirnov test. The used tests were Chi-square test, Likelihood ratio, and linear by linear association.
Results
A total of 223 patients participated in the service development project.
Baseline characteristics
The median participant age was 61 years (IQR of 12) and there was a similar proportion of males (50.7%) and females (49.3%). Our cohort was ethnically diverse, but there was a higher proportion of Black Africans/Caribbean (57%) followed by Caucasian/White (18.4%), Mediterranean (11.2%), Latin/Hispanic (5.8%), Asian (4.9%), and Middle East (2.7%).
Table 1 shows the baseline characteristics of subjects who participated in this study.
Baseline characteristics of the type 2 diabetes study cohort.
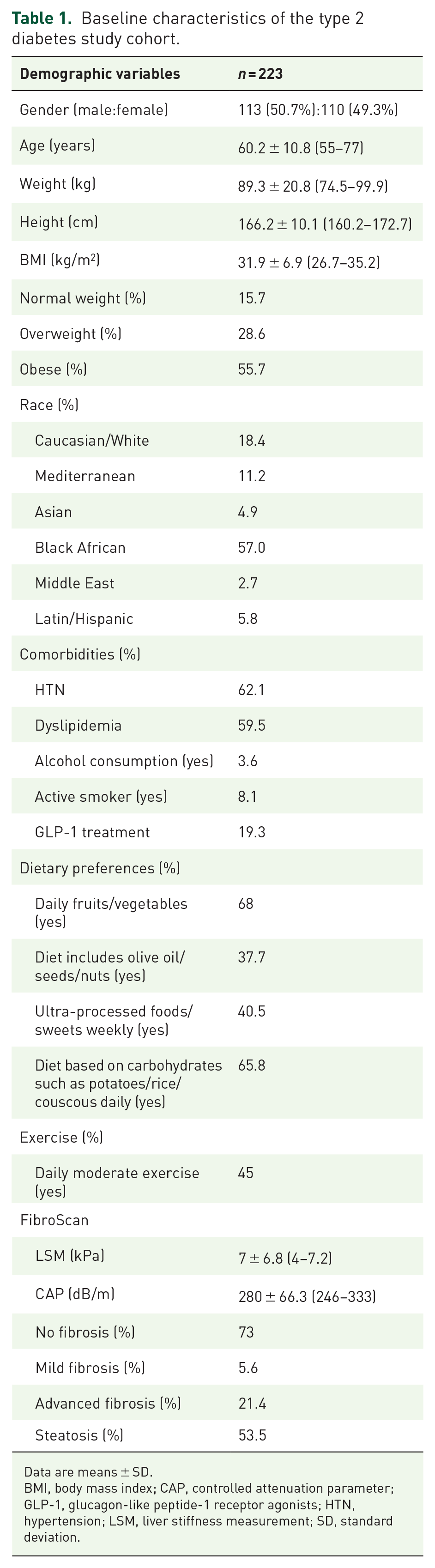
Data are means ± SD.
BMI, body mass index; CAP, controlled attenuation parameter; GLP-1, glucagon-like peptide-1 receptor agonists; HTN, hypertension; LSM, liver stiffness measurement; SD, standard deviation.
MAFLD awareness
Awareness of MAFLD was low (30.9%) and the majority of patients with liver fibrosis (69%) had never heard of this condition. Understanding varied between ethnic groups, and the highest levels were demonstrated in the Caucasian/White population (of whom 41.5% within ethnicity were aware of MAFLD). This was followed by Black African/Caribbean (32.5%), Latin/Hispanic (23%), Mediterranean (20%), Asian (18%), and Middle East (16.7%).
Surprisingly there was no statistical differences in the MAFLD awareness according to BMI, presence of other comorbidities (hypertension, dyslipidemia), presence of steatosis, and presence of advanced fibrosis (Table 2).
Demographic and clinical characteristics in our cohort divided by awareness of MAFLD.

BMI, body mass index; CAP, controlled attenuation parameter; IQR, interquartile range; LSM, liver stiffness measurement; MAFLD, metabolic associated fatty liver disease; NAFLD, non-alcoholic fatty liver disease; ns, not significant.
Overall, the average BMI was 32 kg/m2 (26.7–35.2) but only 48% of patients considered themselves to be ‘overweight’.
Lifestyle preferences
According to our structured questionnaires, most patients preferred diets that were rich in carbohydrates (65.8%), including ultra-processed foods/sweets (40.5%). Daily fruits/vegetables were present in the diet of 68% subjects but healthy foods such as olive oil/seeds/nuts were taken only in 37.7%.
Intake of fruit and vegetables was highest in subjects from the Middle East (83.3%), followed by the Mediterranean (80%). Lowest intake was seen among Caucasians (63.4%) and Asians (63.6%). Foods such as nuts/olive oil were also taken more frequently by the Latin/Hispanic population (61.5%), followed by those originating from the Mediterranean (56%), Middle East (50%), and African groups (31%).
There was also variation in the consumption of highly processed food; White/Caucasians had diets containing the most processed food (46.3%), followed by Black African/Caribbean (45.2%), Asian (36.4), Middle East (33.3%), Latin/Hispanic (23.1%), and Mediterranean (20%).
Most subjects preferred high carbohydrate diet with subjects from Middle East leading with (83.3%), followed by Asians (81.8%), Mediterranean (72%), Latin/Hispanic (69.2%), Black African (62.9%), and White/Caucasians (62.5%).
Only 43% subjects performed moderate exercise daily, despite the majority (96%) receiving specific lifestyle advice from healthcare professionals. Subjects of Black African/Caribbean ethnicity performed the most exercise (50%) followed by Caucasians (46%) and those from the Middle East (33%). A total of 99% of participants were strongly supportive of a multidisciplinary approach and lifestyle guidance in clinics.
The GLP-1 analogs were already being prescribed to 50% in the group with mild fibrosis and 32.6% in the subjects with high fibrosis. The patients with steatosis 27.8% were given GLP-1 analogs.
Comorbidities
In study subjects diagnosed with T2D, only 15.7% had normal weight, 28.6% were overweight, and 55.7% were obese. The other comorbidities in this group included hypertension 62% and dyslipidemia 59.5%. Within the mild fibrosis group 66.7% had hypertension and within the advanced fibrosis group 59.5% had hypertension. Within the steatosis group 66.4% had hypertension.
Within the mild fibrosis group, 33.3% had dyslipidemia, and within the advanced fibrosis group, 69% had dyslipidemia. Within the steatosis group, 64.5% had dyslipidemia.
Only 3.6% were drinking alcohol (above the recommended weekly allowance) and 8% were active smokers. Among the different ethnicities, White/Caucasians were leading as active smokers (14.6%) and least were Middle East and Latins regarding smoking.
MAFLD distribution and severity based on racial diversity
Based on FibroScan results, the prevalence of MAFLD in study subjects with T2D (n = 219) was 63% (n = 138). LSM and CAP data showed that 53.5% had fatty liver disease and 27% had liver fibrosis. The study further determined the prevalence of steatosis, mild fibrosis, and advanced fibrosis in different ethnic groups.
Steatosis
It showed that prevalence of steatosis was 66.7% among Whites (overall prevalence in steatosis population as 22.6%), 56.5% among Mediterranean (overall prevalence in steatosis population as 11.3%), 54.5% among Asian (overall prevalence in steatosis population as 5.2%), 43.1% among Black African/Caribbean (overall prevalence in steatosis population as 46.1%), 100% among Middle East (overall prevalence in steatosis population as 5.2%), and 84.6% among Latin/Hispanic (overall prevalence in steatosis population as 9.6%). The Pearson Chi-square significance was 0.02 (Figures 1 and 2).

Pie chart showing different ethnicities presenting with steatosis in the study. Yellow as Black African/Caribbean (overall prevalence in steatosis population as 46.1%), dark blue as Caucasians/Whites (overall prevalence in steatosis population as 22.6%), Orange as Mediterranean (overall prevalence in steatosis population as 11.3%), Green as Latin/Hispanic (overall prevalence in steatosis population as 9.6%), light blue as Middle East (overall prevalence in steatosis population as 5.2%), and gray as Asian (overall prevalence in steatosis population as 5.2%).
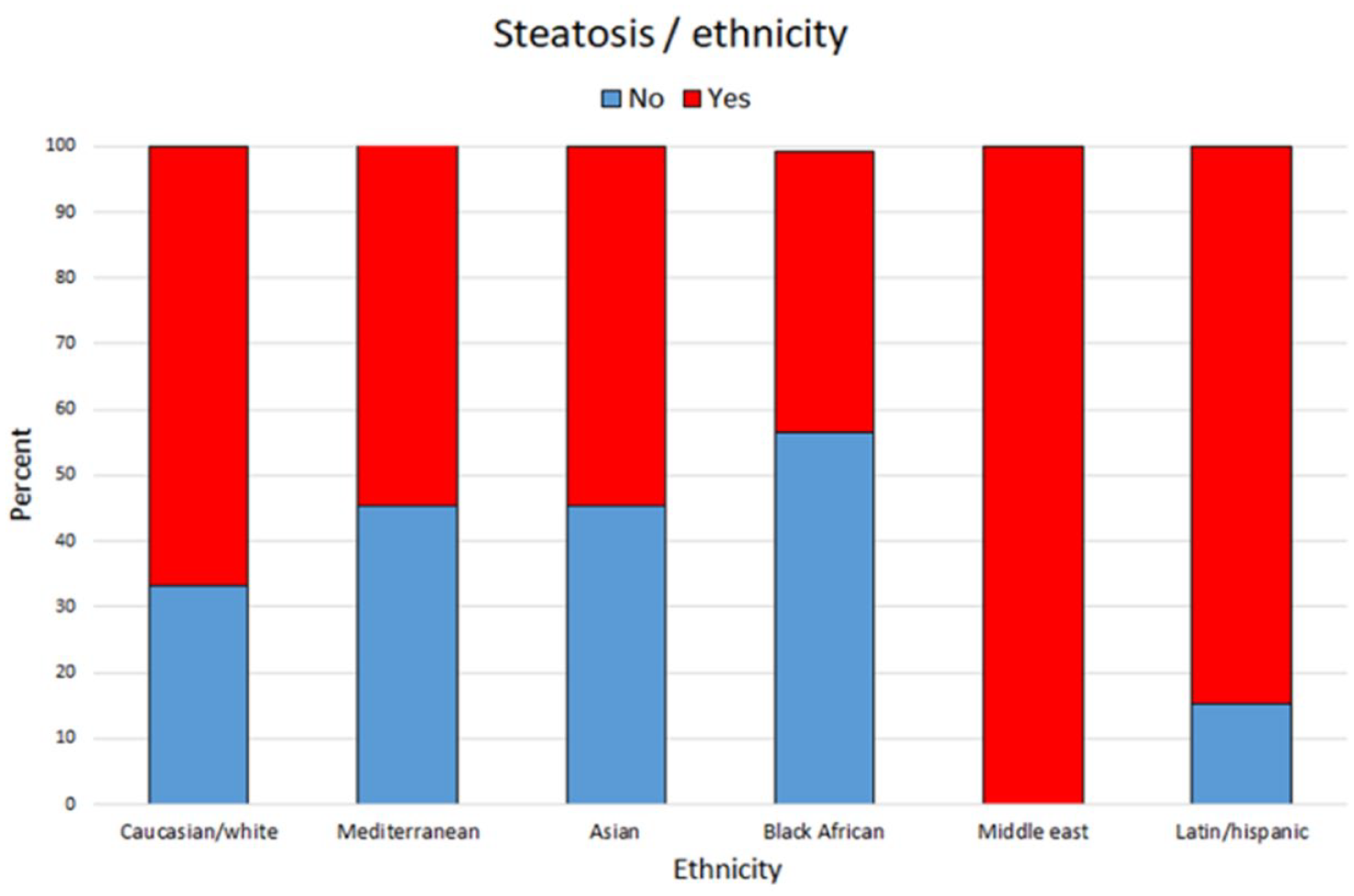
The bar chart shows prevalence of steatosis within each ethnicity. It was 66.7% among Whites, 56.5% among Mediterranean, 54.5% among Asian, 43.1% among Black African/Caribbean, 100% among Middle East, and 84.6% among Latin/Hispanic.
Unsurprisingly those with normal BMI and self-reported moderate/high exercise activity had the lower proportion of steatosis (Table 3). In contrast, the majority of T2D patients with obesity had steatosis. Their median of BMI was 33 (IQR 29–38).
Clinical characteristics in our cohort divided by the presence of steatosis.
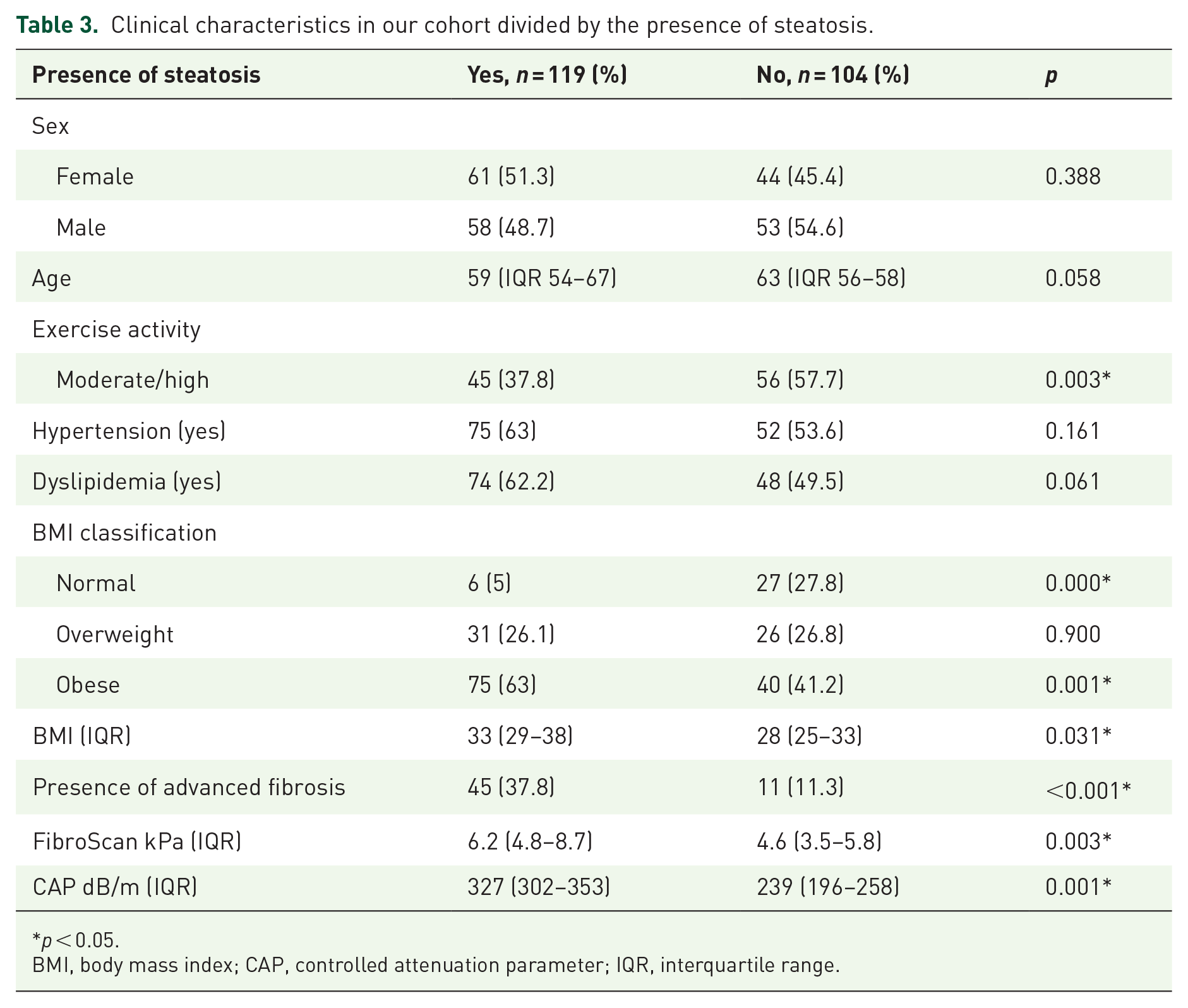
p < 0.05.
BMI, body mass index; CAP, controlled attenuation parameter; IQR, interquartile range.
Additionally, advanced fibrosis was higher in those with steatosis in comparison with those without steatosis (37.8% versus 11.3%, p < 0.001) (Table 3).
Fibrosis
The prevalence of mild fibrosis was 2.6% among Whites (overall prevalence in mild fibrosis population as 8.3%), 4.5% among Mediterranean (overall prevalence in mild fibrosis population as 8.3%), 27.3% among Asian (overall prevalence in mild fibrosis population as 25%), 5.6% among Black African/Caribbean (overall prevalence in mild fibrosis population as 58.3%), and none among Latin/Hispanic (Figure 3).

Percentage of ethnicities with liver fibrosis in the study. The prevalence of mild fibrosis was 2.6% among Whites, 4.5% among Mediterranean, 27.3% among Asian, 5.6% among Black African/Caribbean, and none among Latin/Hispanic. The prevalence of advanced fibrosis was 28.2% among Whites, 45.5% among Mediterranean, 36.4% among Asian, 12.1% among Black African/Caribbean, 50% among Middle East, and 23.1% among Latin/Hispanic.
The prevalence of advanced fibrosis was 28.2% among Whites (overall prevalence in advanced fibrosis population as 23.9%), 45.5% among Mediterranean (overall prevalence in advanced fibrosis population as 21.7%), 36.4% among Asian (overall prevalence in advanced fibrosis population as 8.7%), 12.1% among Black African/Caribbean (overall prevalence in advanced fibrosis population as 32.6%), 50% among Middle East (overall prevalence in advanced fibrosis population as 6.5%), and 23.1% among Latin/Hispanic (overall prevalence in advanced fibrosis population as 6.5%). The Pearson Chi-square significance was 0.00 (Figure 3).
Discussion
Our results suggest the lack of awareness of MAFLD epidemic in type 2 diabetic patients who are regularly follow up in secondary care. Importantly, despite having a BMI above the normal range, the majority of these patients did not perceive themselves as overweight or obese.
In UK, there has been a rise in the prevalence of diabetes, especially among ethnic minority groups and low-income households. 17 The current study was performed over a period of 18 months at the Lambeth Diabetes Centre to assess the prevalence of MAFLD, burden of advanced fibrosis, and general awareness of this condition among the diabetic population. A report published by Lambeth council found that neighborhoods experiencing greater levels of deprivation have a higher proportion of people diagnosed with multiple long-term conditions. More than one in five people in the most deprived places in Lambeth live with multiple long-term conditions, compared to only 1 in 10 in the least deprived neighborhoods. 18 According to the state of Borough 2022 health report, life expectancy is low in Lambeth compared to the rest of London, and the rate for people dying from liver disease is the second highest in London. 19
It has also been shown that there is a strong relationship between MAFLD and deprivation. The prevalence of MAFLD is higher in socially deprived communities due to the commonality of obesity and diabetes. 20 Only recently there has been changes in guidelines that now recommend screening for high-risk population such as patients with T2D. 21
The prevalence of HCC in patients with MAFLD who do not have cirrhosis presents a significant clinical paradox, given the traditional understanding that severe fibrosis or cirrhosis is a precursor for HCC development. Intriguingly, research indicates that up to 30–40% of MAFLD-related HCC occurs in the absence of cirrhosis, suggesting alternative pathogenic mechanisms are at play in this subset of patients. 22
The mechanisms contributing to HCC development in non-cirrhotic MAFLD patients likely involve metabolic derangements that go beyond simple hepatic fat accumulation. Factors such as insulin resistance, oxidative stress, and chronic systemic inflammation might directly induce oncogenic pathways in hepatocytes. 23 Clinically, the absence of cirrhosis in MAFLD patients diagnosed with HCC often leads to a later presentation and diagnosis of liver cancer, primarily because surveillance protocols are generally more relaxed for non-cirrhotic patients. This delay in diagnosis can adversely affect prognosis.
Given the significant proportion of non-cirrhotic MAFLD patients developing HCC, there is a pressing need for targeted surveillance strategies. Adjusting current guidelines to incorporate risk assessments for HCC in non-cirrhotic MAFLD patients could potentially improve early detection rates. Research by Kanwal et al. (2018) emphasizes the importance of integrating noninvasive markers of liver health, such as elastography and serum biomarkers, to identify patients at high-risk of HCC. 24 Our study highlights that in high-risk patients there is high prevalence of advanced fibrosis. Screening these patients is crucial for optimizing clinical management and improving patient outcomes.
Our study population was diverse and comprised a majority of Black African/Caribbean (57%), followed by Caucasians (18.4%), Mediterranean (11%), Latin (5.8%), Asians (4.9%), and Middle East (2.7%). About 53.5% had steatosis and 27% were diagnosed with liver fibrosis on FibroScan. Of the subjects with steatosis, 77.4% were non-Caucasians and 22.6% Caucasians. Similarly with those diagnosed with high fibrosis, 76% were non-Caucasians and 23.9% Caucasians. Only 48.9% were aware of being overweight while average BMI was 32 kg/m2. MAFLD awareness was 30% in the whole group with highest in the Caucasians with 41.5%. The study is not only about the prevalence of undiagnosed MAFLD patients in this population but more importantly investigate the awareness about MAFLD within different ethnicities and lifestyle preference in this variable population contributing to the high prevalence of MAFLD. These areas have never been studied in high-risk, highly diverse population in UK. The diverse ethnic backgrounds within our cohort, far from being a limitation, actually enrich our study by offering a more comprehensive understanding of how MAFLD manifests in multicultural urban settings.
Lifestyle modification, which encompasses diet, physical activity, and/or exercise, is the primary recommended therapy for MAFLD, especially in the absence of approved pharmaceutical agents. Despite this, the evidence underpinning the use of lifestyle therapy in liver disease is limited, thus significantly restricting its application in clinical care. Dietary pattern is one of the most important factors in preventing and treating MAFLD. 25 To understand the role of diet, food preference, and physical activity we designed the questionnaire for this high-risk population. The results highlighted that 68% of subjects had more than four servings of fruits or vegetables in their diet per week. Only 37.7% of subjects consumed healthy foods such as olives oil, nuts, and seeds. Despite having diabetes, 40.5% of subjects admitted to having ultra-processed foods and sweets daily in their diet. A total of 65.8% confirmed that their diet consisted of high-carbohydrate diet such as rice, pasta, potatoes, and couscous. Alcohol intake was minimal with only 3.6% drinking more than five glasses of alcohol per week. These results suggest that most high-risk subjects do not adhere to a healthy lifestyle despite specific guidance. This could be due to general lack of awareness regarding the fatty liver disease or people are aware about the healthy food choices but can’t afford the good food. High use of glycemic diets along with fatty liver considered as a normal of variation are factors that are major contributors for the high prevalence of this disease.
According to Public Health England, physical inactivity is the fourth leading risk factor for global mortality accounting for 6% of deaths globally. WHO guidelines for 2023 state that regular physical activity is associated with a reduced risk of diabetes, obesity, and other noncommunicable diseases. 26 Our study population comprised subjects with T2D and 68% had dyslipidemia. Most (96%) of subjects confirmed that they were given lifestyle management advice by their healthcare team. However, only 43% of the study participants were undertaking moderate exercise for least 3 or more times per week. This highlights the urgent need to identify a more preventative approach, intervening earlier and considering the social determinants of health. Raising MAFLD awareness, early recognition, and intervention are important in high-risk groups in order to improve clinical outcomes.
The demographic composition of our study, predominantly consisting of individuals of Black African/Caribbean descent, was a result of our focus on a specific geographical area to provide locally relevant health insights. While this approach enhances the applicability of our findings to the community served, it introduces limitations in generalizing these results to broader populations. The sample size calculation was not performed for this study as this was a unique service development pilot project; however, we acknowledge it can be a limitation as it may impact the applicability and sensitivity of the findings.
Our study also did not collect socioeconomic status (SES) data, a decision influenced by the focus on a MAFLD in a diabetic population attending secondary care and the constraints of a busy clinical setting. Adding comprehensive socioeconomic assessments could have increased the complexity and length of our data collection process, potentially affecting participation rates and data quality. We advocate for further research in more demographically varied populations and suggest future research include SES data to provide a more comprehensive analysis of these issues.
Conclusion
Our study provides a detailed baseline assessment of MAFLD in the T2D population in South London, examining their awareness of MAFLD and lifestyle preferences as a contributing factor, while setting the stage for longitudinal studies and tailored interventions for this specific demographic. The questionnaire showed that 99% of our study group wanted more guidance and multidisciplinary approach from healthcare workers regarding lifestyle modification. Early detection should be followed by lifestyle modification as a preventative strategy, with a focus on health optimization. It is critical to screen patients who are already in our healthcare system with other preexisting conditions such as metabolic syndrome to ascertain an early diagnosis of MAFLD. Greater awareness of MAFLD and the development of cost-effective risk stratification strategies are warranted to address the growing burden of MAFLD, with its additive morbidity and mortality.
Supplemental Material
sj-docx-1-taj-10.1177_20406223241264539 – Supplemental material for Lack of awareness and ethnic polarity is a major cause of metabolic associated fatty liver disease in high-risk diabetes population in South London
Supplemental material, sj-docx-1-taj-10.1177_20406223241264539 for Lack of awareness and ethnic polarity is a major cause of metabolic associated fatty liver disease in high-risk diabetes population in South London by Saima Ajaz, Mark Chamley, James Lok, Riham Soliman, Reece Khan, Karan Ahir, Monique Curtis, María Fernanda Guerra-Veloz and Kosh Agarwal in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
We extend our heartfelt gratitude to all the patients who participated in the service evaluation project. Your involvement was invaluable and deeply appreciated. Additionally, we would like to thank the staff of the Lambeth Diabetes Intermediate Care Team for their unwavering support and dedication.
Recording of verbal consent
All subjects coming to the clinic were sent information regarding the service evaluation project. This was done to give them enough time to understand that if they want a liver scan it can be carried out by a dedicated team who will also give them a questionnaire regarding their lifestyle choices. The researcher explained the process in detail again on the day to the subjects who wanted to take part in this project. Subjects also consented for publication. Once they agreed verbally, the researcher entered the consent date, time, location of the consent discussion, the information provided to the participant, and the participant’s verbal agreement with anonymized ID in the data set. The questionnaire provided to participants outlined the study details, along with boxes to check. Instead of requiring a signature, the form includes a box that the researcher checks to indicate that verbal consent was obtained.
Follow-up confirmation
After obtaining verbal consent, a follow-up letter was given to the participant summarizing their outcomes. This step provided the participants with a record of their participation.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.