
Abstract
Background:
Patients with incidental eosinophilia is becoming increasingly common in clinical practice. But it remains challenging to diagnose and treat owing to its complex etiology. The awareness of physicians and the strategies of diagnosis and treatment toward eosinophilia are still unclear.
Objective:
We aimed to evaluate attention, diagnosis, treatment, and awareness of eosinophilia among physicians, as well as factors influencing clinical practice, and to find ways to improve the efficacy of this disease.
Design:
This is a cross-sectional survey.
Methods:
A cross-sectional study was conducted from 1 to 4 June 2021 in a tertiary hospital. Self-administered and validated electronic questionnaire was used to investigate the attention toward eosinophilia, the strategies of diagnosis and treatment, and the awareness in physicians.
Results:
A total of 607 valid questionnaires were collected, with a response rate of 84.5%. Among the responders, 65.4% of physicians claimed to be familiar with patients with eosinophilia but only 11.0% of them had read the relevant guidelines or expert consensus. Among 207 physicians who had ever diagnosed patients with eosinophilia, only 19.4% had performed detailed examinations. The accuracy of awareness questions was 1.6–53.5%, and only 26.5% of physicians had high levels of awareness. An increase in the awareness level of up to 2.82 folds was seen among physicians with factors such as job title, encountering patients with eosinophilia, linking patients’ conditions to peripheral blood eosinophil count, and paying attention to guidelines.
Conclusion:
This study highlighted the importance of raising awareness and knowledge of eosinophilia among physicians in China. More works on education about eosinophilia guideline are needed, which may help physicians make decision with more benefits to patients.
Introduction
At present, the number of peripheral blood eosinophils being greater than 3–5% is defined as eosinophilia while the corresponding absolute upper limit is 3.5 × 109/l. The severity of eosinophilia is arbitrarily classified as mild (0.5–1.5 × 109/l), moderate (1.5–5 × 109/l), or severe (>5 × 109/l).1–3 Peripheral blood and tissue eosinophilia may develop and lead to organ damage which has usually been diagnosed as hypereosinophilic syndrome (HES). There has been a large report series indicating that the most common causes of secondary eosinophilia were lymphocyte variant of HES subtype (L-HES), immunoglobulin G4-related disease (IgG4-RD) and vasculitides such as eosinophilic granulomatosis with polyangiitis (EGPA). 4
Peripheral blood eosinophilia is becoming increasingly common in clinical practice, and it is associated with many diseases, including allergic diseases, parasitic worm infections, certain dermatologic diseases, hematologic diseases, and malignancies.5–7 Physicians, however, paid little attention to the eosinophil count in blood routine tests.1,8 Martin Peju et al. 9 reported that nearly half of patients with eosinophilia did not have eosinophilia being mentioned in their medical records, but the actual peripheral blood eosinophil counts were high. Physicians have not linked patients’ conditions to the peripheral blood eosinophil count unless there was significant organ dysfunction.
Similar situation could be seen in Mainland China. The Chinese expert consensus on eosinophilia mentioned that further examination and intervention would not be required if mild eosinophilia was not accompanied by other clinical presentations. 3 This statement might not be appropriate, however, as an increasing number of studies have found that the peripheral blood eosinophil count may be a good biomarker that can guide asthma treatment or predict tumor progression.10–12
Although eosinophilia tests, diagnosis, and treatment guidelines or reviews are available in other countries,1,13–15 overseas guidelines may not be suitable for extrapolation in China given the different situations and ethnicity. Furthermore, there are differences in the levels of development between different hospital grades in China. Although some guidelines or consensus are available for reference, we assumed that most physicians remained unclear about the complex diagnosis and treatment of eosinophilia.
Robust data on how physicians actually responded to the demand for clinical services are lacking, however. Previous reports on eosinophilia mainly included the case reports with small sample sizes. Only South Korea 16 and Austria 17 have published studies with larger sample sizes to describe the clinical characteristics of eosinophilia. There is a paucity of epidemiological studies on eosinophilia and physicians worldwide that are considered to have limited awareness.
Because eosinophilia is often overlooked in clinical practice, accurate identification and treatment may have important impact on patient’s outcomes. Moreover, no previous study has examined the attention, diagnosis and treatment situation, and awareness of physicians toward eosinophilia. Therefore, we conducted a questionnaire survey on all physicians in a tertiary hospital in southern China to examine the potential factors affecting the awareness of eosinophilia. We expected that physicians with a higher level of awareness could make the correct diagnosis and treatment decisions. We advocated the popularization and implementation of dialectics for relevant guidelines, emphasize on the importance of early diagnosis and treatment of eosinophilia, and the improvement in clinical practice to provide better diagnosis and treatment services for patients. Future research linking physician’s altitude, awareness, and clinical practice to patient’s outcomes can inform the planning for additional continuing education of this disease or other events in the future.
Materials and methods
Participants
The cross-sectional survey was conducted in a tertiary hospital in southern China. We included all in-service clinical staff in the hospital and excluded pharmacists, nurses, hospital administrator, and hospital researchers. This is an online survey, so we cannot obtain the written informed consent from the participants. We, however, provided the information including the purpose of the study, how the data will be used, stating the data anonymity and voluntary participation during the first survey’s window. Only the potential participant clicks on the ‘next’ button after reviewing the above information, and would be directed to the research survey questionnaire. Therefore, we assumed that the physicians who filled in the questionnaire indicated that they have read the consent information and agreed to participate in the study. In addition, the contents of the first survey window with the protocol were submitted to the Ethics Committee for review (no. 20210040).
Questionnaire
The draft questionnaire written in Chinese was developed by the authors based on the ‘Chinese expert consensus on the diagnosis and treatment of eosinophilia’ 3 and other relevant reviews and guidelines.1,13,18–21 The questionnaire was further revised following discussion with 10 multidisciplinary specialists including respiratory physician, oncologist, digestive physicians, hematologists, cardiologists, and infectiologists.
The questionnaire was divided into 4 parts which contained 37 question items. Ten questions were inquiring the general information of the physician (age, sex, educational level, years of work experience, job title, and department), nine questions were asking about the physician’s attention to eosinophilia (Was attention paid to white blood cell count or eosinophil count? What channels were used to pay attention to this disease? Was attention paid to guidelines or consensus?), nine questions were related to the diagnosis (Had the physician encountered these patients before? What departments will be invited to the consultation meeting if physician encounter such patients? What was examined? How was diagnosis performed? What treatments were given?), and nine questions were associated with the awareness (awareness toward eosinophilia and eosinophilia-related diseases) (Supplemental Appendix 1).
The survey was administered from 1 to 4 June 2021. Responders were invited by telephone to complete the survey online using an electronic survey tool. All mail correspondence was addressed to the hospital departments’ chief physicians.
Attention and clinical practice questions were multiple-choice questions, in which one or more answers could be selected and the awareness question contains multiple-choice questions and single questions. The nine awareness questions were divided into six groups. The causes of eosinophilia and various organ damages were complex, so the sixth group did not contain any clear wrong answer and only the first five groups were scored. For the single-choice questions, a correct answer was given a score of 1 and a wrong one of 0. For multiple-choice questions, only those who chose all correct options would be scored 1 point, otherwise scored zero. The total possible score ranged from 0 to 5. The correct answer rate of the knowledge question was calculated as follows: (the number of responders with correct answers/the total number of responders) × 100%. Awareness was divided into two categories: high awareness, defined as a score ⩾50% of the total score (⩾2.5 points) and low awareness, defined as a score <50% of the total score (<2.5 points).
The survey data were exported from the online platform in Excel format. Repeated data were excluded based on the physicians’ ID numbers. If repeated ID numbers were found, the earliest record submitted was used as the questionnaire information for that subject. Because the questionnaire could only be submitted after all questions were filled in, there would be no missing data. Reliability was evaluated by Cronbach’s alpha coefficient of the questionnaire. Questions about demographics, clinical practice, and questions like ‘How did you learn about eosinophilia’, ‘The year of publication of this consensus?’ and ‘How many patients had you ever encountered?’ were developed to form a pool of supplement and were not included in reliability assessment. The Cronbach’s alpha for the attention and awareness was 0.573 and 0.645, respectively. In addition, we developed the questionnaire according to the guidelines and consulted with specialists to ensure the content validity. To ensure the face validity, we piloted the survey with three investigators and one chief physician majored in respiratory medicine to obtain their feedback about the content, form, and structure.
Statistical analysis
SPSS 26.0 software (SPSS, Chicago, IL, USA) was used for statistical analysis. Continuous variables were expressed as the median and interquartile range, and categorical variables were expressed as the frequency and percentage. The Chi-square test was used to analyze the differences in the diagnosis and treatment between physicians with a different awareness. Unconditional bivariate logistic regression was used to analyze potential factors affecting awareness in physicians. A p value < 0.05 was considered to indicate statistical significance.
Results
Participant’s characteristics
Out of the 718 physicians in the hospital, 607 accepted and completed questionnaires, with a response rate of 84.5%.
The median age was 34 years and more than half were in the 20- to 35-year age range (54.9%). Most participants were males (57.7%), and most had a bachelor’s degree (78.6%). The median number of work experience was 10 years. Nearly half of participants were physicians (42.7%). The departments of participants in descending order were surgery (36.1%), the internal medicine (33.1%), and other departments (30.8%) (Table 1).
Baseline characteristics of respondents (n = 607).

IQR, interquartile range.
Surgery: ENT (ear–nose–throat) department, gynecology, obstetrics, stomatology, ophthalmology department, anesthesiology department, radiology department, orthopedics department, breast surgery, burns surgery, cardiothoracic surgery, anorectal surgery, general surgery, hepatobiliary surgery, neurological surgery, urology surgery, and pediatric surgery.
Internal medicine: dermatology, intensive care unit (ICU), oncology, general practice, traditional Chinese medicine department, infectious diseases department, vasculocardiology department, hematology, endocrinology department, gastroenterology department, geriatrics, rheumatology, nephrology department, pneumology department, respiratory department, pediatric integrative medicine, internal medicine for children, neonatology, and hepatology.
Other departments: medical imaging department, clinical laboratory, function room, pathology department, electrocardiogram room, ultrasonography, emergency, physical examination center, rehabilitation department, child health department, blood transfusion department, out-patient department, and traditional Chinese medicine department.
Attention
Among all responders, 76.6% reported that they will link patients’ conditions to the peripheral blood eosinophil count test; nevertheless, 65.4% felt that they understood eosinophilia (397/607: 48.3% had ‘fair understanding’, 12.9% had ‘good understanding’, and 4.3% had ‘extremely good understanding’). The physicians tended to read professional journals to understand the disease (71.8%, 285/397) (Supplemental Table 1). Overall, only 11.0% (67/607) of physicians paid attention to the ‘Chinese expert consensus on the diagnosis and treatment of eosinophilia’ or referred to the relevant guidelines, yet only 41.8% (28/67) correctly answered the question on the year of publication of this consensus. Furthermore, 89.1% mentioned that they were willing to participate in continuing education courses.
Diagnosis and treatment status
About 34.1% of physicians had previously encountered patients with eosinophilia and 52.2% (108/207) had only encountered one to two patients (Figure 1(a)). Furthermore, among the 207 physicians who had previously diagnosed eosinophilia, only 19.3% performed detailed examinations in all cases with eosinophilia to confirmed their diagnosis (Figure 1(b)) and among the 154 physicians who had scheduled examinations ever, 89.6% prescribed routine biochemistry tests, 85.7% serum immunoglobulin E (IgE) tests, and 81.2% parasitic worm tests, 55.8% of physicians arranged circulatory system tests, and 46.8% ordered coagulation function and D-dimer tests for patients with eosinophilia, while 22.7% of physicians opted for thyroid function tests and 18.2% ordered serum aldosterone-level tests, both of which are unrelated to eosinophilia per se (Figure 1(c)). Meanwhile, to examine eosinophilia in greater depth, physicians who chose the examinations mentioned above also selected bone marrow aspiration and smear and bone marrow biopsy (90.3%), while 39.6% of physicians opted for the platelet-derived growth factor subunit A (PDGFA), janus kinase 2 (JAK2), and other gene mutation tests (Figure 1(d)).

Examinations and treatments performed by physicians. (a) The percentage of physicians who encountered patients with eosinophilia. (b) The percentage of physicians who examined patients with eosinophilia (n = 607). (c) The percentage of physicians who chose the initial examinations (n = 154). (d) The proportion of physicians choosing specialist examinations (n = 154). (e) The treatment would be chosen (n = 607).
If physicians encountered patients with eosinophilia, most would consider consulting with their colleagues (76.3%), asking the patients about the relevant medical history (69.0%), ruling out organ dysfunction (56.5%), and scheduling for targeted examinations (52.6%) (Figure 2(a)) and most physicians would choose the hematology department (76.9%) or rheumatology department (54.6%) for a consultation meeting, while a few would select the respiratory medicine (16.6%), gastroenterology (7.6%), and cardiology (7.6%) departments for a consultation meeting (Figure 2(b)). Only half of the 419 physicians who stated that they would perform detailed history taking would focus on the medical history and symptoms of the cardiovascular system (50.4%) and digestive system (49.2%) (Figure 2(c)).

Management of eosinophilia cases. (a) The percentage of answers on various diagnostic and therapeutic methods (n = 607). (b) Consultation department selected by physicians (n = 463). (c) Medical history was asked by physicians (n = 419).
Routine biochemistry tests, serum IgE tests, parasite tests, circulatory system tests, autoimmunity antibodies, coagulation function and D-dimer tests, abdominal ultrasound, and serology and stool examination for bacteria, virus, and other pathogen were recommended by the Chinese expert consensus (Xiao 2017).3 A total of 27.9% (43/154) of physicians accurately chose all the above requested test items. After ordering these examinations, 4.5% (7 of 154) of physicians did not further order special tests (bone marrow aspiration and smear and bone marrow biopsy; PDGFA, JAK2, and other gene mutation tests; biopsy of the affected tissues; flow cytometry; serum vitamin B12, serum tryptase; examinations targeting the involved organs) and 95.5% chose one or more special tests (one to six tests: 14.2%, 15.5%, 22.7%, 14.9%, 9%, and 18.8%, respectively) (Supplemental Figure 1).
Although 53.5% of physicians understood that moderate and severe eosinophilia could result in major organ dysfunction, those who knew that eosinophilia might lead to heart failure would seldom decide to have a consultation meeting with the cardiology department (12.6%, 31/246). Moreover, physicians who knew that eosinophilia might lead to respiratory failure would seldom decide to have a consultation meeting with the respiratory medicine department (29.5%, 57/193) (Supplemental Table 2 and Supplemental Figure 1).
More physicians would select the treatment of the primary disease (57.0%) or watchful waiting (45.6%), while few physicians would select glucocorticoids (19.9%), tyrosine kinase inhibitors (10.0%), and monoclonal antibody (14.3%). On the contrary, 41.0% of physicians did not know how to treat patients with eosinophilia. Among physicians who would select tyrosine kinase inhibitors and monoclonal antibody drugs, only 20.4% (11/54) and 30.4% (24/79), respectively, would choose the correct drugs.
Awareness
The rate of the awareness questions was 1.6–53.5% and 26.5% of physicians who had high levels of awareness. Only 33.4% and 45.3%, respectively, were aware of the characterization of marked eosinophilia and hypereosinophilia, but only 17.6% could determine the severity of eosinophilia. Furthermore, only 1.6% of physicians were aware of the categories of hypereosinophilia (familial, secondary, clonal, and idiopathic). Although 53.5% of physicians knew that moderate and severe eosinophilia could cause fatal organ and systemic dysfunction, only 18.5% knew the comprehensive types of organs being involved (Figure 3). Very few physicians knew that respiratory diseases (39.2%), lymphoma (29.3%), digestive tract diseases (28.7%), vasculitis (28.5%), and solid tumors (28.0%) could cause eosinophilia (Figure 4 and Supplemental Table 3).

Awareness of physicians. (a) In the bar chart, blue shows the percentage of physicians who answered correctly, and red shows the percentage of physicians who answered incorrectly (n = 607). (b) The pie chart shows the physicians’ responses to organ damage caused by eosinophilia, with red indicating the percentage of physicians who answered correctly in all cases (n = 325).

Pareto chart of eosinophilia relevant disease.
Factors affecting awareness in physicians
Physicians with a high level of awareness included those who were assistant director physicians [adjusted odds ratio (aOR) = 1.90, 95% confidence interval (CI) = 1.14–3.16], had previously encountered such patients (aOR = 2.71, 95% CI = 1.55–4.73), had linked patients’ conditions to the peripheral blood eosinophil count (aOR = 2.82, 95% CI = 1.46~5.46), and had read or applied the eosinophilia guidelines (aOR = 2.36, 95% CI = 1.33~4.19) (Figure 5 and Supplemental Table 4).
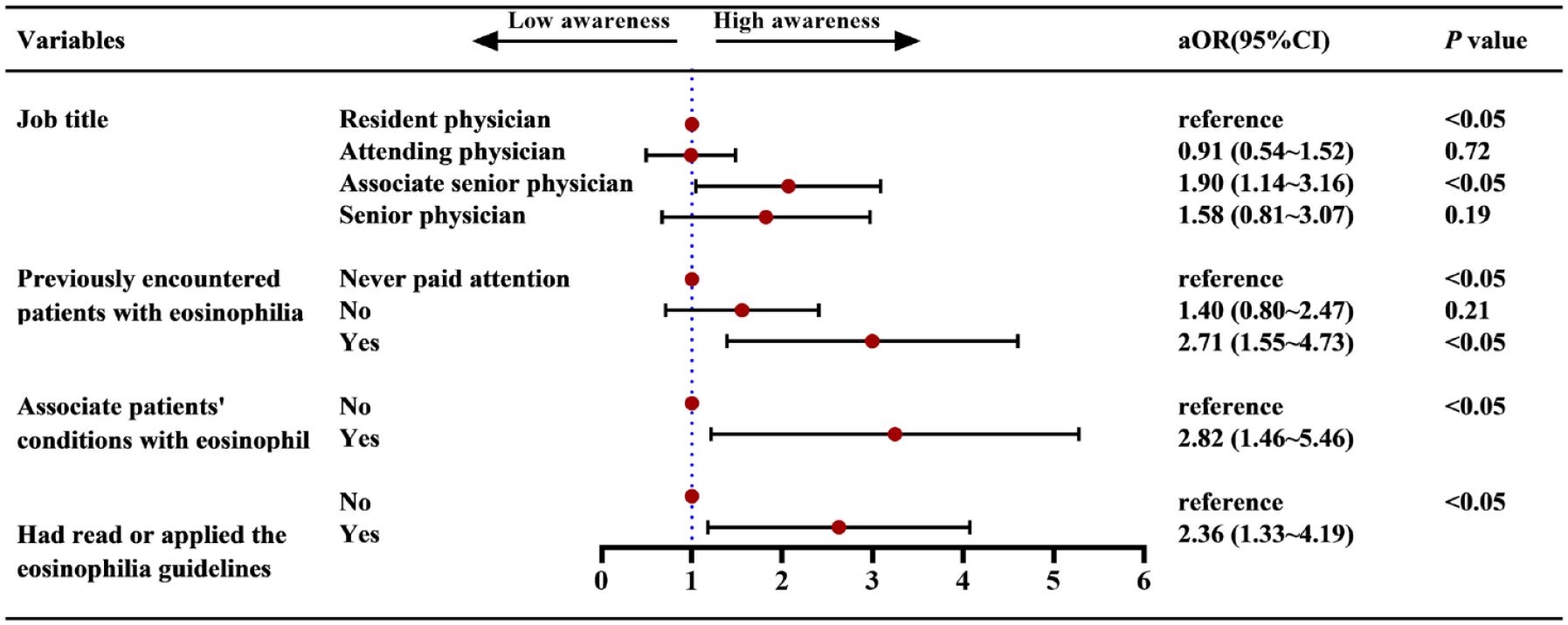
The odds ratio and the 95% confidence interval for the variables associated with awareness toward eosinophilia.
Comparison of the diagnosis and treatment between physicians with different awareness
Physicians with a high level of awareness of eosinophilia tended to order detailed examinations for all patients (10.6% versus 5.2%, p < 0.05), paid more attention to the white blood cell count (100.0% versus 97.1%, p < 0.05) and eosinophil count (92.5% versus 70.9%, p < 0.05), and they perform detail history taking (82.6% versus 64.1%, p < 0.05), arranged for targeted examinations (73.3% versus 45.1%, p < 0.05), ruled out life-threatening organ dysfunction caused by eosinophilia (77.6% versus 48.9%, p < 0.05), and could make an accurate diagnosis and treatment plan. Most physicians with a low level of awareness did not know how to prescribe for the treatment (50.7% versus 14.3%, p < 0.05) (Figure 6 and Supplemental Table 5).

Comparison of treatment measures between physicians with high awareness and those with low awareness.
Discussion
To our knowledge, this is the first cross-sectional survey on eosinophilia attention, diagnosis, treatment, and awareness among physicians.20,22–24 From the questionnaire survey conducted in Yangjiang People’s Hospital, we found that physicians self-reported a high level of attention toward eosinophilia but that their actual understanding of eosinophilia was lacking in each content domain. Therefore, the corresponding diagnosis and treatment practices were both unclear and insufficient. Job title, consultation experience, and attention might have affected the awareness among clinicians. Clinicians’ awareness could significantly affect their clinical practice.
Although Chinese and international studies have mentioned the low level of attention to guidelines and the differences between guidelines and actual clinical practice,25–27 physicians seemed to have a lower level of attention toward eosinophilia, which might lead to the insufficient diagnosis and treatment. To standardize eosinophilia diagnosis and treatment behavior in China, the Leukemia and Lymphoma Group of the Chinese Society of Hematology solicited expert opinions and referred to the relevant overseas literature reports and guidelines (published in English language) to develop an expert consensus suitable for clinical practice in China. Our survey, however, showed that only 11.0% of physicians paid attention to the ‘Chinese expert consensus on the diagnosis and treatment of eosinophilia’ and the relevant guidelines. In addition, we assumed that physicians who answered the year of publication would have already reviewed the consensus. Most physicians, however, selected the wrong answer, suggesting that they had limited attention toward this disease. The low level of attention was consistent with the results of a recent questionnaire study on eosinophilic esophagitis guidelines and practice. 27
Many physicians were unable to give a correct diagnosis and treatment when encountering patients with eosinophilia. In the analysis of this questionnaire, one-third of physicians encountered patients with eosinophilia, and three-fourths of physicians claimed to have paid attention to eosinophil count in a routine blood test. For example, when encountering patients with eosinophilia, the percentage of physicians who would enquire about the patients’ medical history and symptoms of the cardiovascular system and digestive system diseases was low. This showed that physicians lacked sufficient awareness of eosinophilia associated with the circulatory system and digestive system. In clinical practice, eosinophilia often involved the heart, and eosinophilic esophagitis and gastroenteritis were common.28,29 This might help interpret the likelihood of physicians who had overlooked the eosinophilia caused by the aforementioned diseases, resulting in missed diagnosis and misdiagnosis.
This study found that the awareness of the relevant diseases of eosinophilia might be limited. Furthermore, diagnosis of the etiology of eosinophilia in clinical practice might be insufficient. Most physicians were not aware that vasculitis, solid tumors, lymphoma, and rheumatic disorders would be associated with eosinophilia, and 1.4% mentioned that they did not understand which diseases were relevant to eosinophilia. For these reasons, clinicians were unable to link these diseases to eosinophilia, so the delays in diagnosis and treatment were not uncommon.
As an important and emerging cause, IgG4-RD can lead to end-stage organ failure and even death if unrecognized, but has rarely been examined in many centers.30,31 A recent study found a positive association between peripheral eosinophil count and serum IgG4 levels, the duration of disease, the number of organs involved, and prognosis in IgG4-RD. 32 When IgG4-RD was suspected, serum protein electrophoresis (SPEP) and IgG subclasses measurement would be helpful as the initial tests. 33 Moreover, secondary causes of HES such as EGPA and L-HES would be difficult to recognize. A firm diagnosis of EGPA, the most common cause of eosinophilic vasculitis, often required a close follow-up of the patients over time, because overt vasculitis might not occur until after a long, latent, and profound phase of peripheral eosinophilia. Confirming L-HES required a combination of bone marrow biopsy, cytogenetics, flow cytometry, and T-cell clonality measurements. 34 Only one in five physicians opted for bone marrow aspiration smear and bone marrow biopsy. Only one-tenth of physicians chose flow cytometry. Even less physicians were aware of some specialist’s examinations. The conscious of genetic tests also might be insufficient. In 2008, the World Health Organization defined a subtype of ‘Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA (Platelet Derived Growth Factor Receptor Alpha), PDGFRB (platelet-derived growth factor receptor beta), or FGFR1 (fibroblast growth factor receptor 1), or with PCM1-JAK2 (PCM 1: Pericentriolar material 1)’ of which the most common fusion gene was FIP1L1-PDGFRA. These patients did not show a significant response to glucocorticoids but responded very well to imatinib. 1 JAK2V617F mutations were identified in 4% of hypereosinophilia among some patients in the German Registry. 35 Survival of patients with hypereosinophilia whose JAK2V617F mutation was poorer compared with those with FIP1L1-PDGFRA mutation. Given that the V617F mutation in JAK2 is an oncogenic driver in several myeloproliferative neoplasms (MPNs), including essential thrombocythemia, myelofibrosis, and polycythemia vera (PV), 36 there are necessary and urgent indications for testing in these patients. Interestingly, chronic eosinophilic leukemia has been shown to be associated with PCM1-JAK2 fusion gene mutation. 1 After excluding secondary eosinophilia, however, only one-fifth of clinicians stated that they would select PDGFRA and JAK2 gene mutation tests and only 9.7% of clinicians knew of tyrosine kinase inhibitors. Out of these physicians, only 30.4% could select the correct drug, imatinib, which may result in poor prognosis in these patients.
Although eosinophil counts and eosinophil-mediated tissue damage may not be completely related, it was generally believed that a peripheral blood absolute eosinophil count >1.5 × 109/l would be related to tissue eosinophil infiltration. Regardless of the reasons, this might result in irreversible and life-threatening organ damage. 37 Eosinophils often infiltrate the skin, lungs, kidneys, gastrointestinal tract, heart, and nervous system. Differences in organ infiltration sites may lead to different clinical complications; the most serious of which might include thrombosis, myocardial injury, respiratory failure, and nervous system involvement. 37 On the contrary, 314 (48.4%) physicians did not know that organ infiltration by eosinophils may cause organ dysfunction. Moreover, nearly half of the physicians said that they would not order the ‘coagulation function and D-dimer’ tests when they encountered patients with eosinophilia. This showed that they lack sufficient understanding that hypereosinophilic disorders might also cause thrombosis. Only 55.8% (86/154) of physicians stated that they would select for the circulatory system examinations. Many guidelines and consensus, however, stated that cardiac involvement should first be ruled out in hypereosinophilic disorders. With regard to the further examinations for organ involvement, only 68.8% (105/154) of physicians selected tissue biopsy and examinations targeting the eosinophil-induced organ damage. Although a multidisciplinary team (MDT) has been promoted and practiced in many medical fields, and Samuel Ndoro 38 also emphasized the importance of an MDT in providing high-quality diagnosis and treatment, many physicians still tended to choose hematology for a consultation meeting when they encounter the patients with eosinophilia. By contrast, few physicians would select the respiratory medicine, gastroenterology, and cardiology departments for a consultation meeting. Physicians might not have accurately identified whether organ dysfunction would have occurred in the patients with eosinophilia and conducted any intervention before irreversible terminal organ damage or complications have occurred.
Furthermore, 41.0% of physicians mentioned that they did not know how to treat patients with eosinophilia, which would increase the risk of organ damage. With regard to physicians who mentioned that they knew how to treat eosinophilia, most would select to treat the primary disease or conduct watchful waiting, while very few would select glucocorticoids, tyrosine kinase inhibitors, and monoclonal antibodies. Even though physicians knew that tyrosine kinase inhibitors and monoclonal antibodies can be used to treat eosinophilia, an extremely low proportion of physicians selected the correct therapeutic drug such as imatinib, mepolizumab, reslizumab, or benralizumab.
The awareness toward eosinophilia was generally inadequate among clinicians. Although many high-quality reviews and guidelines have been published overseas, the recommended classification and diagnosis procedures for patients with eosinophilia were not identical, which might result in an impaired awareness among physicians. Although 75.3% of physicians mentioned that they had paid attention to the eosinophil count, only 33.4% knew of the definition of eosinophilia. This showed that their attention was superficial, which might affect the correct diagnosis and treatment. There was also a gap in the awareness related to eosinophilic disorders. Job title, consultation experience and attention strongly influenced the awareness, which was consistent with the results of studies in other countries.39–45 We also found that physicians who have reviewed the consensus had a higher level of awareness of the eosinophilic disorders. Our findings indicated that reviewing the consensus was effective in improving the awareness of the physicians. Most physicians mentioned that they were willing to participate in the continuing education courses, and many studies found that training was associated with improved awareness,7,46 demonstrating a need to increase the physician-oriented education programmers, professional training, and medical education for physicians.
This study reported the electronic questionnaire results on eosinophilia, described physicians’ attention, diagnosis and treatment practices, and awareness toward this disease, and examined the potential factors affecting the awareness. The response rate was higher than previous hardcopy questionnaires, which helped to reduce selection bias. 45 There were some limitations of the study design, however. First, the questionnaire results were self-reported by the physicians, and there might still be recall bias. Second, we only surveyed the physicians from a tertiary hospital, and primary hospital physicians might also tend to have overlooked eosinophilia. We planned to survey more centers in the future so that the study results would be more reliable. Third, the questions such as demographics and clinical practice were a nonscoring scale, and the reliability and validity may not be applicable to further calculation. We, however, performed stringent quality control on the questionnaire to ensure that the questionnaire structure and content were rigorous and reliable. Fourth, this study did not provide the sample size calculation, although we have included all the physicians who met the inclusion criteria.
Conclusion
This study shows that clinicians have low eosinophilia awareness, and remain unclear about the diagnosis and treatment practices. There are still gaps in clinical practice and guideline recommendations. It is necessary to improve clinicians’ awareness by organizing continuing education courses, updating guidelines, and publishing high-quality academic papers.
Supplemental Material
sj-doc-2-taj-10.1177_20406223221146938 – Supplemental material for Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey
Supplemental material, sj-doc-2-taj-10.1177_20406223221146938 for Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey by Bigui Chen, Yu Fu, Zhufeng Wang, Qiuping Rong, Qingling Zhang, Jiaxing Xie, Xuetao Kong and Mei Jiang in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-doc-4-taj-10.1177_20406223221146938 – Supplemental material for Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey
Supplemental material, sj-doc-4-taj-10.1177_20406223221146938 for Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey by Bigui Chen, Yu Fu, Zhufeng Wang, Qiuping Rong, Qingling Zhang, Jiaxing Xie, Xuetao Kong and Mei Jiang in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-doc-5-taj-10.1177_20406223221146938 – Supplemental material for Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey
Supplemental material, sj-doc-5-taj-10.1177_20406223221146938 for Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey by Bigui Chen, Yu Fu, Zhufeng Wang, Qiuping Rong, Qingling Zhang, Jiaxing Xie, Xuetao Kong and Mei Jiang in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-doc-6-taj-10.1177_20406223221146938 – Supplemental material for Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey
Supplemental material, sj-doc-6-taj-10.1177_20406223221146938 for Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey by Bigui Chen, Yu Fu, Zhufeng Wang, Qiuping Rong, Qingling Zhang, Jiaxing Xie, Xuetao Kong and Mei Jiang in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-doc-7-taj-10.1177_20406223221146938 – Supplemental material for Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey
Supplemental material, sj-doc-7-taj-10.1177_20406223221146938 for Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey by Bigui Chen, Yu Fu, Zhufeng Wang, Qiuping Rong, Qingling Zhang, Jiaxing Xie, Xuetao Kong and Mei Jiang in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-3-taj-10.1177_20406223221146938 – Supplemental material for Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey
Supplemental material, sj-docx-3-taj-10.1177_20406223221146938 for Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey by Bigui Chen, Yu Fu, Zhufeng Wang, Qiuping Rong, Qingling Zhang, Jiaxing Xie, Xuetao Kong and Mei Jiang in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-tif-1-taj-10.1177_20406223221146938 – Supplemental material for Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey
Supplemental material, sj-tif-1-taj-10.1177_20406223221146938 for Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey by Bigui Chen, Yu Fu, Zhufeng Wang, Qiuping Rong, Qingling Zhang, Jiaxing Xie, Xuetao Kong and Mei Jiang in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
The authors express their sincere appreciation and gratitude to the staff members of Yangjiang People’s Hospital for their great assistance in field surveying in this study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.