
Abstract
Objectives:
Sodium-glucose cotransporter-2 (SGLT2) inhibitors have been found to reduce serum urate in patients with type 2 diabetes mellitus. To evaluate if this effect applies to both patients with and without diabetes, we conducted a systematic review and meta-analysis of SGLT2 inhibitors on serum urate levels in this population.
Methods:
Four electronic databases (PubMed, Embase, Cochrane and SCOPUS) were searched on 25 September 2021 for articles published from 1 January 2000 up to 25 September 2021, for studies that examined the effect of SGLT2 inhibitors on serum urate in study subjects. Random-effects meta-analysis was performed, with subgroup analyses on the type of SGLT2 inhibitor agent administered, presence of type 2 diabetes mellitus, presence of chronic kidney disease and drug dose.
Results:
A total of 43 randomized controlled trials, with a combined cohort of 31,921 patients, were included. Both patients with [−31.48 μmol/L; 95% confidence interval (CI): −37.35 to −25.60] and without diabetes (−91.38 μmol/L; 95% CI: −126.53 to −56.24) on SGLT2 inhibitors had significantly lower urate levels when compared with placebo. This treatment effect was similarly observed across different types of SGLT2 inhibitors. However, in type 2 diabetes mellitus (T2DM) patients with chronic kidney disease, the reduction in serum urate with SGLT2 inhibitors became insignificant (95% CI: −22.17 to 5.94, p < 0.01).
Conclusion:
This study demonstrated that SGLT2 inhibitors are beneficial in reducing serum urate in patients with and without diabetes. SGLT2 inhibitors could therefore contribute to the general treatment of hyperuricaemia.
Keywords
Introduction
Sodium-glucose cotransporter-2 (SGLT2) inhibitors are an emerging class of glucose-lowering medications that decrease plasma glucose levels in an insulin-independent manner. 1 By blocking SGLT2 receptors located in the early proximal renal tubule, the renal reabsorption of glucose is limited to approximately 80 g/day, 2 thus lowering the glucose burden.
Beyond glycaemic control, 3 SGLT2 inhibitors have also been found to have beneficial effects on blood pressure, 4 body weight, 5 cardiometabolic markers, 6 cardiovascular outcomes 7 and renal function. 8 Several mechanisms of how SGLT2 inhibitors exert their cardiorenal-protective effects have been proposed, one of them being a reduction in the levels of serum urate. 9
An elevated level of urate is an independent predictor of diabetes and often precedes the development of diabetes.10,11 High levels of urate have been found to inhibit post-receptor insulin signalling pathways, thus inducing insulin resistance.12,13 Raised serum urate levels have also been implicated in gout and are also associated with other common comorbidities such as hypertension, metabolic syndrome, nonalcoholic fatty liver disease, and chronic kidney disease. 14 Previous studies on urate-lowering therapy demonstrated benefits such as an improvement in kidney function,15,16 prophylaxis of gout flares17,18 and a reduction in the risk of major adverse cardiovascular events and all-cause mortality. 19 Given the increasing amount of evidence implicating the contributory causal role of urate in the pathogenesis of cardiovascular and renal diseases, 20 it is thus crucial to study the impact of SGLT2 inhibitors in reducing serum urate levels.
In previous meta-analyses, SGLT2 inhibitors demonstrated an effect in reducing serum urate levels in patients with type 2 diabetes mellitus (T2DM).21–23 To the best of our knowledge, there has not been any meta-analysis examining whether this effect applies to patients without diabetes as well. We hypothesized that SGLT2 inhibitors would reduce serum urate levels in both patients with and without diabetes. Therefore, we conducted a systematic review and meta-analysis of SGLT2 inhibitors on serum urate levels in this population.
Methods
Search strategy
This meta-analysis was performed according to the 2020 Preferred Reporting Items of Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 24 Ethical approval was not required for this study as this study utilized publicly available data that were already previously published. Four electronic databases (PubMed, Embase, Cochrane and SCOPUS) were searched on 25 September 2021 for articles published from 1 January 2000 up to 25 September 2021, for studies that examined the effect of SGLT2 inhibitors on serum urate in study subjects. A combination of the following terms was used for the literature search: (‘empagliflozin’ OR ‘canagliflozin’ OR ‘dapagliflozin’ OR ‘ertugliflozin’ OR ‘luseogliflozin’ OR ‘ipragliflozin’ OR ‘remogliflozin’). The detailed search strategy is shown in Supplemental Table 1. A manual search of ClinicalTrials.gov, the retrieved references, relevant meta-analyses and reviews was carried out to identify additional trials.
Study selection
All randomized controlled trials comparing the effects of SGLT2 inhibitors against placebo on serum urate were included, according to the Population, Intervention, Comparison, Outcome, and Study (PICOS) framework (Table 1). We excluded all studies that were not randomized controlled trials.
PICOS, inclusion criteria and exclusion criteria applied to database search.

PICOS: Population, Intervention, Comparison, Outcome, and Study design; SGLT2, sodium-glucose cotransporter.
Data extraction and quality assessment
Four independent reviewers evaluated the literature and extracted study data including participant baseline characteristics, study design, date of publication and sample size. Discrepancies were resolved by mutual consensus. Based on the title and abstract sieve, studies that were not randomized controlled trials or did not involve the use of SGLT2 inhibitors were first excluded. A full-text review was subsequently performed to assess for inclusion and exclusion criteria in detail.
Full-text articles and their respective supplementary materials from included publications were then retrieved for data extraction. The following baseline information of patients from eligible trials was collected: age, sex, body weight, body mass index (BMI), systolic blood pressure, diastolic blood pressure, haemoglobin A1c (HbA1c) and low-density lipoprotein cholesterol (LDL-C). Data of the SGLT2 inhibitor regimens were collected, namely drug name, drug dosage, drug frequency, control group, length of intervention and mean duration of follow-up and outcome (change in serum urate levels from baseline). For serum urate levels, a conversion factor of 1 mg/dl to 59.48 μmol/L was adopted. All repeated observations for participants were extracted. The quality of the included studies was evaluated using the Cochrane Risk of Bias tool, which comprises seven domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome, incomplete outcome data, selective reporting and other sources of bias, as shown in Supplemental Figure 1. The quality of pooled evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system, 25 which considered statistical heterogeneity, publication bias, risk of bias, indirectness and statistical imprecision, as shown in Supplemental Table 2. Consensus was reached among the four independent reviewers when assessing for risk of bias. The 2020 PRISMA checklist and Meta-analyses Of Observational Studies in Epidemiology (MOOSE) checklist are attached in Supplemental Figures 3 and 4, respectively.
Statistical analysis
In studies without standard deviations, p-values and confidence intervals, the square root of weighted mean variance of all other studies was used to estimate the standard deviation. The heterogeneity between studies was examined using I2 and τ 2 statistics. Heterogeneity was considered as significant for I2 >50%. 26 Random-effects meta-regression analysis with the inverse-variance method was performed within each SGLT2 inhibitor to assess the association between drug dosage and the reduction of serum urate. 27 Additional subgroup analyses were carried out to explore the association between effect size and baseline characteristics, namely: the SGLT2 inhibitor agent administered, presence of T2DM, presence of chronic kidney disease and drug dose. Two-tailed p-values <0.05 were considered statistically significant. All results were analysed using Review Manager (RevMan) Version 5.4 and Stata 16.0 (StataCorp, TX, USA).28,29
Results
Study selection and characteristics
The PRISMA flowchart is illustrated in Figure 1. A systematic literature search identified 8648 articles. Four additional articles were identified from hand search. A total of 3062 duplicate articles were excluded. Title and abstract screening further excluded 5029 nonrelevant articles which did not assess serum urate as an outcome. Full-text screening excluded 536 articles. In total, 43 randomized controlled trials (published from 2010 to 2021) were included for the meta-analysis. The sample size of the studies ranged from 20 to 7034, giving a total of 31,921 participants.
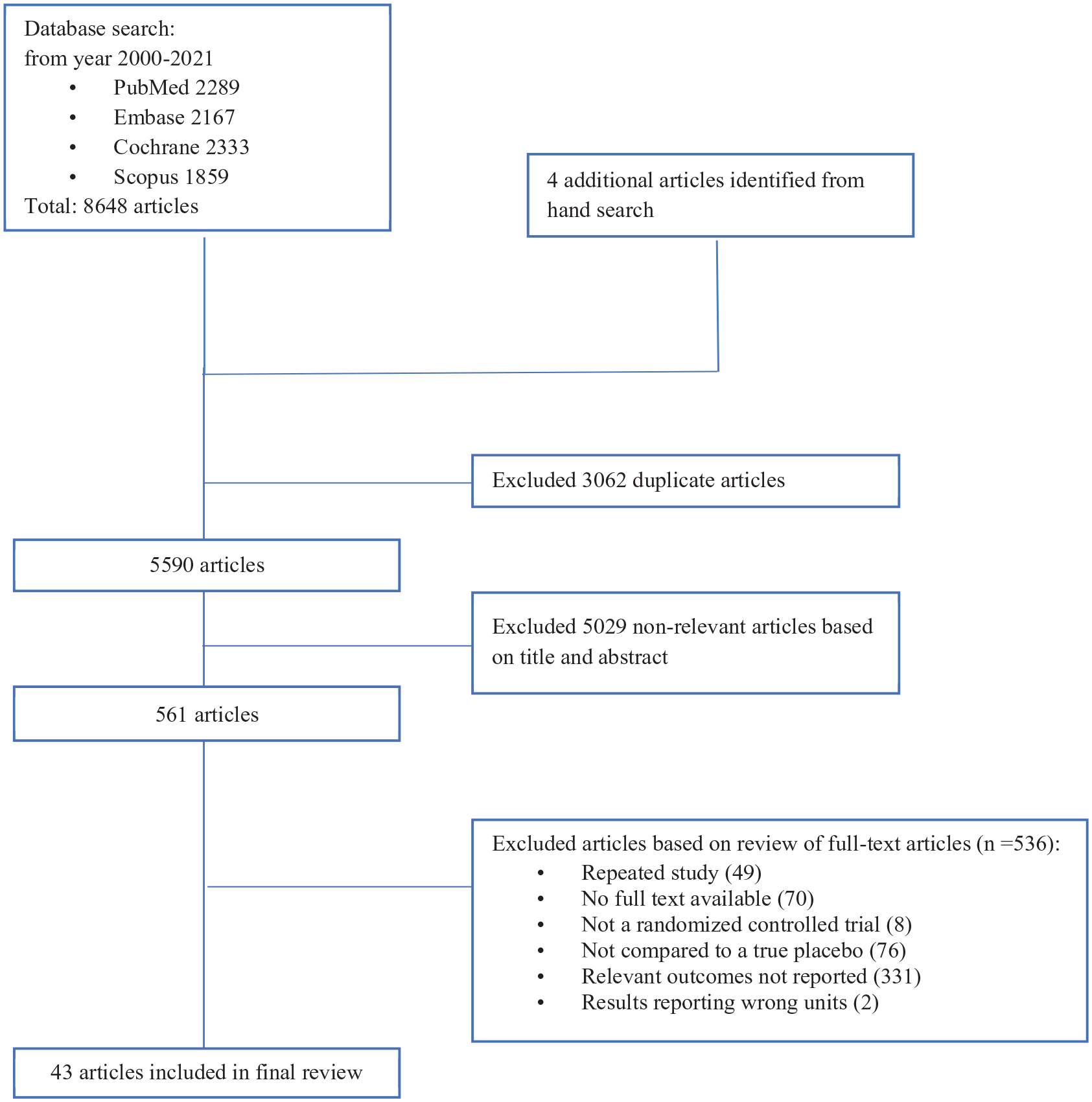
PRISMA flowchart.
The baseline characteristics of participants are compiled in Table 2. Out of the 43 randomized controlled trials, 39 trials included patients with T2DM, and none of the trials included patients with type 1 diabetes mellitus. Among the remaining four trials, healthy subjects were recruited in Chino et al. 30 and Zanchi et al., 31 while subjects with prediabetes were recruited in Lee et al. 32 and Ramírez-Rodríguez et al. 33
Baseline characteristics of subjects.

ACEi, angiotensin-converting enzyme inhibitors; AMI, acute myocardial infarction; ARB, angiotensin II receptor blocker; CAD, coronary artery disease; CKD, chronic kidney disease; DM, diabetes mellitus; DPP-4, dipeptidyl peptidase-4; GLP-1, glucagon-like peptide-1; HbA1c, haemoglobin A1c; LDL-C, low-density lipoprotein cholesterol; NR, not reported; T2DM, type 2 diabetes mellitus.
Combination therapy of antihyperglycaemic agents include metformin, sulphonylurea, DPP-4 inhibitor, α-glucosidase inhibitor, GLP-1 agonist, insulin and pioglitazone.
The SGLT2 inhibitor drug name, dose, frequency, length of intervention and length of follow-up are summarized in Supplemental Table 3. Empagliflozin, Dapagliflozin, Canagliflozin, Luseogliflozin and Ipragliflozin were administered in 14, 13, 7, 3 and 2 trials, respectively. All trials had a once-daily dosing regimen except Rosenstock et al., 36 Qiu et al. 47 and Schumm-Draeger et al., 49 which have a twice-daily regimen. The length of follow-up ranged from 1 week to 3.1 years.
Pooled outcome analyses
The pooled urate outcomes are presented in Figure 2. Overall, SGLT2 inhibitors reduced serum urate by 33.03 μmol/L (95% CI: −37.38 to −28.69, p < 0.001).
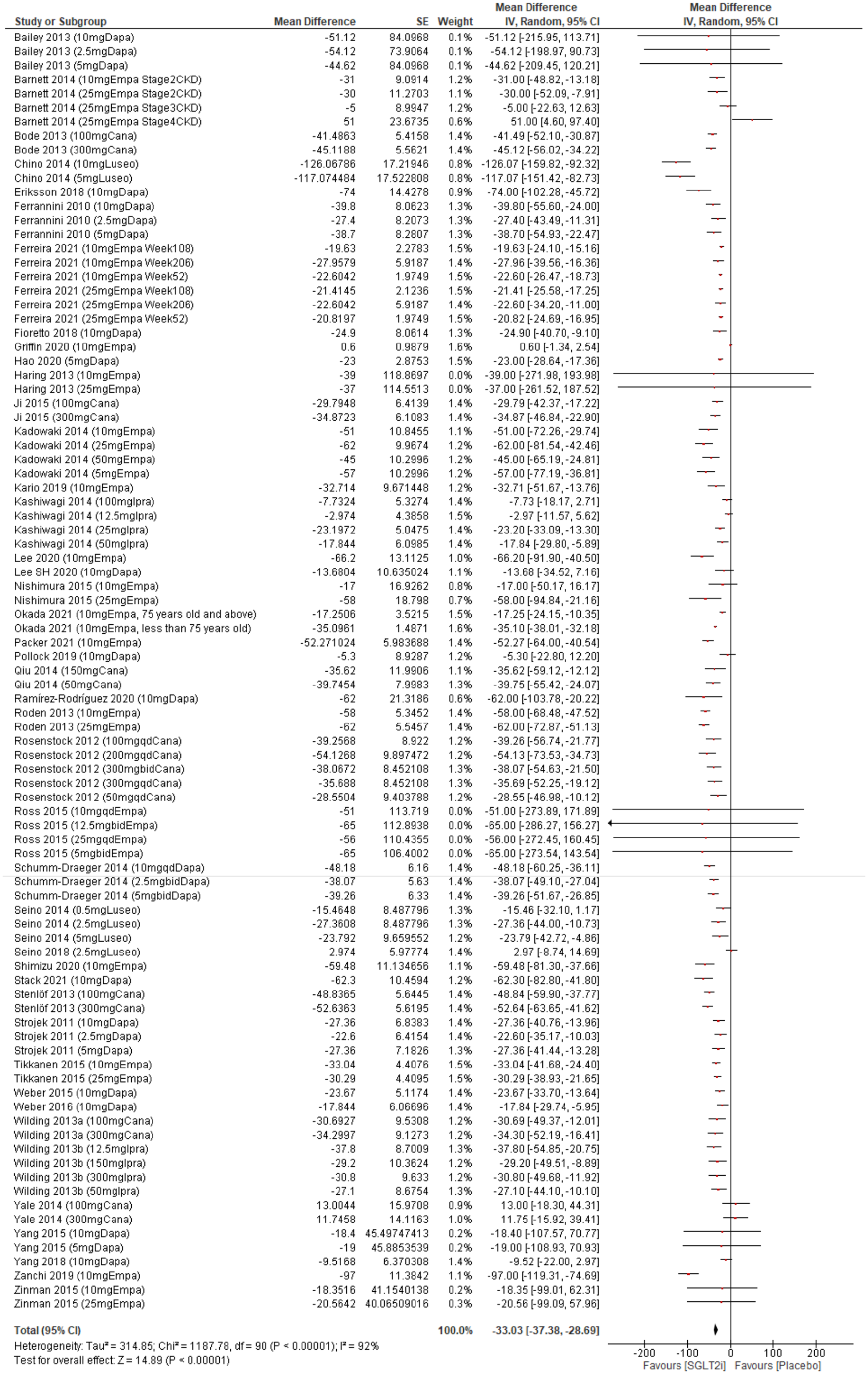
Forest plot of mean change in serum urate in μmol/L.
Subgroup analyses
Subgroup analyses were carried out to explore the association between effect size and baseline characteristics, focusing on the type of SGLT2 inhibitor administered, presence of T2DM, presence of chronic kidney disease and the drug dose.
SGLT2 inhibitor administered
Significant reduction of urate level was associated with each of the five SGLT2 inhibitors administered (canagliflozin, dapagliflozin, empagliflozin, ipragliflozin and luseogliflozin). The random effects model demonstrated that luseogliflozin had the greatest mean reduction in urate of 47.73 μmol/L (95% CI: −79.50 to −15.96, p = 0.003) (Figure 3(a)). This was followed by canagliflozin, which had a mean reduction in urate of 36.62 μmol/L (95% CI: −42.67 to −30.56, p < 0.001) (Figure 3(b)). Empagliflozin led to a mean reduction in urate of 35.19 μmol/L (95% CI: −42.61 to −27.78, p < 0.001) (Figure 3(c)), while dapagliflozin had a mean reduction in urate of 30.32 μmol/L (95% CI: −36.20 to −24.43, p < 0.001) (Figure 3(d)), and ipragliflozin had a mean reduction in urate of 20.37 μmol/L (95% CI: −29.17 to −11.56, p < 0.001) (Figure 3(e)).

(a) Meta-analysis of mean difference and 95% CI for changes in serum urate in μmol/L with administration of (a) luseogliflozin, (b) canagliflozin, (c) empagliflozin, (d) dapagliflozin and (e) ipragliflozin.
Presence of T2DM
The results demonstrated that patients without T2DM receiving SGLT2 inhibitors had a mean reduction in urate of 91.38 μmol/L (95% CI: −126.53 to −56.24, p < 0.001) (Figure 4(a)). Patients with T2DM receiving SGLT2 inhibitors had a smaller mean reduction in urate of 31.48 μmol/L (95% CI: −37.35 to −25.60, p < 0.001) (Figure 4(b)).
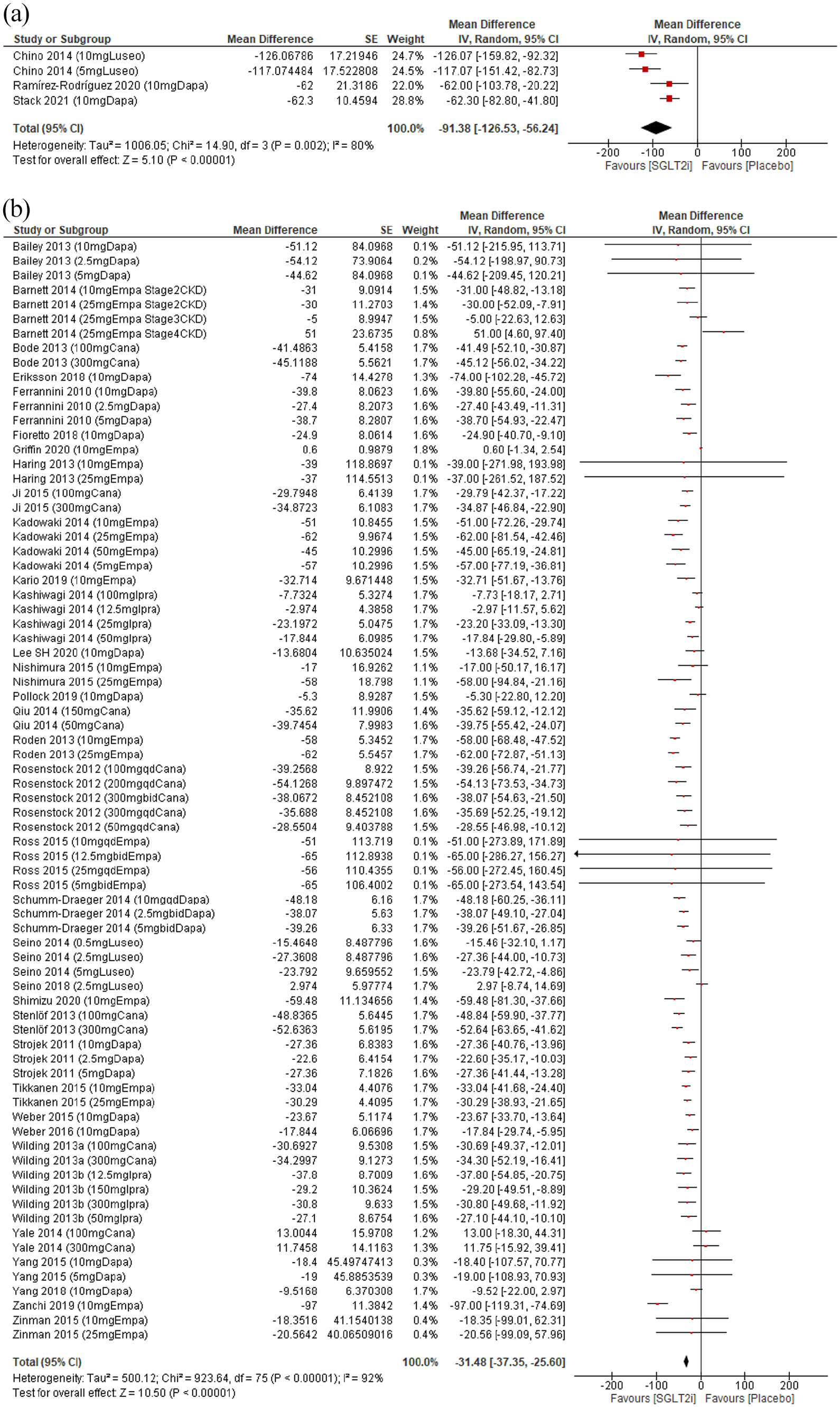
Subgroup analysis of reduction in serum urate (in μmol/L) in (a) patients without diabetes and (b) patients with diabetes.
Presence of chronic kidney disease with T2DM
Barnett et al., 44 Fioretto et al., 59 Pollock et al. 63 and Yale et al. 50 included patients with diabetes with an estimated glomerular filtration rate (eGFR) ranging from 15 to 90 ml/min/1.73 m2, 40 to 65 ml/min/1.73 m2, 25 to 75 ml/min/1.73 m2 and 30 to 50 ml/min/1.73 m2, respectively. No significant reduction in serum urate was shown in these patients (95% CI: −22.17 to 5.94, p < 0.01) (Supplemental Figure 2).
Meta-regression: drug dose of dapagliflozin, canagliflozin and empagliflozin
Random-effects meta-regression was performed to evaluate whether reduction in serum urate levels was dependent on the dosage of any specific SGLT2 inhibitor (data not shown). There was no significant association between drug dosage and serum urate-lowering capacity of dapagliflozin (beta coefficient = −0.476, 95% CI: −3.04 to 2.09, p = 0.704), canagliflozin (beta coefficient = −0.0073, 95% CI: −0.064 to 0.050, p = 0.79) and empagliflozin (beta coefficient = 0.267, 95% CI: −0.654 to 1.19, p = 0.559). We could not perform a meta-regression analysis for ipragliflozin and luseogliflozin in view of the limited number of studies.
Risk of bias of included studies
The risk of bias is summarized in Supplemental Table 4. All included studies were randomized controlled trials. Majority of the studies had a low risk of reporting bias. Three trials were assessed to have a high risk of other bias, due to the small sample size. Chino et al., 30 Griffin et al., 64 Ramírez-Rodríguez et al. 33 and Stack et al. 71 had a sample size of 24, 20, 24 and 36, respectively. One trial 30 had a high selection bias due to allocation concealment.
Discussion
This updated, pair-wise meta-analysis of 43 randomized controlled trials demonstrated that SGLT2 inhibitors had a beneficial effect on serum urate levels. This effect remained significant when stratified across the SGLT2 inhibitor agent administered, and the presence of T2DM. In patients without diabetes mellitus, there was a larger reduction in serum urate. No dose-dependent relationship was observed for dapagliflozin, canagliflozin and empagliflozin.
These findings largely concur with previous meta-analyses which quantify the serum urate-lowering properties of SGLT2 inhibitors in patients with T2DM.21–23 In the study by Hu et al., luseogliflozin was also found to have the greatest effect on reduction of serum urate levels in patients with T2DM, where a dose of 10 mg was shown to be the most efficacious when compared with lower doses. 23 This is in contrast to our study, as well as Xin et al. 21 and Chino et al., 30 which did not find any significant dose-dependent difference in the urate-lowering effects of SGLT2 inhibitors.21,22 In addition, while there might be differences in the urate-lowering effect between different agents, this may not be clinically significant.
SGLT2 inhibitors lower serum urate by increasing the renal elimination of urate.30,72 Urate is freely filtered by the kidney and most of it is reabsorbed in the S1 segment of the proximal convoluted tubule (PCT).73,74 As such, the mechanism for the uricosuric properties of SGLT2 inhibitors has been attributed to the suppression of GLUT9 isoform 2 activity. GLUT9 isoform 2 is a facilitative hexose/urate transporter GLUT9 isoform 2 (SLC2A9b) found on the apical membrane of epithelial cells in the S1 segment of the PCT, involved in the excretion of urate. 9 Therefore, when SGLT2 is inhibited, the increased concentration of glucose within the lumen of the PCT competes with urate for GLUT9 isoform 2. 30 In addition to being found in the PCT, GLUT9 isoform 2 is also found in the collecting ducts, where it mediates urate reabsorption. 75 It has been found that an increased concentration of glucose in the lumen by SGLT2 inhibition also inhibits urate reabsorption mediated by GLUT9 isoform 2 found in the collecting ducts. 30 This uricosuric effect is also seen with phloridzin, a non-selective SGLT inhibitor, which induces uricosuria in healthy subjects. 76
It was previously reported that urate reduction by SGLT2 inhibitors declined or became absent in patients with chronic kidney disease, where the reduction in both urate and glucose filtration might mask the contribution of decreased urate reabsorption as a result of SGLT2 inhibition. 22 In our analysis, comparing the effect of SGLT2 inhibitors against placebo, we demonstrated a larger mean reduction in serum urate levels in the subgroup of patients without diabetes, compared with the subgroup of patients with diabetes. An analysis of a subgroup of patients with both chronic kidney disease and T2DM also revealed an attenuated effect of SGLT2 inhibitors in terms of reducing serum urate levels. As such, it seems that the urate-lowering effect of SGLT2 inhibitors is dependent on renal function. Given that the progression of T2DM in patients with diabetes affects renal filtration function, 77 this could contribute to the decreased effect of SGLT2 inhibitors on urate reduction in patients with diabetes. Even then, the reduction in serum urate levels in the diabetic population was still significant.
However, it is also important to note that at this current time, urate-lowering therapy is not indicated for asymptomatic hyperuricaemia in patients with chronic kidney disease 78 and for the prevention of gouty arthritis.79,80 While lowering serum urate levels may have benefits, this effect has been difficult to characterize. Nevertheless, lowering serum urate has not been shown to be harmful. 19 Given the strong association between urate levels and many other comorbidities, 14 the urate-lowering properties of SGLT2 inhibitors should be viewed as an additional benefit in the management of the overall morbidity in patients with diabetes.
Strengths and limitations
To the best of our knowledge, this is the first and largest meta-analysis investigating the effects of SGLT2 inhibitors on serum urate in patients with and without diabetes. However, our study should be interpreted in light of its limitations. First, serum urate level was reported as the primary endpoint in only two of the included studies,22,30 of which Chino 2014 was a small study with a 1-week study period. Otherwise, there was no clear inclusion or exclusion criteria specific for baseline serum urate levels and no specified methodology for the urate assay as well. We also recognize the lack of information on the presence of other urate-modifying therapies. Should there be unreported concomitant use of urate-lowering therapies, the true effect of SGLT2 inhibitors on uric acid could be overestimated. Second, due to limited studies available, we were unable to comment on the urate-lowering effect of individual SGLT2 inhibitors in the nondiabetic population. It is also to be noted that these are small studies, thus these results should be re-evaluated in clinical trials on a larger scale. Third, heterogeneity of the studies present was likely attributed to the difference in baseline characteristics of the study population.
Conclusion
Our study demonstrated that SGLT2 inhibitors significantly reduced serum urate levels in patients with and without diabetes, compared with placebo. With the clinical importance of hyperuricaemia and associated comorbidities such as gout and chronic kidney disease, SGLT2 inhibitors might prove to be beneficial in the treatment of patients with diabetes with concomitant hyperuricaemia. Adequately powered randomized controlled trials are also required to formally interrogate the use of SGLT2 inhibitors in patients without diabetes. Future studies should also consider SGLT2 inhibitors in patients with gout, who have an absolute indication for urate-lowering therapy.
Supplemental Material
sj-docx-1-taj-10.1177_20406223221083509 – Supplemental material for Effect of sodium-glucose cotransporter-2 (SGLT2) inhibitors on serum urate levels in patients with and without diabetes: a systematic review and meta-regression of 43 randomized controlled trials
Supplemental material, sj-docx-1-taj-10.1177_20406223221083509 for Effect of sodium-glucose cotransporter-2 (SGLT2) inhibitors on serum urate levels in patients with and without diabetes: a systematic review and meta-regression of 43 randomized controlled trials by Alicia Swee Yan Yip, Shariel Leong, Yao Hao Teo, Yao Neng Teo, Nicholas L. X. Syn, Ray Meng See, Caitlin Fern Wee, Elliot Yeung Chong, Chi-Hang Lee, Mark Y. Chan, Tiong-Cheng Yeo, Raymond C. C. Wong, Ping Chai and Ching-Hui Sia in Therapeutic Advances in Chronic Disease
Footnotes
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the National University of Singapore Yong Loo Lin School of Medicine’s Junior Academic Faculty Scheme.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.