
Abstract
Capsule retention is a rare complication to capsule endoscopy. It is often asymptomatic and resolves itself spontaneously. In some cases, endoscopy or surgery is necessary to remove the capsule. Cases of capsule retention in the colon are not reported very often and precautions in subsequent investigations must be considered. We present a case of a 74-year-old woman who underwent colon capsule endoscopy (CCE) due to a positive fecal immunochemical test. The CCE was incomplete, and the patient was referred to conventional colonoscopy, which was complicated by perforation of the large bowel during the procedure. This lead to a CT scan showing the capsule proximal to a stenotic colon segment which was subsequently surgically removed. In patients who report lack of capsule excretion and stenosis is not verified, colonoscopy can be carried out, but with caution.
Background
In capsule endoscopy (CE), very few complications are reported. Capsule retention (CR) is considered the most severe complication and occurs in less than 1% of investigations. 1 CR is defined by the European Society of Gastrointestinal Endoscopy (ESGE) as retention of the capsule for > 15 days or when intervention is required. 2 In most cases, a conservative strategy is used and the capsule will eventually be excreted spontaneously, but if the patient shows symptoms of bowel obstruction, the capsule must be retrieved endoscopically or surgically. 3 Most reported cases show retention in the small bowel, and only few cases of colonic CR have been reported.4,5
We present a case of CR in a patient with an asymptomatic and undiagnosed stenosis in the colon and the subsequent endoscopic and surgical treatment initiated by the incomplete CE.
Case presentation
A 74-year-old woman participated in the Danish screening program for colon cancer. She had a positive fecal immunochemical test (FIT > 100 µg hgb/ml buffer) and was allocated to further investigation by colon capsule endoscopy (CCE). The CCE was incomplete due to lack of capsule excretion and she was referred to a colonoscopy. In the evaluation of the CCE investigation, the capsule was reported to have reached the left colon, although a precise location could not be ascertained. Four days after ingesting the capsule, the patient contacted the department to inform that the capsule had not passed. She reported no symptoms from the gastrointestinal (GI) tract and a watchful waiting strategy was chosen.
Seventeen days after capsule ingestion, the patient was admitted for colonoscopy in general anesthesia. The procedure was planned to complete investigation of the large bowel and was not prompted by CR or GI symptoms. The endoscopy was complicated by an iatrogenic perforation near the rectosigmoid junction, and the procedure was converted to a laparoscopy. The surgeon sutured the perforation without further complications. Four days after surgery, the patient showed signs of bowel obstruction and a computed tomography (CT) was performed showing colon ileus caused by a stenosis at the rectosigmoid junction. Orally to the stenosis, the colon capsule was still present (Figures 1–3).

Initial CT scan showing the retained colon capsule (coronal plane).
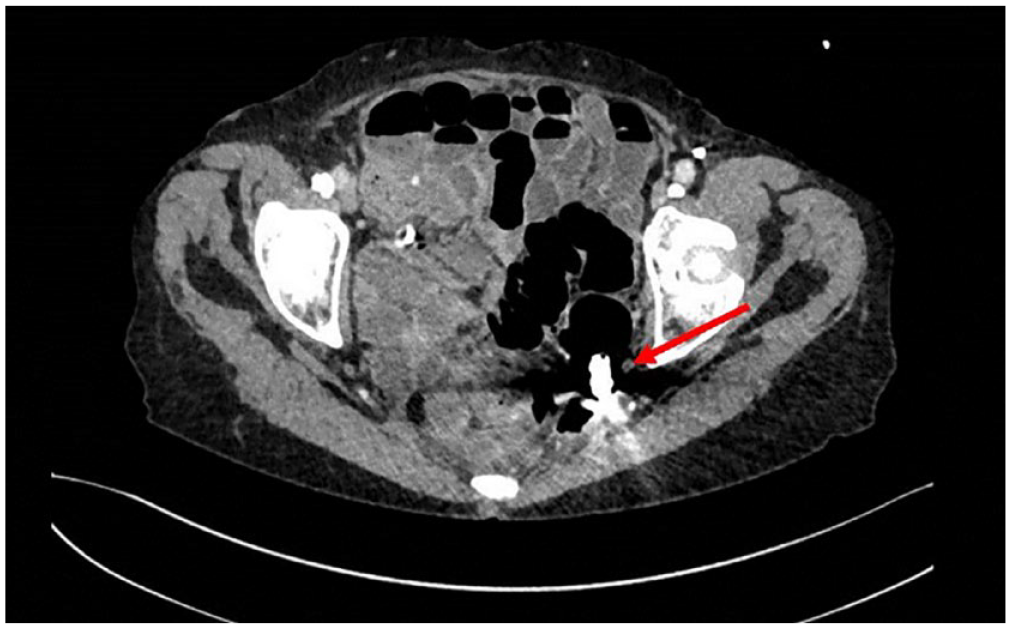
Initial CT scan showing the retained colon capsule (axial plane).

Three-dimensional (3D) reconstruction of the initial CT scan showing the retained capsule in the pelvic region.
The patient was treated conservatively, but did not recover bowel function. Nine days after surgery, a sigmoidoscopy confirmed the presence of a stenosis. A laparoscopic resection of the stenotic colon segment was carried out, and a temporary colostomy was formed. The colon capsule was not found in the resected bowel segment. Pathology showed diverticulosis and acute inflammation in the resected bowel segment. There were no signs of malignancy.
A CT scan later on did not show the colon capsule, which might have passed spontaneously and unnoticed through the colostomy. Two weeks after the initial colonoscopy, a laparotomy was carried out to resolve a mechanical obstruction of the small bowel caused by adhesions. Afterward, the patient slowly recovered bowel function with the use of laxatives.
Discussion
In the clinic, CE is an integral part of investigation of the small bowel and an upcoming modality in investigation of the colon. This imposes the risk of new complications such as CR. There is currently no widely accepted guidelines for the treatment of asymptomatic patients with CR in the colon. ESGE recommend awaiting spontaneous passage, but only discuss retention in the small bowel. 2 When choosing the conservative path, how long should you await spontaneous passage before changing strategy? Cases of long-term CR for up to 12 years have been reported. 6 Some cases of long-term retention are reported without any symptoms, while others report light symptoms such as abdominal pain or severe symptoms of bowel obstruction or perforation.6–8 Only in rare cases capsule disruption is reported.9,10 To avoid these adverse events that can occur months to years after capsule ingestion, Rondonotti 11 suggests capsule retrieval after retention for 3–6 months.
In our case, the patient had no symptoms of bowel obstruction, and the indication for colonoscopy was not to remove a retained capsule, but to complete the investigation of the patients’ large bowel after incomplete CCE. Neither was the retention indication for following surgical procedures. In patients with known or suspected gastrointestinal stenosis, a patency capsule is a safe way to diminish the risk of CR. 12 It is of importance to screen patients before CCE asking for symptoms indicating a bowel stenosis and former abdominal surgery as a guidance for an initial patency capsule examination.
In patients who report lack of capsule excretion, we need to consider the possible explanations for this before proceeding with further examinations. The patient might not have observed the capsule passing, but there is a risk of bowel stenosis in these patients. The last known location of the capsule can aid the endoscopist in predicting the colon segment that might be challenging to pass. Water-assisted colonoscopy has been found to facilitate completion of difficult colonoscopies 13 and could therefore be a wise addition when performing investigations with a high risk of complications.
Conclusion
In patients with CR in the colon, colonoscopy should be carried out with caution to avoid iatrogenic perforation. With increasing use of CCE, it is important that the clinicians are aware of the possible implications when treating patients with colon CR.