
Abstract
Background:
Metabolic-associated fatty liver disease (MAFLD) has become an important cause of liver cancer. The current understanding of MAFLD-related liver cancer is not sufficient, however.
Objective:
The objective of this study was to investigate the clinical and metabolic characteristics of inpatients with MAFLD-related liver cancer.
Design:
This is a cross-sectional investigation.
Methods:
An investigation was conducted to collect the cases of hepatic malignant tumor hospitalized in Beijing Ditan Hospital, Capital Medical University from 1 January 2010 to December 31 2019. The basic information, medical history, laboratory examination results, and imaging examination results of 273 patients diagnosed with MAFLD-related liver cancer were recorded. The general information and metabolic characteristics of patients with MAFLD-related liver cancer were analyzed.
Results:
In total, 5958 patients were diagnosed with hepatic malignant tumor. Among them, liver cancer due to other causes accounted for 6.19% (369/5958), MAFLD-related liver cancer was diagnosed in 273 cases of them. From 2010 to 2019, MAFLD-related liver cancer showed an increasing trend. Among 273 patients with MAFLD-related liver cancer, 60.07% were male, 66.30% were ⩾60 years old, and 43.22% had cirrhosis. The 273 patients were comprised by 38 patients with evidence of fatty liver and 235 patients without evidence of fatty liver. There was no significant difference in the proportions of sex, age, overweight/obesity, type 2 diabetes, and the presence of ⩾2 metabolic-related factors between the two groups. In the group without evidence of fatty liver, 47.23% patients had cirrhosis, which was significantly higher than 18.42% in the group with evidence of fatty liver (p < 0.001).
Conclusion:
MAFLD-related liver cancer should be considered in liver cancer patients with metabolic risk factors. Half of MAFLD-related liver cancer occurred in the absence of cirrhosis.
Introduction
Liver cancer is one of the most common malignancies in the world and the most common cause of death in patients with chronic liver disease.1–3 In 2020, the incidence of primary liver cancer in China ranked fifth among malignant tumors and second among causes of cancer death. 2 With the increasing incidence of obesity, type 2 diabetes, and metabolic syndrome, metabolic-associated fatty liver disease (MAFLD) has gradually become the main cause of liver diseases worldwide, and MAFLD has also become an important cause of liver cancer.4–6 This creates a severe economic burden on health and leads to a decline in health-related quality of life.7,8 The current understanding of MAFLD-related liver cancer, however, is not sufficient, and the diagnosis is controversial. 9 MAFLD differs from other common causes of liver cancer, such as chronic viral hepatitis and alcoholic liver disease (ALD), in that there are no simple, highly effective therapies directed against MAFLD. There is also no simple consistent way to diagnose MAFLD in patients with cirrhosis and hepatocellular carcinoma (HCC) because MAFLD may have ‘burned out’, with hepatic steatosis no longer evident in advanced stage. Most previous studies on MAFLD/non-alcoholic fatty liver disease (NAFLD)–related liver cancer were cohort studies with clear past medical history. In clinical practice, it is difficult for many patients to provide an accurate medical history of MAFLD, which may lead to serious underestimation of MAFLD-related liver cancer.
Previous cohort studies in Europe and the United States have shown that the incidence of liver cancer in NAFLD patients without cirrhosis is not low 10 and the risk of liver cancer is increased in men and diabetic patients. 11 At present, there are not many data on NAFLD/MAFLD-related HCC in Chinese patients. As reported herein, a cross-sectional study was conducted on MAFLD-related liver cancer admitted to Beijing Ditan Hospital, Capital Medical University. We attempted to diagnose MAFLD-related liver cancer based on the presence of metabolic abnormalities, including overweight/obesity, type 2 diabetes mellitus, hypertension, and hyperlipidemia and analyze the clinical and metabolic characteristics of these patients using hospital medical record.
Materials and methods
Study design
We conducted a single-center cross-sectional study. Using the hospital medical record information management system, version 5.20, patients diagnosed with hepatic malignant tumor hospitalized in Beijing Ditan Hospital, Capital Medical University from 1 January 2010 to 31 December 2019 were queried. According to the International Statistical Classification of Diseases and Related Health Problems–Tenth Edition (ICD-10) code 12 on the first page of the medical records, viral hepatitis B15–B19, including common hepatotropic hepatitis and nonhepatotropic hepatitis, was classified. Liver diseases K70–K77 include ALD, drug-induced liver injury (DILI), NAFLD, autoimmune liver disease (AILD), liver failure, chronic hepatitis, liver fibrosis and hardening, other diseases of the liver, and so on. Liver tumors, C22.0–C22.9, include HCC, intrahepatic cholangiocarcinoma, benign liver tumors, and so on. Patients with the same main diagnosis and repeated admission were counted as 1 person.
Basic information and medical history, laboratory examination results, and imaging examination results were recorded for the enrolled patients, focus on metabolism-related risk factors, including overweight/obesity, type 2 diabetes, hypertension, blood triglyceride level of ⩾1.70 mmol/l, high-density lipoprotein cholesterol (HDL-C) levels of <1.0 mmol/l in males and 1.3 mmol/l in females, and prediabetes.
Study population
A total of 5958 patients diagnosed with hepatic malignant tumor hospitalized in Beijing Ditan Hospital, Capital Medical University from January 2010 to December 2019 were queried, including 4617 cases of hepatitis B virus (HBV)–related liver cancer, 407 cases of hepatitis C virus (HCV)-related liver cancer, and 249 cases of alcoholic-liver-disease-related liver cancer. There were 43 cases of autoimmune liver cancer, 239 cases of secondary malignant tumor, 34 cases of HBV + HCV–related liver cancer, and 369 cases of liver cancer due to other causes. Among the 369 patients, 273 patients met the diagnostic criteria of MAFLD. These patients were diagnosed with MAFLD-related liver cancer, excluded participants with other etiologies of liver disease, such as viral hepatitis, ALD, autoimmune diseases, and hepatic metastatic carcinoma. MAFLD was diagnosed based on any of the following: body mass index (BMI) ⩾23, type 2 diabetes mellitus, or two or more of four metabolic-related factors (hypertension, blood triglyceride level of ⩾1.70 mmol/l, HDL-C levels of <1.0 mmol/l in males and 1.3 mmol/l in females, and prediabetes). A total of 38 patients also had fatty liver, 235 patients showed no fatty liver on imaging, histopathological examination of liver, and whether they had a history of fatty liver was unknown, but metabolic abnormality–related factors were present (Figure 1).

Flowchart of study participants.
Statistical analysis
SAS 9.2 statistical software was used for data analysis, the mean value ± standard deviation was used for statistical descriptions of age, analysis of variance was used for inter-group comparisons, and the Student–Newman–Keuls (SNK) test was used for inter-group comparisons. Data on sex and liver disease spectrum in different years were described by the frequency and composition ratio, and p < 0.05 was considered to indicate a statistically significant difference.
Results
Analysis of the etiological composition of inpatients with liver disease
From 2010 to 2019, a total of 46,818 patients were hospitalized with liver disease, among which liver diseases K70–K77 accounted for the highest proportion at 51.27% (24,003/46,818), presenting an upward trend, followed by viral hepatitis B15–B19, presenting a downward trend, and accounting for 33.77% (15,810/46,818). The proportion of liver tumors C22.0–C22.9 was 14.96% (7005/46,818) and was basically stable, as shown in Figure 2. Excluding 775 cases of benign liver tumor and 272 cases of repeated hospitalization, a total of 5958 cases of hepatic malignant tumor were hospitalized.

Etiological composition of inpatients with liver disease.
Etiological distribution of inpatients with hepatic malignant tumor
Among the 5958 patients hospitalized with hepatic malignant tumor from 2010 to 2019, HBV-related liver cancer accounted for the highest proportion at 77.49% (4617/5958), followed by HCV-related liver cancer, accounting for 6.83% (407/5958). The proportion of liver cancer related to ALD was 4.18% (249/5958), that of metastatic liver cancer from a malignant tumor was 4.01% (239/5958), that of autoimmune-liver-disease-related liver cancer was 0.72% (43/5958), and that of HBV + HCV-related liver cancer was 0.57% (34/5958). The proportion of liver cancer due to other causes was 6.19% (369/5958), and that proportion increased in the latter 4 years (Figure 3). The proportion of MAFLD-related liver cancer was 4.58% (273/5958), and increased gradually, from 3.09% in 2010 to 6.40% in 2019.

Etiological distribution of inpatients with hepatic malignant tumor.
General data on 273 patients with MAFLD-related liver cancer
Among the 273 patients with MAFLD-related liver cancer, 60.07% were male, 66.30% were aged ⩾60 years, and 43.22% were patients with liver cirrhosis suggested by imaging at first hospitalization. Furthermore, 44.69% were overweight/obese, 41.03% were diagnosed with type 2 diabetes, 75.09% presented ⩾2 metabolic-related factors, 179 cases were hypertensive, 81 cases presented increased serum triglyceride level (⩾1.70 mmol/l), 231 cases presented decreased blood HDL-C (<1.0 mmol/l in males and <1.3 mmol/l in females), and 66 cases presented prediabetes (5.6–6.9 mmol/l). During 2010–2014 and 2015–2019, there was no statistical difference in terms of sex, and no statistical difference in the proportions of patients with cirrhosis, overweight/obesity, type 2 diabetes, and ⩾2 metabolic factors. The average age of the 2015–2019 group was 65.32 ± 12.31, up from 61.25 ± 16.03 in 2010–2014 (p = 0.019). 76.30% of the 2015–2019 group were ⩾60 years, up from 60.14% in the 2010–2014 group (p < 0.001) (Table 1).
Clinical characteristics of MAFLD-related liver cancer during 2010–2014 and 2015–2019.

HDLC, high-density lipoprotein cholesterol; MAFLD, metabolic-associated fatty liver disease; TG, triglyceride.
Clinical characteristics of MAFLD-related liver cancer without evidence of fatty liver and with evidence of fatty liver
Among the 273 patients with MAFLD-related liver cancer, 235 patients was considered for the diagnosis of MAFLD-related liver cancer without evidence of fatty liver, 38 patients was considered for the diagnosis of MAFLD-related liver cancer with evidence of fatty liver, 7 patients by pathology, 24 patients by imaging, and 7 patients by previous medical history.
There was no significant difference in the ratios of sex, age, overweight/obesity, type 2 diabetes, and presence of ⩾2 metabolic factors between 38 cases of MAFLD-related liver cancer with evidence of fatty liver and 235 without evidence of fatty liver. The proportion of liver cirrhosis in patients without evidence of fatty liver was higher than that in patients with evidence of fatty liver (p < 0.001), and the proportion of elevated triglycerides was lower than that in patients with evidence of fatty liver (p < 0.001) (Table 2).
Clinical characteristics of MAFLD-related liver cancer without evidence of fatty liver and with evidence of fatty liver.

HDLC, high-density lipoprotein cholesterol; MAFLD, metabolic-associated fatty liver disease; TG, triglyceride.
Clinical characteristics of MAFLD-related liver cancer with cirrhosis and noncirrhosis
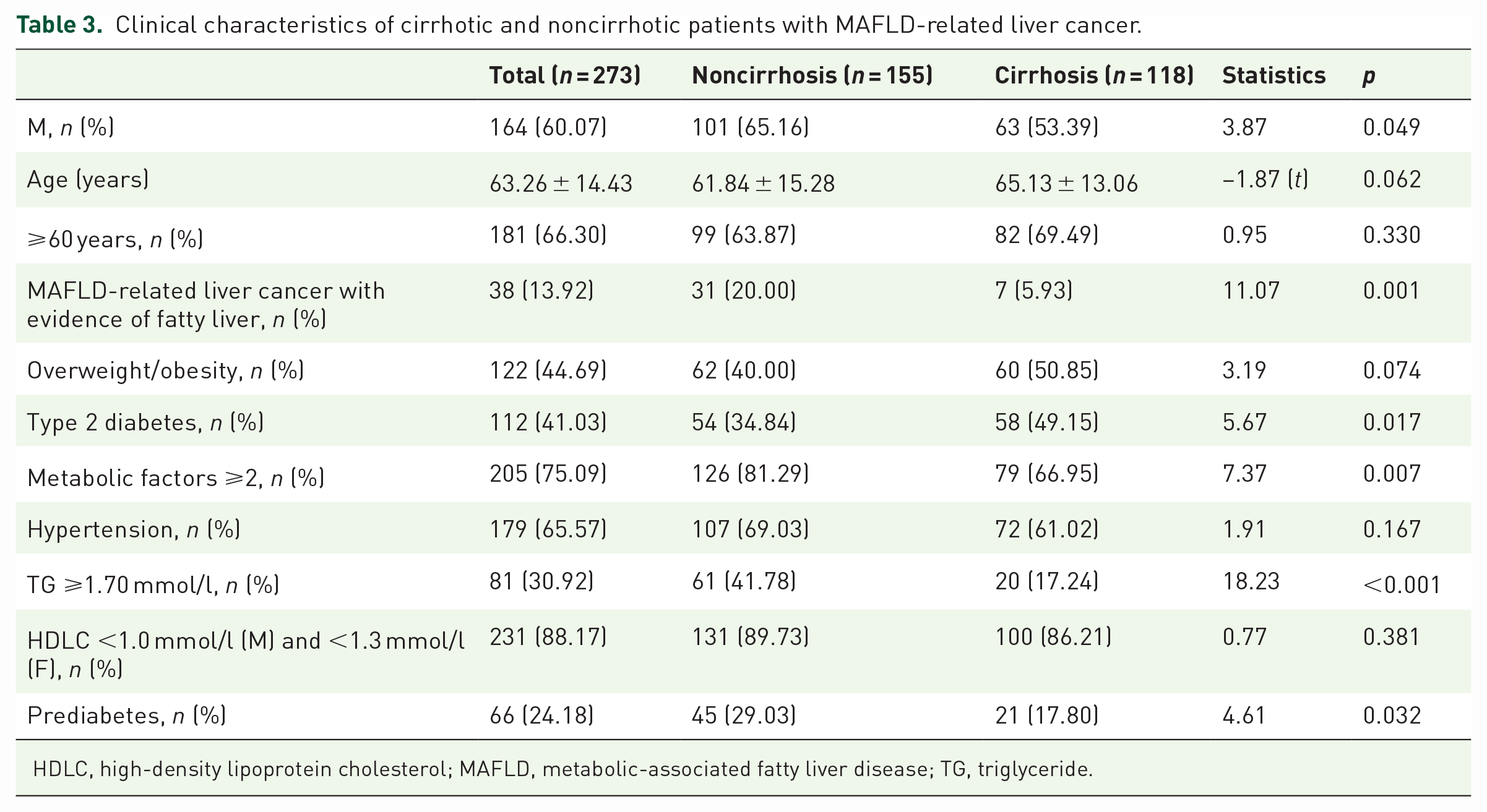
Among the 273 patients, 118 patients showed cirrhosis by imaging examination, and 155 patients showed no cirrhosis. The proportion of male in noncirrhosis group was higher than that in cirrhosis group (p = 0.049). There was no significant difference in average age. The proportion of MAFLD-related liver cancer with evidence of fatty liver in noncirrhosis group was higher than that in cirrhosis group (p < 0.001). There was no significant difference in the proportion of overweight/obese patients between the two groups, and the proportion of type 2 diabetes in noncirrhosis group was lower than that in cirrhosis group (p = 0.017). The proportion of patients with ⩾2 metabolism-related factors in noncirrhosis group was higher than that in cirrhosis group (p = 0.007). The proportion of those with elevated triglycerides in noncirrhosis group was higher than that in cirrhosis group (p < 0.001). The proportion of those with prediabetes in noncirrhosis group was higher than that in cirrhosis group (p = 0.032) (Table 3).
Clinical characteristics of cirrhotic and noncirrhotic patients with MAFLD-related liver cancer.
HDLC, high-density lipoprotein cholesterol; MAFLD, metabolic-associated fatty liver disease; TG, triglyceride.
Discussion
We summarized the clinical data relating to cases of MAFLD-related liver cancer and liver cancer with unknown cause admitted to Beijing Ditan Hospital from 2010 to 2019. In these recent 10 years, the proportion of liver tumors C22.0–C22.9 was basically stable. Liver cancer due to other causes was on the rise. Among the 369 patients with liver cancer due to other causes, 273 patients who met the diagnostic criteria for MAFLD could be diagnosed MAFLD-related liver cancer. The proportion of MAFLD-related liver cancer increased gradually. Among 273 patients with MAFLD-related liver cancer, 60.07% were male, 66.30% were ⩾60 years old, and 43.22% had cirrhosis. Only 38 cases could be diagnosed with MAFLD by pathology, imaging, and previous medical history. There were no statistically significant differences in the proportions of sex, age, overweight/obesity, type 2 diabetes, and presence of ⩾2 metabolic-related factors in 38 patients with evidence of fatty liver and 235 patients without evidence of fatty liver.
In this study, the etiological composition of inpatients with liver diseases from 2010 to 2019 was analyzed. The proportion of liver diseases K70–K77 was the highest and showed an upward trend, followed by viral hepatitis with a downward trend, and the proportion of liver tumors C22.0–C22.9 was basically stable. From the analysis of the etiology of liver tumors, viral hepatitis is still the main cause, among which viral hepatitis B accounts for 77.49%. Liver cancer due to other causes was on the rise in the latter 4 years. In the past 5 years, the average annual incidence of liver cancer in the world was 995,000, of which 423,000 were in China, accounting for 42.5% of the world’s cases. 2 Chronic HBV-related liver cancer is still the primary type of liver cancer. 13 With the widespread use of antiviral drugs, however, HBV and HCV have been effectively suppressed or eradicated; the incidence of MAFLD-related liver cancer is on the rise and has become an important cause of liver cancer in Europe and the United States.6,14,15 At present, China also has the same development trend.
Among the 273 patients with MAFLD-related liver cancer, 60.07% were male, 66.30% were aged ⩾60 years, and 43.22% had liver cirrhosis on imaging at first hospitalization. The average age at onset of liver cancer varies from 30 to 60 years old in Asia and Africa. BRIGDE’s study showed that the average age at onset of liver cancer was 52 years old in China, 69 years old in Japan, 59 years old in South Korea, 65 years old in Europe, and 62 years old in North America. 16 Of the 410,000 new cases of liver cancer in China, 303,000 were men – much more than women. 2 A Chinese study that included 14,891 cases of liver cancer from 2016 to 2018 showed that the incidence rate was 76.01% for men and 23.99% for women. 17 Previous studies in the literature have reported that cirrhosis due to various reasons is the most important link in the occurrence of liver cancer, and 85–95% of liver cancer has a background of liver cirrhosis. 18 Compared with the above data, the proportion of patients with MAFLD-related liver cancer in our hospital was slightly lower in the proportion of males, slightly higher in age, and lower in the rate of cirrhosis.
Among the 273 patients, nearly 45% were overweight/obese, nearly 40% had type 2 diabetes, and nearly 3/4 had ⩾2 metabolic-related factors. It was been reported that the prevalence of NAFLD in overweight/obese people is 50.1–75.8%.19,20 A meta-analysis of 80 studies in 20 countries showed a prevalence of NAFLD in patients with type 2 diabetes of 55.5% [95% confidence interval (CI) = 47.3–63.7]. 21 A recent cross-sectional study of 2420 patients from six provinces and municipalities in China showed that the prevalence of NAFLD in type 2 diabetes was 55.3%. 22 A population-based cohort study showed an increased risk for HCC was found in patients with NAFLD compared with controls [adjusted adjusted HR (aHR) = 12.18, 95% CI = 7.15–20.79]. 23 NAFLD is associated with an increased risk of developing HCC, especially among those who have cirrhosis or advanced fibrosis, but 20–30% of cases of NAFLD-related HCC occur in the absence of advanced fibrosis. 24 Our data showed that the proportion of imaging manifestations of fatty liver was very low and the proportion of history of fatty liver was very low, but the proportion of fatty liver manifestations in liver puncture was not low. Therefore, it can be inferred that the proportion of MAFLD in this group is not low, and the proportion of MAFLD-related liver cancer may be seriously underestimated.
The reasons for the low proportion of MAFLD-related liver cancer in this study were analyzed. (1) Most patients had not made a habit of regular physical examination in the past, and their past medical history was not clear, so metabolic factors such as diabetes, abnormal metabolism of blood lipids, and hypertension were found only when they were treated for liver cancer. 25 (2) Some patients were overweight in the past but had begun to lose weight. Liver cancer was found when they visited the doctor, and weight loss leads to insignificant fatty liver. (3) There are certain limitations in the diagnosis of fatty liver by imaging. Liver pathology is the gold standard for the diagnosis of fatty liver. The proportion of tumor patients who can undergo liver biopsy or surgical resection is low. (4) Currently, there is no unified diagnosis standard for MAFLD-related liver cancer, and liver pathology or liver imaging examination may not show typical manifestations of fatty liver in patients with MAFLD-related liver cancer.
We further analyzed 273 patients with metabolic risk factors; only 38 patients had evidence of fatty liver and 235 patients showed no objective evidence of fatty liver. There was no statistical significance in the proportions of sex, age, overweight/obesity, type 2 diabetes, and the presence of ⩾2 metabolic-related factors. The proportion of cirrhosis in patients with evidence of fatty liver was lower than that in patients without evidence of fatty liver (18.92% versus 47.64%). A multicenter, retrospective, cohort study of MAFLD-related HCC included 1382 patients from 11 centers in the United States and East/Southeast Asia showed cirrhosis was present in 62% of patients. 26 A population-based cohort study including 8982 adults in Sweden with biopsy-confirmed NAFLD showed HCC incidence rates increased monotonically across categories of simple steatosis, nonfibrotic nonalcoholic steatohepatitis (NASH), noncirrhotic fibrosis, and cirrhosis (0.8 per 1000 person-years, 1.2 per 1,000 person-years, 2.3 per 1,000 person-years, and 6.2 per 1,000 person-years, respectively). 27 In a meta-analysis of 168,571 participants from 19 studies, the HCC prevalence of noncirrhotic NASH was 38.0%. Other causes of noncirrhosis accounted for 14.2% (p < 0.001). Noncirrhotic NASH patients were more likely to develop HCC than noncirrhotic patients with other etiologies [odds ratio (OR) Rd2.61, 95% CI I%1.27–5.35, p = 0.009]. 28 In this study, half of MAFLD-related liver cancer occurred in the absence of cirrhosis. Steatosis-related lipotoxicity and oxidative DNA damage can induce hepatocarcinogenesis. These factors may explain the association between NAFLD and HCC, especially in the absence of cirrhosis. 29
In 273 patients with abnormal metabolism of liver cancer, HDL-C was decreased in 88.17%, hypertension was present in 65.57%, prediabetes was present in 24.18%, and triglycerides were increased in 30.92%. A retrospective cohort study in the United States showed that each additional metabolic trait increases the risk of cirrhosis and liver cancer in NAFLD patients, with diabetes being the highest risk factor for the progression of hepatocellular carcinoma. Patients with diabetes, hypertension, and obesity thus need special attention. 30 A study of real population data from the United Kingdom, the Netherlands, Italy, and Spain showed that diabetes was an independent predictor of advanced liver disease (cirrhosis and liver cancer). 31 Results of a meta-analysis showed that the presence of diabetes was associated with an increased risk of HCC (HR HR2.65, 95% CI IR2.02–3.49, heterogeneity = 0.589, I2 = 0.0%), and overweight/obesity was slightly associated with an increased risk of HCC in NAFLD patients (HR = 1.31, 95% CI = 1.00–1.71, heterogeneity = 0.888, I2 = 0.0%). 32 Therefore, MAFLD-related liver cancer should be considered for patients with overweight/obesity, type 2 diabetes, or metabolic-abnormality-related factors (hypertension, blood triglycerides of ⩾1.70 mmol/l, blood HDL-C levels of <1.0 mmol/l in males and <1.3 mmol/l in females, prediabetes), even if there is no fatty liver manifestation in imaging and liver pathology.
Limitations of this study include its single-center cross-sectional study. We did not calculate the sample size because of the lack of exact data on MAFLD-related liver cancer inpatients in China. In particular, it is not possible to reliably determine history of MAFLD. Also, biopsy was not performed in the majority of patients, so we could not distinguish between simple steatosis and nonalcoholic steatohepatitis, which may be especially relevant in patients without cirrhosis. We also lack sufficient data for additional factors, such as blood biochemical indexes, clinical staging liver cancer, statin use, markers to assess for the severity of metabolic syndrome, or long-term outcome of patients.
Conclusion
In conclusion, among 5958 patients hospitalized with hepatic malignant tumor from 2010 to 2019, 273 cases diagnosed as MAFLD-related liver cancer were analyzed. It was found that only 13.92% patients had objective evidence of fatty liver, and 56.78% of them occurred without cirrhosis. Therefore, patients with high-risk factors for metabolic abnormalities should pay attention to screening for liver cancer, even if they had no objective evidence of fatty liver and cirrhosis.