
Abstract
Background:
Metformin is a potent antiglycemic agent, but its importance has receded owing to the launch of novel antidiabetic medications. The benefit of metformin includes not only blood sugar control but also anti-inflammation, autophagy activation, and neuroprotection. This study investigated the risk of cardiovascular disease (CVD) in people with type II diabetes mellitus (T2DM) who adhered to metformin after adding on a second-line antiglycemic agent.
Objectives:
The purpose of this study was to investigate the benefits of metformin in CVD prevention in patients with T2DM.
Design:
We designed the study by comparing the incident rate of CVD events in patients with T2DM who received metformin continually and who ceased metformin during 2002–2014.
Methods:
Medical information was obtained from the National Health Insurance Research Database, and patients with T2DM receiving second-line antiglycemic agents were categorized into metformin-adherent and nonadherent groups according to prescription claims. The study outcomes were the incidence of CVD hospitalization, including stroke (ischemic and hemorrhagic) and myocardial infarction (MI).
Results:
A total of 31,384 patients with T2DM constituted the metformin-adherent group and were 1:1 matched to nonadherent patients. Metformin adherence was associated with a lower risk of hospitalization due to stroke [adjusted hazard ratio (aHR) = 0.51, 95% confidence interval (CI): 0.43–0.59, p < 0.001] and MI (aHR = 0.47, 95% CI: 0.43–0.53, p < 0.001). The risk reduction persisted in both ischemic and hemorrhagic strokes. Our subgroup analysis revealed that the protective effect on stroke and MI hospitalization persisted in metformin-adherent patients, both sexes, patients aged ⩽65 or >65 years, and patients with or without concurrent insulin treatment.
Conclusions:
This study revealed that metformin adherence in patients with T2DM who required a first-line treatment may reduce the risk of subsequent CVD. Despite the availability of numerous novel antiglycemic agents, metformin adherence by patients who require a combination of antiglycemic agents provides an additional benefit of CVD protection.
Introduction
Cardiovascular disease (CVD) is a leading cause of death globally. Approximately 17.9 million people died of CVD in 2019, representing 32% of all global deaths. 1 CVD, including stroke, myocardial infarction (MI), and ischemic heart disease (IHD), is a significant complication of type II diabetes mellitus (T2DM). It is caused in T2DM by complex alterations of coronary endothelial dysfunction and atherosclerotic plaque instability and rupture, as by multivessel coronary stenosis. CVD is strongly associated with poor life quality and poor glycemic control in people with diabetes mellitus (DM), which further increases the recurrence of CVD in a vicious cycle. 2
Metformin, a biguanide derivative, has been recommended as the first-line therapy for T2DM since the 1950s because of its potent glucose-lowering effect, affordable cost, and safety. Metformin lowers blood glucose by suppressing hepatic gluconeogenesis and increases peripheral tissue insulin sensitivity without causing severe hypoglycemia. 3 Studies have revealed that metformin not only demonstrates a hypoglycemic effect in T2DM but also lowers the risk of CVD in nondiabetic patients. 4 These effects may be due to the modification of CVD risk factors such as obesity, dyslipidemia, and hypertension. Recent studies have also revealed that metformin may modulate mitochondrial oxidative phosphorylation and prevent intracellular calcium dyshomeostasis in cardiovascular tissues, both of which are crucial for the atherosclerotic process. 5 Furthermore, metformin may activate the cellular energy sensor Adenosine monophosphate (AMP)-activated protein kinase–mammalian target of rapamycin (mTOR) pathway to promote autophagy and prevent atherosclerosis. 6 Metformin also plays a regulative role in patients with T2DM with stable IHD by reducing coronary endothelial dysfunction. 7 Another study also indicated that metformin may reduce inflammatory tone and leptin-to-adiponectin ratio in pericoronary fat such as in those prediabetic patients with acute MI. 8
Novel antidiabetic medications have emerged during the 21st century, such as glucagon-like peptide 1 (GLP-1) receptor agonists and dipeptidyl peptidase 4 (DPP-4) inhibitors, which, similar to metformin, may reduce blood glucose with low risk of hypoglycemia. 9 Currently, multiple treatment choices are available for T2DM and involve different strategies for the management of blood sugar, and the role of metformin is being relegated by these novel agents. However, metformin may provide further benefits beyond lowering blood glucose for patients with DM; for instance, according to some observational studies, it reduced the risk of dementia in patients with DM.10,11
Pericoronary fat overinflammation might lead to the development and destabilization of coronary plaque in patients with prediabetes. Moreover, recent studies also showed that pericoronary fat may overexpress sodium-glucose cotransporter 2 (SGLT2) and leptin. In patients with acute myocardial infarction (AMI), and explicitly investigating at the level of pericoronary fat, the metformin works in regulating the expression of SGLT2 pathways 12 and the expression of inflammatory cytokines/cells, thus leading to improvement of clinical symptoms.
Obese prediabetic patients overexpress cytokines that influence myocardial function via microRNA (miR) expression, and recent studies compared metformin with placebo in obese patients. Metformin significantly reduces inflammation/oxidative stress, and miR-195 and miR-27 cause reduction in intima–media thickness (IMT) and left ventricular mass (LVM). 13 The superficial adipose tissue expresses cytokines, and sirtuins in obese patients may affect myocardial function. Celestino Sardu and his colleagues found that metformin therapy may reduce inflammation and oxidative stress by reducing cholesterol and triglycerides and significantly reducing inflammatory markers, which may be associated with ameliorating myocardial performance. 14
We hypothesized that metformin exerts beneficial effects on CVD, including stroke (ischemic and hemorrhagic) and MI. Therefore, using data from real-world settings, we conducted a population-based retrospective cohort study to investigate the association of metformin adherence with the risk of CVD in patients with T2DM requiring second-line treatment after metformin.
Method
Data source
Data were obtained from the National Health Insurance Research Database (NHIRD), which is maintained by the National Health Insurance Administration (NHIA) of Taiwan. The NHIRD is a nationwide claims-based database of those insured under the National Health Insurance (NHI) scheme, which is a compulsory insurance program that has provided coverage for most healthcare services in Taiwan and nearly 30,000 prescription medications since 1995. The NHIRD includes inpatient, outpatient, and pharmaceutical claims and disease diagnoses coded according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), and (after 2016) ICD-10-CM. To verify the accuracy of diagnoses and treatment rationales, the NHIA routinely samples a portion of the NHI claims and penalizes hospitals and clinics if it ascertains that unnecessary medical treatment has been provided. 15
Characteristic of the study
This study was an observational cohort study and the report of this study followed the suggestions of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist.
Study population
Patients diagnosed as having DM were defined as those who had diagnostic claims (ICD-9-CM: 250) and prescription claims for metformin [Anatomical Therapeutic Chemical (ATC): A10BA02] alone in the first place and added other oral antidiabetic drugs or insulin between 2002 and 2014. We divided the included patients into two groups: those who adhered to metformin (metformin-adherent group) and those who did not adhere (nonadherent group, discontinued metformin after adding on other antidiabetic agents) during the follow-up period.
Patients were excluded from the study if they were aged <18 years; their sex information was missing; or they had type I DM, pregnancy, or chronic kidney disease history (contraindicated to metformin) during the study period. We further excluded patients who used only metformin because we intended to enroll patients receiving second-line therapy in addition to metformin. We also excluded patients with a medication possession ratio (MPR) of <40. The date of discontinuation of metformin was regarded as the index date. Because the metformin-adherent group did not have a date of discontinuation, a pseudo-index date was randomly assigned. Subsequently, to minimize the confounding of underlying diseases, we excluded patients who had a history of stroke hospitalization, dementia, Parkinson’s disease, polyneuropathy, retinal disease, or vascular events such as MI and peripheral arterial occlusion disease before the index date. Patients who died within 1 year of follow-up were also excluded. Finally, each metformin-adherent patient was matched with a nonadherent patient through propensity score matching (PSM) using a caliper width of 0.2, to select two comparable groups with similar baseline characteristics but differences in treatment status (here is metformin adherence). Consequently, both cohorts had similar baseline characteristics but differed in metformin adherence. The propensity score was calculated on the basis of sex, age, year of DM diagnosis, and year of metformin prescription.
Study outcome
The metformin-adherent patients and nonadherent patients were followed up to determine their risk of CVD (stroke hospitalization, MI hospitalization, hemorrhagic stroke, and ischemic stroke). To ensure the validity of diagnoses, we defined stroke hospitalization as ICD-9-CM diagnostic codes 431–436 plus neuroimaging (computer tomography or magnetic resonance imaging) during the course of hospitalization. A validation study showed that the positive predictive value (PPV) and sensitivity of diagnosis of stroke on inpatient claims data were both high. 16 We defined MI hospitalization as ICD-9-CM diagnostic codes 410–414 plus prescription of antiplatelet agents (ATC code: B01AC). The end of the observation period was the date of the first CVD event, the date of death, or 31 December 2018, whichever came first.
Statistical analysis
Baseline characteristics were analyzed using the standardized mean difference (SMD). An SMD of ⩾0.1 indicated non-negligible differences between the two groups. Conditional Cox proportional hazards regression was used to evaluate the risk of stroke hospitalization and MI hospitalization. All analyses were performed using SAS/STAT software (version 9.4; SAS Institute Inc., Cary, NC, USA). A value of p < 0.05 was considered statistically significant.
Results
Initially, we identified 1,545,669 patients with DM. After exclusion criteria and PSM were applied, 31,384 patients with T2DM were included in each of the metformin-adherent and nonadherent groups (Supplemental Figure 1). The mean age was 55.2 ± 9.64 years, and 56.3% of the patients in both groups were men. The mean follow-up period was 5.24 ± 2.78 years for the adherent group and 5.04 ± 2.65 years for the nonadherent group (Table 1).
Demographic data of matched metformin-adherent and nonadherent patients with type II diabetes mellitus.

ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CABG, coronary artery bypass graft; CCB, calcium channel blocker; DM, diabetes mellitus; DPP-4, dipeptidyl peptidase 4; MPR, medication possession ratio; SMD, standardized mean difference; TZD, thiazolidinedione.
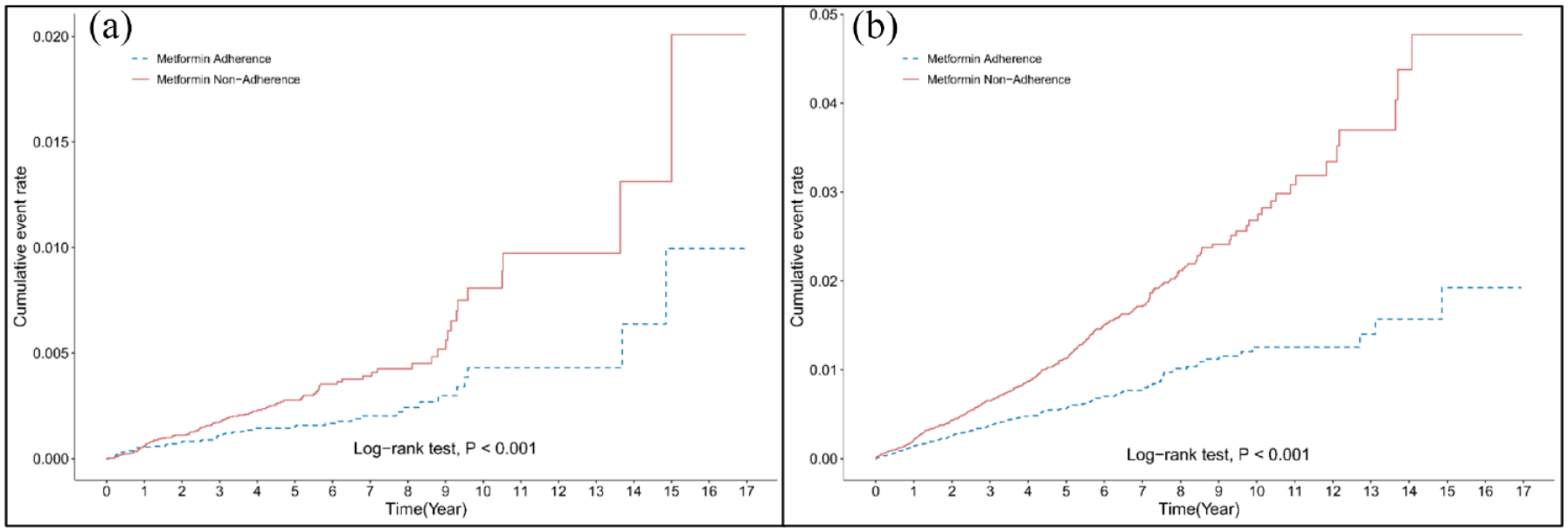
During the follow-up period, the incidence rate of stroke hospitalization was 1.69 [95% confidence interval (CI): 1.50–1.90] per 1000 person-years (PY) in the adherent group and 3.36 (95% CI: 3.08–3.66) per 1000 PY in the nonadherent group. The metformin-adherent group exhibited a low risk of stroke hospitalization, with the adjusted hazard ratio (aHR) being 0.51 [95% CI: 0.43–0.59, p < 0.001; Figure 1(a)] with the adjustment of age, sex, presence of atrial fibrillation, hypertension, hyperlipidemia, history of coronary artery bypass graft (CABG) surgery, concurrent antiglycemic agents, antiplatelet agents, and antihypertensive agents. On further classification of the stroke into the hemorrhagic and ischemic stroke, the incidence of hemorrhagic stroke was 0.33 (95% CI: 0.25–0.43) and 0.61 (95% CI: 0.50–0.75) per 1000 PY in the metformin-adherent and nonadherent groups, respectively [aHR = 0.55, 95% CI: 0.39–0.78, p = 0.001; Figure 1(b)]. The incidence of ischemic stroke was 1.18 per 1000 PY in the adherent group (95% CI: 1.02–1.36) and 2.44 per 1000 PY in the nonadherent group (95% CI: 2.21–2.70), with the aHR being 0.48 [95% CI: 0.40–0.57, p < 0.001; Figure 2(a)]. In the analysis of MI hospitalization outcome, the incidence of MI was 3.68 in the metformin-adherent group (95% CI: 3.40–3.99) and 7.63 in the nonadherent group (95% CI: 7.20–8.07), with the aHR being 0.47 [95% CI: 0.43–0.53, p < 0.001; Figure 2(b)]. During the follow-up, it was also noticed that the metformin adherence group had a lower risk of hospitalization due to heart failure (aHR: 0.26, 95% CI: 0.22–0.31, p < 0.001), hospitalization due to lactic acidosis (aHR: 0.18, 95% CI: 0.11–0.29, p < 0.001), and hospitalization for glycemic control (aHR: 0.23, 95% CI: 0.20–0.27, p < 0.001) (Table 2).

Kaplan–Meier failure curves of the cumulative risk of (a) stroke hospitalization and (b) myocardial infarction hospitalization for metformin-adherent and nonadherent patients with type II diabetes mellitus.
Kaplan–Meier failure curves of the cumulative risk of (a) hemorrhagic stroke hospitalization and (b) ischemic stroke hospitalization for metformin-adherent and nonadherent patients with type II diabetes mellitus.
The incidence (per 1000 PY) and adjusted HR of vascular events after PSM.

CI, confidence interval; HR, hazard ratio; MI, myocardial infarction; PSM, propensity score matching; PY, person-years.
The results of the subgroup analysis revealed that metformin adherence was associated with a lower risk of stroke hospitalization in patients aged ⩽65 or >65 years, both sexes, patients with and without hyperlipidemia, and patients concurrently receiving insulin, sulfonylurea or DPP-4 inhibitors. The association between decreased risk of stroke hospitalization and metformin adherence was not significant in patients with atrial fibrillation, patients without hypertension, and patients concurrently receiving thiazolidinediones (TZDs). Reduced risk of MI hospitalization was associated with metformin adherence in all conditions of the subgroup analysis (Figure 3(a) and (b)).

Forest plot showing the hazard ratios of stroke hospitalization (a) and MI hospitalization (b) in different comorbidities in metformin-adherent and nonadherent patients with type II diabetes mellitus.
Discussion
The results of this study reveal that patients with T2DM who adhered to metformin after receiving combined medication treatments had a significantly lower risk of CVD events, including stroke and MI hospitalization, during the follow-up period than did the nonadherent patients. This association was also observed in hemorrhagic and ischemic strokes. Furthermore, metformin adherence reduced the risk of stroke and MI hospitalization in patients aged ⩽65 or >65 years and in both sexes. This association was significant in patients with and without concurrent insulin, sulfonylurea, or DPP-4 inhibitor treatment, suggesting that the beneficial effect was not affected by other antiglycemic agents.
Whether metformin reduces the risk of CVD remains controversial. Some studies have reported that a metformin-containing regimen reduced the risk of stroke 17 and MI.18,19 However, the protective effect of metformin on CVD cannot be explained solely by glycemic control. 20 In vivo studies have demonstrated that metformin reduces the formation of atherosclerotic plaque, which may be due to the reduction of serum high-sensitivity C-reactive protein and inhibition of inflammatory changes in the vascular wall. 21 Furthermore, metformin reduces the calcification of atherosclerotic plaque, which is crucial for plaque stability, hence the risk of atherosclerotic vascular occlusion. 22 Metformin is also known to inhibit lipid deposition in plaque-laden macrophages. 23 However, a large-scale meta-analysis failed to demonstrate protection, and substantial heterogenicity was observed. CVD protection may be limited to patients with specific characteristics such as older age, effective glycemic control, and non-White ethnicity. 24 This study investigated patients with T2DM in the NHIRD, which includes more than 99% of the Taiwanese population, meaning nearly all categories of patients with DM were covered, except for those with contraindications to metformin and poor drug compliance (MPR < 40%). Furthermore, instead of comparing patients exposed to metformin with those not exposed, we focused on patients with moderate to advanced T2DM who adhered to metformin while receiving at least one other antiglycemic agent. The protective effect of metformin adherence on CVD suggests the benefit of a metformin-containing regimen to patients with DM receiving a second-line treatment, which probably extends beyond the glucose-lowering effect.
Novel antidiabetic medications, including DPP-4 inhibitors and GLP-1 agonists, exhibit potent glucose-lowering effects. 9 In addition, multiple studies have demonstrated the benefit of these medications to CVD outcomes.25–28 The latest guidelines have also replaced metformin with this class of medications in patients with DM who have CVD or are at a high risk of CVD, 29 further weakening the relevance of metformin in CVD prevention. This study presents population-based evidence that metformin provides CVD protection in patients with T2DM, which suggests that adherence to metformin while using another antiglycemic agent is required to retain this protective effect. Besides, the reduced risk of metformin adherence to CVD remained among patients with concurrent treatment of sulfonylureas and DPP-4 inhibitors, and this phenomenon faded away only for patients with concurrent treatment of TZDs. Because both metformin and TZDs work on increasing insulin sensitivity, some interactions may need further study.
The strength of this study is the comparison between metformin adherence and nonadherence in patients with T2DM who were receiving second-line therapy. Adherence to a metformin-containing regimen provided a protective effect from CVD; nonadherent patients did not demonstrate this effect. This prevents bias resulting from comparing metformin users with those who were not prescribed metformin owing to contraindications. This finding may be useful for clinicians when they need to prescribe add-on second-line treatments for glycemic control. This study also has a few limitations. First, the NHIRD lacks information about body weight, lifestyle, and details of glycemic control, such as glycosylated hemoglobin levels. To compensate for these limitations, we excluded patients with T2DM with severe diabetic complications to avoid bias from people who already have severe underlying disease or diabetic complications, which undermined the generalizability of this study. On the other hand, we used PSM to match disease duration, age, sex, comorbidity, and compliance by MPR. Second, information about interactions between metformin and DPP-4 inhibitors or GLP-1 agonists was unavailable. Although we enrolled patients with DM between 2004 and 2014, who used metformin, the prescription of these two classes of drugs was not common during this period. We also conducted a subgroup analysis of concurrent insulin therapy, an indicator of greater DM severity, which addressed the possible confounding effects of the interaction between metformin CVD protection and the severity of DM. Finally, it was one of the limitations that the calculation of the sample size before the conduction of the study was not performed. As a population-based study, all participants who fulfilled the selection criteria were included in the analysis, so the calculation was omitted.
Conclusion
This study revealed that metformin adherence reduced the risk of CVD events, including stroke and MI hospitalization, in patients with T2DM. The benefit persisted in both sexes, patients aged ⩽65 or >65 years, and people receiving concurrent insulin therapy. Metformin may provide not only antiglycemic effects but also CVD protection, which is noteworthy despite the availability of numerous novel antiglycemic agents.
Supplemental Material
sj-docx-1-taj-10.1177_20406223231163115 – Supplemental material for Metformin adherence and the risk of cardiovascular disease: a population-based cohort study
Supplemental material, sj-docx-1-taj-10.1177_20406223231163115 for Metformin adherence and the risk of cardiovascular disease: a population-based cohort study by Shun-Fan Yu, Chien-Tai Hong, Wan-Ting Chen, Lung Chan and Li-Nien Chien in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
The authors acknowledge the statistical and computational support of the Health Data Analytics and Statistics Center, Office of Data Science, Taipei Medical University, Taiwan.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.