
Abstract
Cryptococcal neoformans is a rare fungal pathogen that has been associated with immunocompromised individuals. Due to its rare occurrence, clinicians have a low index of suspicion for diagnosis, which can lead to increased morbidity and mortality. We present an 81-year-old fully functional woman with no known predisposing risk factors or previous immunocompromising conditions who was found to have cryptococcal meningitis on cerebrospinal fluid analysis in the setting of newly diagnosed uncontrolled type 2 diabetes and systemic lupus erythematosus (SLE).
Keywords
Introduction
Cryptococcus neoformans is an encapsulated yeast that primarily affects immunocompromised individuals with meningo-encephalitis as the most common form of infection. 1 Due to its predilection for patients with impaired immunity, cryptococcal meningitis is often initially overlooked in the absence of typical immunocompromising risk factors such as HIV, hematologic malignancy, use of immunosuppressive therapies, sarcoidosis, and liver disease.1,2 Therefore, it is important to keep a broad differential as well as consider alternative comorbidities that have been associated with Cryptococcus. Recent literature data have also seen an emergence of cases with systemic diseases such as diabetes mellitus and systemic lupus erythematosus (SLE).3,4 We present an 81-year-old woman without known predisposing risk factors or previous immunocompromising conditions, found to have cryptococcal meningitis in the setting of newly diagnosed uncontrolled type 2 diabetes and SLE.
Case report
An 81-year-old woman with recently diagnosed uncontrolled diabetes presented to the emergency department with rapidly progressive mental status change. Two months prior, she was admitted for diabetic ketoacidosis, found to have an A1C of 14.7%, and ultimately discharged on insulin. Over the following month, she experienced progressive cognitive decline. At baseline, she was able to carry out activities of daily living (ADLs) and then over the course of a month, she declined to the point that she was only responsive to name and minimally arousable. Relevant medications included recent prescriptions of memantine and sertraline for which the patient’s sister endorsed no missed doses. The history was obtained from the sister who stated the patient had no acute complaints prior to these symptoms. Upon initial examination, she was noted to be hemodynamically stable and only minimally arousable to speech. Brudzinski’s and Kernig’s signs were negative and hyperreflexia was evident on her patellar reflex. An initial extensive serological evaluation was unremarkable (Table 1). Brain imaging was obtained with computed tomography and subsequently magnetic resonance imaging (MRI) (Figure 1), which demonstrated microvascular changes consistent with age without acute intracranial pathology
Initial serologic and urologic workup.
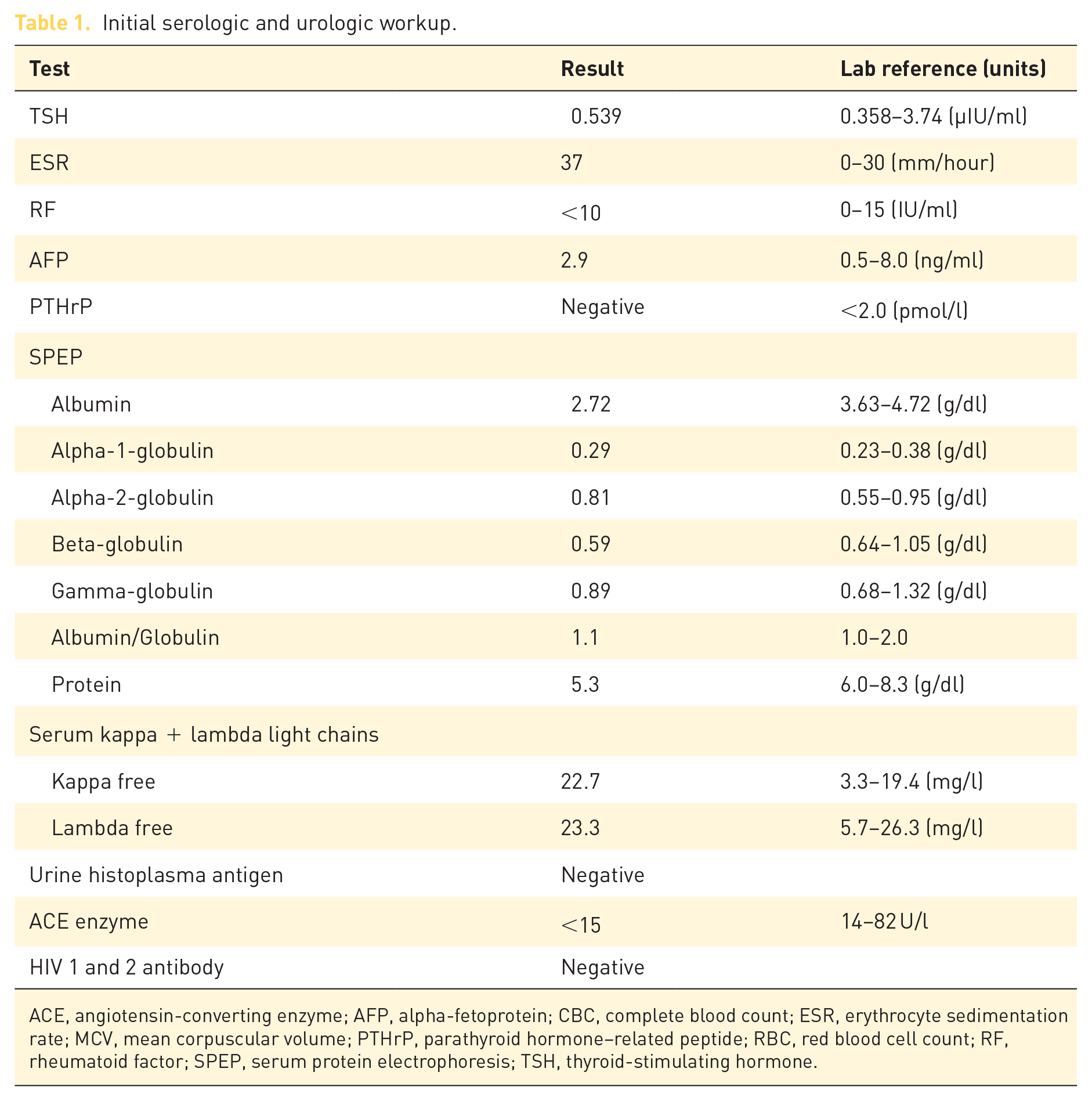
ACE, angiotensin-converting enzyme; AFP, alpha-fetoprotein; CBC, complete blood count; ESR, erythrocyte sedimentation rate; MCV, mean corpuscular volume; PTHrP, parathyroid hormone–related peptide; RBC, red blood cell count; RF, rheumatoid factor; SPEP, serum protein electrophoresis; TSH, thyroid-stimulating hormone.
Cerebrospinal fluid studies.

HSV, herpes simplex virus; PCR, polymerase chain reaction; RBC, red blood cell; WBC, white blood cell.

MRI of the brain.
Electroencephalogram (EEG) demonstrated decreased generalized activity but otherwise unremarkable. A lumbar puncture (LP) was performed with cerebrospinal fluid (CSF) showing lymphocyte pleocytosis, low glucose, and elevated protein (Table 2), raising suspicion for infectious meningitis and prompting initiation of broad-spectrum antibiotics, antiviral drugs, and corticosteroids. HIV screening was negative. On the third hospital day, cryptococcal antigen from the LP returned positive as did the India ink stain. Prior antimicrobials were discontinued and amphotericin 4 mg/kg every 24 h was initiated. Flucytosine was not available, so fluconazole (renal dosing) 400 mg PO once daily was used as an alternative. Two-week follow-up CSF cultures were without growth, and she was transitioned to fluconazole consolidation. Atovaquone was also started for opportunistic prophylaxis in the setting of identified lymphopenia. Over the next few months, the patient slowly returned to baseline and was able to perform all ADLs/instrumental ADLs. Following discharge, she was evaluated as an outpatient for lymphopenia that was noted while inpatient. Upon further review of labs, she was noted to have lymphocytopenia for over 10 years although a CD4 count had never been obtained. CD4 count was noted to be decreased at 79 cells/µl, HIV remained negative, and an autoimmune workup was initiated (Table 3). She was subsequently found to have elevated antinuclear antibody (ANA) dilution of 1:640 and anti-double-stranded DNA level of 70 IU/ml. These serologic findings in the setting of leukopenia without alternative cause led to the diagnosis of SLE. Idiopathic CD4 + lymphopenia was entertained, but the constellation of the patient’s symptoms coupled with the strong positive ANA and elevated anti-dsDNA level favored a diagnosis of SLE. Mild proteinuria was also noted on urologic assessment. She was started on hydroxychloroquine and remained stable at subsequent follow-ups.
Leukopenia and autoimmune lab results.

WBC, white blood cell.
Discussion
C. neoformans is a clinically important basidiomycete first illustrated in 1895 with numerous cases seen at the peak of the HIV epidemic in 1980. 1 Global estimations approximate an incidence of 1 million new cases and over 625,000 deaths annually.1,2 The previous classification of the genus was sub-classified into four different serotypes (A, B, C, and D); however, recent molecular capsular assays have allowed the proper identification of these organisms and labeled accordingly. 1 Serotype A is now classified as C. neoformans, B and C as C. neoformans var. grubii, and D as C. neoformans var. neoformans. 5 Serotype A is the most common cause of cryptococcal meningitis worldwide and is commonly implicated in immunocompromised individuals.1,5
Cryptococcal meningitis is primarily seen in individuals with impaired cellular immunity such as HIV, hematologic malignancies, or other immunosuppressive therapies. 1 However, recent literature data have also seen an emergence of cases with systemic diseases such as diabetes mellitus and SLE.3,4 The emerging number of case reports has thus dubbed them among the top 5 risk factors for cryptococcal meningitis infection.3–5 Microbial infections are commonly seen in autoimmune diseases such as SLE as a result of the disease itself, treatment with immunosuppressive therapy, and intrinsic disorder of cellular mediated immunity.4,6 Recent cohort studies in Chinese patients with SLE have noted an increased susceptibility to infection with C. neoformans, accounting for 25.8% of invasive fungal infections.4,6 Over the last few decades, a number of case series and reports have also been seen within the literature correlating the increasing incidence of this fungal disease.7–19 However, while the majority of these reports noted fungal infection in the setting of concurrent immunosuppressive therapy, at the time of diagnosis our patient was not on any immunosuppressive therapy. In fact, her SLE diagnosis was noted after her infection had been treated and this was only suspected due to her long-standing lymphopenia. To our knowledge, there is only one case report which noted a similar presentation of cryptococcal meningitis preceding SLE. 8 The predisposing lymphopenia in the setting of undiagnosed SLE coupled with uncontrolled diabetes mellitus likely led to a dysregulated immune function resulting in a clinical gateway for her cryptococcal infection.
The clinical presentation of cryptococcal meningitis varies largely depending on the host immune system. 1 Immunocompetent patients can present asymptomatically but at times with classical signs and symptoms of clinical meningitis. 1 However, in those with impaired immunity, the clinical presentation can be insidious ranging from asymptomatic nodules to widely disseminated disease.11,12,15 Kwok et al. 16 reported a unique presentation in the form of an isolated cranial nerve 6 palsy. A recent cohort study by Liu et al. comparing clinical and laboratory presentations of cryptococcal meningitis in patients with and without acquired immunodeficiency syndrome (AIDS) noted a substantial difference. In general, patients with cryptococcal meningitis were more febrile, had higher inflammatory scores, had less classical meningeal signs or symptoms, had less imaging findings such as classical MRI meningeal enhancements, and had less specific CSF findings. There are several postulated reasons for the difference in presentation. First, most of the patients with autoimmune diseases are on immunosuppressive therapy which mitigates the inflammatory response, lowering intracranial pressure and thus delaying the clinical meningeal signs/symptoms commonly representative of central nervous system infections.11,18,19,20 Second, the severity of immunosuppression with lymphopenia plays a role in the severity of infection with a lower nadir correlating with higher pathogen burden but lower severity of related symptoms.11,18,19,20 Thus, this can lead to a delay in diagnosis and treatment. Our patient was the perfect analogy of this owing to her non-specific clinical presentation and initial unremarkable diagnostics.
The diagnosis of cryptococcal meningitis has withstood the test of time with relatively little change. The gold standard remains CSF culture.20,21 Unfortunately, this may necessitate up to 2 weeks of time for definitive results. The India ink staining is also utilized primarily in low-resource settings for diagnosis, but the diagnostic utility is poor. 22 Sensitivity can range from 42% to 86% depending on the titer of Cryptococcus burden in the CSF. 22 Thus, it has become prudent for new methods and more readily accessible methods to be introduced. Cryptococcal antigen has a sensitivity and specificity of greater than 99% in both CSF and blood.21–24 Previously, this was performed with the latex agglutination assay, but due to difficulty of performing this specific test, it has been abandoned. Recently, in 2011 the lateral flow assay was approved by the Food and Drug Administration (FDA) due to equivocal results with the former latex assay and can be easily performed in any laboratory.21–24 Neuroimaging with MRI is recommended in these patients but is often unremarkable as discussed above. The classical imaging findings of meningeal enhancement may be present but are often absent, and even if present are not necessarily representative of cryptococcal meningitis. Hence, it is crucial for the clinician to take into account the overall clinical presentation and remain on alert for this diagnosis.
The treatment of cryptococcal meningitis involves 4–6 weeks of induction therapy with amphotericin B and flucytosine, followed by 8 weeks of consolidation therapy with fluconazole and 6–12 months of maintenance therapy with fluconazole. 25 However, in resource-limited setting, there a number of regimens that have been designed to take this into account. Our health system did not have access to flucytosine; thus, we utilized an alternate combination regimen of amphotericin B and fluconazole for the induction therapy. Lepak and Andes 26 examined the pharmacokinetics and pharmacodynamics of antifungals, noting fluconazole to be an acceptable alternate in combination with amphotericin with fewer side effects than seen with flucytosine. However, there are growing reports of failed therapy with the classical combination, and thus new treatment methods have been proposed. Isavuconazole and voriconazole are possible avenues in a few case reports for refractory cases, but the data are few and require more extensive prospective studies. Recently, there has also been introduction of a neurapheresis device to the FDA which is capable of performing extracorporeal filtration in human subjects removing CSF yeast burden. The results in animal models have been promising, but human trials are still pending and yet to begin.
Conclusion
Cryptococcal meningitis is an opportunistic infection that can present in HIV-negative patients with underlying immunocompromised conditions. It is a major cause of morbidity and mortality in immunocompromised hosts. Early recognition and treatment can lead to improved outcomes. Previously, immunocompetent patients should be screened for HIV and CD4 count. First-line treatment involves the utilization of amphotericin and flucytosine, but fluconazole is also an acceptable alternative.
Footnotes
Acknowledgements
The authors express our gratitude to the patient for permiting us to present this case.
Ethics approval and consent to participate
Our study did not require formal approval from an IRB board because this was a case report. Informed consent was verbally obtained from the patient.
Consent for publication
Informed consent was obtained from patient for publication and use of images.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
Not applicable.