
Abstract
Background:
Despite the importance of influenza vaccination, its rates in subjects with asthma are suboptimal, especially in the young population.
Methods:
Among 72,843 adults aged ⩾18 years from the Korea National Health and Nutrition Examination Survey conducted between 2010 and 2019, 1643 with asthma were included. The yearly trends and factors associated with influenza vaccination were analyzed in subjects with asthma. In addition, stratified analyses were performed by age group (<65 versus ⩾65 years).
Results:
During the study period, the overall influenza vaccination rate among subjects with asthma fluctuated from 51.0% to 64.3%, with a consistently higher vaccination rate in elderly subjects than in young subjects. Among young subjects with asthma, factors positively associated with influenza vaccination were female sex [adjusted odds ratio (aOR) = 1.66, 95% confidence interval (CI) = 1.11–2.49], current asthma being treated (aOR = 1.69, 95% CI = 1.14–2.50), history of pulmonary tuberculosis (aOR = 2.01, 95% CI = 1.04–3.87), and dyslipidemia (aOR = 1.86, 95% CI = 1.05–3.30). However, unmarried subjects showed an inverse relationship (aOR = 0.50, 95% CI = 0.34–0.75). In elderly subjects, unmarried status (aOR = 0.52, 95% CI = 0.29–0.94), being underweight (aOR = 0.29, 95% CI = 0.09–0.97), and having a low income (aOR = 0.42, 95% CI = 0.18–0.97) were factors negatively associated with influenza vaccination.
Conclusion:
In the last 10 years, influenza vaccination rates have still been insufficient in subjects with asthma, particularly in young subjects. Considering the factors that are influencing the vaccination rates of young subjects, public policies to increase influenza vaccination rates in subjects with asthma need to be established urgently.
Introduction
Asthma is a common inflammatory disorder of the airways characterized by airway hyperresponsiveness. 1 Acute exacerbation of asthma is an important factor associated with increased health care needs, including emergency department visits and hospital admissions.2,3 As a virulent respiratory virus, influenza is one of the common triggers for acute exacerbation of asthma. 4 Subjects with asthma are more susceptible to influenza infection due to impaired antiviral immunity.5,6 Consequently, asthmatics are at increased risk of acute exacerbation, often leading to hospitalization, attributable to influenza infection.7,8
Although there are antiviral treatments for influenza infection, vaccination is the most effective strategy for coping with influenza. 9 The effectiveness of vaccination has been demonstrated in subjects with asthma, which prevented nearly half of influenza infections and approximately 60–80% of asthma attacks.10,11 Accordingly, guidelines have recommended that subjects with asthma should be vaccinated against the influenza virus every year.12–14 However, the previous literature has consistently reported a suboptimal rate of influenza vaccination in this population.15–19 A study using Korean national data reported that the influenza vaccination rate for the general population more than 40 years of age was 45.2%, while it was 76.8% for those aged 65 years and older. 20 In patients with asthma, the influenza vaccination rate for those aged 65 years and older was higher at 81.5%, but the vaccination rate below 50 years of age was only 28.3%. 18 In addition, several factors have been suggested to be associated with low influenza vaccination rates, with young age contributing as a significant factor.16–18,21 Consequently, various methods, such as social marketing, were proposed to increase influenza vaccination rates in young subjects. 22
However, despite these efforts, there are no recent data on whether influenza vaccination rates have increased in subjects with asthma and whether younger age is no longer associated with the low influenza vaccination rates. Therefore, we aimed to investigate the recent yearly trends of influenza vaccination rates and the factors associated with influenza vaccination in subjects with asthma, with a focus on age.
Materials and methods
Study population and design
The Korea National Health and Nutrition Examination Survey (KNHANES) is a population-based nationwide survey that assesses the health and nutritional status of the non-institutionalized Korean population. The survey was conducted by the Korea Disease Control and Prevention Agency (KDCA). The study population was selected using a stratified multistage probability cluster sampling method. More detailed information on the KNHANES has been provided in a previous study. 23
We used data from the KNHANES V (2010–2012), VI (2014–2015), VII (2016–2018), and VIII (2019). In this study, data from the KNHANES 2013 were not included because the influenza vaccination data were not available to the public. A total of 93,338 subjects were included in the surveys over 9 years, and 72,843 agreed to participate (participation rate, 78.0%). Of the 72,843 participants, we excluded subjects aged <18 years (n = 14,659) or those who had missing data for influenza vaccination (n = 6,004). Of the remaining 52,180 subjects, we excluded 50,537 who did not have a history of physician-diagnosed asthma. Finally, 1,643 subjects with asthma were included in the analysis (Figure 1).

Flow chart of the study population.
Outcomes
The outcomes were as follows: (1) influenza vaccination rate over the study period and (2) factors associated with influenza vaccination in subjects with asthma. Subject’s history of influenza vaccination was investigated using the following question: ‘Have you ever been vaccinated against influenza in the past year?’
Exposure
Subjects with asthma were defined as those with a history of physician-diagnosed asthma. Physician-diagnosed asthma was assessed by the question, ‘Have you ever been diagnosed with asthma by a doctor?’ For stratified analyses, subjects with asthma were further subdivided into (1) young subjects (age < 65 years) and (2) elderly subjects (age ⩾ 65 years).
Measurements and other definitions
Body mass index (BMI) was calculated by dividing an individual’s weight by the square of their height (kg/m2). Past smoking was defined as a person who smoked five or more cigarettes in their lifetime but who does not currently smoke. Single, separated, divorced, and widowed individuals were defined as unmarried. Monthly household income was defined as low for the lowest quartile, intermediate for the second to third quartiles, and high for the highest quartile. Regular walking was defined as walking at least five times a week for more than 30 min at a time. Chronic cough was defined as a cough symptom lasting 3 months or longer. Chronic sputum was defined as sputum accompanied by coughing for more than 3 months per year. Physical limitation was defined using the question, ‘Do you have limitations in your daily life?’ Hypertension was defined as a systolic blood pressure ⩾140 mmHg, diastolic blood pressure ⩾90 mmHg, or treatment with antihypertensive medication. Dyslipidemia was defined as low-density lipoprotein cholesterol level greater than 130 mg/dl, high-density lipoprotein cholesterol level less than 40 mg/dl, or treatment with lipid-lowering medications. Diabetes mellitus was defined as a fasting plasma glucose level of ⩾126 mg/dl or treatment with glucose-lowering medications. Other comorbidities were defined on the basis of a physician’s diagnosis. 24
Statistical analysis
Data are expressed as weighted percentages with standard errors. The p values for differences according to influenza vaccination history were calculated using Pearson’s chi-square test. Logistic regression analysis was performed to explore factors associated with influenza vaccination in subjects with asthma. In multivariable analysis, demographic profiles (age, sex, and BMI), personal habits (smoking status and regular walking), socioeconomic factors (marital status, income, and education), symptoms (any respiratory symptoms and physical limitation), asthma status (no asthma at present, not being treated for asthma, and currently being treated for asthma), and comorbidities were included. Income is included in the adjustment because subjects with asthma have to pay for influenza vaccination, whereas it is free for the elderly (⩾65 years) in Korea.
The sampling weights were adjusted for all analyses using the ‘survey’ package of R. Participants in the single primary survey unit stratum were centered at the sampled grand mean. Missing values were handled using the missing indicator method, which analyzes missing values by grouping them into missing categories. Statistical significance was defined as a two-sided p value of less than 0.05. All analyses were performed using R version 4.0.3 (R Core Team 2021; R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline characteristics
The baseline characteristics of the subjects with asthma are shown in Table 1. Among subjects with asthma, compared with unvaccinated subjects, those vaccinated against influenza were more likely to be older (58.1% versus 11.5%, p < 0.001) and female (67.5% versus 55.5%, p < 0.001). Vaccinated subjects were less likely to be current smokers (11.4% versus 24.2%, p < 0.001), unmarried (35.5% versus 48.6%, p < 0.001), college graduates (16.3% versus 34.4%, p < 0.001), and regular walker (33.7% versus 41.0%, p = 0.014), but had more respiratory symptoms (18.8% versus 9.6%, p < 0.001) and physical limitations (25.7% versus 12.9%, p < 0.001) and were more likely being treated for asthma (45.7% versus 21.5%, p < 0.001). However, there were no differences in BMI and income between the two groups.
Baseline characteristics of the study population.

Data are expressed as weighted percentages (standard errors).
Regarding comorbidities, compared to unvaccinated subjects, vaccinated subjects had more history of pulmonary tuberculosis (12.3% versus 4.6%, p < 0.001), hypertension (51.7% versus 22.6%, p < 0.001), diabetes mellitus (18.0% versus 8.5%, p < 0.001), dyslipidemia (40.4% versus 26.3%, p < 0.001), and cardiovascular disease (7.0% versus 3.3%, p = 0.002), but less atopic dermatitis (4.9% versus 13.3%, p < 0.001) and allergic rhinitis (14.7% versus 26.0%, p < 0.001).
Influenza vaccination rates and yearly trends
The overall influenza vaccination rates were 57.2% for all subjects with asthma, 38.7% for young subjects with asthma, and 87.1% for elderly subjects with asthma. The annual trends in influenza vaccination are shown in Figure 2. More than 10 years, the vaccination rate fluctuated in subjects with asthma, ranging from 51.0% to 64.3%. In younger subjects with asthma, the vaccination rate increased from 36.3% in 2010 to 46.6% in 2014 and then sharply decreased in 2015. This dropped vaccination rate was maintained until 2017 and started to increase in 2018. In elderly subjects with asthma, small fluctuations in vaccination rates were observed between 2010 and 2012, ranging from 80.0% to 88.1%. Thereafter, the vaccination rate increased steadily from 86.8% in 2014 and peaked in 2019 (92.6%).
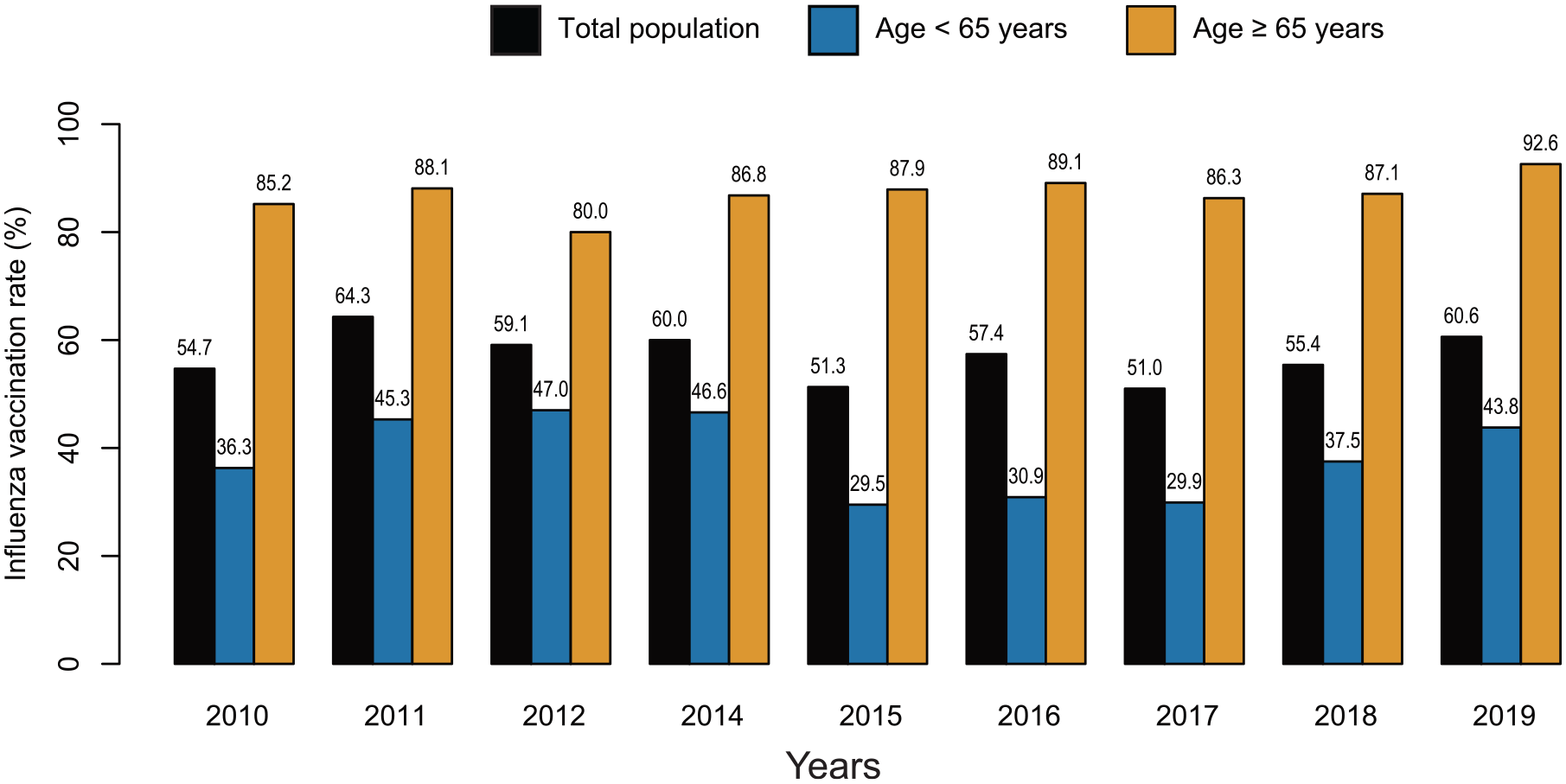
Influenza vaccination trends in subjects with asthma between 2010 and 2019.
Factors associated with influenza vaccination
Supplemental Table S1 and Table 2 show univariable and multivariable logistic regression analyses of influenza vaccination in the subjects with asthma, resprectively. In multivariable analysis, age was the factor most strongly associated with influenza vaccination [adjusted odds ratio (aOR) = 6.49, 95% CI (confidence interval) = 4.35–9.67 for ⩾65 years]. Other identified factors showing an association with influenza vaccination were female sex (aOR = 1.72, 95% CI = 1.21–2.44), unmarried state (aOR = 0.51, 95% CI = 0.37–0.71), current asthma being treated (aOR = 1.82, 95% CI = 1.32–2.51), hypertension (aOR = 1.47, 95% CI = 1.07–2.01), and dyslipidemia (aOR = 1.75, 95% CI = 1.07–2.85).
Factors associated with influenza vaccination in subjects with asthma.

OR, odds ratio; CI, confidence interval.
Bold font indicates statistical significance.
In the stratified analysis, young subjects with asthma, who are female (aOR = 1.66, 95% CI = 1.11–2.49), receiving current asthma treatment (aOR = 1.69, 95% CI = 1.14–2.50), and with a history of pulmonary tuberculosis (aOR = 2.01, 95% CI = 1.04–3.87) or dyslipidemia (aOR = 1.86, 95% CI = 1.05–3.30) were positively associated with influenza vaccination, whereas those with an unmarried status were negatively associated (aOR = 0.50, 95% CI = 0.34–0.75). Among elderly subjects with asthma, those who were underweight (aOR = 0.29, 95% CI = 0.09–0.97), unmarried (aOR = 0.52, 95% CI = 0.29–0.94), and had a low income (aOR = 0.42, 95% CI = 0.18–0.97) were less likely to be vaccinated against influenza.
Discussion
This study comprehensively investigated trends of and factors associated with influenza vaccination rate in subjects with asthma using recent nationwide population-based data of Korea. In the analysis of the trend between 2010 and 2019, the influenza vaccination rate among subjects with asthma has fluctuated at a suboptimal level without a significant increase. In addition, our results showed that lower influenza vaccination rate in subjects with asthma is mostly attributable to young subjects and revealed several important factors associated with vaccination uptake.
Previous studies from western countries have shown the low influenza vaccination rate in subjects with asthma. According to the 2007 Behavioral Risk Factor Surveillance System in the United States, influenza vaccination coverage was 39.9% for adult asthmatics (⩾16 years of age). 15 Influenza vaccination rates in European countries (⩾16 years of age) were 38.0% in the Spanish National Health Study 2006 17 and 35.2% in the European Health Survey 2009, 16 which is comparable to that in the United States. In Korea, the influenza vaccination rate was 61.1% for adults with asthma from 2010 Korean Community Health Survey (⩾19 years of age). 18 However, in another recent Korean study using 2017 Korea Youth Risk Behavior Web-Based Survey, the influenza vaccination rate was 41.8% in Korean adolescents (13–18 years of age) with asthma. 19
After the 2009 influenza pandemic, only a few studies have investigated the influenza vaccination rates in subjects with asthma,18,19 and studies that have evaluated the long-term trend of influenza vaccination are even scarcer. Previously, World Health Assembly recommended increasing influenza vaccination coverage up to at least 75% in subjects with underlying diseases. Surprisingly, contrary to expectations, the influenza vaccination rate in subjects with asthma remains suboptimal and has not increased over the last decade. This suggests that despite national and international asthma guidelines emphasizing the importance of influenza vaccination for asthmatics,12,13 the current vaccination strategies are insufficient to encourage them to be vaccinated. Moreover, given that coinfection with SARS-CoV-2 and influenza virus was associated with a higher risk of poor outcomes,26,27 it would be important to re-evaluate whether influenza vaccination for asthma is adequately implemented in each country.
Many factors are associated with influenza vaccination rates in subjects with asthma, and a well-known factor is age.16–18,21,28 In a pooled analysis of a national population-based survey of Canada, Guthrie et al. 29 reported the rate of ‘feeling that influenza vaccine was unnecessary’ was 1.6-fold higher in adult asthmatics aged 18–24 years than those aged 55–64 years. Our study showed that only 38% of young subjects with asthma were vaccinated, whereas almost 90% of elderly subjects with asthma were vaccinated. First, this large difference may be explained by public policies. The Korean government expanded the coverage for free influenza vaccination from 2005 to include elderly subjects (aged ⩾ 65 years), 30 which might have contributed to the results of our study. Second, it is known that many young adults are hesitant to be vaccinated against various diseases, including influenza. 31 The suggested reasons are unawareness of vaccination recommendations, mistrust of vaccination effects, and confidence in their health.17,28 Whether influenza infection in young subjects with asthma who had infrequent asthma symptoms is associated with severe outcomes remains unclear. However, it is well known that subjects with mild asthma are still at risk of severe asthma exacerbation, 32 and exposure to viruses that might trigger this is unpredictable. Thus, clinicians should evaluate the influenza vaccination status of young subjects with asthma and make greater efforts to vaccinate them against influenza.
In line with the previous studies in asthmatics,15,18,33 we found increased adherence to influenza vaccination in women and in subjects who were married. In addition, subjects who received asthma treatment and had a history of pulmonary tuberculosis and dyslipidemia were more likely to be vaccinated against influenza. It seems natural that subjects who have been treated in the past or are currently receiving treatment for respiratory diseases, such as asthma and pulmonary tuberculosis, are more prone to influenza vaccination. 16 Subjects with chronic diseases, such as diabetes and dyslipidemia, might have higher chances to interact with health care providers than those without chronic diseases. Moreover, physicians will probably pay more attention to influenza prevention in their patients. This is because patients with chronic diseases may be at a higher risk of serious influenza-related outcomes if they also have asthma. 34 These circumstances may lead to increased vaccination uptake. However, the exact social or biological mechanism of these factors leading to influenza vaccination remains an issue warranting future studies.
Moreover, being underweight, being unmarried, and having a low income were found to be related to decreased influenza vaccination rates among elderly subjects with asthma. The benefits from vaccination might be greater in this population, as these are known to be associated with various health issues.35–37 Nevertheless, misbeliefs caused by a lack of information, such as concerns about vaccine side effects, may prevent this population from becoming vaccinated. 28 Although the overall influenza vaccination rate is sufficient in elderly subjects with asthma, it is necessary to examine whether there are other underprivileged populations within the elderly.
The strength of this study is that recent influenza vaccination rates among subjects with asthma were analyzed using nationally representative survey data. Through a 10-year trend analysis, our study found that the asthma guidelines’ recommendations for influenza vaccination are not followed in the real world. Nonetheless, very few studies have reported influenza vaccination trends among asthmatic subjects after the 2009 influenza pandemic. Therefore, similar studies need to be conducted in each country to investigate and improve the national influenza vaccination rates in subjects with asthma. Another strength is that comprehensive factors were included to evaluate their association with influenza vaccination, which can help identify subgroups of subjects with asthma in whom to encourage vaccination. However, our study had some limitations. First, the causal relationship identified was uncertain because our study was conducted using cross-sectional data. Second, recall bias was possible because a history of asthma and influenza vaccination was assessed using a questionnaire. Third, common barriers to influenza vaccination among asthmatics, such as support for vaccination and worries about being sick after vaccination, 28 were not investigated in this study. Fourth, although we included the variable of current treatment status (being treated versus untreated) in the analysis, we could not include detailed information on treatment, such as asthma duration or treatment steps, because these data were not available in the KNHANES dataset. Fifth, in some categories, such as underweight elderly subjects, the number of subjects was relatively small. Findings in these categories require cautious interpretation. Finally, the uniqueness of the Korean medical system should be considered when interpreting the results because Korea implements the National Health Insurance System. Therefore, generalizations to other countries must be carefully made.
In conclusion, influenza vaccination rates have been insufficient in subjects with asthma in the last 10 years. The influenza vaccination rate was consistently lower in young subjects with asthma than that in the elderly. In young subjects with asthma, female sex, current asthma treatment, history of pulmonary tuberculosis, and dyslipidemia were positively associated with influenza vaccination, whereas an unmarried status was negatively associated. Public policies to increase influenza vaccination rates in subjects with asthma, considering the factors that are influencing the vaccination rates of young subjects, urgently need to be established.
Supplemental Material
sj-docx-1-taj-10.1177_20406223221123979 – Supplemental material for Trends and factors associated with influenza vaccination in subjects with asthma: analysis of the Korea National Health and Nutrition Examination Survey between 2010 and 2019
Supplemental material, sj-docx-1-taj-10.1177_20406223221123979 for Trends and factors associated with influenza vaccination in subjects with asthma: analysis of the Korea National Health and Nutrition Examination Survey between 2010 and 2019 by Sang Hyuk Kim, Hye Yun Park, Hwasik Jung, Sungmin Zo, Saerom Kim, Dong Won Park, Tai Sun Park, Ji-Yong Moon, Sang-Heon Kim, Tae-Hyung Kim, Jang Won Sohn, Ho Joo Yoon, Hyun Lee and Sun Hye Shin in Therapeutic Advances in Chronic Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.