
Abstract
Background:
The association between prior percutaneous coronary intervention (PCI) and prognosis after coronary artery bypass grafting (CABG) remains uncertain. We aimed to evaluate the aforementioned association in a meta-analysis.
Methods:
PubMed, Cochrane’s Library, and Embase databases were searched for potential studies. A random-effects model was used for the meta-analysis. Meta-regression was performed to evaluate the influence of study characteristics on the outcomes.
Results:
Thirty-six follow-up studies with 308,284 patients were included, and 40,892 (13.3%) patients had prior PCI. Pooled results showed that prior PCI was associated with higher risks of early (in-hospital or within 1 month) all-cause mortality [odds ratio (OR): 1.26, 95% confidence interval (CI): 1.11–1.44, p = 0.003; I2 = 64%] and major adverse cardiovascular events (MACEs; OR: 1.36, 95% CI: 1.12–1.66, p = 0.002, I2 = 79%), but not with late (follow-up durations from 1 to 13 years) mortality (OR: 1.03, 95% CI: 0.95–1.13, p = 0.44, I2 = 46%) or MACEs (OR: 1.03, 95% CI: 0.97–1.09, p = 0.38, I2 = 0%). Meta-regression showed that the study characteristics of patient number, age, sex, diabetic status, and proportion of patients with prior PCI did not affect the outcomes. Sensitivity analyses limited to multivariate studies excluding patients with acute PCI failure showed similar results (early mortality, OR: 1.25, p = 0.003; early MACE, OR: 1.50, p = 0.001; late mortality, OR: 1.03, p = 0.70).
Conclusion:
The current evidence, mostly from retrospective observational studies, suggests that prior PCI is related to poor early clinical outcomes, but not to late clinical outcomes, after CABG.
Keywords
Introduction
With advances in both devices and techniques, percutaneous coronary intervention (PCI) has been increasingly performed as an important treatment for patients with coronary artery disease (CAD), including low-risk patients as well as high-risk patients such as the elderly 1 and those with diabetes, 2 chronic kidney disease, 3 left main lesions, 4 and multivessel CAD. 5 Consequently, increasing numbers of patients undergoing coronary artery bypass grafting (CABG) have received prior PCI. Accordingly, determining the potential prognostic influence of prior PCI on clinical outcomes for patients undergoing CABG is of particular clinical significance. 6 However, previous studies evaluating the association between prior PCI and prognosis after CABG have shown inconsistent results.7–42 Although a number of meta-analyses have been performed on this topic, the results of these studies were also inconsistent. Two early meta-analyses including 9 and 14 studies, respectively, concluded that prior PCI may be related to a higher incidence of postoperative mortality within 1 month, but not to midterm mortality up to 5 years after CABG.43,44 Another meta-analytic study published in 2018 including eight studies without patients with acute PCI failure showed that prior PCI was not a risk factor of mortality or other adverse outcomes in patients undergoing CABG. 45 However, these conclusions were based on a univariate analysis. A more recent meta-analysis included studies published until 2017 and showed that prior PCI may not affect mortality after CABG. 46 Notably, in that analysis, studies reporting early postoperative and long-term follow-up outcomes were combined, which may have confounded the results. Because a number of recently published studies have consistently shown that prior PCI did not affect mortality after CABG,33,35–39 we included these studies in an updated meta-analysis to evaluate the potential influences of prior PCI on early and late clinical outcomes in patients undergoing CABG.
Methods
The Meta-analysis of Observational Studies in Epidemiology (MOOSE) 47 and Cochrane’s Handbook 48 guidelines were followed during the design, performance, and reporting of the meta-analysis. An ethics approval is not needed for this study because this is a meta-analysis of previous published studies.
Literature search
Systematic searches of the PubMed, Cochrane’s Library, and Embase electronic databases were performed to obtain relevant studies from inception to 26 November 2021. The combined search terms were used: (1) ‘previous’ OR ‘prior’ OR ‘before’ OR ‘after’ OR ‘history’; (2) ‘percutaneous coronary intervention’ OR ‘percutaneous transluminal coronary angioplasty’ OR ‘stent’ OR ‘angioplasty’ OR ‘revascularization’ OR ‘reperfusion’ OR ‘PCI’ OR ‘PTCA’; and (3) ‘coronary artery bypass grafting’ OR ‘CABG’. Only clinical studies published in English were included. References of elated original studies and review articles were also searched for potential studies.
Study selection
The inclusion criteria were (1) articles reporting longitudinal follow-up studies published in peer-reviewed journals, including cohort studies, post hoc analyses of randomized controlled trials (RCTs) and nested case–control studies; (2) studies that enrolled at least 100 adult patients with CAD who underwent CABG; (3) studies that compared the early (in-hospital or within 1 month after surgery) and late (during follow-up for at least 1 year) all-cause mortality or major adverse cardiovascular events (MACEs) in patients with and without prior PCI; and (4) studies that reported the odds ratios (ORs) for the associations between prior PCI and outcomes after CABG after adjustment of potential confounding factors. For studies with nonsignificant results on univariate analysis and without further analyses by multivariate analysis, ORs from univariate analysis were used, and these studies were also included to reduce the potential publication bias. The definition of MACEs was consistent with those used in the original articles, which typically included cardiac death, nonfatal myocardial infarction, nonfatal stroke, severe or deterioration of heart failure (HF), or repeated revascularization. Outcomes occurred between 1 month and 1 year after surgery was not evaluated because these outcomes were rarely reported in the included studies. Reviews, duplications, and irrelevant studies were excluded.
Data extraction and quality evaluation
Database searches, data extraction, and study quality evaluation were independently performed by two authors (HZ and ZZ). Discussion with the corresponding author was indicated if discrepancies occurred. Data regarding study information, study design, patient characteristics, PCI methods [percutaneous transluminal coronary angioplasty (PTCA) and stent type], and follow-up duration were extracted. Moreover, confounding factors for which adjustment was made were also recorded. The Newcastle–Ottawa scale was used as an instrument for study quality evaluation. 49 This scale ranges from 1 to 9 stars and assesses study quality mainly regarding three domains: study group selection, between-group comparability, and validation of the outcomes of interest.
Statistical analyses
We used the OR with corresponding 95% confidence interval (CI) as the main measure for the association between prior PCI and outcomes after CABG. For studies reporting ORs with more than one multivariable adjusted model, the one with the most adequate adjusted model was chosen for analysis. ORs and their corresponding standard errors (SEs) were calculated from 95% CIs or p values, and a logarithmical transformation was performed to stabilize variance and normalize the distribution. 48 The Cochrane’s Q test, as well as I2 statistic estimation, was performed to measure heterogeneity. 50 An I2 > 50% suggested significant heterogeneity. We used a random-effects model for the meta-analysis of OR data because this model incorporates the potential heterogeneity among the included studies to calculate a more generalized result. 48 By omitting one individual study at a time, we performed sensitivity analyses to test the robustness of the results. 51 Moreover, univariate meta-regression analyses were performed to evaluate the influences of sample size, patient age, sex, diabetic status, proportion of patients with prior PCI, and follow-up duration on the outcomes. In addition, because inclusion of patients with acute PCI failure may confound the findings, we performed sensitivity analyses limited to multivariate studies that had excluded patients with acute PCI failure. The potential publication bias was initially detected by visual inspection of the symmetry of funnel plots and then confirmed by Egger’s regression asymmetry test. 52 A value of p < 0.05 was considered as statistically significant. RevMan (Version 5.1; Cochrane Collaboration, Oxford, UK) software was used for the meta-analysis.
Results
Literature search
Figure 1 shows the literature search process. Briefly, 3502 articles were obtained via the initial database searches after exclusion of the duplications. An additional 3438 articles were excluded through screening of the titles and abstracts. Subsequently, 64 records underwent full-text review, and 28 were further excluded based on reasons listed in Figure 1. Finally, we included 36 studies in this meta-analysis.7–42

Flowchart of database searches and study identification.
Study characteristics and quality evaluation
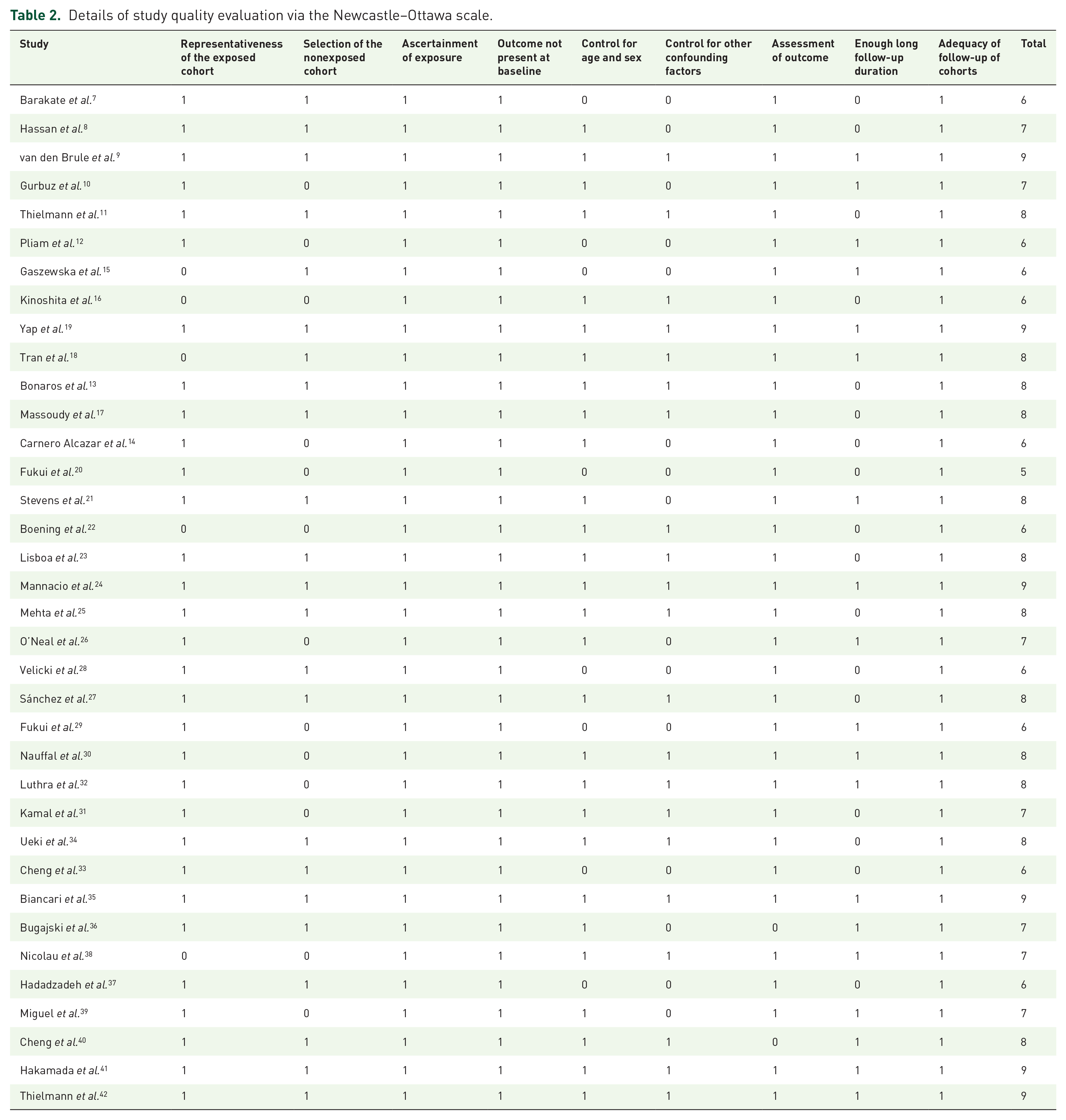
The characteristics of the studies are presented in Table 1. All the studies were retrospective observational studies, except for two studies,23,36 which were prospective. These studies were published between 2003 and 2021. The number of patients in each study varied from 160 to 63,420. In total, 308,284 patients who underwent CABG were included, and 40,892 (13.3%) had received prior PCI. The details of prior PCI were generally poorly reported. Procedures of PTCA with or without stent implantation were performed, and bare metal stents (BMS) seemed to be used more frequently than drug-eluting stents (DES) in most of the included studies. The follow-up durations varied from within hospitalization to 13 years after surgery. Demographic factors, CAD risk factors, comorbidities, coronary lesion characteristics, and perioperative characteristics were adjusted varyingly in most of the included studies, while nine studies with nonsignificant results on univariate analysis were also included.7,12,15,20,28,29,33,36,37 Fifteen multivariate studies excluded patients with acute PCI failure.8,9,11,13,17–19,21,23,25,27,34,35,38,41 Because four studies reported outcomes according to the times of prior PCI11,17,35,41 or the duration of the gap between PCI and CABG, 21 multiple datasets were considered for these studies. The Newcastle–Ottawa scale scores of the included studies ranged from 5 to 9, indicating acceptable study quality (Table 2).
Characteristics of the included studies investigated the association between prior PCI and clinical outcomes of CABG.

ACEI, angiotensin-converting enzyme inhibitor; AF, atrial fibrillation; ARB, angiotensin receptor blocker; BMI, body mass index; BMS, bare metal stent; CABG, coronary artery bypass graft; CAD, coronary artery disease; CCI, Charlson Comorbidity Index; CCS, Canadian Cardiology Society; CHF, congestive heart failure; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CPB, cardiopulmonary bypass; CRF, chronic renal failure; CVD, cardiovascular disease; DES, drug-eluting stent; DM, diabetes mellitus; ECC, extracorporeal circulation; eGFR, estimated glomerular infiltrating rate; EUROscore, European System for Cardiac Operative Risk Evaluation; HR, heart rate; HTN, hypertension; IABP, intra-aortic balloon pump; LM, left main; LVEF, left ventricular ejection fraction; MI, myocardial infarction; NR, not reported; NYHA, New York Heart Association; PAD, peripheral artery disease; PC, prospective cohort; PCI, percutaneous coronary intervention; PTCA, percutaneous transluminal coronary angioplasty; RC, retrospective cohort; UA, unstable angina.
Details of study quality evaluation via the Newcastle–Ottawa scale.
Results of meta-analysis
Pooled results of a random-effects model showed that prior PCI was associated with higher risks of early all-cause mortality [39 datasets; OR: 1.26, 95% CI: 1.11–1.44, p = 0.003; I2 = 64%; Figure 2(a)] and MACEs [15 datasets; OR: 1.36, 95% CI: 1.12–1.66, p = 0.002, I2 = 79%; Figure 2(b)] but not with late all-cause mortality [21 datasets; OR: 1.03, 95% CI: 0.95–1.13, p = 0.44, I2 = 46%; Figure 3(a)] or MACEs [3 datasets; OR: 1.03, 95% CI: 0.97–1.09, p = 0.38, I2 = 0%; Figure 3(b)].

Forest plots for the meta-analysis of the associations between prior PCI and early outcomes after CABG: (a) early all-cause mortality and (b) early MACEs.

Forest plots for the meta-analysis of the associations between prior PCI and late outcomes after CABG: (a) late all-cause mortality and (b) late MACEs.
Meta-regression and sensitivity analyses
Meta-regression showed that patient number, age, sex, diabetic status, proportion of patients with prior PCI, and follow-up duration did not affect the outcomes (Table 3). Sensitivity analyses involving exclusion of each dataset individually did not significantly change the results (Supplemental Table 1). Sensitivity analyses limited to multivariate studies excluding patients with acute PCI failure showed similar results regarding early all-cause mortality [20 datasets, OR: 1.25, 95% CI: 1.08–1.45, p = 0.003; Figure 4(a)], early MACEs [8 datasets, OR: 1.50, 95% CI: 1.18–1.90, p = 0.001; Figure 4(b)], and late all-cause mortality [10 datasets, OR: 1.03, 95% CI: 0.90–1.16, p = 0.70; Figure 4(c)]. Only one multivariate study without patients with acute PCI failure was available, 9 which showed that prior PCI was not associated with late MACEs after CABG (OR: 1.03, 95% CI: 0.97–1.10, p = 0.36).
Results of univariate meta-regression analysis.

CI, confidence interval; DM, diabetes mellitus; MACEs, major adverse cardiovascular events; PCI, percutaneous coronary intervention.

Sensitivity analyses including only multivariate studies without acute PCI failure: (a) early all-cause mortality; (b) early MACEs; and (c) late all-cause mortality.
Publication bias
The funnel plots for the meta-analysis of the associations between prior PCI and risks of early all-cause mortality, early MACEs, and late all-cause mortality are shown in Figure 5(a)–(c). These plots appeared symmetric on visual inspection, suggesting low risk of publication bias. Egger’s regression tests showed similar results (p values = 0.281, 0.385, and 0.402, respectively). The publication bias for the meta-analysis of the association between prior PCI and late MACEs after CABG could not be evaluated because only three studies were included.

Funnel plots for the meta-analysis of the associations between prior PCI and outcomes after CABG: (a) early all-cause mortality; (b) early MACEs; and (c) late all-cause mortality.
Discussion
This updated meta-analysis including data from 36 up-to-date studies showed that overall, prior PCI was associated with increased risks of early all-cause mortality and MACEs after CABG, while the risks of late all-cause mortality and MACEs were not significantly affected. These results were further validated by sensitivity analyses limited to multivariate studies excluding patients with acute PCI failure. Moreover, meta-regression analyses showed that study characteristics including patient number, age, sex, diabetic status, proportions of those with prior PCI, and follow-up duration did not significantly affect the results. Taken together, the current evidence mainly based on retrospective studies suggests that prior PCI is related to poor early clinical outcomes, but not late clinical outcomes, after CABG. Large-scale prospective cohort studies in the era of current PCI status should be performed to validate these findings.
Compared with previous meta-analyses of the same topic,43–46 our study has the following strengths. First, this is the largest meta-analysis in this field to date, with the inclusion of 36 follow-up studies with 308,284 patients. The large number of studies and patients could guarantee adequate statistical power for evaluation of the clinical outcomes. Second, studies with nonsignificant findings on univariate analyses were included, which substantially lowered the risk of publication bias of the meta-analysis. Third, sensitivity analyses limited to multivariate studies excluding patients with acute PCI failure were performed to reduce the potential influence of confounding factors in the main meta-analysis. The results of the sensitivity analyses further confirmed the findings of the main meta-analysis. Finally, meta-regression analyses showed that the findings were independent of study characteristics including patient number, age, sex, diabetic status, proportions of those with prior PCI, or follow-up duration, which further confirmed the robustness of the findings.
The potential mechanisms underlying the association between prior PCI and poor early clinical outcomes after CABG may include the following. First, an implanted stent as compared with naïve vessel may be associated with an increased inflammatory response and endothelial dysfunction, which may lead to an increased risk of vascular events after CABG in patients with prior PCI. 53 A recent study showed that compared with drug therapy alone, coronary stent intervention therapy has better clinical efficacy and short- and long-term prognosis in treating CAD, but it is easy to promote inflammatory reaction after surgery, as evidenced by increased levels of matrix metalloproteinase-9 and interleukin-33 in patients after coronary stenting. 54 Higher levels of inflammatory cytokines before the procedure have been well confirmed as the predictors of poor postoperative prognosis in patients after CABG. 55 Moreover, because anastomosis during CABG could be performed in the segment of coronary arteries that have already been implanted with stents, prior PCI with stents may technically challenge the procedure of CABG by leading to the limitations in distal anastomosis during CABG. 56 Also, prior PCI may compromise the collateral blood flow, which therefore may affect the patency of the graft after CABG. It has been shown that in patients with non-ST-elevation acute coronary syndrome who developed periprocedural myocardial infarction, microvascular resistance increased significantly after PCI. 57 These findings suggested that when collateral flow is accounted for, removal of epicardial stenosis is associated with compromised collateral blood flow, 57 while patients with well-matured collaterals were shown to have a significantly higher rate of procedural success during CABG, particularly for those with chronic total occlusions of the coronary arteries. 58 Finally, prior PCI before CABG may be a marker of generally poor clinical status and a high burden of atherosclerotic lesions, which may also lead to a poor acute outcome after CABG. Future studies are needed for further analyses of the possible mechanism underlying the adverse influence of prior PCI on early outcomes after CABG, which may be helpful to improve the prognosis in these patients. On the other hand, our meta-analysis showed that prior PCI was not related to mortality or incidence of MACEs during follow-up. This seems to be consistent with comparable long-term survival among patients who received PCI or CABG, as evidenced by recent clinical trials or meta-analyses, particularly for those with high-risk lesions such as lesion in the left main artery.59–61
Limitations
The results of meta-regression showed that study characteristics including patient number, age, sex, diabetic status, proportions of those with prior PCI, and follow-up duration did not significantly affect the association between prior PCI and CABG outcomes. However, significant heterogeneity was detected among the meta-analyses. From a clinical perspective, interactions between coronary lesions, features and outcomes of prior PCI, and sources and locations of the grafts are key factors that could affect the clinical outcomes of the patients. Besides, the time gap between prior PCI and CABG may also affect the clinical outcomes of the patients. Unfortunately, none of the above factors were analyzed in detail in the included studies. Accordingly, we were unable to analyze the influences of these factors on the outcomes in our meta-analysis. Specifically, studies published after 2017 almost consistently suggested that prior PCI did not affect early or late clinical outcomes after CABG, which may also indicate that PCI performed in current clinical practice may not adversely affect the prognosis after CABG. Large-scale prospective studies with detailed analyses of the interactions between coronary lesions, features and outcomes of prior PCI, and sources and locations of the grafts are needed to determine the influence of prior PCI on outcomes after CABG in current clinical practice. Other limitations should also be noted when interpreting the results of our meta-analysis. First, most of the included studies were retrospective, which may be associated with possible risk or recall bias and selection bias. Moreover, it has been indicated that some specific procedural conditions related to CABG may also significantly affect the postoperative outcomes in patients with CAD, such as off-pump or on-pump CABG, 62 concurrent coronary atherectomy, 63 achievement of total arterial revascularization, and so on. 64 Prospective studies with adequate details of above procedural characteristics are needed to determine whether differences in these conditions may affect the association between prior PCI and outcomes after CABG. In addition, noncardiovascular postoperative adverse events were not analyzed in our meta-analysis because studies reporting these outcomes were limited and mainly based on univariate analyses. Moreover, studies published as conference abstracts or in languages other than English were not included, which may confound the findings. Finally, the differences in the experience levels of the performers of PCI and CABG may also affect the results, but were generally not evaluated in the included studies.
Conclusion
In conclusion, the results of this updated meta-analysis suggest that prior PCI is related to poor early clinical outcomes, but not late clinical outcomes, after CABG. Large-scale prospective studies with detailed analyses of the interactions between coronary lesions, features and outcomes of prior PCI, and sources and locations of the grafts should be performed to determine the influence of prior PCI on clinical outcomes after CABG in current clinical practice.
Supplemental Material
sj-docx-1-taj-10.1177_20406223221078755 – Supplemental material for Prior percutaneous coronary intervention and outcomes in patients after coronary artery bypass grafting: a meta-analysis of 308,284 patients
Supplemental material, sj-docx-1-taj-10.1177_20406223221078755 for Prior percutaneous coronary intervention and outcomes in patients after coronary artery bypass grafting: a meta-analysis of 308,284 patients by Hongliang Zhang, Zhenyan Zhao, Jing Yao, Jie Zhao, Tao Hou, Moyang Wang, Yanlu Xu, Bincheng Wang, Guannan Niu, Yonggang Sui, Guangyuan Song and Yongjian Wu in Therapeutic Advances in Chronic Disease
Footnotes
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.