
Abstract
Background:
Transmural healing (TH) has emerged as a potential treatment goal for Crohn’s disease (CD). However, further research is needed to confirm its benefits and risk factors associated with TH remain unclear.
Objectives:
We aimed to assess the value of TH based on magnetic resonance enterography (MRE) in Chinese CD patients regarding the long-term outcomes and its associated factors.
Design:
Retrospective, observational cohort study.
Methods:
Patients with CD diagnosed by colonoscopy and MRE examination between 2015 and 2022 were included. All patients were evaluated with endoscopy together with MRE within 6–12 months after baseline and followed up for at least 6 months after evaluation. The primary endpoint was the occurrence of major outcomes during the follow-up, including drug escalation, hospitalization, and surgery. The cumulative probabilities of major outcomes were calculated using Kaplan–Meier survival curves. Logistic regression analyses were used to predict TH within 6–12 months after baseline.
Results:
A total of 175 patients were included in the study. Of these, 69 (39.4%) patients achieved mucosal healing (MH), but only 34 (19.4%) of them achieved TH. The median follow-up duration was 17.4 months (interquartile range, 11.6–25.5), and major outcomes occurred in 58.3% of patients. A lower occurrence rate of major outcomes was noted in patients who achieved TH than in those who achieved MH only (p = 0.012). The baseline lymphocyte/C-reactive protein ratio (LCR) [odds ratio (OR), 1.60; 95% confidence interval (CI), 1.02–2.50; p = 0.039] and bowel wall thickness (BWT) (OR, 0.72; 95% CI, 0.59–0.90; p = 0.003) were independent predictors associated with TH. According to multivariate Cox regression analysis, low LCR [hazard ratio (HR), 2.34; 95% CI, 1.51–3.64; p < 0.001], and no healing (HR, 5.45; 95% CI, 2.28–13.00; p < 0.001) were associated with an increased risk of major outcomes.
Conclusion:
Patients with CD who achieved TH showed improved prognosis compared to those who achieved MH only. Baseline LCR and BWT might predict TH.
Introduction
Crohn’s disease (CD) is a chronic inflammatory disease, which affects any locations of the gastrointestinal tract. CD is characterized by transmural inflammation and is associated with the development of complications, such as strictures, fistulas, and abscesses. 1 Persistent transmural injuries often result in structural bowel damage and even surgical resection. 2 In recent years, treatment strategies for CD have evolved into a ‘treat-to-target’ clinical management approach.3,4 Given the poor correlations between clinical activity indices and mucosal inflammation, clinical remission remains a treatment target, although only in the short term.5,6 Meanwhile, mucosal healing (MH) is starting to be considered as a treatment goal and is associated with a lower incidence of hospitalization, CD-related surgery, and disabling disease.7–9 However, since transmural damage is the key characteristic of CD, patients with persistent MH can also exhibit residual intestinal wall inflammation. 10
Transmural healing (TH) can be assessed by cross-sectional imaging tools, including intestinal ultrasonography, computed tomography enterography, or magnetic resonance enterography (MRE). Evidence has shown that TH is associated with improved long-term outcomes when compared to patients with MH.6,11 Based on these findings, the treatment target of patients with CD could be upgraded to achieving TH. However, to date, there is no proven, globally accepted criterion and evaluation intervals of TH. Furthermore, because TH is harder to achieve, more research is needed to confirm the benefits derived from TH. The Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE)-II consensus recommended TH as a measure of depth of remission, rather as a new treatment target. 3 In addition, risk factors associated with TH still remain unclear.
In this context, the present study aims to assess the value of TH in long-term outcomes from a Chinese cohort and explore the predictive indicators of TH.
Methods
Study design and patients
This retrospective, observational cohort study was conducted at the First Affiliated Hospital of Sun Yat-Sen University, a tertiary inflammatory bowel disease referral center. The data of CD patients between 2015 and 2022 were collected. Patients with a confirmed diagnosis of CD were enrolled. 12 Inclusion criteria included: (a) age ⩾18 years; (b) diagnosis of active CD with relatively complete clinical data at baseline, including colonoscopy and MRE examination; and (c) endoscopy and MRE evaluation within 6–12 months after baseline, with an examination interval ⩽3 months. In summary, each patient completed at least two endoscopy and MRE examinations, one at baseline and the other at evaluation 6–12 months post-baseline. Exclusion criteria included: (a) pregnancy; (b) other intestinal comorbidities, such as intestinal tuberculosis, or malignant intestinal tumor; (c) patients who underwent intestinal surgery within 3 months after baseline; (d) incomplete colonoscopy that failed to reach the terminal ileum; and (e) patients who had less than 6 months of follow-up after the endoscopy/MRE evaluation.
Data collection
Data on patient demographic characteristics, disease duration, the Montreal classification of disease, 13 previous surgery, laboratory indicators, imaging data, colonoscopy results, and treatment strategies were collected via a comprehensive review of the medical records. We evaluated MH and TH at the 6–12 months after baseline, and conducted further follow-ups for at least 6 months after evaluation to assess the patients for CD-related long-term outcomes.
Endoscopic evaluation and definition of MH
All endoscopic reports and images were reviewed by two gastroenterologists who were blinded to radiological information. In the case of a discrepancy, a third investigator was tasked with resolving disputes. According to Simple Endoscopic Score for Crohn’s Disease (SES-CD), the intestinal tract was divided into five segments (i.e. terminal ileum, right colon, transverse colon, left colon, and rectum) and was assessed from four endoscopic variables (i.e. size of ulcer, the extent of ulcerated surface, the extent of affected surface, and presence of stenosis). 14 MH was defined as absence of ulcerations in any bowel segment (SES-CD ⩽ 2). 15
MRE evaluation and definition of TH
MRE was performed by using a 3.0-T Magnetom Trio system (Siemens Medical Solutions, Erlangen, Germany). After bowel clearing, the subjects were administered 1600–2000 mL of 2.5% mannitol solution 1 h before the procedure, as well as an intramuscular injection of 10 mg of raceanisodamine hydrochloride 10 min prior to the MRE. 16 MRE, including T2-weighted imaging (repetition time: 1200 ms, echo time: 87 ms, 320 × 194 matrix, 4 mm slice thickness, 160° flip angle) and diffusion-weighted imaging with b value of 800 s/mm2 (3200 ms, 80 ms, 132 × 132, 5 mm) images, was routinely performed.16,17 The corresponding apparent diffusion coefficient (ADC) map was automatically generated by using the monoexponential model on the scanner console. T1-weighted imaging (4.37 ms, 1.37 ms, 320 × 217, 2 mm, 13°) was performed before and at 30 s, 60 s, 90 s, 2 min, 3.5 min, and 7 min after the intravenous injection of 0.2 mL/kg gadopentetate dimeglumine ( Beilu Pharmaceuticals, Beijing, China) at a rate of 2 mL/s. 16 Two experienced radiologists, who were blinded to the clinical and endoscopic data, evaluated the radiological outcomes. TH was defined as bowel wall thickness (BWT) ⩽ 3 mm with no inflammatory signs (i.e. ulcer, intramural edema, diffusion-weighted hyperintensity, and contrast enhancement) and no complications (i.e. abscess, strictures, or fistula). 2
Group division
Based on the clinical, endoscopic, and MRE evaluations at 6–12 months after baseline, all subjects were divided into three groups: (a) the MH group comprised of patients who achieved MH only without TH; (b) the TH group comprised of patients who achieved MH plus TH; and (c) the non-healing (NH) group comprised of patients who achieved neither MH nor TH.
Long-term outcomes
The primary endpoint was the occurrence of major outcomes, including drug escalation, hospitalization, and surgery. Drug escalation was defined as an increase in the dose of the original drug, shortening of the interval between the doses, step-up treatment, or the use of corticosteroid. Hospitalization was defined as hospital admission related to CD during the follow-up excluding scheduled biologic therapy. Surgery was defined as any CD-related bowel resection.
Statistical analysis
All analyses were performed using the SPSS software (version 25.0; IBM, Chicago, IL, USA). Quantitative variables were expressed as means with standard deviation (SD) or medians with interquartile range (IQR), whereas qualitative variables were described as numbers and percentages. Student’s t test and Mann–Whitney U test were used to compare with quantitative variables. Comparisons among groups were used for χ2 test, or Kruskal–Wallis test, as appropriate. Logistic regression analyses with stepwise selection were used to predict TH at evaluation using baseline factors, and variables with p < 0.1 on univariate logistic regression analysis were included in the multivariate analysis. The cumulative probabilities of the major outcomes were calculated using Kaplan–Meier survival curves, and the log-rank test was performed to compare differences among groups. If multiple adverse outcomes occurred, survival analyses were managed based on the time of the first major outcome. Cox regression analysis was used to determine risk factors associated with major outcomes. Statistical significance was defined as a two-sided p < 0.05.
Results
Baseline characteristics
In total, 322 adult patients with confirmed active CD were evaluated with endoscopic and MRE examination within 6–12 months after baseline. Ultimately, 175 patients were enrolled in the study, and 147 patients were excluded (Figure 1). The baseline characteristics of the study are summarized in Table 1. Of the 175 patients, 65.7% were male. The median age was 30 years (IQR, 23–37), and the median of disease duration was 3.5 years (IQR, 1.0–7.5). According to the Montreal classification, 86.3% of patients were classified as L3 (ileocolonic phenotype), and 60.0% of patients were classified as B1 (non-stricturing, non-penetrating). Upper gastrointestinal lesions were observed in 37 (21.1%) patients at diagnosis, and 101 (57.7%) had perianal disease. Nearly half of the patients (76, 43.4%) had a history of azathioprine/methotrexate, 43 (24.6%) had prior corticosteroids usage, 36 (20.6%) patients had prior biologics therapy, and 47 (26.9%) patients were treatment-naïve. Overall, 40 (22.9%) patients had previous intestinal resection. The median of baseline SES-CD score was 11.0 (IQR, 6.0–18.0).

Flow-chart of the study.
Baseline characteristics.

BMI, body mass index; IQR, interquartile range; SES-CD score, simple endoscopic score for Crohn’s disease.
Post-treatment evaluation
Within the cohort, 69 (39.4%) patients achieved MH and 34 (19.4%) achieved TH after comprehensive evaluations. Specifically, 34 patients showed both MH and TH, whereas 35 patients achieved MH only.
The medication regimens in all patients after baseline and the respective MH/TH rates between different groups are shown in Figure 2. Biologics (103/175, 58.9%) were the most common medication therapy: anti-tumor necrosis factor (TNF) agents accounted for up to 36.6% (64/175), vedolizumab accounted for 10.3% (18/175), and ustekinumab was used for 12.0% (21/175). Next, immunomodulators (i.e. azathioprine, methotrexate, and thalidomide) accounted for 18.3% (32/175) of patients. A total of 40 (22.9%) patients were administered combination therapy (biologics + immunomodulator), whereas 15 (8.6%) patients started therapy with corticosteroids. Patients with anti-TNF agents and ustekinumab achieved higher MH/TH rates than those administered other treatments. Moreover, the ustekinumab group had the highest TH rate (7/21, 33.3%) among the treatment groups (Figure 2). However, no statistically significant difference was observed between any of the group pairwise comparisons.

Patient’s medication regimens and MH/TH rate.
Long-term outcomes in the study groups
In this study, the median follow-up observation interval was 17.4 months (IQR 11.6–25.5) after endoscopy and MRE evaluation. Among the three groups, no significant difference were observed in terms of the median follow-up duration (p = 0.732).
Major outcomes
During the follow-up period, 102 (58.3%) patients experienced major outcomes, including 6 (17.6%), 16 (45.7%), and 80 (75.5%) patients in the TH, MH, and NH groups, respectively (Figure 3). According to the Bonferroni correction, significance was achieved at p < 0.0167. Compared to the NH group, the TH and MH groups showed a significantly lower probability of major outcomes (p < 0.001 and p = 0.001, respectively) after the Bonferroni correction. Furthermore, the TH group had an even lower rate of major outcomes compared to the MH group (p = 0.012) (Figure 3). Further Kaplan–Meier curve analysis suggested that the TH group (log-rank p < 0.001) and MH group (log-rank p < 0.001) showed a longer outcomes-free survival compared to the NH group [Figure 4(a)].
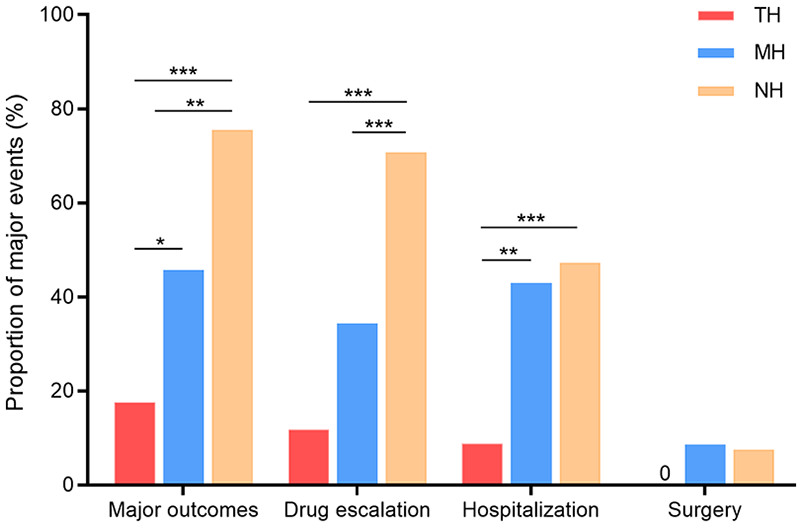
Rates of major outcomes in each group.

Kaplan–Meier curve illustrating major (a) outcomes-free survival, (b) drug escalation-free survival, (c) hospitalization-free survival, and (d) surgery-free survival among three groups (adjusting p-values).
Drug escalation
A total of 91 (52.0%) patients experienced at least one drug escalation. The rates of drug escalation were significantly lower in the TH (11.8%, p < 0.001) and MH groups (34.3%, p < 0.001) compared to the NH group (70.8%). There was no significant difference between the TH and MH groups (p = 0.027) (Figure 3). The Kaplan–Meier curve analysis indicated that the patients in the TH or MH group had a longer drug escalation-free survival than those in the NH group (log-rank p < 0.001 for all). A relatively lower cumulative risk was observed in the TH group than the MH group [log-rank p = 0.059; Figure 4(b)].
Hospitalization
During the follow-up period, 68 (38.9%) patients were hospitalized. Compared to the MH (42.9% versus 8.8%, p = 0.001) and NH (47.2% versus 8.8%, p < 0.001) groups, the TH group showed a lower rate of hospitalization (Figure 3). According to the Kaplan–Meier curve analysis, the time spent hospitalization-free was significantly longer for patients who achieved TH (TH group versus MH group, log-rank p = 0.008; TH group versus NH group, log-rank p < 0.001). No significant difference was observed between the MH and NH groups [log-rank p = 0.221; Figure 4(c)].
Surgery
A total of 11 (6.3%) patients underwent surgery during the follow-up, none of which were from the TH group. However, among the three groups, no significant differences were observed in the rate of surgery or surgery-free survival [Figures 3 and 4(d)].
Factors associated with TH or prognosis
Prediction of TH
In subgroup analysis, the TH group had a higher baseline albumin (ALB, p = 0.003) and lymphocyte/C-reactive protein ratio (LCR, p < 0.001), but lower erythrocyte sedimentation rate (p = 0.013), C-reactive protein (CRP, p < 0.001), and BWT (p < 0.001) than the no-TH group (Table 2). There were no significant differences between the groups in terms of age at diagnosis, smoking history, disease location, and disease behavior. Compared to the NH group, the TH group had a higher tendency of hemoglobin at baseline, and lower tendency of platelet count, neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and SES-CD score.
Comparison of variables at baseline in patients with TH versus no TH.

The bold font represents statistical significance at p < 0.05.
ALB, albumin; BMI, body mass index; BWT, bowel wall thickness; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; HB, hemoglobin; IQR, interquartile range; LCR, lymphocyte/C-reactive protein ratio; MRE, magnetic resonance enterography; NLR, neutrophil to lymphocyte ratio; PLR, platelet to lymphocyte ratio; PLT, platelet count; SD, standard deviation; SES-CD score, Simple Endoscopic Score for Crohn’s Disease; TH, transmural healing; TNF, tumor necrosis factor; WBC, white blood cell.
To identify the potential factors associated with TH, univariate logistic regression analysis was used to screen variables; those with p < 0.1 were included in the multivariate stepwise analysis (Table 3). LCR [odds ratio (OR), 1.60; 95% confidence interval (CI), 1.02–2.50; p = 0.039] and BWT (OR, 0.72; 95% CI, 0.59–0.90; p = 0.003) at baseline were found to be independent factors associated with a higher likelihood of TH (Table 3).
Univariate and multivariate analysis showing variables at baseline associated with TH.

The bold font represents statistical significance at p < 0.05.
ALB, albumin; BWT, bowel wall thickness; CI, confidence interval; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; LCR, lymphocyte/C-reactive protein ratio; OR, odds ratio; PLT, platelet count; TH, transmural healing; TNF, tumor necrosis factor.
Risk factors of prognosis
A multivariable model including demographic, LCR, healing status, treatment, and other variables was used to assess their effectiveness in predicting prognosis. The results of univariate and multivariate analyses for each outcome are shown in Supplemental Tables S1–S4. Multivariate Cox regression analysis demonstrated that an increased risk of major outcomes occurred in patients with low LCR [defined as scored ⩽2.0 based on the optimal LCR cutoff value using receiver operating characteristics analysis (Supplemental Figure S1)] [hazard ratio (HR), 2.34; 95% CI, 1.51–3.64; p < 0.001], and with no healing when evaluation (HR, 5.45; 95% CI, 2.28–13.00; p < 0.001). Low LCR (HR, 2.16; 95% CI, 1.36–3.42; p = 0.001) and patients with no healing (HR, 7.41; 95% CI, 2.61–21.04; p < 0.001) were also found to be associated with a higher risk of drug escalation. Low LCR (HR, 2.05; 95% CI, 1.20–3.49; p = 0.008) and patients without TH (MH only: HR, 4.28; 95% CI, 1.21–15.22; p = 0.025; NH: HR, 4.85; 95% CI, 1.45–16.27; p = 0.010) were associated with a higher risk of hospitalization. Meanwhile, low LCR (HR, 6.58; 95% CI, 1.67–25.93; p = 0.007) and B3 phenotype (HR, 9.17; 95% CI, 1.82–46.10; p = 0.007) were associated with a higher risk of surgery (Table 4).
Multivariate analysis for long-term outcomes.

The bold font represents statistical significance at p < 0.05.
CI, confidence interval; HR, hazard ratio; LCR, lymphocyte/C-reactive protein ratio; MH, mucosal healing; NH, no healing; TH, transmural healing.
Discussion
This study provides retrospective evidence regarding the CD-related long-term outcomes of TH in Chinese CD patients. Patients who had achieved TH were less likely to develop major outcomes during the follow-up observation period. Compared to patients with MH only or NH, patients with TH were found to have a lower risk of hospitalization. Furthermore, baseline LCR and BWT were found to be associated with TH.
Recent evidence has highlighted the benefits of achieving TH in CD-related long-term outcomes. Studies have shown that achieving TH in patients with CD is significantly correlated with clinical remission and a lower risk of hospitalization and surgery.15,18,19 Messadeg et al. 20 discovered that after anti-TNF treatment in patients with CD, an early transmural response at week 12 was able to predict steroid-free remission at week 52. Furthermore, the value of deep healing (defined as MH combined with radiologic healing) has been evaluated in recent studies, with deep healing having been found to be superior in predicting CD-related outcomes. 21 Oh et al. 22 analyzed 392 patients with CD and found that patients who achieved both radiologic and endoscopic healing had a decreased risk of poor clinical outcomes compared to MH-only patients and those without MH regardless of imaging findings. A similar result was obtained in the present study. However, in terms of surgery, neither the TH nor MH group showed a lower probability compared to the NH group, which may be explained by the relatively small sample size of surgical patients in this cohort.11,23 An interesting observation from our study was made, where the MH group had a higher rate of hospital admission compared to the TH group, while there was no statistical difference with the NH group. This observation may be explained by the broader definition of hospitalization used in this study, including any admissions related to CD, whereas some symptom-driven admissions but inactive conditions were also included. Tse et al. 24 demonstrated that gastrointestinal symptoms correlated weakly with endoscopic disease activity. They found that one-third of patients in endoscopic remission continued to report gastrointestinal symptoms. The low-risk benefit of MH regarding hospitalization may be offset by these symptom-driven admissions. However, on the other hand, patients with MH only were more likely to experience symptoms of discomfort and had more clinical needs compared to those with TH, which should be taken into consideration.
It should also be noted that the currently available treatments have a limited ability to achieve TH, even to an extent where biological agents have limited ability. A study of CD patients being administered anti-TNFs found that only 23% of patients achieved TH. 25 In our study, only 19.4% patients achieved TH, reinforcing the viewpoint that TH is a rare event. The efficacy of various drug was also explored in this study and patients being administered ustekinumab had a relatively higher TH rate (33.3%), although no statistically significant differences were observed when compared with other therapies. A prospective, longitudinal cohort study showed that beside thalidomide, patients with anti-TNF agents achieved higher TH rates than those with other drugs, such as 5-aminosalicylic acid and Methotrexate/Azathioprine. 15 Another study comprised of 134 CD patients being administered biologic therapy 1 year after induction reported transmural remission rates between patients with infliximab, adalimumab, ustekinumab, and vedolizumab of 48%, 29%, 33%, and 55%, respectively. 26 Calabrese et al. 27 observed a lack of significance between differences in terms of the speed of effectiveness of TH among biologics.
However, differences in TH rates between various drugs have yet to be elucidated, and a further prospective study with a large cohort is warranted. The difference between our study and previous works was that our study included patients treated not only with anti-TNFs but with various other drug therapy regimens. In our study, 20.2% of patients accepted prior biologics, and the treatment option of other biologics could be their final therapeutic option. The analysis of different inflammatory processes based on patient profiles and personalized therapeutic regimens will probably allow for a better differentiation of TH status with different biologics. However, this study allows for an initial assessment of the achievement of TH with various drug therapies.
The positive prognosis of TH has been recognized, and much attention is focused on the influencing factors of TH. It has been previously reported that baseline MRE indices (i.e. BWT, ADC, and stenosis), 28 Magnetic Resonance Index of Activity score, 29 colon lesion, 27 and fecal calprotectin (FC) value (cutoff of 81.1 mg/kg) 30 were associated with TH. Takenaka et al. 26 found that high drug concentration levels of biologic therapy were correlated with transmural remission (defined as sMaRIA score of the most affected bowel segment <2 combined with modified SES-CD score <4). In our study, the decreased BWT at baseline was independently associated with a higher likelihood of TH, which was consistent with previous studies. In addition, we found a new biomarker LCR was a predictor of TH and that a low LCR status was an independent risk factor for adverse outcomes. LCR, integrating impression of both inflammatory and malnutrition, is often performed as a predictor of the negative progression of the digestive tumor patients, and is also used for prognostic scores.31,32 A low LCR has been shown to be an independent predictor of sepsis in neonates with pneumonia. 33 Therefore, LCR demonstrates potential as a predictive factor of inflammation and disease related outcomes. To the best of our knowledge, the present study is the first to elucidate the role of LCR in TH, which reflects both inflammatory and nutrition conditions. Thus, LCR may be a sensitive and useful factor in the long-term outcomes of CD. However, further research will be needed to confirm these preliminary findings.
This study had several limitations. First, the study was retrospective and had a relatively short follow-up time (median 17.4 months). The latter may limit the evaluation of long-term outcomes, such as the need for surgery. Furthermore, we may have underestimated the incidence of surgery due to the fact that patients who failed to reach the terminal ileum with colonoscopy were excluded from this study. These patients may undergo surgical treatment to relieve the obstructive symptoms. The lower number of surgeries may impact our ability to assess differences between TH and MH. However, we obtained complete intestinal segment information to evaluate whether MH occurred. Second, although FC is a strong indicator for inflammatory status of patients with CD, 34 it was not included in the analysis due to many missing samples in the participants. In addition, because the definition of TH based on MRE remains controversial, the definition used in our study was adopted from that used in previous studies. 2 Lastly, further prospective studies with a longer follow-up time are needed to validate our findings.
Conclusion
Taken together, this study showed that TH was a positive factor of better long-term outcomes, indicating the need to upgrade to a higher therapeutic target compared to those with only MH for patients with CD. In addition, baseline LCR and BWT were associated with TH.
Supplemental Material
sj-doc-1-taj-10.1177_20406223241259654 – Supplemental material for Long-term outcomes and associated factors of Crohn’s disease patients achieving transmural healing based on magnetic resonance enterography: a Chinese retrospective cohort study
Supplemental material, sj-doc-1-taj-10.1177_20406223241259654 for Long-term outcomes and associated factors of Crohn’s disease patients achieving transmural healing based on magnetic resonance enterography: a Chinese retrospective cohort study by Yaming Lu, Shanshan Xiong, Mengchen Zhang, Xiaoman Zu, Jinbin Li, Ren Mao, Zhirong Zeng, Xuehua Li, Minhu Chen and Yao He in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-1-taj-10.1177_20406223241259654 – Supplemental material for Long-term outcomes and associated factors of Crohn’s disease patients achieving transmural healing based on magnetic resonance enterography: a Chinese retrospective cohort study
Supplemental material, sj-docx-1-taj-10.1177_20406223241259654 for Long-term outcomes and associated factors of Crohn’s disease patients achieving transmural healing based on magnetic resonance enterography: a Chinese retrospective cohort study by Yaming Lu, Shanshan Xiong, Mengchen Zhang, Xiaoman Zu, Jinbin Li, Ren Mao, Zhirong Zeng, Xuehua Li, Minhu Chen and Yao He in Therapeutic Advances in Chronic Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.