
Abstract
Background:
Most patients with type 2 diabetes mellitus (DM2) will require insulin for glycemic control during their disease.
Objectives:
We evaluated the willingness to start insulin therapy among insulin-naïve persons with DM2 in urban Northern Uganda.
Design:
A facility-based, quantitative, cross-sectional study was conducted between June and August 2023 recruiting insulin-naïve type 2 diabetes mellitus patients attending routine health care at Gulu Regional Referral Hospital, Gulu, Uganda.
Methods:
We gauged participants’ willingness to use insulin by asking, ‘If your doctor prescribed insulin for you, would you accept to use it?’ with responses categorized as either ‘Yes’ or ‘No’. Poisson regression analysis was performed to assess the factors associated with willingness to start insulin therapy. p < 0.05 were considered statistically significant.
Results:
We enrolled 190 participants, with a mean age of 55 ± 12.72 years. Most participants were female (63.7%, n = 121), attained a primary level of education (70.0%, n = 133), and were unemployed (84.2%, n = 160). Overall, 73.4% (n = 138) of the participants were willing to receive insulin therapy if indicated. Participants recently advised on insulin showed a 34% higher willingness [adjusted prevalence ratio (aPR): 1.34, 95% confidence interval (CI): 1.06–1.72, p = 0.007], whereas those with a disease duration of 6 years or more were 43% less willing (aPR: 0.57, 95% CI: 0.39–0.81, p = 0.002) and those concerns about coping with insulin therapy were 55% less willing to commence insulin therapy (aPR: 0.57, 95% CI: 0.39–0.81, p = 0.002).
Conclusion:
About three in every four participants with DM were willing to receive insulin if indicated. However, healthcare providers should consider personalized counseling strategies to alleviate concerns and enhance informed decision-making regarding insulin initiation. Future interventions should focus on addressing specific barriers associated with prolonged disease duration and apprehensions related to insulin therapy to optimize glycemic control in this population.
Plain language summary
In this study, we investigated the willingness to start insulin therapy among individuals with type 2 Diabetes Mellitus (DM2) in urban Northern Uganda. Understanding the importance of insulin for glycemic control in DM2, we surveyed 190 participants at Gulu Regional Referral Hospital. We found that more than three-quarters of the participants expressed a willingness to receive insulin therapy if recommended. Factors influencing this willingness included recent advice on insulin, which was associated with a 34% higher likelihood of acceptance. Conversely, individuals with a disease duration of 6 years or more were 43% less willing, and those concerned about coping with insulin therapy were 55% less willing to commence treatment. These findings underscore the need for healthcare providers to offer personalized counseling strategies, addressing specific concerns, to facilitate informed decision-making regarding insulin initiation. Looking ahead, interventions should prioritize overcoming barriers related to prolonged disease duration and apprehensions about insulin therapy to optimize glycemic control and improve the well-being of individuals with DM2 in this population.
Introduction
Globally, the number of people with diabetes mellitus (DM) has increased four times in the past 30 years making it the ninth major cause of death. 1 The most prevalent DM is type 2 (DM2) affecting an estimated 90–95% of the global 8.5% adult population with DM. 2 Almost 10% of adults now have DM. 3 Sub-Saharan Africa has witnessed a significant increase in the prevalence of DM2 of 4.3% in 2012 compared with a current global prevalence of 6.4% in the last 50 years. 4
DM2 is a common metabolic disorder caused by the inability of insulin-sensitive tissues to respond appropriately to insulin. Defects in any of the mechanisms involved in its synthesis can lead to a metabolic imbalance responsible for the development of the disease more so when there is an inability of insulin-sensitive issues to respond appropriately to insulin. 5 DM has become a common serious threat with costly management however controllable. It has been found that proper management and control can be done through prevention, early detection, improved delivery of care, and better education for diabetes self-management. 6
Poorly controlled DM2 is considered a significant public health problem and is associated with adverse outcomes. 7 DM2 is a major risk factor for cardiovascular disease and microvascular complications. 8 The prospect of insulin therapy disturbs patients’ sense of self and their psychological well-being. There is a high need to address the psychological insulin resistance in patients with DM2 for effective diabetic management. 9 The reasons for patient unwillingness were injection anxieties, fear of needles, insufficient knowledge of insulin, feeling unable to cope with insulin, and concerns about out-of-pocket costs. 9
Because of therapeutic inertia and the progressive nature of the disease, many need at least a basal insulin supplementation and insulin analogs. 10 Many patients with DM2 refuse insulin therapy even when they require this modality of treatment. Exploring patients’ concerns and beliefs about DM and insulin is crucial to assist physicians in delivering patient-centered care. 11 Early glycemic control leads to better outcomes, including a reduction in long-term microvascular and microvascular complications. 12 Therefore, we aimed to determine the willingness to start insulin therapy among insulin-naïve persons with DM at an urban regional referral hospital in Northern Uganda.
Methods
Study design
A facility-based, quantitative, cross-sectional study was conducted between June and August 2023 recruiting insulin-naïve type 2 diabetes mellitus (T2DM) patients attending routine health care at Gulu Regional Referral Hospital (GRRH), Gulu, Uganda. We followed the Strengthening the Reporting of Observational Studies in Epidemiology Guidelines.
Study setting
The study was conducted in GRRH, located in northern Uganda in Gulu City. GRRH is a tertiary and a teaching Hospital serving Northern Uganda, with an estimated 2000 DM patients at the diabetic clinic. The clinic is run by a physician, medical officers, and intern doctors, with an additional workforce being derived from a pool of general and specialized nurses, lab technologists, nutritionists, and social workers. The diabetes clinic receives patients with DM primarily from the Gulu district but also referral cases of complex patients for specialist review from across districts in Northern Uganda according to Uganda clinical guidelines.
Study population
The study participants were patients with physician-diagnosed DM2 who were, 18 years or older, attending outpatient DM clinics, and provided written informed consent to participate in the study. Participants who were admitted and unconscious or sedated with difficulty communication during the study period were excluded.
Sample size estimation
The sample size was estimated using the Kish–Leslie formula with the following assumptions: margin of error of 5%, at 95% confidence interval (CI), the prevalence of willingness modestly estimated at 50% since there was no previous study in Uganda about willingness to start insulin therapy, we obtain a minimum size of 384 and using Slovin’s formula, a final sample size of 197 was realized.
Sampling procedure
We used a consecutive sampling technique to enroll eligible participants following their clinical reviews.
Data collection and tools
Data were collected using an interviewer-administered, structured questionnaire which was adopted from Ngassa Piotie et al. 9 The questionnaire was written in Luo and back translated in English. It was collected by trained research assistants with regular supervision. Socio-demographic characteristics such as age, sex, religion, marital status, clinical factors, attitudes are barriers to using insulin.
Operational definitions
Participants’ willingness to utilize insulin was assessed through the question: ‘If your physician were to prescribe insulin for your treatment, would you be willing to accept it?’ with response options ‘Yes’ or ‘No’ indicating the participants’ preferences.
For participants who responded ‘No’, a follow-up question was presented: ‘Would you consider receiving insulin if it were the only treatment option?’ A ‘No’ response to this follow-up question was categorized as indicative of hesitancy.
Statistical analysis
Data were entered into Microsoft Excel for coding and cleaning and exported to STATA version 18 for statistical analysis. Descriptive statistics of variables such as age, sex, and marital status were computed in frequency, percentage, median, mean, and standard deviation and presented using tables to show a picture of the data. Bivariate logistic regression was performed to determine each of the explanatory variables with the outcome variable (willingness) and variables with p < 0.2 during bivariate analysis were considered for further analysis to multivariable analysis. Poisson regression was conducted to determine the presence of a statistically significant association between explanatory variables and outcome variables because the prevalence of willingness was greater than 10%. Finally, variables with p ⩽ 0.05 were considered statistically significant, presented by adjusted prevalence ratio (aPR) with corresponding 95% CI.
Results
Socio-demographic characteristics
Of 296 participants screened, 106 were on insulin and were excluded and 190 were eligible. The mean age of the study participants was 55 ± 12.72 years. Most participants were female (63.7%, n = 121), attained a primary level of education (70.0%, n = 133), and were unemployed (84.2%, n = 160). The median household income was 50,000 Ugandan Shillings (UgX) [interquartile range (IQR): 50,000–150,000; 1 USD = 3750 UgX]. In total, 72.5% (n = 132) of the participants earn a monthly household income between 10,000 and 100,000 UgX per month (Table 1).
Socio-demographic characteristics of insulin naïve patients with type 2 diabetes attending diabetes clinic at Gulu Regional Referral Hospital, Gulu, Uganda.

I USD = 3750 Ugandan shillings.
Clinical characteristics
Overall, 38.5% (n = 70) of the participants had diabetes for a period of 1–3 years, 37.0% (n = 70) have had treatment for 1–3 years. In total, 91.0% (n = 122) had hypertension and 8.3% (n = 11) had HIV. For treatment, 70.6% (n = 132) were on a combination of glibenclamide and metformin for DM treatment and 91.7% (n = 121) on high blood pressure treatment. About 37.6% (n = 71) visited the clinic every month and 71.5% (n = 133) had never been advised about insulin (Table 2).
Clinical characteristics of insulin-naïve patients with type 2 diabetes attending diabetes clinic at Gulu Regional Referral Hospital, Gulu, Uganda.

Willingness to start insulin therapy
Overall, 73.4% (n = 138) of the participants were willing to commence insulin therapy if indicated. However, 15.3% (n = 29) were hesitant.
Attitudes toward insulin use
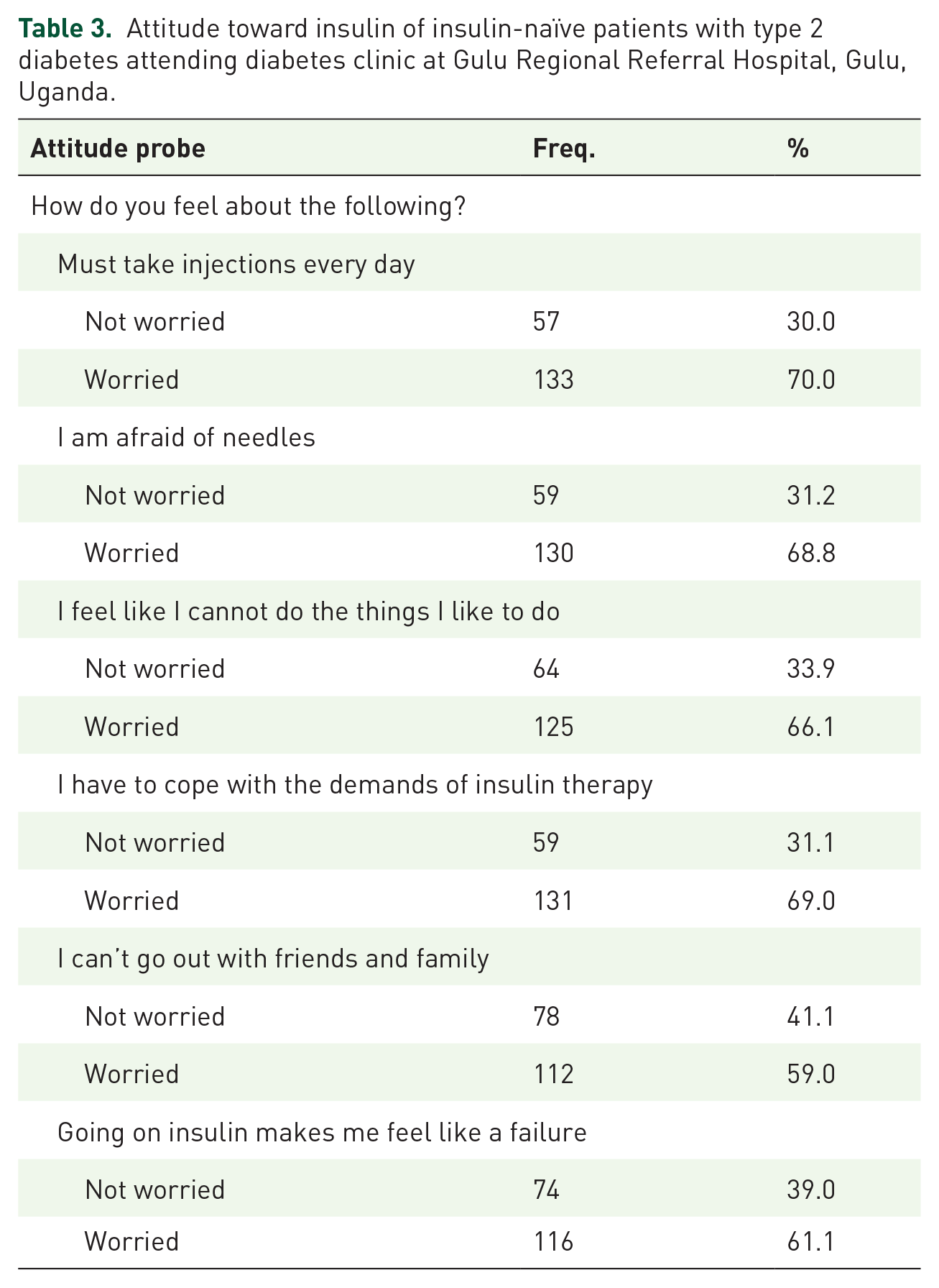
The study participants expressed concerns about receiving daily injections (70.0%, n = 133), fear of needles (n = 130, 68.8%), coping with the demands of insulin therapy (n = 131, 69.0%), and feeling like a failure when starting insulin (n = 116, 61.1%) (Table 3).
Attitude toward insulin of insulin-naïve patients with type 2 diabetes attending diabetes clinic at Gulu Regional Referral Hospital, Gulu, Uganda.
Barriers to insulin use
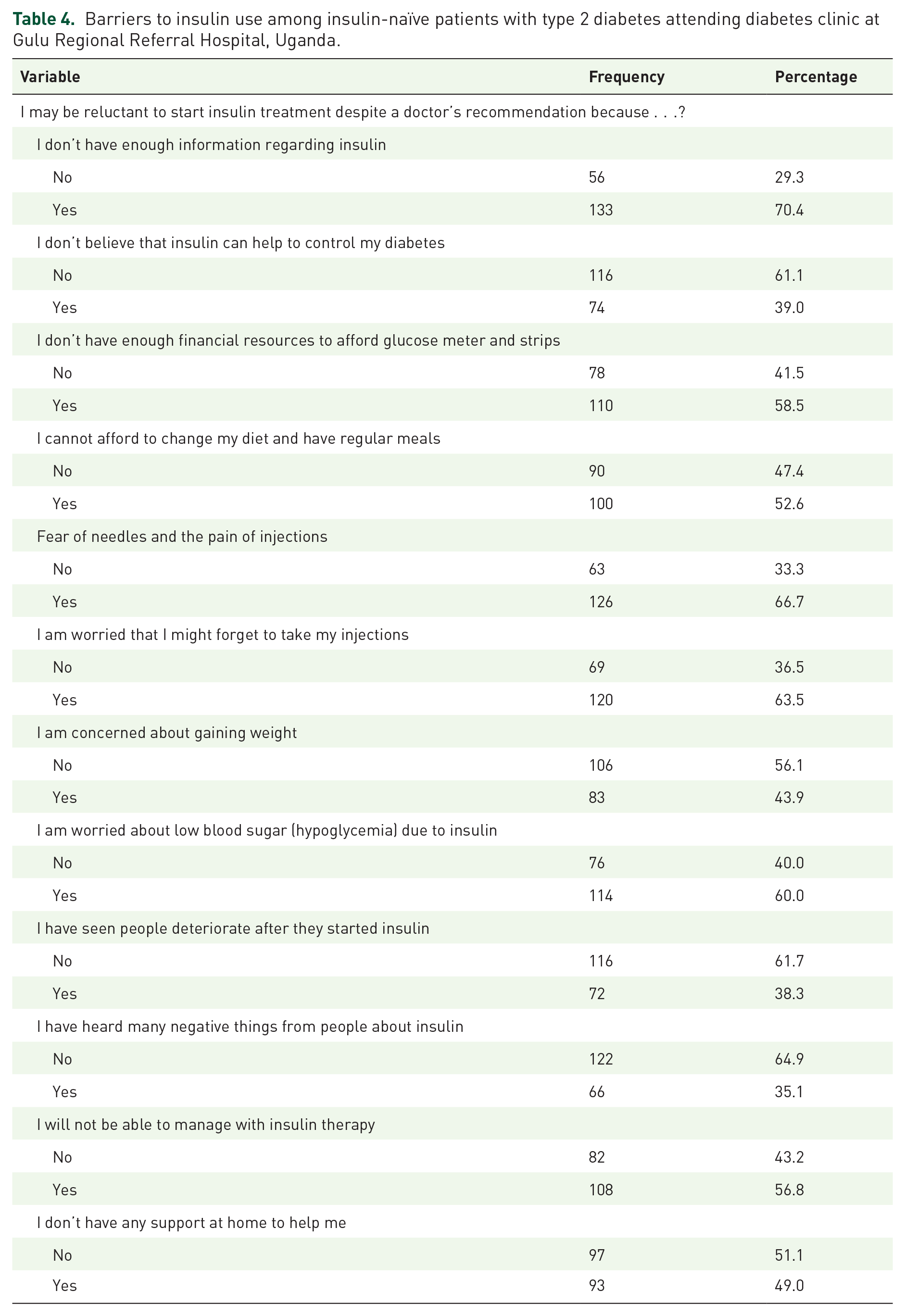
Regarding barriers to insulin use among insulin-naïve DM2 patients who are willing or hesitant to start insulin therapy; 70.4% (n = 133) do not have enough information regarding insulin; 66.7% (n = 126) fear needles and the pain from injections; and 63.5% (n = 120) are worried that they might forget to take the injections (Table 4).
Barriers to insulin use among insulin-naïve patients with type 2 diabetes attending diabetes clinic at Gulu Regional Referral Hospital, Uganda.
Factors associated with willingness to start insulin therapy
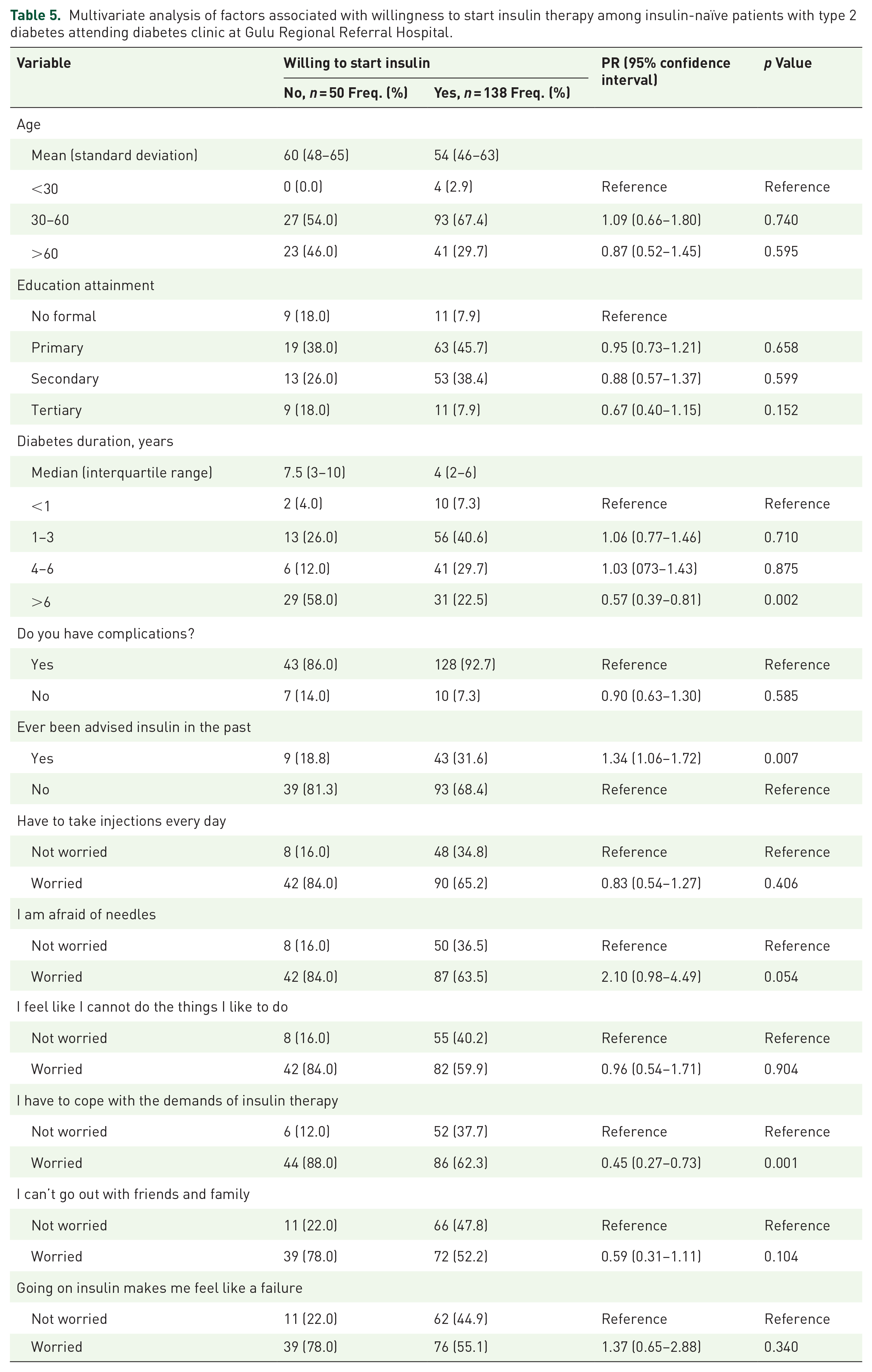
Factors independently associated with willingness to start insulin therapy were diabetes duration of 6 years or more (aPR: 0.57, 95% CI: 0.39–0.81, p = 0.002), those ever been advised recently on insulin (aPR: 1.34, 95% CI: 1.06–1.72, p = 0.007) and those worried about coping up with the demands of insulin therapy (aPR: 0.45, 95% CI: 0.27–0.73, p < 0.001) (Table 5).
Multivariate analysis of factors associated with willingness to start insulin therapy among insulin-naïve patients with type 2 diabetes attending diabetes clinic at Gulu Regional Referral Hospital.
Discussion
The current study investigated the willingness to initiate insulin therapy among insulin-naïve individuals with DM2 at GRRH in Uganda. Our findings indicate that more than three-quarters of participants expressed willingness to commence insulin therapy, with only 15% displaying hesitancy. Furthermore, a longer duration of DM and concerns about coping with insulin therapy were associated with lower willingness, while recent physician advice on insulin was linked to increased willingness. These findings highlight the need for tailored interventions addressing specific concerns to enhance insulin acceptance in this population.
Our observed high willingness to commence insulin in Uganda is in line with a study carried out in South Africa where about 48% of the study participants expressed a willingness to start insulin therapy. 9 In that study, 52% of the participants who were unwilling to start insulin, had negative attitudes, reluctance, injection anxieties, fear of needles, insufficient knowledge of insulin, feeling unable to cope with insulin, and concerns about out-of-pocket costs related to insulin treatment. A study conducted in Iran also showed that more than half of the participants were unwilling to start insulin therapy because they did not have enough knowledge about insulin efficacy and manifested inadequate knowledge about diabetes. 13 Denial of the severity of the disease and denial of the failure of oral agents were the main reasons for refusing insulin therapy among patients. 14
In our study, among the factors independently associated with willingness to start insulin therapy were those ever been advised recently on insulin and those worried about coping with the demands of insulin therapy. Similar findings were obtained in the study from South Africa 9 where the majority of the respondents (84.8%) said that they had never been advised to take insulin. Patients’ belief that injecting insulin is embarrassing was a reason for their delaying initiation of insulin therapy, thus highlighting the importance of injection stigma and how it affects the proper treatment of diabetes. 15 On the other hand, a family history of insulin use increased the patient’s willingness to start insulin. It seems that the presence of another family member using insulin can help overcome the barriers and increase the patient’s willingness to start insulin therapy. 16
We found that a longer duration of DM2 treatment with oral agents was associated with a 34% lower willingness to commence insulin therapy. The difficulties in fulfilling daily responsibilities and difficulties with injecting the right amount of insulin negatively affect motivation to use insulin. According to a study by Abu Hassan et al., 11 about half of the patients with poor control T2DM did not timely start insulin therapy and the initiation was usually 3–5 years after failure of oral hypoglycemic agents. There are many factors influencing delayed insulin initiation including those caused by healthcare providers and its system, as well as the patients themselves. 17
In this study, more than half of the participants could not afford to change their diet and have regular meals. Insulin therapy comes in when there is a proven failure of dietary and lifestyle modifications together with glucose-lowering agents in the achievement of adequate glycemic control. 10 Therefore, the basal insulin dose in conjunction with oral therapy is widely used to initiate insulin therapy, though, even when fasting hyperglycemia is under control, it is necessary to control post-prandial hyperglycemia to achieve target HbA1c levels. 18 According to a study by Bzowyckyj and Begert, 19 the factors that led to therapeutic inertia related to patients’ medication experiences such as the concerns about medication side effects and treatment costs, society-attached stigma, confusion about frequent changes in evidence-based guidelines, low health literacy, and social determinants of health. 12
We also found out that 68% of participants had a fear of needles. Similarly in a study by Abu Hassan et al., 11 majority of participants were reluctant to use insulin due to their negative concerns about insulin injection. This anxiety related to fear of injection pain or needles is very common among diabetics, reported to be more than half among insulin-naïve diabetics; thus, the use of thinner and shorter needles could reduce this fear, making injection less painful. 16 However, a substantial proportion of diabetes patients who were treated with insulin naïve (43%) using thinner needles still admitted ‘Injecting insulin is painful’. 15
One particularly interesting finding of our study was that 70.4% do not have enough information regarding insulin. Similarly, participants with lower compared to higher educational levels had uncertainty about the efficacy of insulin therapy. 15 These findings are based on the fact that patients with low and high education levels had little knowledge about diabetes and its treatment. 9
Our study has some limitations. It was a single-center study, conducted in a regional referral hospital, with a relatively small sample size and findings cannot be generalized to all Ugandan patients with DM2 attending various primary healthcare facilities. This was minimized by carefully selecting a representative sample that adequately reflects the demographic and clinical characteristics of these participants. Future research endeavors should consider longitudinal designs and diverse healthcare settings to validate and expand upon the current findings, providing a more comprehensive understanding of the factors influencing insulin therapy acceptance in individuals with DM2. The high burden of complications of DM2 among the study participants merits further studies into the quality of DM care in this tertiary facility. We also recommend comparative studies investigating glycemic control and rates of complications in primary care facilities compared with our findings from tertiary care settings to further advanced best practices in diabetes care across the lifespan.
Conclusion
In conclusion, we found that over three-quarters of participants demonstrated a willingness to commence insulin therapy, contrasting with only 15% displaying hesitancy. Notably, a longer duration of diabetes and concerns about coping with insulin therapy were associated with diminished willingness, while recent physician advice on insulin correlated with increased willingness. Future interventions should prioritize addressing specific barriers related to prolonged disease duration and apprehensions about insulin therapy to optimize glycemic control in this population.
Supplemental Material
sj-pdf-1-taj-10.1177_20406223241247650 – Supplemental material for Willingness to start insulin therapy among insulin-naïve persons with type 2 diabetes mellitus at Gulu Regional Referral Hospital, Gulu City, Uganda
Supplemental material, sj-pdf-1-taj-10.1177_20406223241247650 for Willingness to start insulin therapy among insulin-naïve persons with type 2 diabetes mellitus at Gulu Regional Referral Hospital, Gulu City, Uganda by Brenda Nakitto, Moses Opedo, Federes Nansubuga, Edward Omondi, Emmanuel Musinguzi, Edwin Cleopas Otile, Steven Ekak, Christine Nannungi, Paska Apiyo, Pebalo Francis Pebolo and Felix Bongomin in Therapeutic Advances in Chronic Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.