
Abstract
Background:
Non-communicable diseases (NCDs) are the leading cause of mortality worldwide, and increasingly so in low- and middle-income countries. Afghanistan is dealing with a double burden of diseases, yet there has been no evidence synthesis on the prevalence of major NCDs and their risk factors.
Objective:
This study aims to provide a comprehensive synthesis of the existing data on the prevalence of major NCDs and the common related risk factors in Afghanistan.
Method:
We systematically reviewed scientific articles from 2000 to 2022 that reported the prevalence of diabetes, chronic respiratory diseases (CRDs), cardiovascular diseases (CVDs) or cancer, and their risk factors in Afghanistan. Four online databases (PubMed, Web of Science, Cochrane and Google Scholar) and two local journals in Afghanistan (not indexed online) were systematically searched and screened. Two reviewers independently screened and appraised the quality of the articles. Data extraction and synthesis were performed using tabulated sheets.
Results:
Among 51 eligible articles, 10 (19.6%) focused on cancer, 10 (19.6%) on diabetes, 4 (7.8%) on CVDs, 4 (7.8%) on CRDs and 23 (45.1%) on risk factors as the primary outcome. Few articles addressed major NCD prevalence; no evidence of CVDs, cancer was 0.15%, asthma ranged between 0.3% and 17.3%, and diabetes was 12%. Pooled prevalence of hypertension and overweight were 31% and 35%, respectively. Central obesity was twice as prevalent in females (76% versus 40%). Similarly, gender differences were observed in smoking and snuff use with prevalence rates of 14% and 25% among males and 2% and 3% among females, respectively. A total of 14% of the population engaged in vigorous activity. Pooled prevalence for physical inactivity, general obesity, fruit and vegetable consumption, dyslipidaemia and alcohol consumption couldn’t be calculated due to the heterogeneity of articles.
Conclusion:
Only little evidence is available on the prevalence of major NCDs in Afghanistan; however, the NCD risk factors are prevalent across the country. The quality of the available data, especially those of the local resources, is poor; therefore, further research should generate reliable evidence in order to inform policymakers on prioritizing interventions for controlling and managing NCDs.
Introduction
Non-communicable diseases (NCDs) pose a significant global health challenge, with 71% of all deaths globally corresponding to 41 million annual deaths. 1 NCDs affect people of any age, religion and nation; however, the burden is higher among older population residing in low- and middle-income countries. NCD-related deaths rose by 5 million between 2006 and 2016 globally. 2
Among many health conditions, almost 80% of premature deaths attributed to NCDs result from four common disease groups: cardiovascular disease (CVD), cancer, diabetes and chronic respiratory diseases (CRDs). 1 Genetic, physiological, environmental, and, most importantly behavioural factors can cause chronic diseases; additionally, population ageing, unhealthy lifestyles, rapid urbanization and globalization are considered to be drivers of NCDs worldwide.1,3
Tobacco consumption is one of the leading risk factors for most NCDs contributing to 7.2 million annual deaths globally. 1 Diet high in saturated fats and processed foods is another major risk factor which results in overweight and obesity and in turn increases the risk of NCDs. 4 In 2017, around 3.9 million global deaths were attributed to eating insufficient fruits and vegetables. 5 Physical inactivity which is an established risk factor for several NCDs has a global prevalence of 21.4% 6 , and according to recent reports of WHO, globally, around 3.2 million deaths and 32.1 million Disability-Ajdsted Life Years (DALYs) are attributable to inadequate physical activity. 7 Moreover, alcohol consumption, in the 2019 Global Burden of Disease Report, was found to have contributed to approximately 320,000 deaths and nearly 10 million DALYs in EU member states. Moreover, metabolic risk factors contribute to around 18 million deaths each year, with hypertension accounting for 9.4 million, overweight and hyperglycaemia each for 3.4 million and hypercholesterolaemia for 2.0 million. 8
The Afghanistan Mortality Survey 2010 showed that NCDs were responsible for 33.3% of all deaths 9 which exceeds the number of deaths caused by war. Some locally conducted studies10–16 have revealed that the prevalence of NCD risk factors, especially the metabolic risk factors, are at alarming levels which will consequently have a significant social, economic and health impact. In Afghanistan, several studies have been conducted on NCDs and/or the common risk factors in small cities, but limited national-level studies exist. The WHO STEP[AQ] survey 2018 is the first and only national survey which provided national-level data on the prevalence of NCD risk factors.
Although several articles were published on NCDs and their associated risk factors in Afghanistan, there is only one systematic review from 2021 which summarized the prevalence of diabetes, and there have been no efforts to consolidate the evidence and synthesize all available NCD data. Hence, to address the data gap, this study aims to provide a comprehensive synthesis of the existing data on the prevalence of major NCDs and the common related risk factors in Afghanistan. The significance of this study lies in addressing a notable gap within the existing literature in Afghanistan. Systematic reviews and meta-analysis play a vital role in synthesizing evidence from diverse studies and providing a holistic overview of a specific research area. By conducting this review, we can provide a comprehensive and up-to-date understanding of major NCDs and their associated risk factors in Afghanistan. The findings of our review which will consolidate the fragmented evidence, will guide evidence-based public health policies and interventions tailored to the needs of the Afghan population.
Methodology
Protocol
A protocol for this study was registered in PROSPERO (Registration No: CRD42022298595).
Study context
This review focuses on Afghanistan, a war-torn country with a low human development index of 0.4 located in South Asia region. 17 As of 2022, the estimated population of Afghanistan was 41,549,080, with a sex ratio of 105.33 males per 100 females. 18 About 26% of Afghans are urbanites, 19 and approximately 43% are under 15 years of age. 20 Afghanistan is divided into 34 provinces and 400 districts. The average literacy rate is 37%, with 52% among males and 24% among females. 21
Despite ongoing efforts, Afghanistan’s health situation remains challenging, with high maternal and child mortality rates, significant malnutrition, a considerable burden of NCDs and overall poor health indicators. Afghanistan is one of only three polio-endemic countries in the world. The National NCD STEP survey (2018), the Afghanistan NCD alliance and the development of a National Strategy for NCDs (2015–2020) are some of the key initiatives for the control and prevention of NCDs in Afghanistan.
Information sources and search strategy
This study followed the PRISMA guidelines for the conduct of systematic reviews and meta-analyses. We searched four online databases (PubMed, Google Scholar, Web of science and Cochrane) from 21 July 2022 to 4 August 2022. A unique approach for this study included searching local journals published in Afghanistan, which are not indexed online. The search terms included the variations of the categories, ‘prevalence’, ‘NCDs’ and ‘Afghanistan’ (Supplemental Appendix 1), with the variations within the categories combined with the Boolean Operator ‘OR’ and the categories themselves combined ‘AND’. For Google Scholar, we first sorted for relevance and then scanned the first 200 search results for eligibility. The literature lists of the included studies were also screened. Two locally published journals (Afghan Medical Journal and Ghazanfar Medical Journal) which are published quarterly were manually searched for relevant articles. We screened the table of contents of all the volumes published since 2000 and kept the abstracts of the relevant articles. We used the EndnoteX9 software (The Endnote Team, Philadelphia, PA) to remove the duplicates and Rayyan 22 to perform the title/abstract screening.
Eligibility criteria
We considered peer-reviewed articles published in English, Persian and Pashtu languages, reporting the prevalence of any of the major NCDs and/or common NCD risk factors in Afghanistan. Since we were concerned with the prevalence, we only included articles with cross-sectional designs. Articles that focused on the Afghan population residing outside the country, studies addressing treatment, prevention, screening, knowledge, complications, management and clinical characteristics of NCDs, and those published before 2000 were excluded. To comprehensively capture the NCD landscape, we included all the relevant articles independent of the participants’ age groups.
Selection process
The first and second authors independently conducted the search, removed duplicates, performed title and abstract screening, and selected articles for full-text review. Conflicts were then discussed with all the authors and resolved accordingly. Included articles underwent quality assessment in duplicate before data extraction and data synthesis.
Data collection process
Tabulated excel sheets were used to extract the data from the specified articles. First reviewer extracted whole data, and all other authors critically reviewed the process and provided suggestions to ensure the accuracy and completeness of the extracted data.
Measurement of the outcome variable
The outcome variable of this study was the prevalence of four major NCDs and common risk factors (e.g., Smoking, physical inactivity, unhealthy diet, hypertension, obesity, dyslipidaemia and other relevant factors).
Data extraction and data items
Data was extracted using excel tabulated forms including the following information: authors and year, title, study aim, sample size, data collection period, study design, main outcome, location and population/setting, methods and measuring equipment, diagnostic criteria, key findings (demographics, prevalence of NCDs and risk factors) and study limitations.
Effect measures
Prevalence rates for all identified outcomes were presented as percentages in the ‘Result’ section.
Quality assessment
Two reviewers independently assessed the quality of articles. We employed the appraisal tool for cross-sectional studies (AXIS) 23 to assess the quality of the articles. The AXIS checklist comprised 20 questions addressing study quality, reporting and key areas such as study aim, design, sample size/sampling frame, target population, measurement validity and reliability, methods, results and limitations.
Data analysis and synthesis
Articles were divided based on their main outcome and different tabulated sheets were used to synthesize the data. Prevalence of major NCDs was narratively synthesized within the four disease categories. Common risk factors were analysed individually, and their prevalence data were reported. We could not calculate the pooled prevalence of major NCDs due to the limited number of population-based articles and the heterogeneity of outcome measures across studies; however, for certain risk factors, we have calculated the pooled prevalence. Initially, risk factors were assessed using the funnel plots in the Stata to identify their eligibility for meta-analysis, and consequently, the pooled prevalences of certain risk factors were calculated using the metaprop command in Stata version 12 (StataCorp, TX, USA). We examined the pooled prevalence of the various risk factors with associated 95% confidence interval (CI) and visualized them using forest plots.
Results
This systematic review adhered to the PRISMA guideline for reporting systematic reviews and meta-analysis. 24
Study selection
A total of 2982 hits were obtained from the online databases and 1036 articles from the local journals. After removal of duplications, we identified 1542 unique articles from online databases of which 98 (6.4%) records were kept after title screening. Subsequently, after abstract screening, 54 (55.1%) articles were kept for eligibility assessment. Similarly, for the local journals, 100 articles were retained after title screening, of which 32 articles remained after abstract screening. Ultimately, a total of 41 online articles and 14 local articles met the eligibility criteria and were included in the full-text review (Figure 1).

Flowchart of included studies (PRISMA-Preferred Reporting Items for Systematic Reviews and Meta-Analysis flow diagram).
Study characteristics
A total of 51 articles fulfilled the inclusion criteria. Of these, 11 (21.5%) exclusively reported the prevalence of major NCDs, 24 (47%) articles reported both disease prevalence and risk factors and 16 (31.3%) articles solely reported the prevalence of at least one risk factor. In terms of primary outcome (as shown in Table 1), 10 (19.6%) articles25–34 focused on cancer, 10 (19.6%)35–44 on diabetes, 4 (7.8%) on CRDs (2 on asthma,45,46 1 on chronic obstructive pulmonary diseases (COPDs) 47 and 1 on chronic bronchitis 48 ) and 4 (7.8%) articles49–52 on CVD. The remaining 23 (45.1%) articles focused on common NCD risk factors, including hypertension (n = 8),53–60 obesity (n = 5),61–65 tobacco use (n = 2)66,67 and a combination of risk factors (n = 8).10,11–16,68
Summary of the characteristics of the included articles.

BMI, Body Mass Index; CS, cross sectional; Gen P, general population; MI, myocardial infarction; NR, Not Reported.
Eight articles (all from the local resources) were written in Persian, and the remaining 43 articles were in English. Only six studies were conducted at national level, while the rest were conducted at the provincial level, mainly in Kabul, Herat, Balkh, Jalalabad and Kandahar cities.
The largest sample size was 238,491 from a national campaign-based survey, 26 while the smallest sample size comprised 57 individuals from a cross-sectional hospital-based study on cancer. 28 Notably, the target population for 19 studies was patients, while the remaining 32 studies were conducted among the general population. In terms of age group, majority of the articles were focusing on adults aged 15–70 years. However, three studies27,45,46 solely focused on children aged less than 12 years and seven studies26,28–30,35,47,68 did not report the age of the participants. Table 1 illustrates/shows the detailed characteristics of included studies.
Quality assessment
The quality of the articles were assessed using the AXIS tool (Supplemental Table – Appendix 2). Majority of the articles (n = 33) scored
Prevalence of major NCDs and risk factors
Major NCDs
We have divided the analysis of prevalence in two sections: one highlighting the prevalence of four major NCDs individually and the other discussing common risk factors’ prevalence.
Cancer
Cancer prevalence in Afghanistan was reported in eight studies (Supplemental Table 2 – Appendix 3). All except one exclusively focused on patients. The highest reported prevalence was 66% for renal cancer in a sample of 160 biopsies, while the lowest was 0.5% for duodenal cancer in a study of 364 patients in northern Afghanistan. From seven hospital-based studies, three reported the prevalence of oesophagus cancer ranging from 2.5% 33 to 25.3%. 32 Stomach cancer prevalence was reported in three articles, reporting 4.8%, 2.4% and 3.6% conducted in Kabul, 29 Mazar-e-Sharif 34 and Jawzjan, 32 respectively. Stratified data in two studies29,33 showed higher cancer prevalence among men. A study with a large sample size of approximately 238,000 participants reported an overall cancer prevalence of 0.15% with breast cancer comprising the highest proportion (33%) and brain cancer the lowest (2.4%). This article further reported on other types of cancer prevalence reporting 17% for stomach cancer, 14% for blood cancer, 5% for liver cancer, 2.9% for oesophagus cancer and 2.4% for cervix and uterine cancer. It is important to note that the study’s quality was suboptimal due to its campaign-based survey nature and reliance on self-reported data. Nonetheless, it provides a rough estimation of cancer types and their prevalence in Afghanistan.
Chronic respiratory diseases
The prevalence of CRDs, was presented in five articles, of which three35,45,46 reported on Asthma and two37,47 reported on COPD. The prevalence of COPD was similar in both articles with rates of 11.3% and 9.8%. Asthma prevalence ranged from 0.3% to 17.3%. The article 35 that reported the prevalence of 0.3% was conducted among adults, while the remaining 2 were conducted among children aged under 14 years. Among children, asthma prevalence was higher in the 13–14 age group (17.3%) compared to the 6–7 age group (12.5%).
Cardiovascular disease
Overall, three articles37,50,54 reported the prevalence of CVDs all conducted on patients. Two articles reported the prevalence of myocardial infarction,37,54 the lower reported at 11.1% in Kandahar province and the higher at 18.8% among hypertensive patients in Faryab province. Only one articles reported the prevalence of ischaemic heart diseases, which presented at 7.7% in Kandahar 37 province. The prevalence of heart failure was also reported in one article, which reported 12.8% among outpatients in Faryab Province. Moreover, one article reported the prevalence of coronary artery diseases at 17.4%, with higher rates among females (20.1% versus 14.9%).
Diabetes, hyperglycaemia
Among 27 articles reporting the prevalence of diabetes, 5 focused on patients and 22 on the general population (Supplemental Table 3 – Appendix 4). Patient-based articles showed comparatively higher diabetes prevalence with the highest 42.8% among H-Pylori-positive patients 51 and the lowest at 11.2% among 555 patients in Faryab province. 52 Among the general population, diabetes prevalence varied from 7.8% in Kabul 31 to 22.4% in Kandahar. 42 The pooled prevalence (Figure 2) of hyperglycaemia calculated from 12 eligible articles was 12% (95% CI: 10–14%). Notably, Kandahar had a higher prevalence of diabetes, with a pooled prevalence of 18% (95% CI: 14–22%).
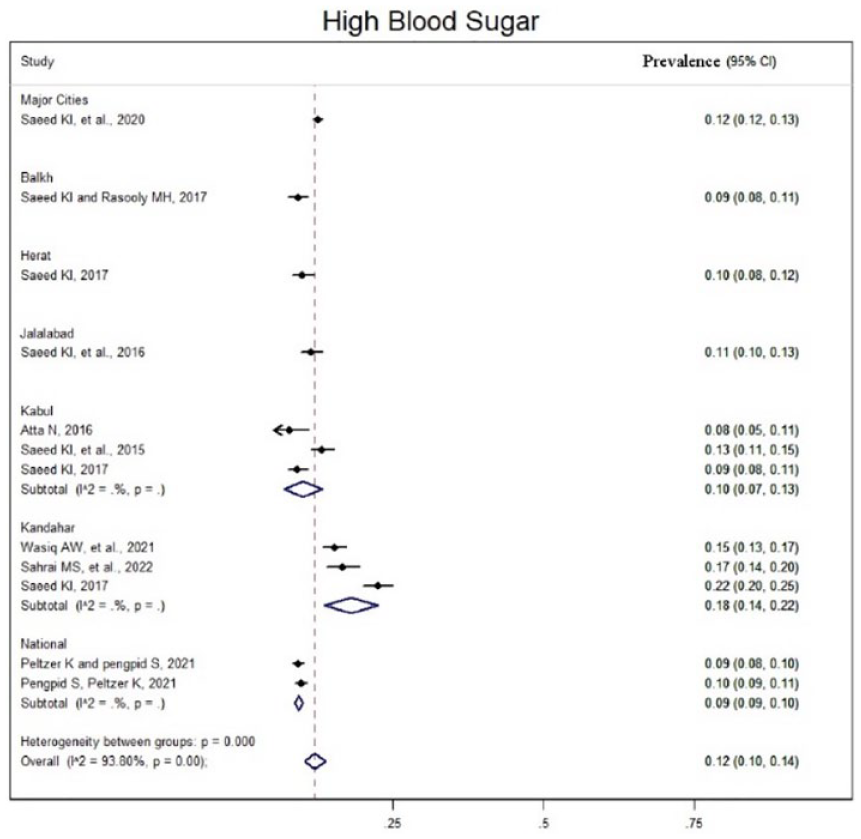
Pooled prevalence of hyperglycaemia by region.
Major risk factors
The majority of articles examined the prevalence of major risk factors, including smoking, physical inactivity, low fruit and vegetable consumption, hypertension and obesity. Notably, snuff consumption, a specific risk factor not commonly reported in other countries, was frequently addressed in included articles. Additionally, some studies reported on dyslipidaemia (elevated cholesterol, high LDL (Low-density lipoprotein), low HDL (High-density lipoprotein) and high triglyceride), family history, type of oil consumption, elevated levels of HbA1c and alcohol consumption.
Smoking
Overall, 38 articles reported the prevalence of smoking from which 10 studies were conducted among patients and 28 among the general population (supplemental Table 4 – Appendix 5). Among patients, smoking prevalence ranged from 8.1% 35 to 46.6% in both reported in Kabul province. 48 Among the general population, smoking prevalence ranged from 5.1% in Kabul in 2013 10 to 28% in a national study in 2021. 62 There was a significant difference in smoking prevalence between nationally conducted studies and those conducted in major cities. The overall pooled prevalence, including national-level data, was 11% (95% CI: 6–16%) (Figure 3), however when stratified by province, the pooled prevalence in national-level data was 25% (95% CI: 21–29%), and for province-level data it was 7% (95% CI: 5–8%). Interestingly, a substantial difference in smoking prevalence was observed between males and females, with a pooled prevalence of 2% (95% CI: 1–3%) in females and 14% (95% CI: 12–16%) in males (Figure 4).

Pooled prevalence of smoking.

Pooled prevalence of smoking by sex.
Snuff use
In total, 29 articles assessed the prevalence of snuff use, with 4 studies conducted among patients and 25 studies among the general population (Supplemental Table 5 – Appendix 6). Patients exhibited higher prevalence of snuff use, often exceeding 30%, compared to the general population. Among the general population, the lowest prevalence was reported in Balkh at 8.3%, 55 while the highest prevalence was observed in Kandahar at 23.6%, followed by Jalalabad. Meta-analysis of 11 articles yielded an overall pooled prevalence of 12% (95% CI: 9–11%) (Figure 5). Sex-specific analysis revealed pooled prevalence of 3% (95% CI: 0.02–0.04) for females and 0.25 (95% CI: 0.18–0.33) for males (Figure 6).
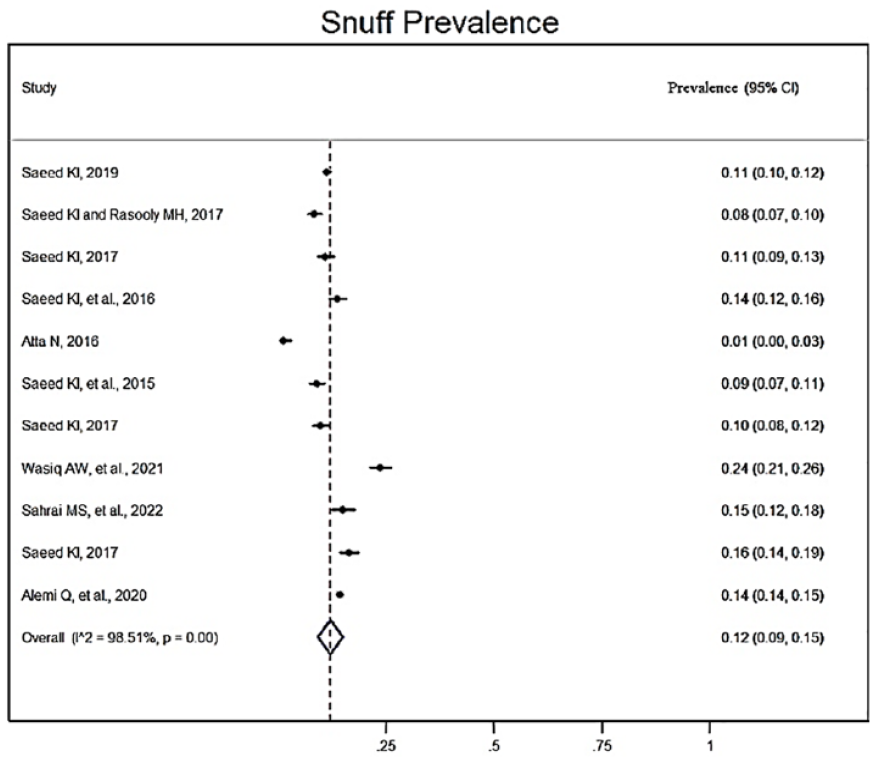
Pooled prevalence of snuff use.

Pooled prevalence of snuff use by sex.
Physical inactivity
Overall, 31 articles reported the prevalence of physical inactivity, with 6 articles focused on patients and 25 on the general population (Supplemental Table 6 – Appendix 7). Overall, there was no significant difference in the prevalence of physical inactivity between these two groups. The highest prevalence was reported at 86.4% in Kabul 65 in 2012 among 1169 individuals aged above 40, while the lowest was 38.4% in a nationwide study 49 conducted in 2021. Eleven articles provided information on the prevalence of physical inactivity stratified by sex showing no significant difference. Jalalabad had relatively low prevalence compared to other provinces. On the other hand, 19 articles reported the prevalence of vigorous activity, ranging from 5.9% in Kandahar in 2016 16 to 35% in Jalalabad in 2014. 44 Vigorous activity was more prevalent among males, as reported in seven articles. In a meta-analysis (Figure 7) of eight articles, the pooled prevalence of vigorous activity was 14% (95% CI: 9–18%).

Pooled prevalence vigorous activity.
Sedentary behaviour
Overall, 16 articles reported on the prevalence of sedentary behaviour (refer to Supplemental Table 7 – Appendix 8). All of the articles were conducted among general population, with two being nationally representative and the remainder conducted in different provinces. Due to variations in the measurement tools used in these studies, it was challenging to reach a meaningful conclusion. Among the 10 articles that measured sedentary behaviour as more than 3 h/day, the prevalence was ranging between 34.8% and 65.1%. Two articles measured it as sedentary time exceeding 8 h/day, and the prevalence was 44% and 48%. The remaining four articles measured it on a weekly basis (more than 30 h/week), and all of them reported a prevalence of 11%.
Alcohol consumption
Excessive alcohol consumption is a global risk factor for NCDs. In Afghanistan, only two studies35,62 reported its prevalence. The percentages were very low: 0.5% in a national sample of 3779 participants 62 and 0% among 321 patients in Kabul. 35
Hypertension
In total, 29 articles (Supplemental Table 8 – Appendix 9) reported hypertension prevalence: 24 among the general population and 5 among patients. Prevalence among the general population ranged from 24.3% (2021) to 46.2% (2014) in Kabul province. The meta-analysis of 14 articles (Figure 8) calculated a pooled prevalence of hypertension at 31% (95% CI: 29–32%). The pooled prevalence was 26% (95% CI: 22–30%) for men and 33% (95% CI: 27–40%) for women (Figure 9). One article 40 focused on diabetes and found that hypertension prevalence was nearly double in diabetics compared to nondiabetics. No tendency towards region was seen in the prevalence.
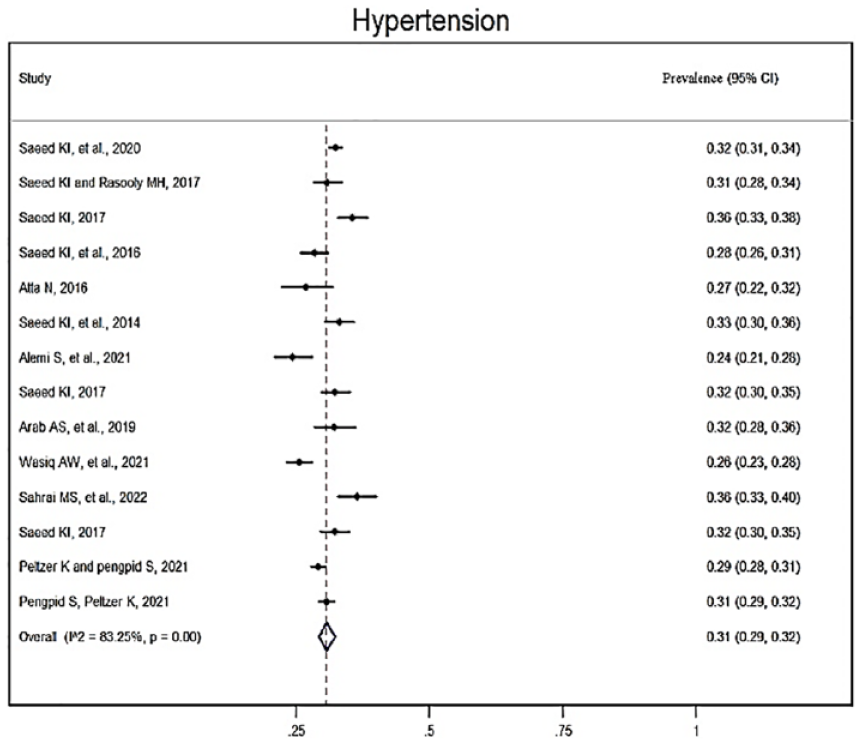
Pooled prevalence of hypertension.

Pooled prevalence of hypertension by sex.
Overweight and obesity
Overweight and obesity were assessed using BMI measurements. In the majority of the articles, individuals were systematically categorized individuals into discrete groups of either overweight or obese based on BMI value. Participants were classified as overweight if their BMI fell within the range of 25 to

Pooled prevalence of overweight.
Further to this, 19 articles also reported on central obesity which is measured as the waist circumference of ⩾94 cm for men and ⩾80 cm for women. The prevalence of central obesity ranged from 50% in Jalalabad (2015) 59 to 67.1% in Kandahar (2021). 36 The pooled prevalence of central obesity was 59% (95% CI: 56–62%). There was a significant difference in the prevalence of central obesity between men and women. Among the six articles reporting the prevalence separately, the pooled prevalence was 76% (95% CI: 71–82%) for females and 40% (95% CI: 33–47%) for males (Figures 11 and 12).

Pooled prevalence of central obesity.

Pooled prevalence of central obesity by sex.
Fruit and vegetable consumption
In total, 26 articles reported the prevalence of inadequate fruit consumption (ranging between 34% and 88.6%) and/or low vegetable consumption (ranging between 19.6% and 71.4%) among the general population (Supplemental Table 10 – Appendix 11). All except three studies reported that over 55% and 40% of individuals consumed fruits and vegetables below the recommended levels. Herat province showed lower fruit and vegetable consumption compared to other provinces.
Lipid profile
In total, 15 articles reported the prevalence of elevated total cholesterol, of which two focused on patients (Supplemental Table 11 – Appendix 12). 11 articles reported on each high triglyceride levels, high LDL levels and low HDL levels. Prevalence of high total cholesterol (
Articles reporting on the prevalence of low HDL indicated a higher prevalence among females.
In summary, the meta-analysis revealed a higher prevalence of certain risk factors for NCDs, which are listed from highest to the lowest in Table 2.
Pooled prevalence of the most common risk factors of NCDs.

NCD, non-communicable diseases.
As shown in Table 2, central obesity emerges as the most prevalent risk factor in Afghanistan, with the pooled prevalence of 59%, followed by overweight and hypertension, each representing 35% and 31%, respectively. The data presented in the table suggests a noteworthy pattern, indicating that metabolic risk factors exhibit significantly higher prevalence compared to behavioural risk factors among Afghan population.
Discussion
This systematic review is the first to examine the prevalence of major NCDs and their associated risk factors in Afghanistan. The inclusion of articles from locally published journals in Afghanistan, despite their low quality, has provided valuable ground data for this review filling a critical gap in knowledge.
One of the major findings of this review is the lack of population-representative data on the prevalence of major NCDs in Afghanistan. The few available articles were confined to local resources with relatively lower quality and solely focused on hospital patients, which hinders their generalizability to the entire population. Consequently, our understanding of the true burden of these diseases remains restricted. The only exception was diabetes, for which population-level data was available. This highlights a significant evidence gap in this area, necessitating further research to accurately estimate the prevalence of major NCDs across the country.
In contrast, the majority of studies in this review were focused on risk factors, which predominantly emerged from the general population. This wealth of empirical evidence provides a realistic depiction of the magnitude of the risk factors in Afghanistan.
Notably, the local resources mostly reflected the prevalence of disease among patients, while studies from online databases focused on risk factors among the general population. This could be attributed to the affiliation of local journals to the medical university, affording of conducting studies within the university hospital setting, thereby facilitating easier access to patients and pertinent data.
We noticed that multiple articles used the same dataset and reported similar rates of risk factors. While all these articles were included in the review, in the meta-analysis, to preserve the real size effect, we only included one article (the most recent or the largest sample sizes) and calculated the pooled prevalence based on unique datasets.
Moreover, during the screening phase, we identified certain articles with diverse study designs, such as case-control and case-series, which reported on the prevalence of some diseases and/or risk factors. However, we exclude these studies from the systematic review due to their inappropriate study design. Nevertheless, we leveraged some of their findings for comparative purposes within our review.
The heterogeneity observed in articles reporting on cancer prevalence and patterns in Afghanistan poses challenges in drawing definitive conclusions. Breast cancer emerged as the most common cancer type, aligning with regional trends in India, 69 Bangladesh 70 and Pakistan, 71 while lung cancer, the second commonest cancer worldwide 72 was absent in the included studies. This could be attributed to the poor quality of articles, failing to accurately estimate proportions of cancer types in Afghanistan.
The prevalence of COPD was reported in two articles, with rates of 9.8% and 11.4% which are comparable to some neighbouring countries such as Pakistan (13.8%), 73 and Bangladesh (9.9%), 74 but are higher than in India 75 and Iran. 76 Similarly, a comparable overall prevalence of 11.1% was reported in a systematic review of South Asian countries. 77
Contradicting trends were observed in asthma prevalence compared to global evidence in terms of age and sex. One study reported a higher prevalence of asthma among girls in the under-five age group, which contradicts the global evidence suggesting the prevalence to be almost twice higher in boys. 78 This highlights the importance of ensuring representative sample sizes to accurately reflect national data and draw more reliable conclusions.
The unavailability of any single article on CVDs among the general population is concerning, given the high prevalence of CVD risk factors in Afghanistan. All available studies on CVD focused solely on patient groups, indicating a significant gap in the literature. Interestingly, an article reported a lower prevalence of heart failure among opium users (however, this article is not included in this review), contradicting many regional and global trends.79–82 Further research is necessary to explore this area and understand the CVD landscape in Afghanistan.
The pooled prevalence of hyperglycaemia was calculated at 12%, which is higher than in countries like India (8.9%), 83 Iran (8.7%) 84 and Bangladesh (7.4 %), 85 but lower than in Sri Lanka and Pakistan with prevalence of 23% 86 and 26.7%. 87 Kandahar province in Afghanistan had the highest pooled prevalence of hyperglycaemia (18%), based on three articles. The reasons for this variation are not clear and could be attributed to differences in diet, lifestyle or genetic factors.
The pooled prevalence of hypertension in Afghanistan was high, presenting at 31%, with women having a higher likelihood compared to men. Limited access to recreational parks and gyms, less engagement in physical activities and higher levels of mental stress as being housewives and spending most of the time at home may contribute to their likelihood of being hypertensive. These findings do not necessarily represent high prevalence of hypertension in the entire country, as the articles mainly focused on urban populations. Rural areas, where people are physically more active and have healthier diets, may exhibit different patterns. A comparable overall prevalence of 28.4% was reported in a systematic review from Nepal, 88 while Iran, Bhutan and Pakistan had lower rates of 25%, 89 17.4% 90 and 26.3%, 91 respectively.
Higher prevalence of overweight, general obesity and central obesity were observed in Kandahar, a southern province. This could be attributed to lower physical activity, as the review indicated that Kandahar had the lowest prevalence of vigorous physical activity. Other factors, such as diet patterns and genetics, may also contribute to these variations. Additionally, central obesity was almost twice as prevalent among females, consistent with global and regional trends,92–94 potentially influenced by biological factors, sedentary lifestyle and sociocultural beliefs.
Alcohol consumption was rarely reported and poorly defined in the reviewed publications. Only two articles provided data on alcohol prevalence and the reported percentages were very low. This low prevalence on one side, aligns with the religious aspect of Afghanistan as a Muslim country; however, on the other hand, cultural and religious beliefs may have introduced information bias, leading to underreporting of alcohol use. It is possible that respondents incorrectly reported non-use due to social stigma and cultural taboos surrounding alcohol in Afghanistan.
The prevalence of smoking among the general population was 11%, which is comparable to India with 10.38%, 95 and Pakistan with 15.2%, 96 but higher than Tajikistan with 2.9%. 97 There was a significant difference in smoking prevalence between males and females, which is in line with regional trends. Social and cultural values play a significant role, as smoking is culturally unacceptable for Afghan women. Interestingly, smoking prevalence was higher among national representative articles compared to those conducted in major cities, concluding higher rates in rural areas compared to urban settings. However, no specific justification can be made for this conclusion; implementation of anti-smoking legislation in different regions may partially explain this finding. Law enforcement may vary across cities and provinces, with urban areas often experiencing stronger implementation compared to rural settings. This variation in the implementation of legislation may potentially contribute to the higher rates of smoking prevalence in rural areas. Parallel to this, the overall prevalence of snuffing was 12%, with significant sex differences. Although snuffing specifically is rarely reported in other studies, smokeless tobacco that includes snuffing, is widely reported in regional studies which are comparable to our findings both in terms of prevalence and sex distribution. Among men, the pooled prevalence of snuff use was 25%, similar to India (36.7%), Nepal (34.8%) and Bangladesh (21.4%). 98 Similarly, among women, the prevalence was 3%, comparable to the Philippines (5.2%), Maldives (4.6%) and Pakistan (4.02%). 98
Fruit and vegetable consumption in Afghanistan was below recommended levels for the majority of the population. More than half of the population did not meet the recommended fruit intake. Although vegetable consumption was relatively higher, overall consumption was still suboptimal. Socioeconomic factors likely contribute to this, as the majority of Afghans are poor and are not able to afford adequate amounts of fruits. Furthermore, urbanization affected the dietary patterns of the people and those living in big cities prefer eating meat and processed foods instead of fruits and vegetables. Additionally, the measurement of fruit and vegetable consumption in the reviewed articles was not well-described. Only the frequency of consumption per week was reported without specifying the exact amount or serving per day. This lack of detail may have led to miscalculations and underreporting. Additionally, it should be noted that the reviewed articles mostly focused on urban populations, potentially leading to underestimation of fruit and vegetable consumption. Rural areas, where agriculture is prevalent may exhibit higher intakes of fruits and vegetables. Therefore, the findings may not represent the dietary habits of the entire population.
Strengths and limitations
This study is novel in including articles from both online and local resources, providing a comprehensive data synthesis. Additionally, various studies were analysed, covering the general population and patient cohorts of all ages, minimizing the likelihood of missing relevant articles. However, low-quality articles, inconsistent measurement methodologies for some risk factors not allowing us to compare, limited data for certain factors, and a potential lack of national representation due to the majority of articles being focused on six main cities in Afghanistan are the key limitations of this review.
Conclusion
In this review, we have identified limited evidence on the prevalence of major NCDs in Afghanistan; however, the presence of risk factors for NCDs is widespread throughout the country. Prevalent factors include overweight and obesity, hypertension, unhealthy diet and physical inactivity. Based on these findings, we strongly recommend policymakers and international donors to increase investment in healthcare infrastructure, especially in rural areas, for effective NCD diagnosis and control. Conducting health promotion campaigns to promote healthy lifestyle is also strongly advised. Moreover, recognizing the low quality of the available data, especially those of the local resources, additional research is imperative to generate reliable evidence that can inform policymakers on prioritizing interventions for NCD control and management in Afghanistan. We advocate for the prioritization of comprehensive and nationally representative surveys to understand the prevalence of major NCDs in diverse regions, and inform targeted interventions. Additionally, healthcare providers are urged to integrate different health components into NCD prevention programmes, including nutrition education mental health aspects, to promote healthy lifestyle.
Supplemental Material
sj-docx-1-taj-10.1177_20406223241229850 – Supplemental material for Prevalence of major non-communicable diseases and their associated risk factors in Afghanistan: a systematic review and meta-analysis
Supplemental material, sj-docx-1-taj-10.1177_20406223241229850 for Prevalence of major non-communicable diseases and their associated risk factors in Afghanistan: a systematic review and meta-analysis by Ahmad Siyar Noormal, Volker Winkler, Sneha Bansi Bhusari, Olaf Horstick, Valérie R. Louis, Andreas Deckert, Khatia Antia, Zahia Wasko, Pratima Rai, Aline Frare Mocruha and Peter Dambach in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
We would like to express our gratitude to the Heidelberg Graduate School of Global Health for their invaluable support throughout the review process. Additionally, we extend our appreciation to Dr. Shinkay Noormal, professor at Kabul Medical University for their tireless efforts and assistance in searching and collecting articles from the local journals.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.