
Abstract
Objective
To investigate the clinical features and outcomes of cryptococcal meningitis (CM) in HIV-negative patients with and without lung infections.
Methods
We retrospectively reviewed the medical records of HIV-negative patients with CM admitted to two university hospitals in Southwest China over the past 5 years.
Results
Seventy-one patients were included, of whom 35 (49.3%) had lung disease. Compared with patients without lung infection, CM patients with lung infection tended to be male and younger (≤30 years), experienced more fever, less vomiting and fewer central nervous system symptoms; more often had low white blood cell (WBC) counts (<20 × 106/L), and fewer often had ethmoid sinusitis, maxillary sinusitis, paranasal sinusitis, and otitis media. Cryptococcus neoformans isolates from these patients were sensitive to itraconazole, voriconazole, fluconazole, and amphotericin B but resistant to flucytosine. CM patients with lung infection had higher mortality at discharge compared with patients without lung infection (8.6% vs. 0%). Multivariable analyses showed that a WBC count <20 × 106/L was significantly associated with poor treatment outcome (odds ratio 0.01, 95% confidence interval 0–0.83).
Conclusion
HIV-negative CM patients with lung infections tended to be male and younger. Fever, fewer central nervous system symptoms, and WBC counts <20 × 106/L were characteristic of this patient group.
Keywords
Introduction
Cryptococcosis is a fungal infection caused by members of the Cryptococcus gattii-Cryptococcus neoformans species complex. The two varieties of C. neoformans have been raised to species level, as have the five genotypes within C. gattii.1,2 Cryptococcal meningitis (CM) caused by C. neoformans is a common opportunistic infection and the main cause of mortality in human immunodeficiency virus (HIV)-infected patients. Annually more than 200,000 HIV-positive individuals develop CM with approximately 180,000 die.3,4 Recently, CM has increasingly been observed among patients with non-HIV immunosuppression, and the mortality of CM in HIV-negative individuals seem to be no better than in HIV-positive patients.5–7 In immunosuppressed individuals, infection begins in the lung following inhalation of fungal spores and often spreads to other organs, particularly the brain. 8 Many CM patients also have concomitant lung involvement, which is often overlooked or misdiagnosed as tuberculosis. 9 Lung infection can cause many symptoms, such as fever and headache, which may be confused with central nervous system (CNS) infection. In addition, the clinical features and computed tomography signs associated with pulmonary cryptococcosis are not specific. 10 The disease can mimic bacterial pneumonia, pulmonary tuberculosis, and lung cancer.11–13
The clinical characteristics and outcomes of CM have been shown to vary depending on the patient’s underlying condition. Hepatitis B virus (HBV)-positive CM patients present with lower cerebrospinal fluid (CSF) white blood cell (WBC) counts, lower total protein in the CSF (levels less often exceeding 0.45 g/L), higher glucose levels in the CSF, and a higher proportion of normal brain images compared with HBV-negative CM patients. 14 Compared with immunocompromised patients, CM presents in a younger population of immunocompetent patients with more frequent initial complaints of visual and auditory symptoms, higher CSF WBC counts, and higher proportions of normal brain images. 15 In addition, elderly patients (≥65 years) are more vulnerable to CM than adults aged <65 years; these patients were more often women and had higher rates of altered consciousness and recent cerebral infarction. 16 Therefore, we hypothesized that HIV-negative CM patients with lung infection may present with atypical features, leading to significant delays in diagnosis and poorer outcomes.
Many HIV-negative CM patients with and without lung cryptococcosis are seen in the clinic, but few epidemiological studies have been conducted on these patients. Although the long-term risk of CM in patients with HIV is clear, the same cannot be said regarding this infection in HIV-negative patients with lung infection. Here, we retrospectively reviewed the medical records of HIV-negative patients with CM who were admitted to two Chinese university hospitals in Southwest China over the past 5 years.
Patients and methods
Study population and definitions
Inclusion criteria were: (1) hospitalized in the First Affiliated Hospital of Army Medical University in Chongqing or the Affiliated Hospital of North Sichuan Medical College in Nanchong City of Sichuan Province, China, from January 2014 to December 2018; (2) an isolate of C. neoformans detected from CSF culture; and (3) diagnosis of CM.
Patients with pneumonia and tuberculosis were classified as having lung infection. Sex, age, length of hospitalization, CSF profiles, brain images, underlying diseases, initial presentation, drug resistance of C. neoformans, antifungal therapies and outcomes were recorded. Patient outcomes were classified as “cured”, “improved”, “other”, “untreated”, “invalid”, and “death” at discharge and further classified as either satisfactory (cured or improved) and unsatisfactory (other) in accordance with previous studies.15,17
This study was approved by the Ethics Committee of the First Affiliated Hospital of Army Medical University (KY2019132) and was conducted in accordance with the principles laid out in the Declaration of Helsinki. Because the study did not disclose the patients’ personal information, an exemption from informed consent was obtained from the ethics committee. No administrative permission was required to access data.
Detection of C. neoformans and drug resistance
CSF isolates were identified at the species level using the Vitek-2 Compact automatic analyzer (BioMeriéux, Craponne, France). The minimum inhibitory concentration was determined in the Clinical & Laboratory Standards Institute document M44-A2 to assess in vitro susceptibility of isolates to systemic antifungal agents. Candida glabrata (ATCC15126) was used as a control strain.
Statistical analysis
SPSS version 17.0 (SPSS Inc., Chicago, IL, USA) was used to analyze the data. Data were presented as means ± standard deviations or medians and ranges. Independent Student’s t-tests and Mann–Whitney U tests were used to compare normally-distributed and non-normally distributed data, respectively. Categorical variables were compared using the Chi-squared test or Fisher’s exact test. Regression equations for predicting the outcomes of CM were established. Values of P<0.05 were considered statistically significant. All tests were two-sided.
Results
Demographic data
Over the 5 years from January 2014 to December 2018, 58 patients from Southwest Hospital were enrolled in the study. Fourteen (24.1%) patients were HIV-positive. Forty patients from North Sichuan Medical College were included in the study, of whom 13 (32.5%) were HIV-positive. Among the 71 HIV-negative CM patients, 35 (49.3%) had lung disease.
Compared with patients without lung infection, CM occurred more frequently in male and younger (age <30 years) patients with lung infection. Compared with CM patients without lung infection, CM patients with lung infection more often had fever (P = 0.001), edema of the lower extremities (P = 0.001), and cough and expectoration (P = 0.001). These patients also experienced less vomiting, fewer CNS symptoms, and less ventosity although these differences were not statistically significant. There were no significant differences in underlying diseases, clinical factors, or complications between CM patients with and without lung infections (Table 1).
Demographic and clinical features of HIV-negative CM patients with and without lung diseases.

Data are shown as n (%) or median (range).
Laboratory data
The Pandy test of CSF was often positive for CM patients with and without lung infection. Chloride ion and glucose levels were decreased and total protein levels were increased in both patient groups. However, the percentage of CM patients with lung infection who had WBC counts <20 ×106/L was higher than that of CM patients without lung infection (P = 0.036). Computed tomography or magnetic resonance imaging showed that the frequencies of ethmoid sinusitis, maxillary sinusitis, paranasal sinusitis, and otitis media in CM patients without lung function were higher than those of patients with lung infection (P = 0.02, Table 2).
Cerebrospinal fluid characteristics and brain images of patients with cryptococcal meningitis in HIV-negative cryptococcal meningitis patients with and without lung diseases.
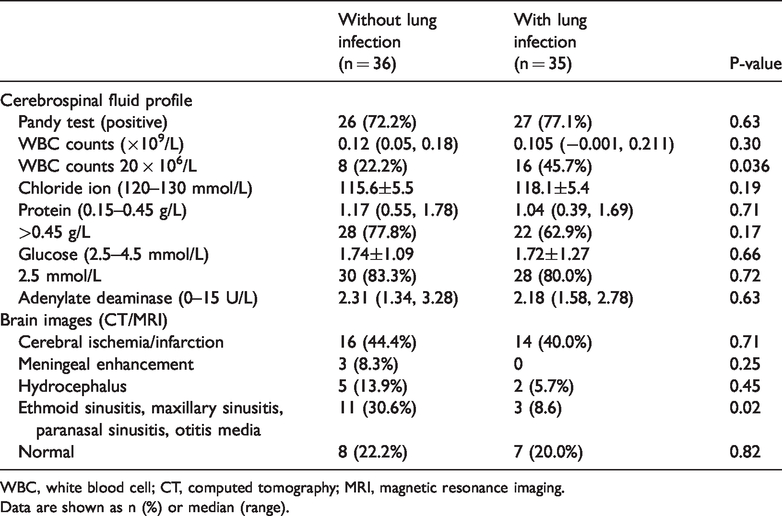
WBC, white blood cell; CT, computed tomography; MRI, magnetic resonance imaging.
Data are shown as n (%) or median (range).
Antifungal therapy and outcome
Most of the C. neoformans isolates from the CSF of patients with and without lung infection were sensitive to itraconazole, voriconazole, fluconazole, and amphotericin B but resistant to flucytosine (Table 3). More CM patients with lung infection were treated with fluconazole + amphotericin B than patients without lung infection (P = 0.035). The symptoms of CM in most patients with and without lung infection were improved at discharge (Table 4).
Drug resistance of Cryptococcus neoformans isolates.

Data are shown as n (%).
Antifungal therapies and outcomes.

Others* include discharged and lost to follow-up.
Data are shown as n (%).
Risk factors for poor treatment outcomes
We included eight factors potentially impacting the prognoses of CM patients in a regression model: lung infection, sex, age, fever, WBC counts <20 × 106/L, chloride ion level, protein level, and glucose levels. Multiple regression analysis showed that WBC counts <20 × 106/L were significantly associated with poor treatment outcome (P = 0.041). Lung infection showed a weak potential association poor with treatment outcome (P = 0.06) (Table 5).
Factors associated with poor prognosis in HIV-negative CM patients.
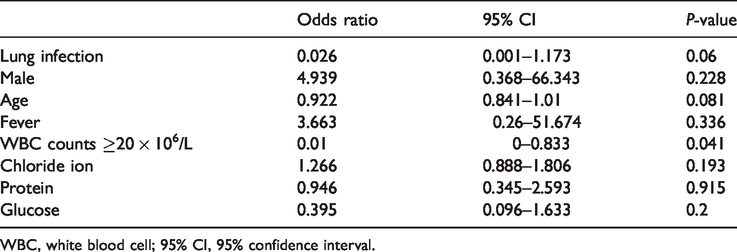
WBC, white blood cell; 95% CI, 95% confidence interval.
Discussion
Lung infection affects many people in China, and our study revealed a high proportion (49.3%) of CM patients with lung infection. In the current study, the sex and age of CM patients with and without lung infection were not significantly different; however, CM occurred more frequently in male and younger patients (aged ≤30 years) with lung infection than in patients without lung infection. Patients with CM presented with neurological symptoms, most typically headache and altered mental status, as well as with fever, nausea and vomiting. In the current study, patients primarily had neurological symptoms such as headache, followed by fever, vomiting, and dizziness, and the symptoms of the two patient groups were similar.
A large proportion of HIV-negative CM patients may have a marked systemic inflammatory response and hydrocephalus. 18 In our study, CM patients with lung infection presented more often with fever, cough and expectoration, less often with CNS symptoms, and more often WBC counts in CSF <20 × 106/L. This may suggest a higher inflammatory response in the brain in patients with lung infection than in patients without lung infection. In addition, patients with lung infection had less vomiting, ventosity, ethmoid sinusitis, maxillary sinusitis, paranasal sinusitis, and otitis media than patients without lung infection. In addition, 28.6% of patients had edema of the lower extremities; clinicians should pay attention to this symptom.
In contrast to the rare resistance of C. neoformans to flucytosine (12%) observed in previous studies,19,20 our results showed that C. neoformans isolates from CSF were sensitive to fluconazole but often resistant to flucytosine (22.5%). Most of the recommendations for the management of non-HIV CM patients have been extrapolated from studies of HIV patients receiving combination therapy with amphotericin B and flucytosine.21,22 However, only 11.3% of CM patients were treated with amphotericin B + flucytosine in our study; most (62.0%) patients received fluconazole + amphotericin B because of C. neoformans resistance to flucytosine. Assessment of outcomes in patients with HIV-associated CM in Africa suggested a 3-month mortality of 70%. 23 In prospective studies, the mortality of patients treated with fluconazole at 10 weeks was 50% to 60%.23,24 In the current study, 67.6% of patients had satisfactory results of treatment at discharge, consistent with previous studies. In HIV-negative individuals, altered mental status, markers of poor inflammatory response, and low CSF WBC counts have been linked with poor prognosis. 25 According to our results, the mortality of CM patients with lung infection group was elevated, consistent with their reduced CSF white cell counts. Furthermore, multivariable analyses showed that a WBC count <20 × 106/L was associated with poor treatment outcome.
Our study had some limitations. First, the study was performed in only two hospitals in Southwest China, we only investigated the past 5 years of clinical records of CM patients, and the number of patients enrolled was relatively small. Second, C. neoformans can be divided into three genotypes: AFLP1/VNI, AFLP1A/VNB/VNII and AFLP1B/VNII.2,26 Some C. neoformans isolates with unique genotypes have higher virulence or rates of azole resistance. This investigation was a retrospective study, so we could not provide genotype data for related C. neoformans isolates, and we could not assess the long-term outcomes of patients. Further multicenter studies are needed to confirm our results and to investigate the factors contributing to improved diagnosis and treatment of CM patients with lung infection. Third, the mechanisms through which patients develop CM with CNS involvement without developing cryptococcosis in the lung prior to dissemination are unclear, and need further investigation.
In conclusion, we found that compared with CM patients without lung infection, patients with lung infection tended to be male and younger. These patients more often experience fever, edema of the lower extremities, and cough and expectoration, less often experienced CNS symptoms, vomiting and ventosity. More often had WBC counts <20 × 106/L, and less often had ethmoid sinusitis, maxillary sinusitis, paranasal sinusitis, and otitis media. Understanding the roles of these factors in the diagnosis of CM in patients with lung infection is important for clinical decision making.
Footnotes
Authors’ contributions
Ming Yang and Fengjun Sun collected and analyzed the data. Fu Liu, Wei Feng, Pu Yao, and Bangbi Weng collected the data. Lin Cheng wrote the manuscript. Peiyuan Xia reviewed the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Sichuan Science and Technology Program of China (2018JY0415).