
Abstract
Up to now, a variety of immune checkpoint inhibitors (ICIs) have been proved to have good therapeutic effects in the treatment of hepatocellular carcinoma (HCC). However, the effects of their applications in liver transplant (LT) recipients are still unclear. In this analysis report, the clinical applications and therapeutic effects of ICIs on LT recipients with hepatic tumor recurrence or de novo carcinoma based on eight databases, including PubMed, EMBASE, Web of Science, Google Scholar, China National Knowledge Infrastructure, Wanfang Data, and CQVIP, were investigated. And the prior treatment, disease response, adverse reactions, and prognosis of patients with malignant tumors after LT and receiving ICI treatments were analyzed. After screening, a total of 28 articles with 47 recipients on the application of ICIs after LT were included. In these patients, their median age was 57 (14–71) years and the main type of tumor after LT was HCC (59.6%). The overall remission rate following ICI treatment was 29.8% (14/47) and the disease progression rate was 68.1% (32/47). Among all these patients, 31.9% (15/47) of patients had immune rejection; the median survival time was 6.5 (0.3–48) months, and the fatality rate was 61.7% (29/47). Considering that the therapeutic effect of ICIs in LT recipients with HCC recurrence or de novo carcinoma is not ideal, ICI treatment should be carefully considered for LT patients, and further research is needed.
Introduction
Liver transplantation (LT) is an effective treatment for the various end-stage liver diseases such as decompensated cirrhosis and hepatocellular carcinoma (HCC), and the postoperative survival rate of patients is continuously improving. 1 However, due to long-term use of immunosuppressants, the incidence of postoperative HCC recurrence in LT recipients is significantly higher than in the general population,2–5 which is an important factor affecting the long-term survival of recipients after surgery. In recent years, immune checkpoint inhibitors (ICIs), a new type of anti-tumor drugs, have shown significant survival benefits in a variety of tumor types.6–9 Nevertheless, there are few studies in the field showing that ICIs are effective in malignant tumors after LT. This study collected data from LT patients using ICIs to treat malignant tumors through literature search and performed a preliminary analysis of the safety and effectiveness of the clinical application of ICIs after LT.
Methods
Literature search
In this study, eight databases including PubMed, EMBASE, Web of Science, Google Scholar, China National Knowledge Infrastructure, Wanfang Data, and CQVIP, were used to search relevant literature in Chinese and English from the establishment of the databases to 1 February 2021. The searching term included ‘((Immune Checkpoint Inhibitors) OR (ICIs) OR (Immunocheckpoint Inhibitors)) OR ((Nivolumab) OR (Pembrolizumab) OR (Camrelizumab) OR (Ipilimumab) OR (Avelumab) OR (Atezolizumab) OR (Daratumumab) OR (Durvalumab) OR (SHR-1210) OR (Cemiplimab) OR (Toripalimab) OR (Camrelizumab) OR (Sintilimab))OR ((PD-1) OR (PD-L1) OR (CTLA-4)) AND ((Liver Transplantation) OR (Liver Transplant) OR (LT)) AND (Cancer) OR (Neoplasm) OR (Carcinoma) OR (Malignance)’ and the screening process was listed in Figure 1.

The screening process of the literature analysis.
The conduct of our study was approved by the Ethical Affairs Committee of the Affiliated Hospital of Qingdao University (the ethics approval number: QYFYWZLL 26944).
Inclusion and exclusion criteria
Inclusion criteria of this study were (1) detailed reports on the specific process and follow-up results of ICI treatments for recipients after LT, including patient gender, age, tumor type, ICI type and usage, immunosuppressive regimen, rejection, tumor response, treatment effect, and prognosis and (2) articles on ICI application to treat LT patients with new or recurring malignant tumors. The exclusion criteria of this study were articles with (1) repetitive content, (2) incomplete data and reports, and (3) patients who had graft failure before ICI treatment.
Data extraction
The data extracted from the included literature were median age, gender, malignant tumor type, ICI type, time from LT to immunotherapy, immunosuppressive regimen during ICI treatment, occurrence of graft rejection, clinical effects, and survival time.
Statistical analysis
SPSS software (24.0, IBM, Armonk, NY) was used for statistical analysis in this study. The numerical variables conforming to the normal distribution are expressed by mean ± SD (minimum ~ maximum) and analyzed by t-test; The numerical variables that do not conform to the normal distribution are represented by M (Q1, Q3) and Mann–Whitney test; The utilization rate of counting data is statistically described, and Fisher exact test is used for statistical analysis, and Kaplan–Meier method was used for survival analysis. The value p < 0.05 indicated a statistically significant difference.
Results
Based on the inclusion and exclusion criteria described above, a total of 28 articles10–37 including 27 articles in English and 1 article in Chinese that met the criteria were identified. A total of 47 patients who received ICI treatments after LT were reported in this study (Table 1).
Application of immune checkpoint inhibitors (ICIs) in patients after liver transplantation (LT).

ALD, alcoholic liver disease; Eve, everolimus; HCC, hepatocellular carcinoma; ICC, intrahepatic cholangiocarcinoma; ICI, immune checkpoint inhibitor; Ipil, ipilimumab; IS, immunosuppressive; Mel, melanoma; MMF, mycophenolate mofetil; NA, not available; Nivo, nivolumab; Pemb, pembrolizumab; Pred, prednisone; PTLD, post-transplant lymphoproliferative disease; Rap, rapamycin; Tac, tacrolimus.
Description of demographics and disease characteristics
The 28 articles that met the inclusion criteria included a total of 47 patients who received ICIs after LT, including 37 males and 10 females, with a mean age of 57 (14–71) years (Table 2). The main tumor types that occurred after transplantation were HCC recurrence (28 cases), followed by malignant melanoma (11 cases), non-small cell lung cancer (3 cases), with colorectal cancer, cholangiocarcinoma, squamous cell carcinoma, hypopharyngeal squamous cell carcinoma, and post-transplant lymphoproliferative disease (PTLD) for 1 case each.
Characteristics of LT patients and malignant tumors.
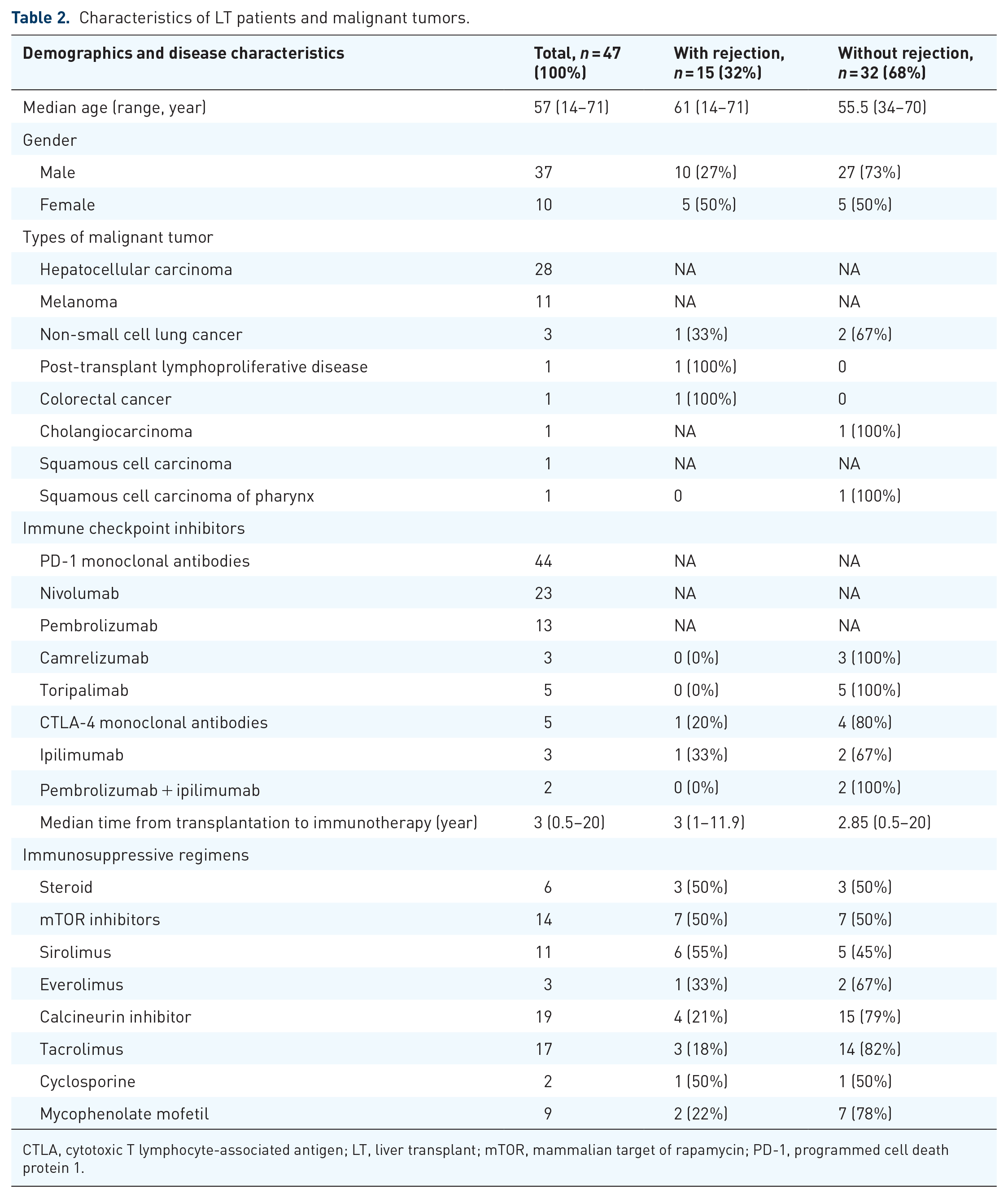
CTLA, cytotoxic T lymphocyte-associated antigen; LT, liver transplant; mTOR, mammalian target of rapamycin; PD-1, programmed cell death protein 1.
In these 47 cases, the ICIs were applied as first-line therapy after LT in only 6 cases (two studies), and was used along with other locoregional therapy or systemic therapy in the other 41 cases (Table 3).
Treatments applied before ICIs used in these 47 cases.

HCC, hepatocellular carcinoma; ICC, intrahepatic cholangiocarcinoma; ICI, immune checkpoint inhibitor; Mel, melanoma; NA, not available; PTLD, post-transplant lymphoproliferative disease.
The immunotherapy regimens used included 42 cases of programmed cell death protein 1 (PD-1) monoclonal antibodies alone (23 cases of nivolumab, 11 cases of pembrolizumab, 5 cases of toripalimab, and 3 cases of camrelizumab), 3 cases of cytotoxic T lymphocyte-associated antigen (CTLA-4) monoclonal antibodies (ipilimumab) alone, and 2 cases of combined regimen (pembrolizumab plus ipilimumab).
Among the 47 patients, immunosuppressive regimen included steroids in 6 cases, mammalian target of rapamycin (mTOR) inhibitors in 14 cases (sirolimus in 11 cases, everolimus in 3 cases), calcineurin inhibitors in 19 cases (tacrolimus in 17 cases, cyclosporine in 2 cases) and mycophenolate mofetil in 9 cases.
The follow-up time of 47 patients was 37.9 (20.5~84.7) months, and the median interval from transplantation to ICIs was 3 (0.5~20) years; The median survival time after treatment was 6.5 (0.3~48) months; The overall remission rate of malignant tumors after LT treated with ICIs was 29.8% (14/47), and the case fatality rate was 61.7% (29/47).
Evaluation of safety and treatment effectiveness of ICIs
Among the 47 patients who were treated with ICIs after LT, 15 patients (31.9%) had graft rejection, and 29 patients (61.7%) died of organ failure(37.9%, 11/29) and primary disease progression (62.1%, 18/29) as shown in (Table 4). Of the 42 LT patients treated with PD-1 monoclonal antibodies, 14 (32%) had rejection, and the median survival time of these patients was 8 (0.3–24) months. Among them, the probability of rejection in the patients treated with nivolumab, pembrolizumab, camrelizumab, and toripalimab was 35% (8/23), 54% (6/11), 0%, and 0%, respectively. Rejection occurred in one (33.3%) of three LT patients treated with CTLA-4 monoclonal antibodies, and the median survival time of these patients was 4 (3–48) months. Two patients with malignant tumors after LT and with the combination therapy of pembrolizumab plus ipilimumab did not experience rejection, and the median survival time of the patients was 16.5 (9–24) months.
Immune checkpoint inhibitors (ICIs) and treatment response.

CTLA, cytotoxic T lymphocyte-associated antigen; PD-1, programmed cell death protein 1; PD-L1, programmed death-ligand 1.
Disease remission included complete remission and partial remission.
The patients with malignant tumors after LT were treated with ICIs and had a disease remission rate of 29.8% (14/47), a disease progression rate of 68.1% (32/47), and mortality was 61.7% (29/47). Among them, the remission rates of treatment with nivolumab, pembrolizumab, camrelizumab, and toripalimab were 13% (3/23), 45.5% (5/11), 0%, and 60% (3/5), respectively. In addition, the disease progression cases of the four drug treatments were 86.9% (20/23), 36.4% (4/11), 100% (3/3), and 40% (2/5), and the mortality rates of these four ICI treatments were 86.9% (20/23), 36.4% (4/11), 100% (3/3), and 0%. Among the patients with CTLA-4 monoclonal antibodies, the disease remission rate was 66.7% (2/3), the disease progression rate was 66.7% (2/3), and the mortality rate was 66.7% (2/3). Among the patients treated with the combination therapy of pembrolizumab plus ipilimumab, the remission rate was 50% (1/2); the disease progression rate was 50% (1/2), and mortality was 0% (0/2).
In this study, five patients with partial data missing were excluded. The probability of graft rejection in the remaining 42 patients receiving ICI therapy at 2 years, 4 years, 8 years, and 20 years after LT was 26.7% (4/15), 57.1% (8/14), 14.3% (1/7), and 16.7% (1/6), respectively, indicating that the rate of rejection in patients gradually reduced as the median time to starting immunotherapy increased (Figure 2).
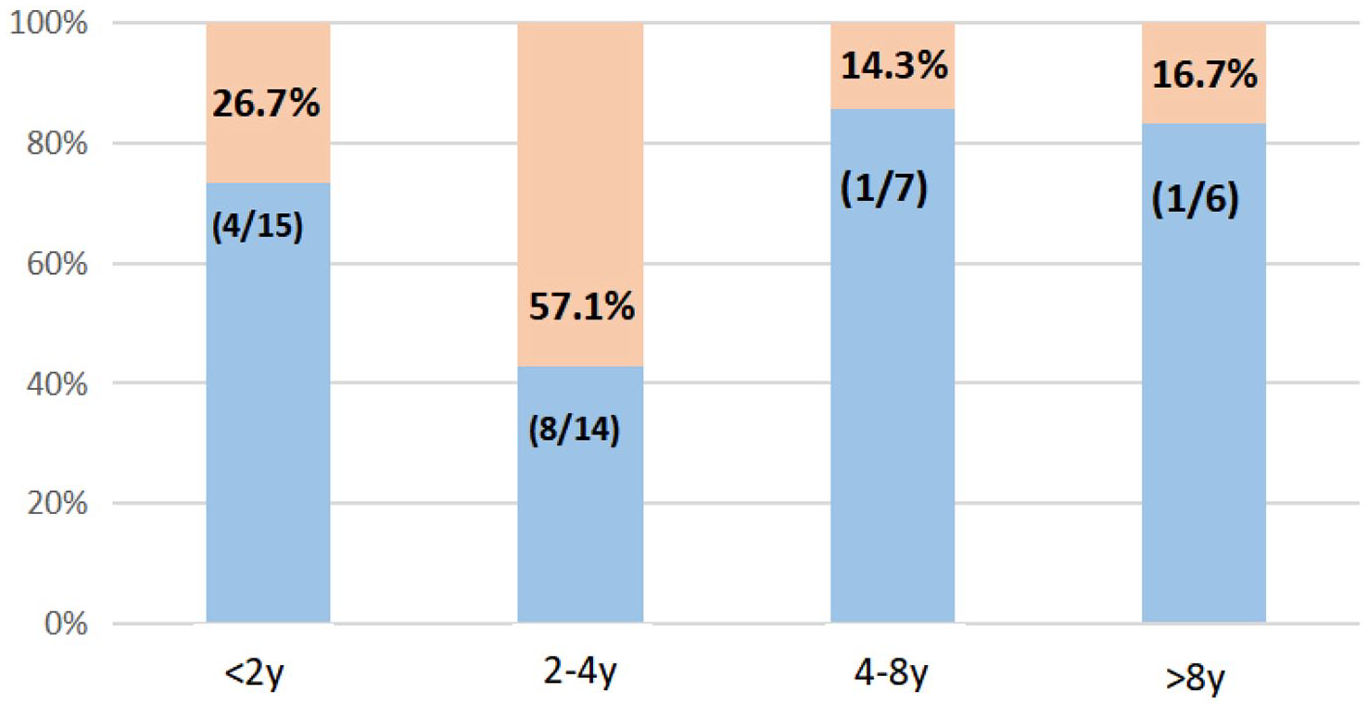
Relationship between the rate of graft rejection and the time to start immunotherapy.
Impact of immunosuppressive therapy on the safety and effectiveness of ICI treatments
Except for some literatures that failed to provide immunosuppressive regimen, a total of 31 patients with immunosuppressive regimens were included for analysis (Table 5). During ICI treatment, the graft rejection rate in patients receiving steroid monotherapy was 100% (2/2) and both of them died of disease progression; the rejection rate of rapamycin (mTOR) inhibitor and sirolimus monotherapy was 60% (3/5), one case had remission, and three cases died of disease progression finally. Among the 10 patients treated with tacrolimus alone, 1 case had rejection, 2 cases had remission, 7 cases died of disease progression, and the only patient treated with cyclosporine alone also had rejection and finally died. For the combined immunosuppressive regimen, of the 10 recipients treated with two immunosuppressive agents, 4 had rejection, 4 had remission, and a total of 7 died. Two patients who were treated with three drugs did not have rejection, but eventually died of disease progression. One patient who was treated with four drugs had remission.
Immunosuppressive regimen, graft rejection, and tumor response.

Survival curve analysis of patients with ICI treatments
Among the 47 cases in this study, 29 cases (61.7%) died, including 15 cases of rejection and 11 cases (73.3%); no rejection occurred in 32 cases and 18 cases died (56.3%). Except for 16 cases with partial missing data, the survival curve of the remaining 31 cases was analyzed. The results showed that the overall survival time of those without rejection (21 cases) was 5.5 months, which was higher than that of those with rejection (10 cases). The difference was statistically significant (p = 0.002, Log Rank = 9.164, Figure 3).

Relationship between graft rejection and patient survival time.
Discussion
Graft rejection and ICIs after transplantation
In this study, we conducted the latest and largest case report of ICI treatments in patients with tumors after LT. The results showed that among the 47 patients treated with ICIs, 31.9% of patients had graft rejection and the median survival time was 6.5 (0.3–48) months. In malignant melanoma, ICI-associated transplant rejections were mostly reported in LT recipients, and the mortality of liver transplant recipients was more than 36.5%. 38 Rejection was often accompanied by high mortality, and 44% of all patients died of graft failure. Abdel-Wahab et al. 26 analyzed 39 organ transplant recipients, including LT. About 41% of the recipients had graft rejection after ICI treatment, of which 81% had graft loss and 46% died. Kumar et al. 39 analyzed the clinical data of 64 organ transplant patients including 37 cases of melanoma, 10 cases of HCC, 7 cases of lung cancer, and 10 cases of other tumors, which showed that overall allograft rejection rate was 40.6% (26/64 cases) in organ transplant recipients following ICI therapy. The graft rejection rate was 44% (17/39 cases) for renal, 31.6% (6/19 cases) for liver, and 20% (1/5 cases) for cardiac allografts. Among LT recipients, the rejection rate of patients treated with nivolumab was the highest (33%, 3/9 cases), the second was pembrolizumab treatment (20%, 2/5 cases), while the lowest incidence was ipilimumab treatment (12.5%, 1/8 cases). These results indicated that after LT, patients with tumors that were treated with ICIs had a higher rate of graft rejection, and their overall prognosis was limited.
The mechanism of graft immune rejection is similar to tumor immune rejection. The response rate of tumors to PD-1 inhibitors is higher than that of CTLA-4 inhibitors. 40 In addition, the positive expression of PD-1 and programmed death-ligand 1 (PD-L1) proteins in some graft biopsies also suggests that the PD-1 pathway may be involved in the pathogenesis of transplant tolerance and immune rejection. 38 Therefore, the rate of graft rejection may be higher when using PD-1/L1 pathway blockers. In the prospective, single-arm study of Shi et al. 37 all the five patients without PD-L1 expression in their grafts received anti-PD1 therapy without developing graft-related immune-related adverse events. Besides, one off study patient with positive graft PD-L1 expression suffered graft rejection. The prospective, single-arm research showed that graft PD-L1 expression may be a promising marker for transplant recipients’ organ rejection following anti-PD1 immunotherapy, although needed to be further investigated in patients with solid organ transplantation.
Safety of ICI treatments in LT
In comparing the safety of different ICI treatment regimens, studies have shown that the rejection rate of patients receiving CTLA-4 inhibitors is lower than that of patients receiving PD-1 inhibitors. The rejection rates of CTLA-4 inhibitors and PD-1 inhibitors were 11% and 30%, respectively. 19 Other studies have shown that CTLA-4 helps induce but fails to maintain transplant tolerance. Organ transplant patients receiving CTLA-4 inhibitor treatment may have relatively low graft rejection in the early stages after transplantation.41,42 The data from this study showed that the risk of rejection of pembrolizumab and nivolumab was higher than that of other ICIs. The rejection rate of CTLA-4 monoclonal antibodies was lower than that of PD-1 monoclonal antibodies. The median survival time of patients with CTLA-4 monoclonal-antibody therapy was longer than those with PD-1 monoclonal-antibody therapy, which was consistent with the findings in another study. 39 Thus, CTLA-4 monoclonal-antibody therapy may be superior to PD-1 monoclonal-antibody therapy in terms of safety in LT recipients. Another study has shown that CTLA-4 monoclonal antibodies are the first-line drugs for the treatment of melanoma in organ transplant recipients and is safer and more desirable than PD-1 monoclonal antibodies. 43 In addition, this study showed that two patients treated with a combined regimen (pembrolizumab plus ipilimumab) did not experience rejection. A recent study reported that a liver LT patient was treated with atezolizumab and bevacizumab without any signs of rejection, suggesting a new breakthrough standard treatment option for HCC. 44 However, because the number of patients receiving the combined regimen was small, the authors could not conclude that the combined regimen was safer than the others.
Effectiveness of ICI treatments in LT
In the evaluation of the effectiveness of ICI treatments, the results of Kumar et al. showed that the disease remission rate of patients treated with nivolumab or pembrolizumab was 26% and 53%, respectively. The disease remission rate of ipilimumab was 20%. 39 In this study, the disease remission rates of patients treated with PD-1 monoclonal antibodies and CTLA-4 monoclonal antibodies were 32% and 67%, the disease progression rates were 73% and 67%, and mortality rates were 66% and 67%, respectively. However, due to the small sample size and the retrospective design of this study, it is impossible to infer which ICIs are more effective. A large sample, prospective study is needed for further clarification.
This study showed that the time interval between immunotherapy and LT was a potential factor affecting the risk of graft rejection. The longer the time interval between immunotherapy and LT, the lower the risk of graft rejection after ICI treatment, which was consistent with the viewpoint of Qiu et al. 19 In contrast, if ICIs are used too early following LT, the risk of transplant rejection may be increased. However, delay in the start of immunotherapy may result in a significant reduction in the effectiveness of ICIs. Therefore, in patients who have received LT and are considered for ICI treatment, close follow-up is recommended during first-line conventional treatment to identify signs of disease progression as early as possible and to carefully weigh the start time of immunotherapy. 45
Immunosuppressants in ICI treatments after LT
Drugs used for immunosuppression after LT include four categories: major steroids, mTOR inhibitors (sirolimus, everolimus), calcineurin inhibitors (tacrolimus, cyclosporine), and mycophenolate mofetil. Since different immunosuppressants work at different stages of the cell cycle, they are often used in combination to achieve optimal results. This study showed that during ICI treatment, patients receiving different immunosuppressive regimens had different rates of graft rejection. Patients treated with steroids had a higher rate of rejection than patients treated with other immunosuppressive regimens. Patients treated with calcineurin inhibitors had a lower probability of rejection, which was consistent with the results of the study of Abdel-Wahab et al. 26 In this study, among the LT patients treated with ICIs, three out of five patients (60%) who were treated with sirolimus alone (single-agent immunosuppressive therapy) had graft rejection, and one out of nine patients (11%) who were treated with tacrolimus had graft rejection. Existing data suggest that patients using tacrolimus may have a relatively low risk of rejection. However, due to the limited data in this study, we cannot definitively infer which immunosuppressive regimens interfere less with immunotherapy. Further verification is needed via future clinical trials.
Although there is concern that immunosuppressive therapy may alter the effectiveness of ICI treatment, clinical studies have shown that LT patients treated with ICIs and immunosuppressive therapy simultaneously responded to immunotherapy. 19 This study showed that patients receiving steroid and tacrolimus treatments had a disease remission rate of 25% and 23%, respectively. The disease remission rate of the patients on a combined immunosuppressive regimen was 44%. These results indicated that a combined immunosuppressive regimen for the initiation of ICI treatment may be more conducive to disease response than single-agent immunosuppression.
The survival analysis results showed that the median overall survival of patients with graft rejection was significantly lower than that of the patients without graft rejection. Among the 25 LT patients treated with ICIs, 64% of the patients died during the follow-up period. The main cause of death was graft rejection or the progression of primary malignant tumors. Among them, four patients (16%) died of transplant organ failure caused by rejection. Therefore, for patients after LT, the occurrence of graft rejection significantly affected overall survival.
By blocking the inhibitory receptors of immune checkpoints, ICIs restore antigen initiation, proliferation, T cell migration and effector function, and stimulate the host immune response. However, initiation of immunity to tumor cells may also lead to fatal transplant rejection. 39 Thus, for patients with LT who have recurrent, refractory, and metastatic malignancies under long-term immunosuppression, immunotherapy with ICIs may be effective. Nevertheless, the risk of graft rejection that may result from this should not be ignored. Thus, we believe that for patients with recurrence or new malignant tumors after LT, the indications for ICI treatment should be carefully considered.
Limitations
The data in this retrospective study were from published case reports that did not represent most of the population but were used to infer the overall situation. Besides, the potential selection and reporting bias might affect the conclusion of this study.
Conclusion
The pooled analysis of 47 recipients in the application of ICIs after LT published in literature showed that the overall remission rate following ICI treatment was 29.8% and the disease progression rate was 68.1%. Among all patients, 31.9% of patients had immune rejection; the case fatality rate was 61.7%, which showed the experience of ICI therapy in LT was still limited and far from rosy.
To further improve the therapeutic effects of ICIs in LT patients, there are still lots of work to be done in the future, including but not limited to preferential selection of recipient and immunosuppressants, careful consideration of risk–benefit in ICIs therapy, combination therapies or monotherapy of ICIs regimen, identifying best predictive biomarkers of response or graft rejection, and more molecular mechanisms or prospective studies are needed to explore the complex interactions between the immune system, tumor antigens, and transplant antigens.
Footnotes
Acknowledgements
The authors thank all the staff working in the Division of Hepatology, Liver Disease Center, Department of Organ Transplantation, the Affiliated Hospital of Qingdao University.
Author contributions
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the Affiliated Hospital of Qingdao University (No. QYFYWZLL 26944).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.