
Abstract
Cardiovascular disease (CVD) causes millions of deaths worldwide each year. Despite the great progress in therapies available for patients with CVD, some limitations, including drug complications, still exist. Hence, the endocannabinoid system (ECS) was proposed as a new avenue for CVDs treatment. The ECS components are widely distributed through the body, including the heart and blood vessels, thus the action of its endogenous and exogenous ligands, in particular, phytocannabinoids play a key role in various pathological states. The cardiovascular action of cannabinoids is complex as they affect vasculature and myocardium directly via specific receptors and exert indirect effects through the central and peripheral nervous system. The growing interest in phytocannabinoid studies, however, has extended the knowledge about their molecular targets as well as therapeutical properties; nonetheless, some areas of their actions are not yet fully recognized. Researchers have reported various cannabinoids, especially cannabidiol, as a promising approach to CVDs; hence, the purpose of this review is to summarize and update the cardiovascular actions of the most potent phytocannabinoids and the potential therapeutic role of ECS in CVDs, including ischemic reperfusion injury, arrhythmia, heart failure as well as hypertension.
Keywords
Introduction
Cardiovascular diseases (CVDs) remain a leading cause of morbidity and mortality worldwide. 1 CVDs are chronic diseases that are often asymptomatic for a prolonged period, although in many cases, the first symptom can be sudden death.2–4 It is estimated that CVDs account for approximately 18.6 million deaths annually. 1 Moreover, according to the World Health Organization (WHO), three-quarters of all CVD mortality may be avoided by proper prevention focusing on risk factors including smoking habit, increased body mass, physical (in)activity, arterial hypertension, dyslipidemia, and type 2 diabetes mellitus.2,5 However, here are some invariable risk factors, which cannot be influenced, such as age, sex, or genetic heritage. 6 Among the most commonly used drugs in CVDs prevention are angiotensin-converting enzyme (ACE) inhibitors (diminishing blood pressure), statins (reducing cholesterol biosynthesis), and beta-blockers. 7 Nonetheless, the use of five and more medications, frequently occurring in CVD patients, may trigger adverse outcomes or potential drug interactions. 8 It is now clear that the endogenous cannabinoid system displays a pleiotropic effect and is responsible for regulating homeostasis, which underlines its role in various pathologies, including CVDs. Phytocannabinoids (pCBs), natural components of the Cannabis sativa plant, exert their action via modulation of the endocannabinoid system (ECS). 9 Great interest in the therapeutical use of pCBs proved that their action is complex and not only limited to cannabinoid receptors, as it is presented in this review. Thus, the ECS, together with pCBs, seems to be a promising target to obtain a novel approach for CVD prevention and treatment.
The ECS
The ECS is an inner signaling system composed of endogenous cannabinoids (eCBs), their specific receptors, and enzymes responsible for their metabolism. 10 The best-characterized cannabinoid receptors are CB1 and CB2, which are G-protein–coupled receptors (GPCR). The CB1 receptor is widely expressed in the central nervous system; however, it is also found in the peripheral nervous system as well as other tissues, such as adipose tissue, liver, cardiac muscle, and blood vessels. Activation of the myocardial CB1 receptor results in a negative inotropic effect – diminishing myocardial contractility, as well as lowering blood pressure,11,12 whereas activation of these receptors in vascular endothelial cells leads to vasodilation and participates in the process of proliferation and migration of vascular smooth muscle cells (Figure 2).11,13 In contrast, the CB2 receptor is mainly expressed on blood cells and immune tissues, and its activation is involved in the regulation of immune cell function, for instance, controlling acute inflammatory response. 14 Recent studies have also demonstrated the expression of CB2 receptor within the cardiovascular system, namely, rat cardiomyocytes 15 and human endothelial cells,16,17 in which it was shown that its activation plays a cardioprotective role, especially in postischemic reperfusion injury. 18 eCBs, also called endocannabinoids, are bioactive lipid mediators that act as ligands of the above-mentioned cannabinoid receptors. They are represented by anandamide (AEA) and 2-arachidonyl glycerol (2-AG), which share a common, arachidonate-based structure.4,19–22 The main enzymes responsible for their metabolism are fatty acid amide hydrolase (FAAH), metabolizing AEA to free arachidonic acid and ethanolamine, as well as monoacylglycerol lipase (MAGL), converting 2-AG to free arachidonic acid and glycerol.10,23 Broad studies on ECS demonstrated its complexity and involvement in a wide range of other metabolic pathways. Therefore, the expanded ECS is nowadays known as the endocannabinoidome (eCBome). 24 Recent studies revealed that eCBs and pCBs also interact with two orphan GPCRs, that is, GPR55 and GPR18, as well as peroxisome proliferator–activated nuclear receptors (PPARs), mainly PPARγ and PPARα, and selected ion channels, namely, transient receptor potential vanilloid 1 (TRPV1). 25 Owing to its pleiotropic effect and ubiquitous occurrence, the ECS is considered to be a key player in many physiological and pathological states.
Both CB1 and CB2 receptors are involved in CVDs pathophysiology, albeit in an opposite manner. As several studies indicated, in various pathological states, when the ECS is dysregulated, AEA, a CB1 agonist, may promote ROS (reactive oxygen species) generation and mediated by activation of MAPK (mitogen-activated protein kinase) cell death pathway, contributing to the development of numerous CVDs.26,27 On the contrary, activation of the CB2 receptor by 2-AG exerts a cardioprotective effect, which was demonstrated in a rat model of ischemia–reperfusion. 28 In addition, infracted CB2−/− mice exhibited lower ejection fraction, an increased lymphocyte B count along with neutrophil infiltration in the heart compared with infracted mice with the expression of the CB2 receptor. 29 Altogether these examples show that the agonism of the CB1 receptor and the antagonism of the CB2 receptor are unfavorable. The mechanism of cardiovascular modulation by cannabinoids is complex and involves both a direct effect on blood vessels and cardiac muscle, as well as autonomic regulation through the central and peripheral nervous system. Thus, the ECS is believed to be a therapeutic target for various CVDs such as hypertension, atherosclerosis, cardiomyopathy, myocardial infarction, or arrhythmia.30,31
PCBs
Undoubtedly, Cannabis is the most commonly cultivated, trafficked, and consumed, both for its physiological and psychoactive effects, drug in the world. According to WHO, nearly 2.5% of the world population uses Cannabis. 32 Hashish or marijuana, derived from the plant Cannabis sativa, has a long history of use among many cultures, both for its therapeutic and psychotropic properties. 33 The Cannabis plant contains approximately 113 cannabinoids, namely, pCBs; however, the proportion of each constituent varies depending on plant variety, geographic location, or growth conditions. 34 The most abundant and thoroughly studied pCBs are Δ9-tetrahydrocannabinol (Δ9-THC) and cannabidiol (CBD), whereas examples of the lesser-known include cannabinol (CBN), cannabigerol (CBG), cannabichromene (CBC), Δ9-tetrahydrocannabivarin (THCV), cannabivarin (CBV), or cannabidivarin (CBDV). 35
CBD
CBD is a major non-psychotropic Cannabis compound, which currently gains a great interest due to its antioxidant, analgesic, anti-anxiety, anti-convulsant, anti-nausea, anti-inflammatory, anti-arthritic, or anti-tumor effects, among others.36–39 CBD displays a very low affinity for CB1 and CB2 receptors. 40 Recent studies, however, suggest that the pCB acts as a negative allosteric modulator of the CB1 receptor as well as a partial agonist of the CB2 receptor, which may explain some of its effects on the organism40–42 (Table 1). Nevertheless, CBD exerts most of its actions by multiple mechanisms, such as the ability to inhibit activation and cellular uptake of endogenous CB receptors ligand – AEA, affecting endocannabinoid tone, which is the baseline activity of the ECS. 35 Cardiovascular events may also be triggered by the proliferation and migration of vascular smooth muscle cells induced by inflammation. Schwartz et al. 43 have proven that CBD exerts anti-proliferative and anti-migratory properties in human umbilical artery smooth muscle cells; however, the exact mechanism of these actions remains largely unclear (Figure 2). CBD also blocks the orphan GPCR – GPR55, which was demonstrated to play a role in innate immunity modulation and inflammation.44,45 The latest study underlines the important role of the GPR55 receptor in regulating cardiac homeostasis as well as responses to ischemia. 46 Other crucial targets for CBD are ion channels belonging to the transient receptor potential (TRP) family. A growing body of evidence suggests their contribution to physiological and pathological responses in the vasculature, including endothelium-dependent vasodilation, angiogenesis, or regulation of vascular tone. 47 TRP channels of the ankyrin type-1 (TRPA1), TRPV1, and TRPV2 are activated by CBD,48,49 while the TRP channel of melastatin type 8 (TRPM8) is antagonized by this pCB. 49 Moreover, CBD influences the heart Ca2+ homeostasis via L-type channels located in ventricular myocytes as well as Na+/Ca2+ exchanger in cardiomyocyte mitochondria, modulating myocyte contractility and protecting the ionic balance of calcium.50,51 Thus, CBD interactions with the above-mentioned ion channels may exert protective function under pathological conditions such as arrhythmia or infarction. 51 PPARs also play a pivotal role in the metabolism of cardiac substrates. All three isoforms of the aforementioned receptors are expressed in the heart; however, PPARγ is less abundant than α and β/δ isoforms. 52 CBD displays a weak/partial agonism to PPARγ, which induces a positive cardiovascular effect, for instance, a time-dependent vasorelaxation of the rat aorta. 53 Other actions following PPARγ activation by CBD include lowering blood pressure or increasing nitric oxide concentration. 54 There is also evidence that CBD acts as a weak activator of the 5-HT1A (serotonin 1A) receptor. In the experiment conducted by Resstel et al., 55 CBD diminished tachycardic response to uncontrolled stress in rats, namely, increased blood pressure and heart rate, and these effects were blocked by a 5-HT1A receptor antagonist. Other proposed targets of CBD include such receptors as α1 and α1β glycine, α1-adrenergic, dopamine D2 as well as µ- and δ-opioid.56–59 Briefly, α1-adrenergic receptors, located within the coronary arteries, are important modulators of vascular tone as well as exert protective outcomes in the heart through augmentation of adaptive hypertrophy and positive inotropy. 60 Dopamine receptor D2 is engaged in regulating blood pressure as well as controlling the function of the cardiac muscle. 61 Glycine receptor was found to exert a protective effect in myocardial cells, 62 whereas δ-opioid receptors not only influence systemic vascular tone but also impact cardiovascular autonomic balance. 63 Finally, cardiac μ-opioid receptors were proposed as a potential target in the treatment of myocardial ischemia-reperfusion injury during doxorubicin-induced chronic heart failure. 64 Despite the great potential of described receptors in targeting CVDs, their interaction with CBD is not yet fully recognized and needs further investigation.
Mechanisms of action of the most common phytocannabinoids.
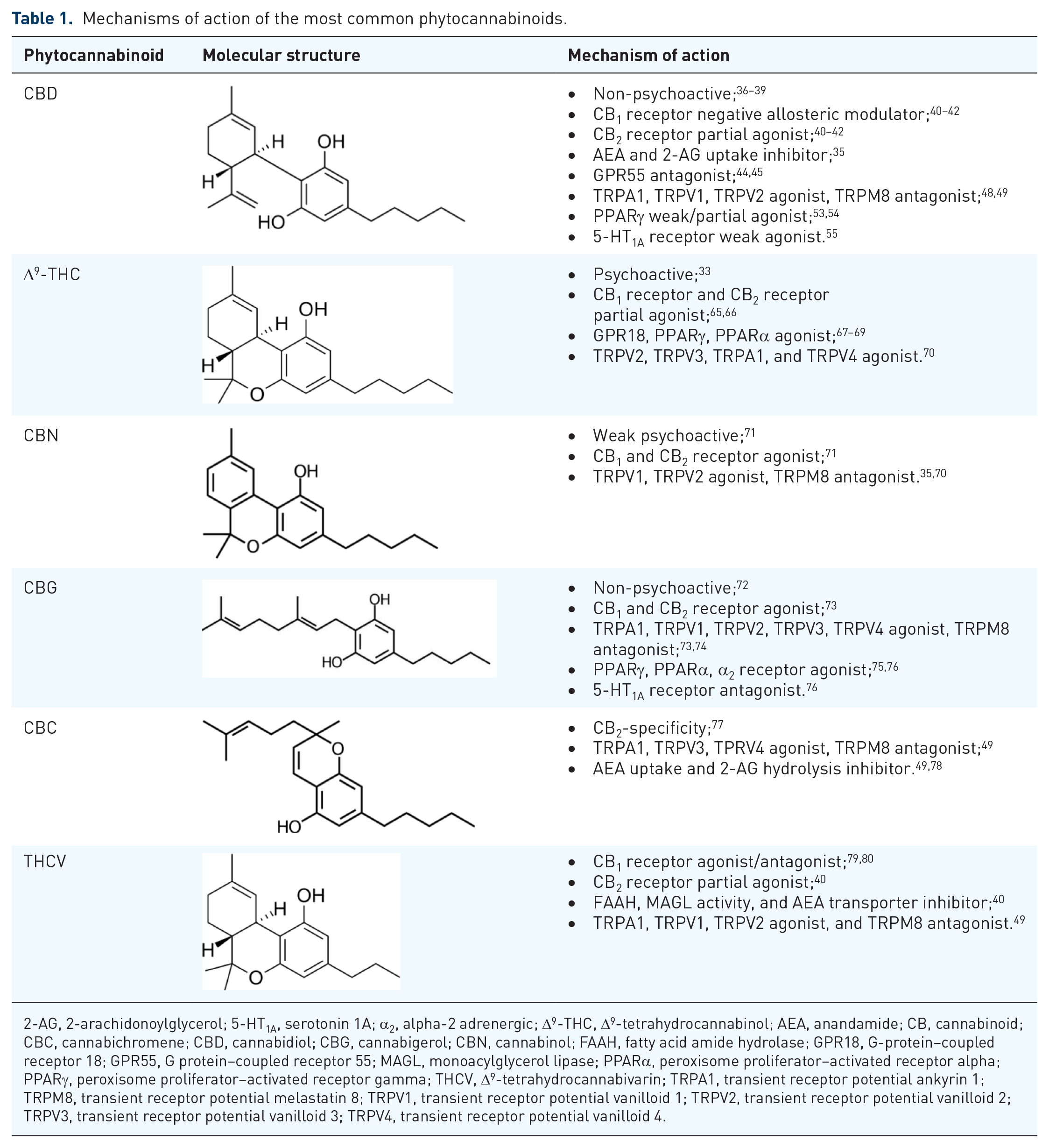
2-AG, 2-arachidonoylglycerol; 5-HT1A, serotonin 1A; α2, alpha-2 adrenergic; Δ9-THC, Δ9-tetrahydrocannabinol; AEA, anandamide; CB, cannabinoid; CBC, cannabichromene; CBD, cannabidiol; CBG, cannabigerol; CBN, cannabinol; FAAH, fatty acid amide hydrolase; GPR18, G-protein–coupled receptor 18; GPR55, G protein–coupled receptor 55; MAGL, monoacylglycerol lipase; PPARα, peroxisome proliferator–activated receptor alpha; PPARγ, peroxisome proliferator–activated receptor gamma; THCV, Δ9-tetrahydrocannabivarin; TRPA1, transient receptor potential ankyrin 1; TRPM8, transient receptor potential melastatin 8; TRPV1, transient receptor potential vanilloid 1; TRPV2, transient receptor potential vanilloid 2; TRPV3, transient receptor potential vanilloid 3; TRPV4, transient receptor potential vanilloid 4.
Δ9-THC
Δ9-THC is the primary compound of Cannabis responsible for many of the adverse effects associated with Cannabis use. 33 The psychotropic effects of Δ9-THC result from its action as a partial agonist of the CB1 receptor, abundantly located in the central nervous system. The aforementioned receptor is also expressed in various organs, including the heart, kidney, liver, and lungs. 65 In addition, this pCB displays a partial agonism toward cannabinoid receptor – CB2. 66 Besides the receptors mentioned above, Δ9-THC was found to act on other targets, like GPR18, which is suggested to be classified as another cannabinoid receptor subtype (Table 1). 67 Matouk et al. 81 demonstrated GPR18 presence in the heart, in which its activation improved left ventricular function, diminished cardiac sympathetic dominance, and resulted in hypotension. GPR18 receptor ligands exert a favorable effect on cardiovascular function; thus, the impact of Δ9-THC on these receptors in the heart and vasculature is advised to be identified. Similar to CBD, Δ9-THC acts as PPARγ ligand, resulting in a time-dependent vasorelaxation in animal models; however, the vascular effect of Δ9-THC could be a result of direct activation of PPARγ or indirect influence involving prostanoids. 68 There are studies showing upregulation of PPARα caused by Δ9-THC; the isoform is mainly expressed in the heart, muscle, liver, or adipose tissue. 69 Moreover, activation of PPARα by its agonists under altered conditions such as pressure overload or ischemia improves endothelial cell function as well as diminishes cardiac fibrosis and hypertrophy in animal models.82–84
Although this pCB does not affect the TRPV1 channel, it acts as an agonist of TRPV2, TRPV3, and TRPV4 as well as TRPA1 channels. 70 Besides the aforementioned role of TRP channels in regulating vascular response, dysregulation of another channel – TRPV4 – has been associated with endothelial dysfunction that can be considered a CVD risk factor. Therefore, the activation of TRPV4 might serve as a possible strategy for CVD treatment.85,86 Other molecular targets affected by Δ9-THC include glycine, 87 µ- and δ-opioid receptors, 88 the cardioprotective role of which was mentioned above. Cardiovascular effects of Δ9-THC in humans encompass a rapid, dose-dependent increase in heart rate (Figure 1). In addition, an increase in blood pressure may occur, but rarely blood pressure is diminished.89–94 Albeit Δ9-THC exerts many therapeutic effects mainly due to its multitarget actions, stimulation of CB1 receptor and following psychotropic activity is the main drawback limiting therapeutic use of this pCB.

Effects of cannabidiol and Δ9-tetrahydrocannabinol on the cardiac muscle.
CBN
CBN is a weak psychoactive pCB and oxidized metabolite of Δ9-THC, mostly found in aged Cannabis. It influences CB1 and CB2 receptors in the central nervous system as well as in the peripheral organs, with a higher affinity toward CB2 receptors. 71 Ex vivo studies presented the cardiac effect of CBN, namely, decreasing heart rate in the perfused rat hearts, 102 albeit in in vivo studies conducted on rats and humans, this pCB did not display such activity.103,104 Its anti-inflammatory, antioxidant, and analgesic effects mainly result from agonism of CB2, TRPV1, and TRPV2 receptors as well as antagonism of TPRM8 channels (Table 1).35,70 Activity toward the above-mentioned receptors could exert a possible role in cardiovascular health as TRP channels are engaged in the regulation of vascular response and activated CB2 receptor has a protective role in the heart. Yet, the exact role of CBN in the cardiovascular system, regarding its acute and chronic effects on the heart and vasculature, requires broader research. Further studies should include studies conducted on cell lines, such as AC16 – human cardiomyocytes, H9c2 – rat cardiomyoblasts, or HL-1 cardiac muscle cell line derived from the AT-1 mouse atrial cardiomyocytes, as well as isolated primary cardiomyocytes, followed by in vivo experimental models on animal and human studies.
CBG
Another non-psychoactive constituent of the Cannabis plant, CBG was isolated and characterized by Gaoni and Mechoulam, 72 the same researchers who discovered the structure of Δ9-THC in 1964. CBG exhibits certain similarities to both Δ9-THC and CBD. It demonstrates an agonistic effect on cannabinoid receptors CB1 and CB2, however, with lower binding affinity in comparison with Δ9-THC. 73 Simultaneously, CBG affinity toward six TRP cation channels TRPA1, TRPV1, TRPV2, TRPV3, TRPV4, and TRPM8 makes it comparable with CBD (Table 1).73,74 CBG is analogous to CBD by being a PPARγ agonist and activating PPARα. 75 It should be underlined that CBG is a potent α2-adrenoceptor agonist and till now no other pCB has been shown to display such activity. Peripheral α2 agonists, affecting receptors located in vascular endothelium, display antihypertensive activity, which implies the potential similar therapeutic application of CBG. Like other α2-adrenoceptor ligands, CBG binds to the 5-HT1A receptor, acting as an antagonist. 76 Central 5-HT1A receptors have a key role in the regulation of cardiovascular reflexes, as their activation leads to the diminishment of blood pressure and heart rate. 105 There is still a lack of studies describing the effects of CBG on the cardiovascular system; however, according to one research, the pCB can inhibit agonist-induced primary and secondary platelet aggregation, 106 which may be considered a promising treatment approach in CVD states, primarily when the platelet aggregation is altered, including myocardial infarction or ischemic events. 107
CBC
CBC is abundantly found in freshly harvested dry-type Cannabis and is known to be the second most plentiful cannabinoid in selected marijuana strains grown in the United States. 108 Despite this, little is known about CBC’s pharmacological effects. Previous studies reported very low affinity to CB1 and CB2 receptors. 109 Although recently Udoh et al. 77 have demonstrated CB2 receptor-specificity for CBC in AtT20 cells with concomitant no effect on CB1 receptor in the same research. In addition, CBC is known to influence the TRP channels, being the agonist of TRPA1, TRPV3, and TRPV4 and antagonist of TRPM8 receptors (Table 1). 49 This pCB also inhibits AEA uptake and 2-AG hydrolysis, although in a weak manner.78,110 In the cardiovascular system, CBC was found to produce a hypotensive effect and cause a reduction in the respiration rate in rats, and importantly, when administered together with Δ9-THC was shown to potentiate the decrease in the heart rate. It was still uncertain whether the described effect was triggered by the compounds themselves or by one of their metabolites. 111 The mentioned results were published in 1979, and nowadays, Δ9-THC has a well-established opposing effect. Multiple studies confirmed the increased heart rate after Δ9-THC administration, which was homogeneous irrespective of routes of administration – oral, intravenous, or inhaled.93,94,112,113 Thus, further studies should be conducted to update and verify the above-mentioned results and determine the exact effect of the CBC on the cardiac muscle as well as vasculature, which would substantially broaden the knowledge in this area.
THCV
THCV is a propyl analog of Δ9-THC, varying from Δ9-THC only by the length of its lipophilic alkyl chain, however, possessing different pharmacological effects.40,114 Discrepancies regarding THCV activity toward the CB1 receptor were found. In in vivo experiments, it was demonstrated that THCV activates the CB1 receptor, albeit to a lesser potency than Δ9-THC. Yet the studies also confirmed that this pCB can behave as a CB1 receptor antagonist both in in vivo and in vitro conditions, in a dose-dependent manner.79,80 In contrast, THCV toward CB2 receptor acts as a partial agonist and may also indirectly influence ECS, increasing endocannabinoid tone, by inhibiting AEA transporter as well as FAAH and MAGL activity.
40
Inhibition of both enzymes results in a prolonged activity of AEA and 2-AG, which might exert opposite effects on the cardiovascular system. Therefore, the exact mechanism of action of THCV should be thoroughly examined. Several studies indicate THCV interactions with ‘thermo-TRP’ channels, for instance, TRPA1, TRPV1, TRPV2 agonism, and TRPM8 antagonism (Table 1).
49
Important findings also revealed its capability to modulate the activity of the 5-HT1A receptor, which is involved in cardiovascular regulation,
115
as well as GPR55 together with inhibition of the activity of LPI (
CVDs
Ischemic reperfusion injury
Ischemia and reperfusion is a condition described as a limitation in blood supply to the organ, which causes a shortage of oxygen – ischemia – followed by restoration of blood flow, usually associated with deterioration of tissue injury and consequent reoxygenation during reperfusion. This state is the major cause of tissue damage in a broad spectrum of pathologies, including myocardial infarction, as the restoration of the coronary blood flow promotes the activation of immune responses as well as cell death programs. 118 Durst et al. 95 were the first who demonstrated the cardioprotective effect of CBD against myocardial infarction in vivo. Administration of CBD to rats caused a reduction of infarct size, cardiac inflammation, and serum interleukin-6 (IL-6) level after left anterior descending coronary artery ligation in an animal model of ischemic reperfusion injury (IRI). Noteworthy, CBD did not exert such effects in in vitro experiment, which suggests that these actions are not due to the direct influence on the cardiac muscle but rather immunomodulatory response, possibly related to adenosine signaling in immune cells. 95 Similar alterations were confirmed on a rabbit model. In this study, two intravenous doses of CBD (100 µg/kg of body weight) were applied before the appearance of left circumflex coronary artery occlusion and reperfusion. Application of CBD caused a reduction in cardiac troponin I (cTnI) concentration in the blood, and significantly increased blood flow in the affected area of the heart muscle – the myocardial tissue within the vascular territory, distally to the culprit lesion of the infract-related coronary artery; as well as decreased infiltrating neutrophils and neutrophil myeloperoxidase (MPO) activity, protecting against IRI (Figure 1). 96 Several studies also suggest a protective role of CB2 receptor in discussed above disorder;12,119,120 however, the exact mechanism underlying this action is not yet clarified. In the experiment conducted by Li et al., 121 the CB2-selective receptor agonist, JWH133 was found to reduce the infarct size of the rat myocardium affected by IRI. Activation of CB2 receptor resulted in the inhibition of intrinsic, mitochondria-mediated apoptotic pathway through activation of phosphoinositide 3-kinase–protein kinase/Akt (PI3K/Akt) signaling pathway, which may be the partial mechanism responsible for the observed cardioprotective effect. In addition, TRP channels, especially vanilloid receptors located on the sensory nerve endings of the heart, were found to sense myocardial ischemia as well as activate cardiac nociceptors in male ferrets, plausibly by the ability to function as transduction molecules. 122 It was shown that activation of TRPV1 is involved in cardioprotection during IRI via increasing substance P release from capsaicin sensory neurons and developing cardiac adaptation to ischemic stress. 123 Interestingly, ultra-low doses of Δ9-THC (0.002 mg/kg of body weight), which do not induce any psychotic side effects, given before myocardial infarction in mice, exerted cardioprotective activity, namely, reduction of the infarct size, diminishment of the level of cTnI in the plasma, or neutrophil infiltration to the heart tissue (Figure 1). 97 Yet another study reported that the protective effect of ischemic preconditioning on the endothelial function of the isolated rat heart requires activation of CB1 and CB2 receptors. 124 Other pCBs are not as thoroughly studied as CBD and Δ9-THC, wherefore their activity in cardiovascular disorders is not yet fully understood. However, their molecular targets and mechanisms of action, described in the previous part, suggest a potential protective role in IRI.
Arrhythmia
Cardiac arrhythmia refers to any alternations in a physiological sequence of the electrical impulses in the intrinsic conduction system of the heart. According to their origin, two main groups of arrhythmias may be distinguished: supraventricular – developing at the level of the bundle of His or above and ventricular – constituting the most common type. 125 The studies revealed that endocannabinoids can reduce arrhythmic events mainly via CB2 receptor signaling.126,127 Hence, AEA was demonstrated to possess significant anti-arrhythmic properties. This effect was proven by the administration of SR 144528, a CB2 receptor antagonist, but not a CB1 receptor antagonist – SR 141716A – rimonabant, an anti-obesity drug, which was withdrawn from the European market due to the adverse psychiatric and neurological effects, including depression, anxiety, or headaches, resulting from its influence on receptors located in the central nervous system. Another CB2 receptor agonist, HU-210, was able to reverse cardiac arrhythmia by as much as 90% in an ischemic model as well as epinephrine and aconitine–induced model.128,129 Noteworthy, the CB2 receptor also plays a crucial role in limiting ischemia-induced arrhythmia in ischemic preconditioned rat hearts. The protective effect of remote ischemic preconditioning was again blocked by the CB2 receptor antagonist AM 630 but not by the CB1 antagonist AM 251, highlighting the protective role of the CB2 receptor in cardiac arrhythmia. 126 In the experiment conducted by Gonca and Darıcı 98 on Wistar rats, CBD presented an anti-arrhythmic effect in ischemia/reperfusion–induced arrhythmias, probably by activating the adenosine A1 receptor. In this study, the duration of ventricular tachycardia, as well as arrhythmias, were markedly diminished. In addition, cardiac complications, including arrhythmia, may be caused by hyperglycemia. 98 The study conducted on Chinese hamster ovary cells incubated in the presence of elevated glucose in the cell medium proved that CBD alleviates the effects of high concentrations of glucose on cells, such as oxidative stress or cell death (Figure 1). Authors suggest that this protective effect of CBD might result from an inhibition of Nav1.5 (one of the cardiac sodium channel isoforms). 130 There is still a lack of studies presenting the role of pCBs other than CBD in cardiac arrhythmia. The protective role of endocannabinoid components indicates a potential role of Cannabis constituents in described disorders.
Heart failure and cardiomyopathy
Heart failure, the syndrome caused by cardiac dysfunction, results from many pathologic conditions affecting cardiac muscle, including coronary artery disease, arterial hypertension, valvular disease, diabetic cardiomyopathy, or myocarditis. 131 Both heart failure and cardiomyopathies are characterized by alterations in cardiomyocytes and vascular cells structure, including hypertrophy or fibrosis. They are accompanied by increased levels of oxidative stress and inflammation markers in the blood and endothelial cells, that is, nitrotyrosine, cyclooxygenase-2 (COX-2), or inducible nitric oxide synthase (iNOS).132,133 In patients with chronic heart failure, changes in the expressions of CB1 and CB2 receptors in the myocardium have been observed. The expression of the CB1 receptor was diminished, whereas the expression of the CB2 receptor was elevated. In addition, the levels of endogenous ECS ligands AEA and 2-AG were also enhanced. 134 Upregulation of the expression of CB2 receptors might serve as a beneficial compensatory mechanism due to its protective properties against heart failure, that is, anti-apoptotic, anti-fibrogenic, and anti-hypertrophic effects. 135 The study conducted by Rajesh et al. 99 indicated the favorable role of CBD in a model of diabetic cardiomyopathy conducted on primary human cardiomyocytes and mice. The pCB was able to diminish elevated ROS generation and activation of nuclear factor kappa B (NF-κB), which are known of contributing to cardiac dysfunction as well as cell death in primary human cardiomyocytes exposed to high glucose concentration. The same effect of CBD was also observed in the murine model, in which the oxidative–nitrative stress (myocardial ROS and nitrotyrosine formation), along with cell death and fibrosis in cardiac tissue, was decreased (Figure 1). 99 The positive effect of CBD was also shown in cardiomyopathy induced by doxorubicin (cytotoxic anthracycline antibiotic) in a rodent model. Chronic administration of CBD diminished nitric oxide level, serum creatine kinase-MB, troponin T, and calcium ion concentrations as well as attenuated the reduction in cardiac selenium and zinc levels in examined rats. Furthermore, the cardiac expressions of NF-κB, iNOS, and tumor necrosis factor-α (TNF-α) were significantly decreased, whereas the expression of survivin was increased, protecting against doxorubicin-induced cardiac injury. 100 Furthermore, a similar experiment conducted on the murine model of cardiomyopathy induced by doxorubicin indicated that CBD attenuates the decrease in cardiac mitochondrial DNA copy number with a simultaneous elevation of mitochondrial biogenesis. Besides, CBD reduced oxidative stress (myocardial iNOS expression, nitrotyrosine formation, and lipid peroxidation), cell death, and improved cardiac dysfunction in the above-mentioned pathology (Figure 1). 101 There is still a lack of studies indicating the role of other Cannabis compounds, including CBN, CBG, or THCV on the aforementioned disorders. Nevertheless, their molecular targets and anti-inflammatory properties suggest a potential role in the treatment and prevention of heart failure and cardiomyopathy. Hence, a need arises to thoroughly investigate the role of pCBs in both in vitro and in vivo studies, and most importantly, in a human model.
Hypertension
Primary studies evaluating cardiovascular actions of Δ9-THC in normotensive and hypertensive animals demonstrated very inconsistent results. In the experiment by Ho et al., 136 the diminishment in the blood pressure occurred in non-obese normotensive rats exposed to this pCB for a prolonged period – 5 and 6 weeks. On the contrary, normotensive lean dogs chronically exposed to Δ9-THC did not develop any significant changes in the blood pressure. 137 Another experiment presented that Δ9-THC decreased the blood pressure in adrenal regeneration hypertensive rats. 138 In addition, Nahas et al. 139 reported the development of tolerance to the hypotensive effect of Δ9-THC in spontaneous hypertensive rats (SHRs) (Figure 2). In addition, human studies revealed that inhalation of 2% Δ9-THC marijuana led to a reduction in systolic blood pressure resulting in orthostatic hypotension. 140 Moreover, prolonged (30 days) Δ9-THC ingestion induced a decrease in the heart rate and blood pressure; however, the development of the tolerance to the orthostatic hypotension, probably due to the expansion of plasma volume, was also observed. 141 Despite inconsistent results from studies regarding the action of Δ9-THC on blood pressure, most of the latest studies indicate the elevation in this parameter after exposure to the pCB.92,93 Recent studies also suggest the cardioprotective effect of CBD in hypertension. It was shown that CBD evoked reduction of the increased width of cardiomyocytes of the left ventricle, which was observed in deoxycorticosterone acetate (DOCA)-salt – secondary hypertension model and spontaneously hypertensive rats (SHRs) – primary hypertension model, whereas only in the case of the SHR group, width of the cardiomyocytes of the right ventricle was altered. 142 Interestingly, CBD is also involved in the regulation of vascular tone in the human pulmonary circulation. Relaxation of the pulmonary arteries after administration of CBD was found to be mediated mainly through prostacyclin (IP), E-type prostanoid receptor 4 (EP4), and TRPV1 receptors as well as calcium-activated potassium (KCa) channels. 143 This effect, however, was diminished by comorbidities such as hypertension or obesity. Furthermore, CBD-induced vasorelaxation in a rat model was enhanced in DOCA-salt, but reduced in SHR group. 143 Chronic CBD administration also improved the blood oxygen saturation and leukocyte number as well as the decrease in the right ventricular systolic pressure in rats with monocrotaline-induced pulmonary hypertension (Figure 2). 144 Another study has shown that chronic CBD administration did not modify blood pressure both in DOCA-salt and SHR models of hypertension, although inhibited the FAAH activity in these models. Furthermore, lipid peroxidation level, free fatty acid concentration as well as activity of FAAH were elevated in the normotensive control rats after administration of CBD. 145 Even though CBD exerts many cardioprotective actions, some untoward effects, mainly caused by increased lipid peroxidation, should be taken into consideration in subsequent studies. There are only limited studies describing the effects of other pCBs in described disorders.

Effects of cannabidiol and Δ9-tetrahydrocannabinol on blood vessels.
Atherosclerosis
Atherosclerosis is a chronic inflammatory disease, mediated by pro-inflammatory cytokines, bioactive lipids as well as adhesion molecules. 148 Due to the inflammation, ECS and pCBs are considered to be a potential therapeutic approach to atherosclerosis. The experiment conducted by Steffens and colleagues 146 on the mice model of atherosclerosis demonstrated that low doses of Δ9-THC (1 mg/kg of body weight) suppressed the disease progression. It was shown that Δ9-THC via CB2 receptor located in atherosclerotic plaques inhibited macrophage migration as well as decreased proliferation capacity of lymphoid cells. In addition, in vitro experiment presented that Δ9-THC also suppressed macrophage chemotaxis in response to monocyte chemoattractant protein (MCP)-1, an important step in a disease progression (Figure 2). 146 Another study carried out on a similar mice model provided evidence of the impact of selective CB2 agonist – WIN55212–2 on atherosclerosis progression. Activation of CB2 receptor caused lessened expression of pro-inflammatory genes (TNF-α, IL-6, and MCP-1) as well as lowered NF-κB activation in aortic tissue, whereas the serum lipid level was not affected. 148 CBD is another pCB, which exhibits therapeutic potential in the treatment of atherosclerosis. Cannabidiol together with its methylated forms: 2’-monomethylated CBD (CBDM) and 2’,6’-dimethylated CBD (CBDD) were demonstrated to selectively inhibit 12/15 - lipoxygenase - catalyzed oxygenation (Figure 2). 147 Oxidation of low-density lipoprotein (LDL) is a crucial step in the development of atherosclerosis; thus, agents preventing the generation of oxidized LDL may diminish the progression of the disease. 147 Both above-mentioned pCBs display potential advantageous roles in atherosclerosis, and, what should be underlined, the dose of Δ9-THC used in the experiment is much lower than the dose associated with its psychotropic activity.
Negative aspects of cannabinoids
It should be noted that the cardiovascular effects of cannabinoids are complex and promising outcomes of studies in animal models are not always reflected in human trials. The main reason for that is a number of differences between animal and human trials, including dose size or route of administration, which influences the pharmacokinetics of the cannabinoids. As an example of the above-mentioned differences, in a rat model of chronic temporal lobe epilepsy, the dose of orally applied CBD was 200 mg/kg of body weight. Whereas, in human trials, resulting in a similar outcome – reduction of seizure burden, the dose was 10 times lower.149,150
Moreover, marijuana use in humans is connected with an increased cardiovascular risk and the development of disorders, such as arrhythmia, myocardial infarction, or cardiomyopathy.151,152 Although several reports indicated such association in Cannabis users, the studies are interfered by the fact that hashish is often used with other substances, for instance, tobacco or alcohol, which also impact cardiovascular system performance. Hence, the exact pathomechanism underlying the adverse effects of Cannabis is not clearly understood. 153 Numerous publications indicated that the pathological outcomes of smoking marijuana are the consequence of CB1 receptor activation. Inhibition of this receptor attenuated hypotension and tachycardia observed after Cannabis inhalation.91,154 Moreover, detrimental effects of activation of the CB1 receptor signaling pathway in the cardiovascular system include elevation of ROS generation by macrophages, a decrease in cardiac contractility, induction of inflammatory response in coronary artery endothelial cells as well as promotion of apoptosis in cardiomyocytes and endothelium. It is also suggested that the CB1 receptor mediates the profibrotic effect, which may influence cardiac physiology leading to increased myocardial stiffness, cell death, arrhythmias as well as heart failure.155–157 Another suggested mechanism underlying adverse Cannabis effects includes elevated cardiac oxygen demand resulting from tachycardia. In addition, during smoking marijuana, coronary blood flow and lowered oxygen supply were also observed as a consequence of carboxyhemoglobin formation.158,159
Conclusion
Accumulating evidence supports the crucial role of ECS in a wide range of physiological and pathophysiological conditions. In the cardiovascular system, ECS is involved in the inflammatory process, hemodynamic homeostasis, or cardiac rhythm control. Thus, it is not surprising that in many CVDs, ECS is highly active. Hence, pharmacological manipulation of the ECS, both by endocannabinoids and pCBs, may offer a novel therapeutic approach to cardiac disorders. Among many components of the Cannabis plant, studies on CBD demonstrate the greatest potential in experimental models of described herein CVDs. Although animal models and in vitro experiments have shown promising outcomes, data from human studies are still extremely limited and only these clinical trials may shed light on the actual therapeutic effect of CBD. Even though some effects of Cannabis compounds on the cardiovascular system are widely known, a thorough examination of their mechanism of action would greatly advance the understanding of pCBs. Molecular targets of Δ9-THC, CBG, CBC, CBN as well as THCV indicate their protective impact on the heart and blood vessels; nonetheless, the lack of in vitro, animal, or human studies creates a huge knowledge gap in this field.