
Abstract
Background:
Active cervical spine rotation (ACROM Rot) shows cervical rotation and flexion rotation test (FRT); side-bending rotation test (SBRT) and upper cervical axial rotation test (C0–C2ART) are described to measure upper cervical rotation. The objectives of this study are (1) to describe the normal range of motion (ROM) of ACROM Rot, and the ROM in FRT, SBRT and C0–C2ART tests; (2) to explore the correlation among the four tests and (3) to investigate the influence of age and sex in their ROM.
Methods:
A cross-sectional study was carried out with healthy volunteers from 18 to 75 years of age. Tests were measured using a CROM device and a bubble inclinometer. Descriptive analysis was performed to establish normative data for the ROM tests. Correlation analysis was conducted to understand the relation between upper and global cervical rotation ROM and among the three upper cervical rotation tests. Linear regression models were developed to understand the influence of age and sex in the ROM of all tests.
Results:
Normative values were obtained from 122 healthy volunteers (50% male), by sex and age strata. The degree of correlation ranged between 0.582 (p < 0.01) for FRT and ACROM Rot left and 0.217 (p < 0.05) for SBRT and C0–C2ART left. Linear regression models showed the influence of sex for ACROM Rot right (men −4.64° less than women), SBRT (men −4.1° less than women) left and C0–C2ART right and left (men −2.24° and −1.78° less than women). The age influenced rotation ROM with a decrease for every 10 years of −2.11° and −1.96° for ACROM Rot right and left, of −1.72° and −1.26° for FRT right and left and −0.58° and −0.41° for C0–C2ART right and left in the linear regression models. No association was found between age and SBRT (p = 0.63 for right SBRT and p = 0.49 for left SBRT).
Conclusion:
Weak-to-moderate correlation was found between the upper cervical spine rotation tests and with the ACROM. Women had a larger ROM in ACROM Rot right, SBRT left and C0–C2ART. Decreases in ROM related with age were observed for ACROM Rot, FRT and C0–C2ART but not for SBRT.
Keywords
Background
Range of motion (ROM) is a standard test and measure used during the examination of patients with cervical spine disorders.1,2 Overall, cervical ROM decreases with age,2–4 with transverse plane motion (i.e. rotation) decreasing 3–4° every decade. 5 Women tend to present with greater mobility than men, although differences are not usually statistically significant. 6 Cervical transverse plane ROM is generally the most impaired. 7 Physiologically, cervical rotation is not uniformly distributed between the upper and lower cervical spinal regions, with upper cervical (UC) accounting for 60% of the available motion.8–10
A number of person-dependent characteristics have been proposed that may influence ROM in the cervical spine. Habits and postures related with occupational demands such as sitting hours or use of data display screens are a risk factor for developing neck pain.11–13 Psychological status, anxiety and depression are related with the risk of developing neck pain.12,14 Frequent exercise has been shown to reduce the risk of developing neck pain.12–14 Pathologies, such as visual deficits, 15 or temporomandibular complaints, such as bruxism, 16 may impact the mobility of the cervical spine due to the changes in head position and tension in muscle structures. Drug use is one of the main strategies in managing neck pain and indicative of symptoms.17,18 Neck pain and disability are related with changes in the ROM of the cervical spine.19–22
Full axial rotation ROM at C1–C2 is generally accepted to be approximately 40–45°, 23 with most in vivo studies reporting values between 36° and 41°.10,24–28 However, there is a wide variability in the literature regarding the amount of UC rotation among the UC rotation ROM tests: the flexion rotation test (FRT), the side-bending rotation test (SBRT) and the C0–C2 axial rotation test (C0–C2ART). For example, UC rotation found in the FRT was described three times larger than in the C0–C2ART. 29
The FRT measures C1–C2 rotation, predominantly, after the cervical spine is prepositioned into maximal ventral flexion in supine. 30 The normal ROM of the FRT is expected to be 44° to each side with 34° as a cut-off value for a positive test. 31 UC rotation ROM is one of the most accurate and reliable examinations for cervicogenic headache. 32 Furthermore, the severity of cervicogenic headache is inversely correlated with the FRT ROM.31,33 Smith et al. 19 concluded that age and sex did not significantly influence FRT ROM. However, Schäfer et al. 34 recently found a decrease in total rotation FRT of 0.55° per year.
The SBRT is a clinical test used to examine UC rotation by prepositioning the cervical spine in maximal contralateral side bending in supine. Swanson et al. 35 determined a ROM around 37° to each side in young and asymptomatic subjects. Cattryse et al. 36 performed an in vitro study that used a similar locking technique and obtained 55.13° of total rotation at C1–C2. However, no study has investigated the clinical utility of this test and the effect of age and sex on this test.
C0–C2ART, also called the rotation stress test, measures UC rotation with manual stabilization of the C2 vertebra with the patient seated. Therefore, this test is differentiated from FRT or SBRT since no end-range movement of the lower cervical spine is used. Theoretically, a more specific motion is generated in the UC spine. 37 Satpute et al. 37 reported a 15.4° (right rotation) and 14.4° (left rotation). Osmotherly et al. 38 measured a right rotation of 10.58° of UC axial rotation by magnetic resonance (MR) in young and asymptomatic subjects from a supine position. C0–C2ART is commonly used as a screening test for ruling out UC instability. 39 Satpute et al. 37 identified a significant positive correlation between FRT and C0–C2ART, although FRT had almost three times more rotation than the C0–C2ART. No study has investigated the clinical utility of this test and the effect of age and sex on this test.
Efficient clinical examination of patients with cervical spine-related complaints is fundamental to establish baselines, define physical therapy objectives and interventions, and evaluate the patient progress.40,41 Understanding the normal ROM values and relationship among the different tests for measuring UC rotation could permit the clinicians to the election of the most useful test depending on the patient characteristics.
A deeper knowledge about the normal values, their variability between sex and age strata, and the correlation among these UC rotation ROM tests would help make a UC rotation ROM diagnosis.
Objectives
The primary purpose of this study was to describe the normal UC rotation ROM values in healthy subjects. The secondary purpose was to describe the correlations among the active cervical spine rotation (ACROM Rot), FRT, SBRT and C0–C2ART. The third purpose of this study was to investigate how sex and age influence the rotation ROM in these tests.
Methodology
Ethics
The study was conducted according to the Declaration of Helsinki and approved by the Research Ethics Committee of the Universitat Internacional de Catalunya (FIS-2020-03). Informed consent for publication was provided by the person in the figures of the article.
Sample size
The sample size for estimating population means was calculated using the software GRANMO-IMIM V 7.12 online version. 42 The calculations were done for the Spanish population, 47 million people, with an accuracy of 3° without an estimate of replacements. The sample size was calculated for ACROM Rot with an SD of 16, 43 for the FRT with an SD of 7.3, 44 for the SBRT with an SD of 3.8 35 and for the C0–C2ART with an SD of 2.8. 37 The sample size estimations were 110 participants for ACROM Rot, 23 participants for FRT, 7 participants for SBRT and 4 participants for C0–C2ART. The most conservative was used for sample size calculations (110 participants for ACROM) and for the recruitment of 10 males and 10 females for each of the six age strata (120 participants).
Design
A cross-sectional study design was used to investigate the rotation ROM of the cervical and UC spine in healthy people, stratified by sex and age. A convenience sample was recruited through an advertisement within the university community. Samples were collected from volunteers who answered the call on a first-come, first-served basis. Participants were stratified by sex and age in each of the six age strata (18–25/26–35/36–45/46–55/56–65/66-75 years) until 10 women and 10 men were assigned to each age group. Data were collected from November 2020 to April 2021 at Universitat Internacional de Catalunya (Sant Cugat del Vallés, Spain). Participants were excluded if they had any condition that might affect cervical ROM, including a medically diagnosed neck condition or having received treatment for neck pain in the last year, whiplash, head trauma, acute infection, recent surgery or if they were currently pregnant. Overall, 10 females and 10 males were recruited from each of the six age strata. All participants signed an informed consent form.
Variables
The dependent variables were active cervical ROM in the transverse plane (ACROM Rot) and UC mobility tests (FRT, SBRT, C0–C2ART). Independent variables were age, sex, daily hours of use of data display screens (continuous), daily sitting hours (continuous), weekly hours and days of physical activity (continuous), visual handicap (discrete yes/no), use of a dental splint (discrete yes/no), drug use (discrete yes/no), having neck pain during last year (discrete yes/no) and at the moment of the measurement (discrete yes/no),12,19,45–47 Hospital Anxiety and Depression Scale (HADS)(ICC: 0.85–0.91) 48 (continuous) and Neck Disability Index (NDI) (ICC: 0.88) 49 (continuous).
Methods
Electronic questionnaires were used to collect all non-ROM data. ROM measurements were taken following a warm-up. Participants were asked to perform three active movements until the end range in each direction of the sagittal, frontal and transverse plane. All participants were measured by the same physiotherapist, who had 10 years of clinical and teaching experience.
ACROM Rot
ACROM device (Performance Attainment Associates, Roseville, MN) was used to measure ACROM Rot according to Youdas et al. 43 and Audette et al. 50 in sitting position. Test retest reliability ICC is 0.92–0.95. 50 Following the warm-up, each participant performed three axial rotations to the right and the left. Participants were instructed to turn as far as possible or stop at the point where they experienced symptoms. The examiner monitored and avoided compensatory movements. Three repetitions were performed and measured using the CROM. Each repetition was then averaged for data analysis. The intratester ICC for the right and left rotation is 0.80 and 0.84 when measured with the CROM device. 43
FRT
ROM of the FRT was measured using a CROM device according to Hall et al. 31 First, the participant was positioned in supine with their cervical spine flexed maximally until the CROM compass was horizontal. Next, the participant’s head rotation was rotated three times in both directions until symptoms were reported and the therapist felt a firm resistance. CROM measurements were taken after each repetition and averaged. Intratester ICC is 0.95–0.97. 51 The inter-examiner ICC is 0.93 31 (Figure 1).

FRT.
SBRT
ROM of the SBRT was measured according to Swanson et al. 35 using a bubble inclinometer (Baseline bubble Inclinometer; Fabrication Enterprises, White Plains, NY) attached to the upper arm of the CROM. The participant was positioned in supine with their cervical spine maximally side bent to one side. From this position, contralateral rotation was performed three times until symptoms were reported and the therapist felt a firm resistance. SBRT measurements were taken after each repetition and averaged (Figure 2).

SBRT.
C0–C2ART
CROM device was used to measure rotation ROM between the cranium (C0) and the axis (C2) according to Satpute et al. 37 The participant was positioned in sitting. Using this method, the tester places their hand on the top of the participant’s head, under the cranial crossbar of the CROM. The tester then uses their other hand to stabilize C2 posteriorly. Next, the index finger was placed on the contralateral side of the spinous process and the thumb on the ipsilateral lamina while using the head contact to rotate the head left and right. Rotation was performed until symptoms were reported and the therapist felt a firm resistance. Measurements were taken after each repetition and averaged. The ICC reported for this test using compass application for iPhone ranged from 0.88 to 0.91 37 (Figure 3).

C0–C2 axial rotation.
Statistical analysis
Medians and interquartile ranges (IQR) or frequencies and percentages for independent and dependent variables in the entire sample were calculated to describe the results obtained and establish normal values for ROM tests.
A study of normality of the ROM variables was performed using a Kolmogorov–Smirnov test to determine if Pearson’s or Spearman’s Rho should be applied. A pairwise correlation analysis was performed to estimate the association between the scores of the four tests of interest. The following relationships were considered: r < 0.3 weak, 0.3 ⩽ r ⩽ 0.5 moderate and r > 0.5 strong. 52
Linear regression models (LRMs) were used to quantify the influence of sex and age on the ROM for the different tests.
First, a univariate LRM was performed to estimate how sex influenced the score of each test. Next, multiple univariate models were developed for each of the independent variables to observe how these variables influence the dependent variable. The final adjusted multivariate model only contained those covariates which had a p-value less than 0.05 in the univariate analysis. However, the variable age strata were kept in the model in all cases.
In all models, the coefficients of regression and 95% confidence intervals (CIs) were the parameters of interest. The coefficient for the variable sex and its 95% CIs represents the influence of being a man (compared to being a woman) on the scoring.
A similar procedure was followed to determine the influence of age on the ROM for the different tests. The adjusted model included only covariates less than 0.05 in the univariate analysis. Here, the coefficient for the variable age strata and its 95% CIs represents the influence of being 10 years older on the scoring.
LRM’s hypothesis was assessed, and the results suggested normality, linearity, homoscedasticity and absence of multicollinearity.
All analyses were done with IBM SPSS statistics 20.
Results
The results are presented in three sections. The first section provides the descriptive analysis for the entire sample and correlations found between the scores of the four tests. The second and the third sections provide the results of the regression models for sex and age strata.
Results for all the sample
Overall, 128 subjects were measured and 6 were excluded due to not meeting the inclusion and exclusion criteria (higher frequency of headaches, cervical treatment, whiplash during the last year and a condition affecting cervical ROM). Finally, data from 122 participants (61 females) between 18 and 75 years of age were analysed. The mean age of the participants was 45.16 (±16.76). The descriptive analysis for all the participants’ independent variables is provided in Table 1.
Descriptive data for independent variables in all the sample as median and IQR or frequency and percentage.
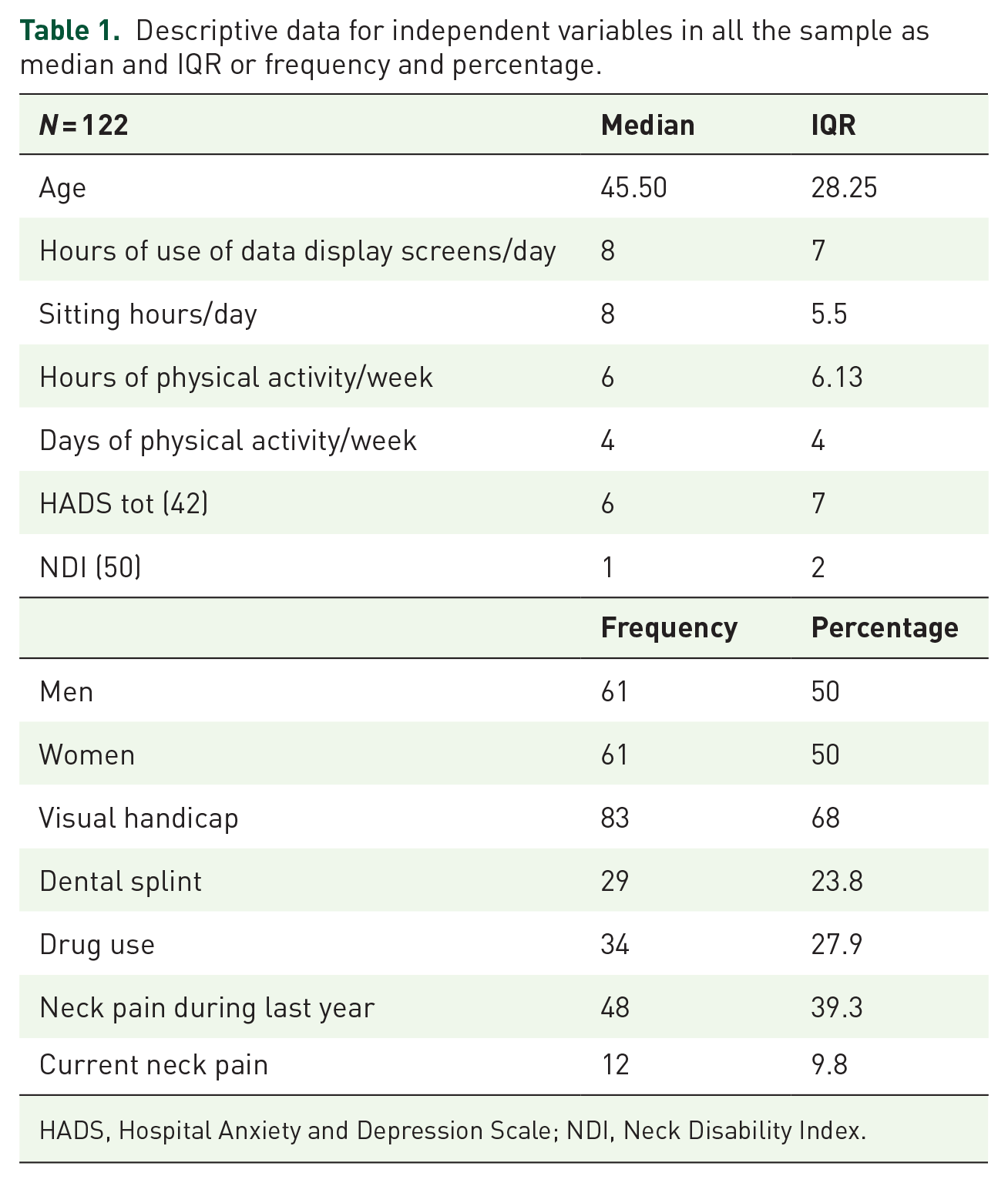
HADS, Hospital Anxiety and Depression Scale; NDI, Neck Disability Index.
The ROM for the four tests performed (ACROM, FRT, SBRT and C0–C2ART) is presented in Table 2.
Descriptive data for the dependent variables as minimum, maximum, median and IQR.

(°), degree; ACROM Rot, active cervical spine rotation; C0–C2ART, upper cervical axial rotation test; FRT, flexion rotation test; SBRT, side-bending rotation test.
A study of normality was performed. The Kolmogorov–Smirnov values showed non-normal distribution of the variables: ACROM Rot right, FRT left, SBRT left and C0–C2ART to both sides (p < 0.05).
A correlation study between the results of the four tests (both right and left sides) was carried out using the Spearman’s Rho test because of the non-normal distribution of most of the variables. A statistically significant correlation was found between the results of all the tests for both sides (Tables 3 and 4). In right rotation, statistically significant correlations (p < 0.01) were found among the tests. The larger correlation value was found between ACROM Rot and FRT (0.555; p < 0.01) and the lesser correlation between SBRT and C0–C2ART (0.253; p < 0.05) and FRT and C0–C2ART (0.256; p < 0.01). A moderate correlation was found between ACROM Rot and SBRT (0.380; p < 0.01) and C0–C2ART (0.384; p < 0.01) and between FRT and SBRT (0.471; p < 0.01).
Correlations between means of rotation ROM tests to the right side.

ACROM Rot, active cervical spine rotation, C0–C2ART, upper cervical axial rotation test; FRT, flexion rotation test; SBRT, side-bending rotation test.
Significant correlation at level 0.01 (bilateral).
Correlations between means of rotation ROM tests to the left side.
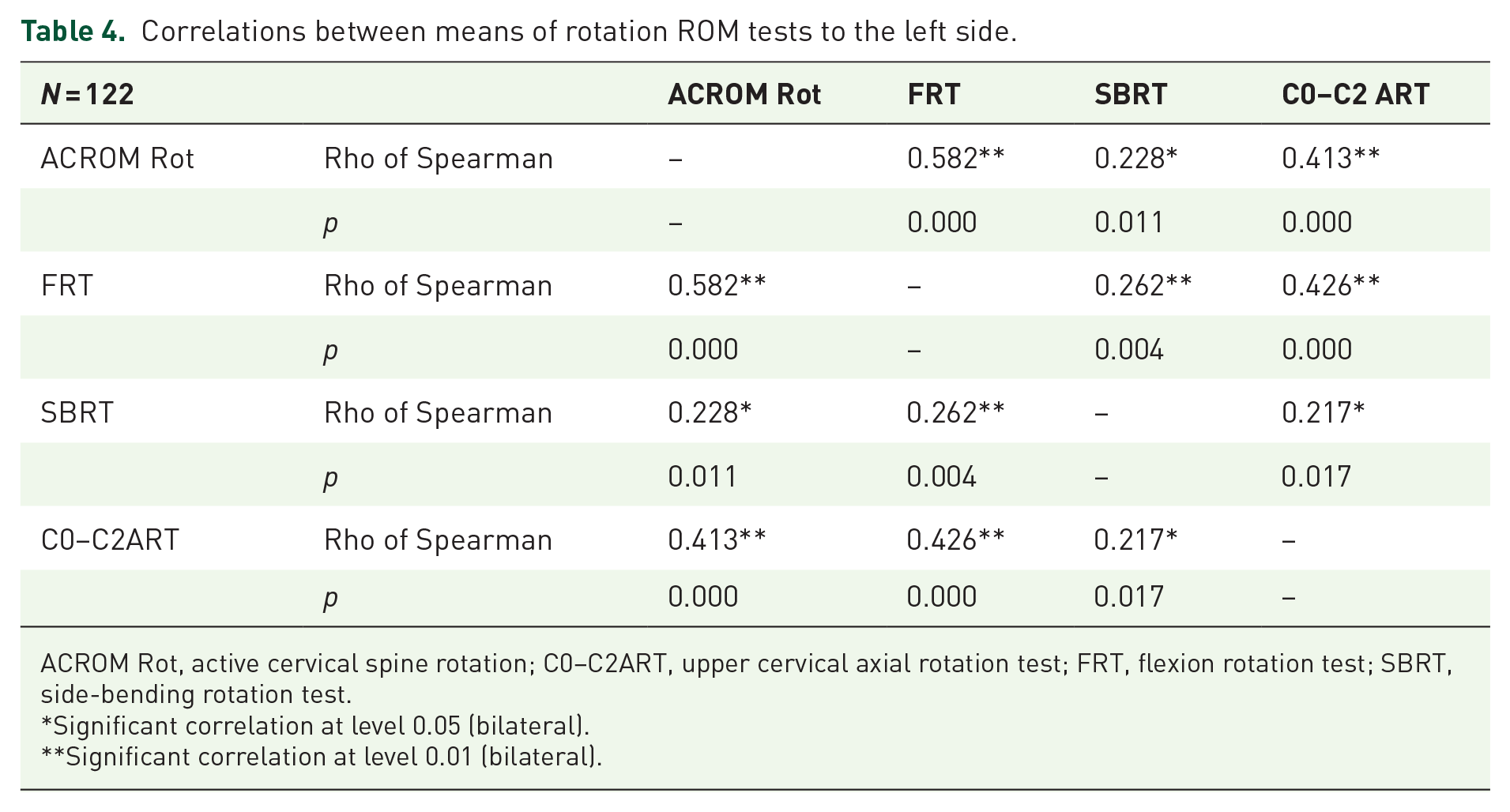
ACROM Rot, active cervical spine rotation; C0–C2ART, upper cervical axial rotation test; FRT, flexion rotation test; SBRT, side-bending rotation test.
Significant correlation at level 0.05 (bilateral).
Significant correlation at level 0.01 (bilateral).
In left rotation, the same Spearman’s correlation test was carried out due to the non-normal distribution of the variables. There were significant correlations between all the left side rotation measurements (p < 0.05) (Table 4). As in right rotation, the larger correlation was found between FRT and ACROM Rot (0.582; p < 0.01) and the lesser between SBRT and C0–C2ART (0.217; p < 0.05). Moderate correlations were found between ACROM Rot and FRT with C0–C2ART (0.413; p < 0.01 and 0.426; p < 0.01, respectively). Weak relationships were found for the rest of pairs analysed.
Results by sex
Means and standard deviations of rotation tests by sex are shown in Table 5. Results show that men tended to have less ROM than women in ACROM Rot and all UC rotation tests. Regression analysis found that the sex was significant (p < 0.05) in the adjusted LRM for the ACROM Rot right, SBRT left, C0–C2ART right and C0–C2ART left. In our predictive model, comparing/evaluating a male instead of a female showed a ROM reduction of: −4.64° (CI 95%: −7.25 to −2.04; p = 0.001) in ACROM Right Rot; −4.1° (CI 95%: −7.97 to −0.23; p = 0.038) in SBRT left; −2.24° (CI 95%: −3.24 to −1.25; p < 0.001) and −1.78° (CI 95%: −2.79 to −0.76; p = 0.001) for right and left C0–C2ART, respectively.
Medians and IQR of ROM tests and coefficients of LRMs by sex.

(°), degree; ACROM Rot, active cervical spine rotation; C0–C2ART, upper cervical axial rotation test; CI, confidence interval; FRT, flexion rotation test; IQR, interquartile range; NDI, neck disability index; ROM, range of motion; SBRT, side-bending rotation test.
Results by age strata
Means and standard deviations by age strata for each test are presented in Table 6. The cervical ROM in ACROM Rot and all UC rotation tests was reduced as the age increased, except in the case of SBRT. This information is corroborated by the LRM that shows this relationship between the age and the decrease in the ROM of ACROM Rot, FRT and C0–C2ART in every case to both sides.
Medians and IQR of ROM tests and coefficients of LRMs by age strata.

(°), degree; ACROM Rot, active cervical spine rotation; C0–C2ART, upper cervical axial rotation test; CI, confidence interval; FRT, flexion rotation test; IQR, interquartile range; NDI, neck disability index; SBRT, side-bending rotation test.
Coefficients showed the reduction of ROM produced with every decade of life. The adjusted LRMs confirmed the results obtained in the non-adjusted models. Being 10-year older decrease ACROM Right Rot [−2.11° (CI 95%: −2.87 to −1.35); p < 0.001]; ACROM Left Rot [−1.96° (CI 95%: −2.77 to −1.14); p < 0.001]; FRT right (−1.72° (CI 95%: −2.53 to −0.9); p < 0.001]; FRT left [−1.26° (CI 95%: −1.94 to −0.57); p < 0.001]; C0–C2ART right [−0.58° (CI 95%: −0.9 to −0.27); p < 0.001] and C0–C2ART left [−0.41° (CI 95%: −0.71/−0.11); p < 0.01].
Discussion
This study examines active cervical rotation ROM and ROM in the FRT, SBRT and C0–C2 axial rotation test in a sample of asymptomatic and subclinical neck pain participants. A weak or moderate correlation was found among the UC rotation tests except for the FRT and ACROM Rot which showed a strong correlation. Regression linear models were developed to examine the relationship between sex and age and the ROM of the cervical and UC rotation tests. Men tended to display a reduced ROM compared to women in all tests. Age had a negative influence on ROM in all movements except for SBRT in both directions.
Descriptive study
ACROM Rot
The results [left rotation 61.28 (±8.50); right 60.89 (±8.37)] are in the lower margin of the angular values (60–86°) described by Chen et al. 6 in their meta-analysis. Our data were also less than the unilateral ROM of approximately 75° described by Smith et al. 19 and the 70° described by Hanney et al. 53 in an asymptomatic sample of 18–50 years and in asymptomatic women. 54 The results are also lower than the asymptomatic groups of Hall and Robinson 33 and Oliveira-Souza et al. 55 and slightly higher than the results of Audette et al. 50 However, these studies did not include both sexes and age ranges from 18 to 75 years. In a more comparable study, Schäffer et al. 34 studied 220 asymptomatic subjects (124 male) from 18 to 90 years of age finding a total transverse ROM of 154.2° (±25.5). Schäffer et al. 34 did not include subclinical neck pain patients, performed, and measured only one repetition of rotation, and did not indicate if compensatory movements of adjacent regions were monitored. These variations could explain the increased rotation ROM reported by Schäffer et al. 34 compared to our study.
FRT
Angular values for right FRT, 46.53 (±8.28), and left FRT, 43.88 (±6.79), are within the upper and lower margins of ROM described for FRT in asymptomatic subjects (40.8–46.4°)19,31,33–35,37,55–59 Despite the different participant demographics or measurements, physiological FRT ROM is consistent throughout the various studies.
SBRT
In spite of being used clinically, 60 the SBRT has not been widely studied in the literature. Our SBRT ROM [32.01 (±12.05) and 36.48 (±10.93) for right and left SBRT, respectively] was similar to the study of Swanson et al. 35 for asymptomatic subjects. Their results were 37.6 (±4.3) and 37.7 (±4.2) for right and left SBRT, respectively. In our sample for the age group that contains the age of Swanson’s sample (26–35 years), results were 33.25 (±14) and 38.36 (±14.64), respectively. The slight differences observed can be due to the participant variations and the measurement instrument (bubble inclinometer versus digital goniometer).
C0–C2ART
The values of C0–C2ART or the similar rotation stress test [right 7.78° (±3.85) and left 8.03° (±3.18)] are inferior to the values of Satpute et al. 37 [15.44° (±2.68) and 14.43° (±2.94) for right and left, respectively] and to the values of Osmotherly et al. 38 [reporting a mean value of 10.58° (±5.12) for C0–C2ART in supine]. These differences can be explained by the ROM measurement (smartphone app for Satpute et al. 37 an MRI measurement after maintaining the end position of the test during 3 min for Osmotherly et al. 38 and a CROM device for our study). Also, differences in how C2 was stabilized by examiners, and patient position, and participant ethnicity 61 could partly explain these ROM differences. Clearly, the values from these studies are far from the largest physiological ROM considered clinically normal for the rotation stress test (35–40°) with a firm end feel. 62 Bosczcyk et al. 63 concluded that coupled motion in the frontal and sagittal planes might be necessary to explain the physiological UC rotation ROM. This may partly explain the limited UC rotation ROM during the C0–C2ART in our study, as no coupled motions are allowed during the test. Also, our values reinforce the idea that the threshold ROM values for considering an unstable UC spine should be revisited as Osmotherly et al. 38 described.
The values obtained in this study allow clinicians to have a reference to compare the ROM of the different UC rotation tests in healthy and subclinical neck subjects. Knowing the relationship among the different rotation tests will allow the therapist to choose the most suitable test according to the patient’s characteristics.
Correlations
This study performed a correlation analysis to understand better the relationship among FRT, SBRT and C0–C2ART for the measurement of passive UC rotation ROM. The main difference among them is the type of stabilization of C2 and the lower cervical segments. While the FRT prepositions all cervical segments in maximal flexion and SBRT in maximal opposite side bending to the tested rotation, C0–C2ART stabilizes C2 manually in the neutral position. Theoretically, this means that C0–C2ART measures UC rotation from a neutral position and isolates UC rotation more than the FRT and SBRT. Both FRT and SBRT measure rotation from a flexed or side bent UC starting position while tightening all upper and lower cervical articular and peri-articular tissues.
This study found significant correlations among all UC tests with the ACROM Rot but with differing degrees of correlation. Approximately 60% of the cervical rotation ROM is believed to occur in the UC.9,10 FRT showed a stronger correlation (0.55–0.58) while C0–C2ART (0.38–0.41) and SBRT (0.38–0.22) showed a moderate and weak correlation with ACROM Rot. These results may reinforce FRT for measuring UC rotation in asymptomatic/subclinical subjects. Takasaki et al. 30 validated that UC segments maintained 73.5% of their rotation during FRT compared to cervical rotation from a neutral position in asymptomatic subjects. However, in the same study, FRT kept more than 25% of the rotation of C2 and lower segments during the test, which may also influence its strong correlation with ACROM Rot. FRT is the most validated clinical test for diagnosing cervicogenic headache. 31 However, more studies are needed to validate FRT for measuring UC rotation in patients with symptoms and dysfunction. C0–C2ART only showed a moderate correlation with ACROM Rot. Lorente et al. 64 reported less movement using a combination of rotation in flexion compared to axial rotation and rotation in extension in vitro. The most frequent coupled movements associated with UC rotation are contralateral side bending and extension10,23,26–28,65,66 C0–C2ART uses axial rotation, which can limit the amount of UC rotation measured during the test and C0–C2ART correlation with ACROM Rot as UC coupled movements are not considered.
Moderate and weak correlations and a large discrepancy in ROM were found among the UC rotation tests. These low levels of correlation and discrepancy in ROM may be related to the prevention of the inherent coupling of rotation and side bending in the C0–C2 segments. FRT and SBRT allow C2 to move with UC rotation, reduce the tightening of the alar ligament system, allowing a larger ROM. C0–C2ART would not allow C2 movement throughout the test preventing this coupling of C2 motion 67 and limiting UC rotation during this test. This may explain the FRT three times larger than C0–C2ART found by Satpute et al. 37 In this study, this proportion was even larger. More studies are needed for a better understanding of the biomechanics of different tests.
Results by sex showed a significant relationship in the LRMs only for ACROM Rot right, left SBRT, and right and left C0–C2ART in the adjusted models. Although males showed less average ROM than females in all movements, sex did not show any relationship with the remaining tests. In ACROM Rot, Youdas et al. 43 found a linear regression coefficient for sex of −4.4° (right rotation) and −2.2° (left rotation). These values for right and left rotation are similar to our results (−4.64° right rotation, −2.7° left rotation), but only the right rotation achieved significance in this study. Similar to Schäfer et al., 34 we found no relationship between FRT and sex. No studies have investigated the relationship between sex with SBRT or C0–C2ART. We found a relationship through LRMs of −4.1° (CI 95%: −7.97 to −0.23; p = 0.038) for left SBRT but not for the right SBRT −3.62° (CI 95%: −7.92 to 0.69; p = 0.099). A reduced C0–C2ART ROM has been observed in men with a linear regression coefficient of −2.24° (CI 95%: −3.24 to −1.25; p < 0.001) for right rotation and −1.78 (CI 95%: −2.79 to −0.76; p = 0.001) for left rotation.
Results by age strata
Dvorak et al. 45 and Smith et al. 19 stated that age did not affect the UC ROM. Only SBRT ROM remained stable over the age strata. This is the first study to examine the interaction of age with SBRT. Lemmers et al. 3 observed changes in motion coupling associated with age, noting increases in side bending with age. This compensatory movement may explain the continued preservation of SBRT ROM with increasing age. However, our study found that age is related with the loss of motion in ACROM Rot, FRT and C0–C2ART. Changes may be explained partly by age-related degenerative changes. 68 In ACROM Rot, Youdas et al. 43 found a coefficient of regression for each year of age of −0.4° and −0.3° for the right and left rotation. Those values are greater than our finding of −2.11°and −1.96° per decade for right and left rotation. Those differences may be due to the broader age periods measured in Youdas et al. 43 Also, they adjusted the effect of sex in both values. We only performed similarly for right rotation because sex did not show any significance in the models for left rotation. Pan et al. 4 stated that age-related changes in cervical AROM are not continuous and differ between males and females. In FRT, previous studies have stated that age did not influence the ROM19,45 but, recently, Schäfer et al. 34 found a loss of ROM in FRT of −2.9° (95% CI: −3.9 to −1.9) in right FRT and −2.6° (95% CI: −3.5 to −1.6) for left FRT for each decade. This is consistent with our results that showed a loss of motion related with age, but the loss is smaller in our sample [−1.72 (CI 95%: −2.53 to −0.9) for right FRT and −1.26 (CI 95%: −1.94 to −0.57) for left FRT] for each decade. Those differences are possibly related to the older ages included in the study of Schäfer et al. 34 In C0–C2ART, we observed a decrease of ROM related to age.
The description and correlation results among the ACROM Rot, FRT, SBRT and C0–C2ART in the same sample allow the comparison of normal UC rotation ROM among these tests. FRT is the most validated test for detecting UC ROM dysfunction, but clinical conditions may contraindicate FRT due to lack of cervical flexion tolerance, and SBRT or C0–C2ART may be used instead. This study reports novel data about the relationship between age and sex with SBRT and C0–C2ART.
Limitations
Only one examiner performed the evaluation limiting the generalizability of the results. We cannot extrapolate the ROM data to other populations with different inclusion and exclusion criteria. External validity is limited by the non-stratified sample size, and the cross-sectional design conducted in a single location. Intratester reliability for SBRT has not been described previously, so results for SBRT test must be interpreted with caution. As this study is descriptive and correlative, we cannot establish a cause–effect relationship. More studies are needed to determine which motions are involved throughout each different UC rotation test.
Conclusion
The ROM values for the FRT, SBRT and C0–C2ART had moderate-to-weak correlations, with a large discrepancy of UC rotation ROM among them. Women tend to have larger ROMs in all tests, but only ACROM Rot right, SBRT left and C0–C2ART showed statistical significance. ACROM Rot, FRT and C0–C2ART demonstrated a decreased ROM with age. SBRT did not demonstrate a decrease in ROM with age.
Supplemental Material
sj-docx-1-taj-10.1177_20406223231170158 – Supplemental material for Association between age, sex and cervical and upper cervical rotation tests. Descriptive and correlational study in healthy volunteers
Supplemental material, sj-docx-1-taj-10.1177_20406223231170158 for Association between age, sex and cervical and upper cervical rotation tests. Descriptive and correlational study in healthy volunteers by Carlos Zárate-Tejero, César Hidalgo-García, Orosia Lucha-López, Mar Hernández-Secorún, John Krauss and Pere Rodríguez-Rubio in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-2-taj-10.1177_20406223231170158 – Supplemental material for Association between age, sex and cervical and upper cervical rotation tests. Descriptive and correlational study in healthy volunteers
Supplemental material, sj-docx-2-taj-10.1177_20406223231170158 for Association between age, sex and cervical and upper cervical rotation tests. Descriptive and correlational study in healthy volunteers by Carlos Zárate-Tejero, César Hidalgo-García, Orosia Lucha-López, Mar Hernández-Secorún, John Krauss and Pere Rodríguez-Rubio in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-3-taj-10.1177_20406223231170158 – Supplemental material for Association between age, sex and cervical and upper cervical rotation tests. Descriptive and correlational study in healthy volunteers
Supplemental material, sj-docx-3-taj-10.1177_20406223231170158 for Association between age, sex and cervical and upper cervical rotation tests. Descriptive and correlational study in healthy volunteers by Carlos Zárate-Tejero, César Hidalgo-García, Orosia Lucha-López, Mar Hernández-Secorún, John Krauss and Pere Rodríguez-Rubio in Therapeutic Advances in Chronic Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.