
Abstract
Immune checkpoint inhibitors (ICIs) represent an important advance in the adjuvant treatment of patients with high-risk melanoma. Although the safety profile of anti-programmed cell death protein-1 (PD-1) is fairly acceptable, different immune-related adverse events (irAEs) are described. Herein we report for the first time a notably multidisciplinary combined approach on a malignant melanoma (MM) patient treated with anti-PD-1 antibody in adjuvant setting. In this novel approach, corticosteroid-refractory immune-mediated colitis (IMC) was effectively treated with Vedolizumab, a selective blockade of the α4β7 integrin and corticosteroids were successfully administered for autoimmune neutropenia. Notably, our patient also express HLA-B*35, a potential biomarker for predicting a genetic basis of autoimmune susceptibility. Our experience offers a possible future perspective about the use of Vedolizumab together with immunotherapy in a strategic early approach for high-risk patients genotyped for HLA.
Keywords
Introduction
Immune checkpoint inhibitors (ICIs) demonstrated originally their efficacy in metastatic melanoma. Targeting the cytotoxic T lymphocyte antigen 4 (CTLA-4) and the programmed cell death receptor 1 (PD-1), they have significantly changed disease outcomes in various cancer, especially in melanoma, becoming standard care. 1 CTLA-4 is a B7/CD28 family member that interacts with activated T cells and inhibits transcription of interleukin-2 (IL-2) through downregulatory signal. Blocking CTLA-4 results in an unrestricted T-cell activation. The first Food and Drug Administration (FDA)-approved ICI in metastatic melanoma was Ipilimumab (Yervoy, Bristol Meyers Squibb, New York, NY), a human monoclonal IgG1 antibody against CTLA-4. 2 PD-1 is an inhibitor cell surface molecule that reduces cytokine production [IL-2, interferon-γ (IFN-γ), and tumor necrosis factor (TNF)], cell cycle progression and pro-survival Bcl-xL gene expression, decreasing levels of the transcription factors involved in T-cell activation. 3 Melanoma cells express PD-L1 reducing the activity of infiltrating lymphocytes. Antitumor immunity can be restored by locking the PD-1/PD-L1 interaction. 4 Recently, multiple PD-1 inhibitors (e.g. Nivolumab, Opdivo, Bristol Meyers Squibb, New York, NY and Pembrolizumab Keytruda, Merck, Kenilworth, NJ) showed encouraging therapeutic effects and moved from clinical trials to frontline therapy for metastatic melanoma due to a more tolerable side-effect profile. Immunotherapy represents a major advancement also in adjuvant setting and has significantly improved outcomes in the last years. 5 Over-activation of T lymphocytes can target the normal tissues with subsequent danger signal triggering on the systemic immunological network, causing autoimmunity; so, immunotherapy could be associated with wide variety of immune-related adverse events (irAEs), in term of severity and involvement of several body systems. 6 This aberrant autoimmune T-cell activation onset in irAEs has been so well studied over the last decades that it has become an ICI indirect efficacy indicator in term of better survival outcomes in metastatic and adjuvant setting. A retrospective analysis of 173 patients treated with anti-PD-1 for metastatic melanoma between July 2013 and January 2018 demonstrated that irAEs occurrence was independently associated with improved progression free survival (PFS) {hazard ratio [HR], 0.47 [95% confidence interval (CI), 0.26–0.86]; p = 0.016}, and correlated with better overall survival (OS) [HR, 0.39 (95% CI, 0.18–0.81); p = 0.007]. 7 A strong association between irAEs and better outcomes in terms of recurrence-free survival (RFS) and OS was also observed in patients with high-risk stage III melanoma treated with ICIs. 8 This study confirms the evidence that irAEs are indicators of greater ICI activity. In the past 5 years, clinical trials have demonstrated the potential therapeutic activity of ICIs in high-risk patients. The first randomized, double blind, phase 3 trial (EORTC 18071) has shown that Ipilimumab is associated to a prolonged RFS, distant metastasis-free survival (DMFS) and OS when administered as adjuvant.9,10 In the CheckMate 238 study, Nivolumab, used in adjuvant setting, has demonstrated superiority versus Ipilimumab: 4-year RFS was 51.7% (95% CI, 46.8–56.3) in the Nivolumab group and 41.2% (36.4–45.9) in the Ipilimumab group [HR, 0.71 (95% CI, 0.60–0.86); p = 0.0003]; 4-year OS was 77.9% (95% CI, 73.7–81.5) with Nivolumab and 76.6% (72.2–80.3) with Ipilimumab [HR, 0.87 (95% CI, 0.66–1.14); p = 0.31]. Regarding the exploratory endpoint, Nivolumab also improved DMFS over Ipilimumab in patients with stage III disease with 4-year DMFS: 59% versus 53%, (HR, 0.79; 95% CI, 0.63–0.99), respectively. 11 Similarly, in the EORTC 1325/KEYNOTE-054 trial, the adjuvant use of Pembrolizumab has been associated with a significantly longer RFS than placebo in the overall population: 3-year rate of recurrence-free survival was 63.7% versus 44.1% (HR, 0.56; 95% CI, 0.47–0.68), respectively. The impact of Pembrolizumab on RFS was similar in subgroups, in particular according to AJCC-7 and AJCC-8 staging, and to BRAF mutation status (HR, 0.51 (99% CI, 0.36–0.73) versus 0.66 (99% CI, 0.46–0.95) for V600E/Kv wild type). At an overall median follow-up of 42.3 months (interquartile range, 40.5–45.9), 3.5-year DMFS was higher in the Pembrolizumab group than in the placebo group [65.3% (95% CI, 60.9–69.5) versus 49.4% (44.8–53.8) HR, 0.60 (95% CI, 0.49–0.73); p < 0.0001]. 12 Patients with recurrence (except brain metastasis) and Eastern Cooperative Oncology Group (ECOG) performance status 0-2 were eligible to enter part two of the trial. Briefly, patients who had received placebo were treated with Pembrolizumab (200 mg every 3 weeks) (cross over group) and patients who had completed 1 year of therapy at least for 6 month were also treated with Pembrolizumab according to the same scheme (rechallenge group). About 40% of the former group experienced a benefit with Objective Response Rate (ORR) of 39%, while the second group showed less benefit and minimal activity. Moreover, PFS and ORR were similar to previous studies of immune checkpoint therapy for advanced melanoma. Median PFS for patients who underwent crossover was 8.5 months (95% CI, 5.7–15.2) and 4.1 months (95% CI, 2.6–not reached) to those who were re-exposed to anti-PD-1. 13 Grade 1 to grade 4 immune-related adverse events occurred among 30% of the crossover group and 20% of the rechallenge group. Most of these were endocrine disorders (crossover; 21%; rechallenge, 15%). 14 The estimated improvement of RFS was greater in patients with BRAF-V600E/K mutant melanoma (HR, 0.51) than in BRAF wild type (HR, 0.66): an increased difference in 3-year RFS rate of approximately 25% (62% versus 37%) and 15% (61% versus 46%), respectively, versus placebo. 13 In the Pembrolizumab group, the incidence was 37% for irAE grades 1–5 and 7% for grades 3–5. The occurrence of an irAE was associated with a longer RFS in the Pembrolizumab arm (HR, 0.61; 95% CI, 0.39–0.95; p = 0.03) in both men and women. The reduction in the hazard of recurrence and death was greater after the development of an irAE than before (HR, 0.37 versus 0.61; p = 0.03). None of these findings was seen in the placebo arm for patients with irAEs. 8 The occurrence of irAEs in patients receiving anti PD-1/PD-L1 mAbs is often mild and self-limiting; however, less than 5% of treated patients reported severe complications which include either pneumonitis, hypophisitis, myocarditis, dermatitis, hematological disorders such as neutropenia 15 or immune-mediated colitis (IMC). Association of the human leukocyte antigen (HLA) class II encoded HLA-DRB1-DQA1-DQB1 haplotype has been detected in the pathogenesis of irAEs. Recent studies of our group have shown that the expression of HLA-B*35 and DRB1*11 in non-small-cell lung cancer (NSCLC) and in malignant melanoma (MM) patients receiving PD-1 blockade presents a very high risk of autoimmune pneumonitis: this risk population requires careful clinical, laboratoristic, and instrumental monitoring when subjected to ICIs’ treatment. 16 Similar results have also been reported for other tumor types and different immune treatments. 17 In particular, B*35 is a frequent class I HLA allele expressed on the surface of both target cells and activated Antigen Presenting Cells (APCs) able to present antigen-derived peptides to cytotoxic T cells and relative precursors. Hematological irAEs, specifically neutropenia, are rarely observed and are associated with high morbidity and mortality due to infective complications. 18 Thus, early detection and treatment is crucial. 18 Instead, immunological trigger generating IMC has not been defined yet, but the results of several studies suggest a critical role of gut microbiota, related to expression of specific microbial epitopes and specific HLA haplotypes, involved in the systemic immunoresponse and in local inflammatory processes. 19 Clinically, IMC is graded by the Common Terminology Criteria for Adverse Events (CTCAE) 20 including severe diarrhea, abdominal pain, nausea, rectal bleeding, and mucous release. Mild (grade 1) events can be managed merely with a symptomatic therapy; nevertheless moderate (grade 2–3) and severe cases (grade 4), with significant morbidity and even mortality 21 require suspension of treatment, hospitalization and the use of immunosuppressive agents. High-dose steroids are often used as a frontline strategy; moreover, some case reports and series report also the use of TNF-α blockers (Infliximab and Adalimumab) in IMC. Anti TNF-α agents are commonly used for moderately to severely active ulcerative colitis (UC), sharing several clinical and immunological features with IMC.22,23 Johnson et al. 24 have shown that patients who received Infliximab and corticosteroids (dexamethasone, methylprednisolone, and prednisone) had a faster symptoms resolution than those treated with steroids alone (3–4 days versus 9–13; p < 0.001). Furthermore, in this study Infliximab did not affect either time to treatment failure (TTF) or OS in patients with metastatic MM. Vedolizumab (Entyvio, Takeda) is a humanized mAb with activity against the a4b7-integrin heterodimer located on the surface of CD4+ T cells and affects lymphocyte trafficking within the gastrointestinal tract; recently this mAb was proven to be a viable alternative treatment strategy in patients not responding to anti-TNF-α therapy or unable to use it.25–27 Nowadays, Vedolizumab has been empirically used in the treatment of patients with severe corticosteroid-resistant IMC. 28 Here, we describe the first case of Vedolizumab use in Pembrolizumab adjuvant treatment for MM patient with corticosteroid-refractory IMC and autoimmune neutropenia.
Case presentation
A 44-year-old female was referred to our observation. The patient, ECOG performance status 0, underwent wide local surgical excision and sentinel node biopsy followed by a complete regional lymphadenectomy, with a diagnosis of ulcerated MM with a Breslow thickness of 1.2 mm, mitosis between 1 and 6 per mm2 and the absence of intense intra-tumor lymphocyte infiltrate (Stage III C); MM cells were bearing BRAF-V600E specific mutation. After discussion with the patient, on January 2020 she was addressed to adjuvant Pembrolizumab 200 mg flat dose planned for 12 months, 29 considering disease staging, patient’s performance status and absence of comorbidities. After 5 treatment cycles, she referred the occurrence of an unexpected severe grade 3 (eight-ten stools/day) diarrhea according to CTCAE, associated with intense abdominal pain, weight loss, and fever refractory to antibiotics. Blood chemistry tests unveiled grade 4 neutropenia (zero neutrophils total count); thus, she was immediately hospitalized. A multidisciplinary approach was activated: the anti-PD-1 treatment was suspended. Loperamide and hydration were administered. Due to the onset of pyrexia with the increase of body temperature up to 39°C, C-reactive protein (CRP), procalcitonin, blood cultures, stool cultures for common pathogens, ova and parasites, fecal calprotectin, serology for Salmonella, Clostridium, and common viruses were performed. Intravenous antibiotic therapy with Piperacillin/Tazobactam, Vancomycin, and antimycotic treatment were promptly started after exclusion of infectious etiology.
A severe hypocellularity (less than 30% cellularity), marked reduction of maturing granulopoiesis, and normal erythroid component were shown in bone marrow biopsy. Expression of CD-34 positive cells, myeloperoxidase (MPO), and glycophorin reactivity by immunochemistry (IHC) analysis were also observed. Based on these findings and according to multidisciplinary evaluation and literature reports, a presumptive diagnosis of autoimmune neutropenia was inferred. High dose of corticosteroids (methylprednisolone 2 mg/kg) and granulocyte colony-stimulating factor (GCSF) were administered. Three days later, the patient underwent initial oxygen therapy with a Venturi mask and subsequent positioning of the high flow oxygenation ventilation device due to the onset of hypoxemic respiratory failure with alkalosis, without radiological signs of pneumonia. The patient was moved to the intensive care unit (ICU) because of worsening of the conditions (pH = 7.511, pCO2 = 25.3 mmHg, pO2 = 50.6 mmHg at the arterial blood sampling). The treatment was maintained with high dose of corticosteroids and GCSF, with progressive improvement of the neutrophil counts for 10 days. Although high doses of steroids were administered, unfortunately, the colitis worsened, requiring ulterior specific diagnostic work-up to exclude possible gastroenteric complications. Stool cultures, serology for Salmonella, Clostridium, and common viruses were reperformed, radiological imaging of abdomen, pelvis and colonoscopy with multiple biopsies within the ileum, and colon were carried out. After exclusion of infectious etiology, endoscopic examination has shown aspect related to severe disease activity (grade 3 according to Mayo Endoscopic score) 30 : erythema, absent vascular pattern, friability, erosions, and ulcerations with spontaneous bleeding (Figure 1(a)–(c)). Histological examination demonstrated crypt architectural distortion, neutrophil-mediated epithelial injury (cryptitis), and neutrophil increase in lamina propria (Figure 1(d)–(f)). Due to the persistence of steroid-resistant colitis after 15 days of high-dose corticosteroid treatment, excluding the use of Infliximab for the risk of a potentially septic state, Vedolizumab was recommended. The patient received the first administration at flat dose of 300 mg according to the induction scheme at 0, 2, and 6 weeks. The first dose was followed by a rapid reduction of the symptoms with stools frequency decreased to 2–3 events per day (mild diarrhea, grade 1). Notably steroids tapering was performed reducing dosage by 5 mg every 5 days. Two weeks later, symptoms and signs of IMC completely disappeared just after the second treatment cycle administered, with subsequent progressive reduction of CRP and calprotectin in the following weeks (Figure 2). Patient was subsequently released from the hospital, considering the slow but progressive improvement of clinical conditions. Ten weeks after the initiation of therapy, a sigmoidoscopy with biopsies was performed, showing an improvement in the endoscopic appearance with mucosal healing (Figure 3(a)–(c)). Histological examination has shown a single layer of columnar or cuboidal epithelium with occasional lymphocytes between epithelial cells (Figure 3(d)–(f)). HLA class I and II were also evaluated to investigate any further causes of this serious reaction, revealing the expression of HLA A*02 *02; HLA B*14 *35; HLA C *04*08; HLA DRB *01 *07. Pembrolizumab therapy was definitely discontinued and patient initiated clinical and instrumental follow-up. Six months later, patient was in good general conditions; laboratory tests and CT scan showed no signs of disease progression and colonoscopy an endoscopic appearance of remission. Vedolizumab treatment is still ongoing according to maintenance scheme.
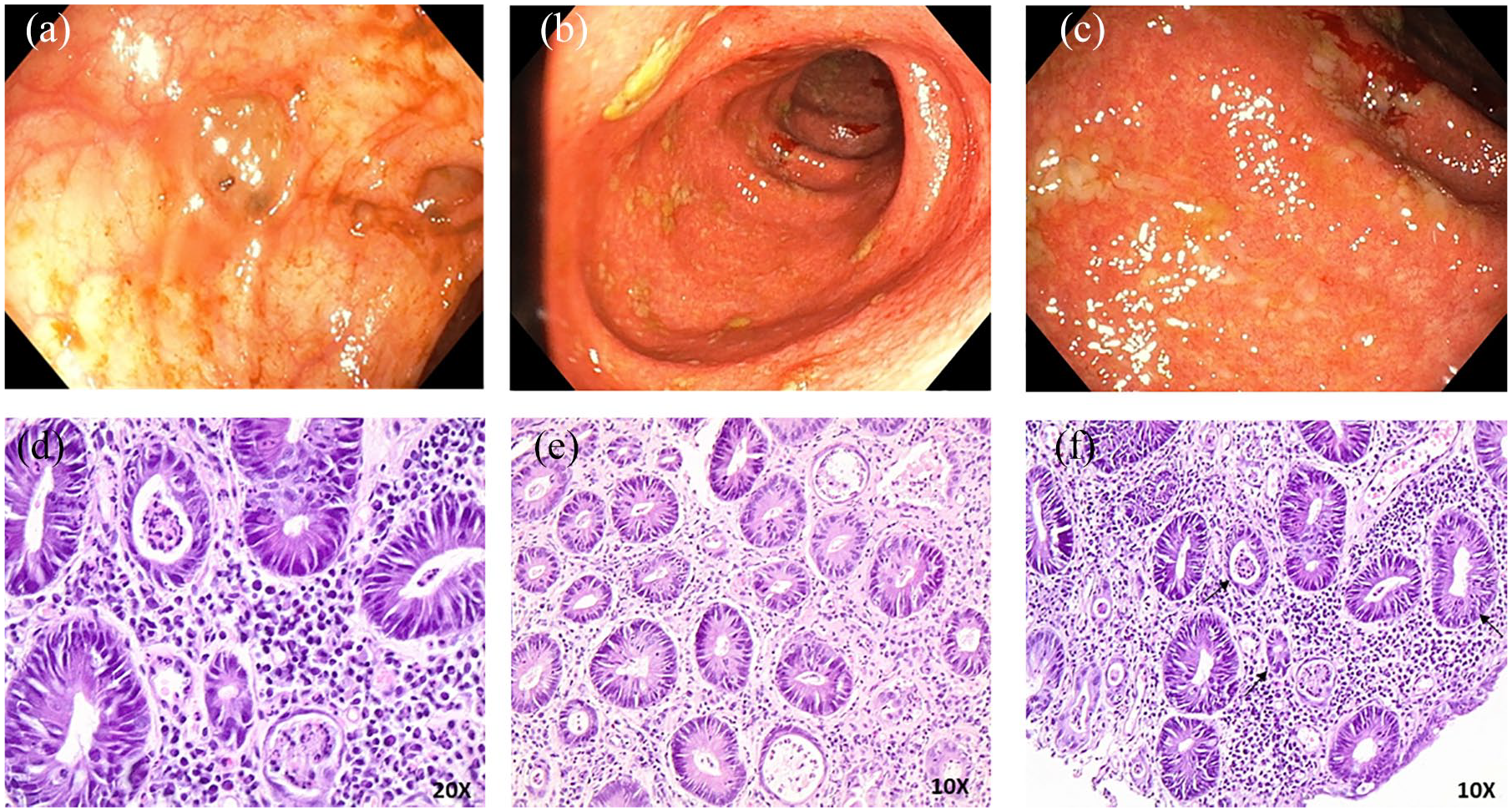
Endoscopic still images of Colitis. (a) Colonic mucosa with deep ulceration; (b and c) Colonic mucosa with mucosal friability, loss of vascular pattern, erythema and edema; (d–f) Biopsy from colonic sample of colitis. This fragment demonstrates crypt architectural distortion, neutrophil-mediated epithelial injury (cryptitis) with >50% crypts involved (left side narrows) and decrease in goblet cells (right side arrows). Moderate neutrophil increase in lamina propria.

Efficacy of Vedolizumab and corticosteroid treatments in patient. (a) Exponential growth of absolute neutrophils and stability of C-reactive protein (CRP) at incremental dosages of corticosteroids. (b) Reduction of CRP levels after Vedolizumab treatment at 300 mg dose flat. (c) Reduction of Calprotectin levels after Vedolizumab treatment at 300 mg dose flat.

Endoscopic still images of colon after 10 weeks of treatment with Vedolizumab. (a–c) Normal endoscopic appearance; (d–f) Biopsy from colonic sample depicts histology near remission. A single layer of columnar or cuboidal epithelium and crypts of Lieberkühn composed of absorptive cells (with basally located nuclei) and goblet cells. Lymphocytes are present between epithelial cells.
Discussion
The occurrence of irAEs may be a highly detrimental event in patients receiving PD-1 blockade for MM in adjuvant setting. Hematological toxicity is a rare but potentially serious immune-related side effect of immunotherapy. In our case report, administration of corticosteroid resulted in a progressive improvement in the neutrophil count but it was not effective in IMC. To the best of our knowledge, this is the first report that describes Vedolizumab as successful first line treatment in anti-PD-1 corticosteroid-refractory IMC during adjuvant treatment for MM. Previous data report individual clinical experiences concerning the use of mAbs Infliximab and Vedolizumab only in the management of metastatic setting. The first case series published by Bergqvist et al. suggests the use of Vedolizumab in the treatment of steroid-refractory immune-mediated enterocolitis reporting a complete remission of symptoms within 56 days from the beginning of the treatment. 31 A retrospective case series of 28 patients with IMC refractory to steroids or Infliximab reports how in 86% of patients Vedolizumab is effective in term of sustained clinical remission with a good safety profile. 32 Similarly, a retrospective analysis of 84 patients who had developed IMC treated with Infliximab or Vedolizumab shows a more favorable clinical outcome than untreated patients. 33 The use of Infliximab, resulting in a potential suppression of tumor and central T cell, was not allowed because of our patient’s immunosuppressive conditions. 34 In this context, it is reasonable to consider the use of Vedolizumab because of its selective action on T-cell trafficking in the gut. Different pharmacological response to the two irAEs could be speculated by several hypothetical pathogenetic mechanism occurring in the same patient, in particular when absence of active disease (adjuvant setting) could be related with an abnormal upregulation of the immune system. This intriguing hypothesis could however be better explained by performing specific molecular and prospective clinical studies. The severe toxicity described in our case report correlates also with the expression of HLAB35 in line with previous studies. 16 In this setting, HLA-B*35 allele could be a potential biomarker for predicting the genetic basis of a susceptibility of high-risk autoimmune disease patients treated with immunotherapy. Indeed evaluation of the inflammatory and immune profile as well as of the autoimmune HLA haplotypes might significantly improve the identification of patients with high risk of severe irAEs, in association with pharmacogenomics studies on targeted small molecules in advanced and adjuvant setting.35–38
Conclusion
Management of irAEs in adjuvant immunotherapy for MM patient is complex and controversial due to potential long-term benefits versus risks of a systemic treatment. Our case describes a novel multidisciplinary management of two side effects requiring different combined treatments. Notably, Vedolizumab is a promising therapeutic option for the treatment of patients with moderate-to-severe IMC, refractory or intolerant to corticosteroid therapy, because of efficacy, gut-selectivity, and safety. Future studies will clarify risk factors and biomarkers for predicting irAEs. Furthermore, in a tailored way, specific HLA typing could be an important biomarker to identify patients with major susceptibility to autoimmune/autoinflammatory disease and to prevent adverse events of immunotherapy. Our experience offers a possible future perspective about the use of Vedolizumab together with immunotherapy in a strategic early approach for high-risk patients genotyped for HLA. Perspective studies with larger sample size are needed to better define this innovative approach.
Footnotes
Acknowledgements
This work has been partially supported by DMSC funds. This is a short text to acknowledge the contributions of specific colleagues, institutions, or agencies that aided the efforts of the authors.
Author contributions
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to PT,
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been supported by funds of the DMSC, UMG, Italy.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethic Statement
Ethics approval was not required for this case report. Upon admission at our University Institution, written informed consent for publication of clinical details and/or clinical images was obtained from the patient.