
Abstract
Objective:
The aim of this study was to evaluate the association between nonalcoholic fatty liver disease (NAFLD) and NAFLD with different comorbidities and risk of chronic kidney disease (CKD) and abnormal albuminuria.
Materials and Methods:
A total of 3872 Chinese individuals excluding those with hepatitis B or C infection and absence of alcohol abuse were included in the study. NAFLD was diagnosed by abdominal ultrasonography. The liver fibrosis was assessed by NAFLD fibrosis score (NFS) and fibrosis-4 index (FIB-4). CKD was defined as an estimated glomerular filtration rate (eGFR) < 60 ml/min/1.73 m2 and/or abnormal albuminuria (urinary albumin-to-creatinine ratio ⩾ 3 mg/mmol). The logistic regression analysis was performed to examine the association between NAFLD and NAFLD with different comorbidities and risk of CKD.
Results:
The prevalence of CKD and abnormal albuminuria was higher in individuals with NAFLD than in those without NAFLD (15.8% vs 11.9%, p < 0.001; 14.8% vs 11.0%, p < 0.001). Logistic regression analysis demonstrated that NAFLD was risk factor of CKD. Notably, after adjustment for sex, age, and DM, NAFLD was associated with 1.31-fold higher risk of prevalent CKD ⩾ 1 (p < 0.05). NAFLD individuals with elder age, DM, obesity, hypertension, MetS, and advanced liver fibrosis had higher risks of both prevalent CKD and abnormal albuminuria than those without comorbidities.
Conclusions:
NAFLD and NAFLD with traditional comorbidities are strongly associated with risk of prevalence of CKD and abnormal albuminuria. Patients with NAFLD especially those with coexisting comorbidities were recommended to carefully access the development of CKD.
Keywords
Introduction
Nonalcoholic fatty liver disease (NAFLD) is one of the most common chronic liver diseases 1 and has become a worldwide health burden over the past two decades. The prevalence of NAFLD has been reported to be approximately 25% in the general population, and it appears to be rapidly increasing, with an estimated 3.6 million new cases annually. 2 NAFLD includes a broad range of disease spectrum, such as simple hepatic steatosis and nonalcoholic steatohepatitis (NASH), which with time can progress to cirrhosis, end-stage liver disease, hepatocellular carcinoma (HCC), or the need for a liver transplant. 3 Studies have demonstrated that NAFLD not only leads to end-stage liver disease but is also strongly associated with extrahepatic diseases, such as obesity, diabetes, dyslipidemia, and hypertension. 4
The known risk factors for NAFLD are strongly similar to those of chronic kidney disease (CKD). CKD was defined by a low serum creatinine-based estimated glomerular filtration rate (eGFR) and/or raised urinary albumin measured by the urinary albumin-to-creatinine ratio (ACR). 5 The prevalence of CKD is estimated to be 9.1% in the global population, which amounts to approximately 700 million cases and brings heavy health burden and socioeconomic costs. 6 Some studies reported that the prevalence and incidence risk of CKD were significantly increased among NAFLD patients compared with those without NAFLD.7,8 Furthermore, CKD is independently associated with an increased overall mortality among patients with NAFLD. 9 One study analyzed the United Network Organ Sharing (UNOS) database during the years 2002–2011 and showed that up to 35% of patients transplanted for NAFLD-related cirrhosis progressed to stage 3b-4 CKD within 2 years after liver transplantation, compared with 10% of patients transplanted for other etiologies. 10 As NAFLD-related cirrhosis and HCC increase, the incidence of simultaneous liver-kidney transplantation has increased remarkably in recent years.11,12 NAFLD is an emerging risk factor for renal dysfunction, unlike other etiologies of cirrhosis. Early recognition and interventions for CKD among NAFLD patients to reduce the staggering cost of CKD and related hospitalizations is a global priority. Unfortunately, the impact of NAFLD on the risk of CKD is often unrecognized and requires further study.
The aim of this study was to evaluate the prevalence of CKD in a unique cohort of Chinese individuals, who attend physical examination in a physical examination center and identify the association between NAFLD, especially in those with different comorbidities, and risk of CKD.
Methods
Study population
This was a single-center cross-sectional general population survey from a physical examination center in Beijing, China, between 1 January 2018 and 31 December 2018. Individuals above the age of 18 years who visited the center for annual physical examination were included. Individuals with a history of hepatitis B surface antigen or hepatitis C antibody positivity, excessive alcohol consumption (⩾30 g/day in men and ⩾20 g/day in women), drug-induced liver disease, decompensated liver cirrhosis, active malignancy, or had missing important clinical and laboratory data or urinary albumin-to-creatinine ratio (ACR) were excluded from the analyses.
Sample size calculation and justification
Different sample sizes can be calculated based on the different prevalence of CKD. Here, the sample size was determined based on the overall prevalence of CKD in China. 13 Using Formula: n = 4pq/d2; p = 10% that is, 0.1; q = 1–0.1 = 0.9; d = allowable error; d = 0.020; n = 4 ×0.1 ×0.9/0.022 = 900. Considering 15% of missing data or refusal, the justified sample size was 1035.
Data collection
The data were obtained from electronic medical records (EMRs), including demographic characteristics, past medical history, drug history, physical assessments (including weight, height, waist circumference, and sitting blood pressure), laboratory parameters, and liver ultrasonography.
A total of 3872 eligible individuals were included in the final data analysis. Written informed consent was obtained from each participant prior to the data collection. The study was approved by the Institutional Review Board of Beijing Ditan Hospital, Capital Medical University, Beijing (approval number: 2018-047-08).
Body mass index (BMI) is calculated as weight in kilograms divided by height in meters squared. Obesity was defined as a BMI of ⩾28 kg/m2. Diabetes mellitus (DM) was defined as a fasting plasma glucose level of ⩾7.0 mmol/L or hemoglobin A1c ⩾ 6.5%, or prescription of antidiabetic drugs. Hypertension was defined as systolic blood pressure (SBP) ⩾ 130 mmHg, diastolic blood pressure (DBP) ⩾ 85 mmHg, or prescription of antihypertensive drugs. Metabolic syndrome (MetS) was defined according to the National Cholesterol Education Program ATP III criteria as the presence of any three or more of the following metabolic conditions: (1) abdominal obesity, waist circumference ⩾ 102 cm in men and ⩾ 88 cm in women; (2) serum triglycerides (TG) ⩾ 150 mg/dL (1.7 mmol/L) or drug treatment for elevated triglycerides; (3) serum high-density lipoprotein cholesterol < 40 mg/dL (1.0 mmol/L) in men and < 50 mg/dL (1.3 mmol/L) in women or drug treatment for low high-density lipoprotein cholesterol; (4) blood pressure ⩾ 130/85 mmHg or drug treatment for elevated blood pressure; (5) fasting plasma glucose ⩾ 100 mg/dL (5.6 mmol/L) or drug treatment for elevated blood glucose. 14
Diagnostic criteria of NAFLD
Fatty liver was defined using liver ultrasonography. Participants with other secondary causes of chronic liver disease were excluded, as described in the exclusion criteria. NAFLD was diagnosed based on evidence of fatty liver on ultrasonography.
The severity of liver fibrosis was assessed non-invasively using the NAFLD fibrosis score (NFS) and fibrosis 4 (FIB-4) score. The NFS was calculated as: −1.675 + 0.037 × age (years) + 0.094 × BMI (kg/m2) + 1.13 × impaired fasting glucose/diabetes (yes = 1, no = 0) + 0.99 × AST/ALT ratio − 0.013 × platelet count (×109 /L) – 0.66 × albumin (g/dL). The FIB-4 score was calculated according to the following formula: age × AST (IU/L) / [platelet count (×109 /L) ×ALT (IU/L)1/2]. The lower and upper cutoffs for NFS were −1.455 and 0.676, respectively, and those for FIB-4 were 1.3 and 2.67, respectively. 15 A score below the lower cutoff was used to exclude advanced fibrosis, while a score above the upper cutoff was indicative of advanced fibrosis.
Assessment of chronic kidney disease
The estimated glomerular filtration rate (eGFR) was calculated using the Modification of Diet in Renal Disease (MDRD) equation as follows: eGFR = 186 × [serum creatinine (mg/dL)]−1.154× [age (years)]−0.203 × (0.742 if female). 16 CKD was defined as eGFR < 60 mL/min/1.73 m2 and/or urinary albumin-to-creatinine ratio (ACR) ⩾ 3 mg/mmol. 17 Stages of CKD were defined according to the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines: stage 1, urinary albumin-to-creatinine ratio (ACR) ⩾ 3 mg/mmol with eGFR ⩾ 90 mL/min/1.73 m2; stage 2, ACR ⩾ 3 mg/mmol with eGFR of 60–89 mL/min/1.73 m2; stage 3, eGFR of 30–59 mL/min/1.73 m2 (with or without ACR ⩾ 3 mg/mmol); stage 4, eGFR of 15–29 mL/min/1.73 m2; and stage 5, eGFR < 15 mL/min/1.73 m2. Abnormal albuminuria was defined as ACR ⩾ 3 mg/mmol. 17
Statistical analysis
Data are presented as mean ± standard deviation (SD), median (interquartile range, IQR), counts, or percentages (%) as appropriate. The normality of the samples was assessed using SPSS. The Kolmogorov–Smirnov test and Q-Q plot were used for this analysis. Continuous data were compared using an independent Student’s t test or Mann–Whitney U test for groups without normal distributions. Categorical variables were compared using the chi-square test or Fisher’s exact test as appropriate. Univariate analysis was performed using Cox proportional hazard analysis to identify the independent parameters of CKD or ACR. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. In addition, stratified analyses to evaluate whether the association of NAFLD with CKD or NAFLD with ACR differed between subgroups defined by sex, age (<60 or ⩾ 60 years), DM, obesity (BMI < 28, ⩾28 kg/m2), hypertension, and MetS was performed. Statistical significance was set at p < 0.05. All statistical analyses were carried out using SPSS (version 16.0; IBM, NY, USA), or R software (version 3.3.2; R Development Core Team, Austria).
Results
Clinical characteristics of the study population
The demographic and clinical characteristics of the study population are shown in Table 1. There were 1967 subjects without NAFLD and 1905 subjects with NAFLD. The mean age was 60.0 years. The mean eGFR was 91.9 mL/min/1.73 m2. The prevalence of NAFLD was 49.2%. Compared with subjects without NAFLD, those with NAFLD were more likely to be male, and have a higher BMI, longer waist, DM, hypertension, and MetS. Similarly, uric acid, urinary ACR, alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum alkaline phosphatase (ALP), gamma-glutamyl transferase (GGT), albumin, glycosylated hemoglobin (HbA1c), fasting plasma glucose (FPG), total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), and platelet count were significantly higher in subjects with NAFLD than in those without.
Demographic and clinical characteristics of the study population.
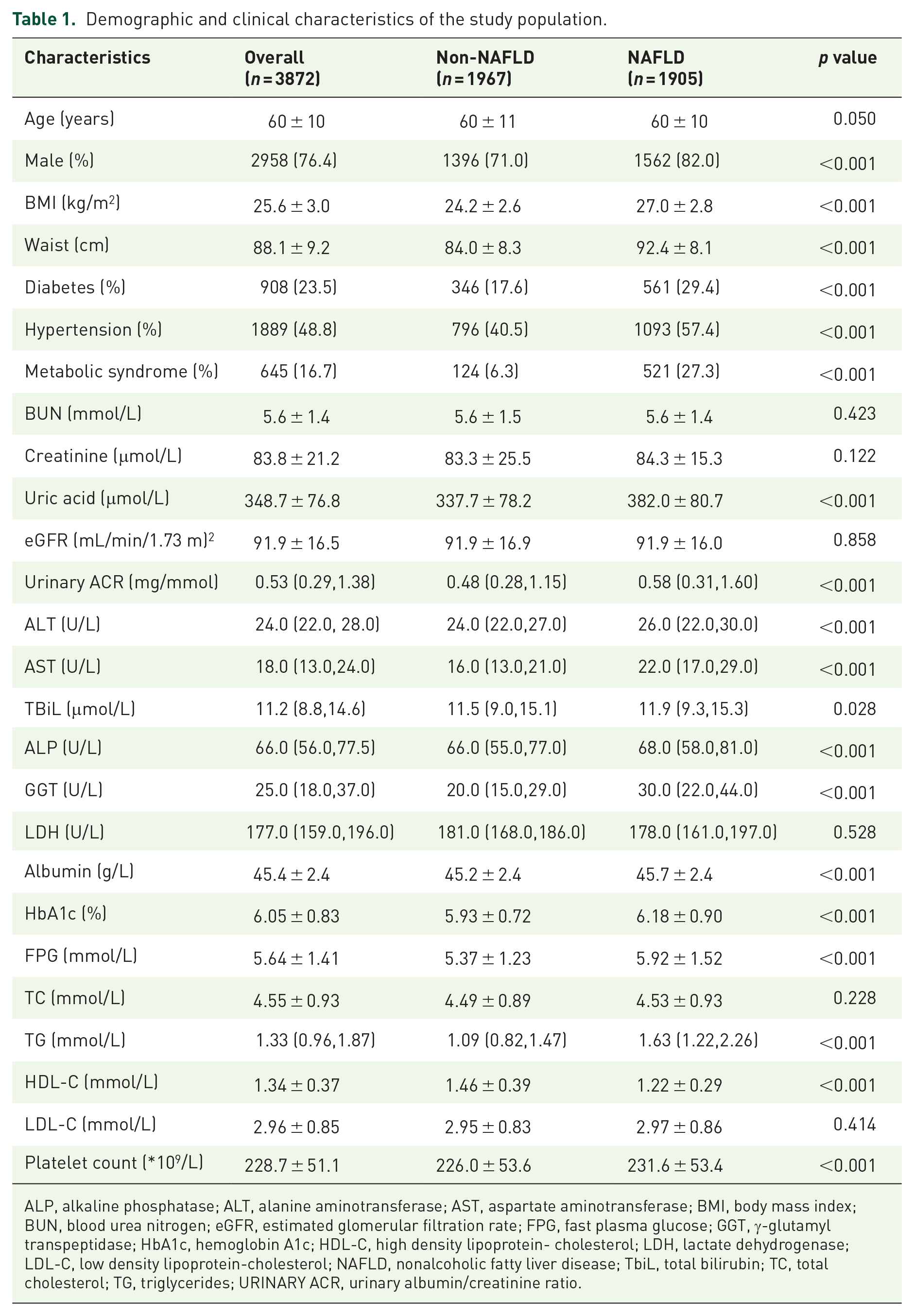
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; BUN, blood urea nitrogen; eGFR, estimated glomerular filtration rate; FPG, fast plasma glucose; GGT, γ-glutamyl transpeptidase; HbA1c, hemoglobin A1c; HDL-C, high density lipoprotein- cholesterol; LDH, lactate dehydrogenase; LDL-C, low density lipoprotein-cholesterol; NAFLD, nonalcoholic fatty liver disease; TbiL, total bilirubin; TC, total cholesterol; TG, triglycerides; URINARY ACR, urinary albumin/creatinine ratio.
NAFLD and the prevalence of CKD or the presence of abnormal albuminuria
The prevalence of CKD and the presence of abnormal albuminuria are shown in Figure 1. The prevalence of CKD was higher in subjects with NAFLD than in those without NAFLD (15.8% vs 11.9%, p < 0.001). In addition, compared with non-NAFLD subjects, the prevalence of CKD was significantly higher in NAFLD with DM, hypertension, and MetS (25.5%, 21.0%, and 25.0%, respectively; all p < 0.001). There was no significant difference in the prevalence of CKD between NAFLD with obesity and NAFLD subjects (15.8% vs 19.1%, p = 0.068). Similarly, the presence of abnormal albuminuria was higher in subjects with NAFLD than in those without NAFLD (11.0% vs 14.8%, p < 0.001). Compared with non-NAFLD subjects, the presence of abnormal albuminuria was significantly higher in NAFLD with DM, hypertension, and MetS (23.5%, 19.3%, and 23.2%, respectively; all p < 0.01). There was no significant difference in the presence of abnormal albuminuria between NAFLD with obesity and NAFLD subjects (14.8% vs 18.0%, p = 0.081). Subjects with NAFLD and DM had the highest prevalence of both CKD and abnormal albuminuria among subjects with NAFLD and comorbidities.

Comparison of prevalence of CKD (panel a) and presence of abnormal albuminuria (panel b) between subjects with non-NAFLD, NAFLD, and NAFLD with difference comorbidities.
Different groups of subjects with NAFLD and CKD stages or abnormal albuminuria
The comparisons of CKD stage and abnormal albuminuria between the non-NAFLD group and different groups of subjects with NAFLD are illustrated in Table 2. The stages of CKD and abnormal albuminuria were significantly different between subjects with and without NAFLD. The NAFLD population was more likely to have CKD 3–5 stage and levels of abnormal albuminuria. In particular, the more advanced CKD stage and increased rate of abnormal albuminuria were more likely to be observed in NAFLD subjects older than 60 years of age, with DM, obesity, hypertension, and MetS.
Comparison of CKD stages and abnormal albuminuria between different groups of subjects with NAFLD. 17

ACR, albumin/creatinine ratio; CKD, chronic kidney disease; DM, diabetes mellitus; NAFLD, nonalcoholic fatty liver disease.
Risk of prevalent CKD and abnormal albuminuria according to logistic regression analysis
Univariate logistic regression analysis was used to further understand the association between NAFLD and kidney damage. As shown in Table 3, the unadjusted OR for prevalent CKD stage ⩾ 1 was 1.39 (95% CI = 1.16–1.67). After adjustment for age and sex, the OR for prevalent CKD stage ⩾ 1 was 1.46 (95% CI = 1.21–1.76). After adjustment for age, sex, and DM, the OR for prevalent of CKD stage ⩾ 1 remained statistically significant (all p < 0.05). Similarly, there was a significant association between NAFLD and albuminuria. Notably, after adjustment for age, sex, and DM, the OR for the presence of abnormal albuminuria remained statistically significant (all p < 0.05). Conversely, for prevalent CKD stage ⩾ 3, no significant association was observed. Compared with NAFLD subjects without comorbidities, those with NAFLD and age more than 60 years, with DM, obesity, hypertension, and MetS had a higher prevalence of CKD stage ⩾ 1 and increased urinary albumin excretion (all p < 0.05). Similarly, NAFLD subjects older than 60 years of age, with DM, hypertension, and MetS had a higher prevalence of CKD stage ⩾ 3 (all p < 0.05).
Associations of NAFLD and NAFLD with comorbidities with CKD (defined as either CKD stage ⩾ 1 or CKD stage ⩾ 3) and abnormal albuminuria (defined as ACR ⩾ 3 mg/mmol). 17

ACR, albumin/creatinine ratio; 95% CI, 95% confidence interval; CKD, chronic kidney disease; DM, diabetic mellitus; NAFLD, nonalcoholic fatty liver disease; MetS, metabolic syndrome; OR, odds ratios.
Subgroup analysis of NAFLD with increased prevalence of CKD and presence of abnormal albuminuria
As shown in Figures 2 and 3, the association between NAFLD and CKD or abnormal albuminuria was evaluated in different subgroups. A positive association between NAFLD and CKD or abnormal albuminuria was consistent in different subgroups, except for sex subgroups (all p values for interaction > 0.10).
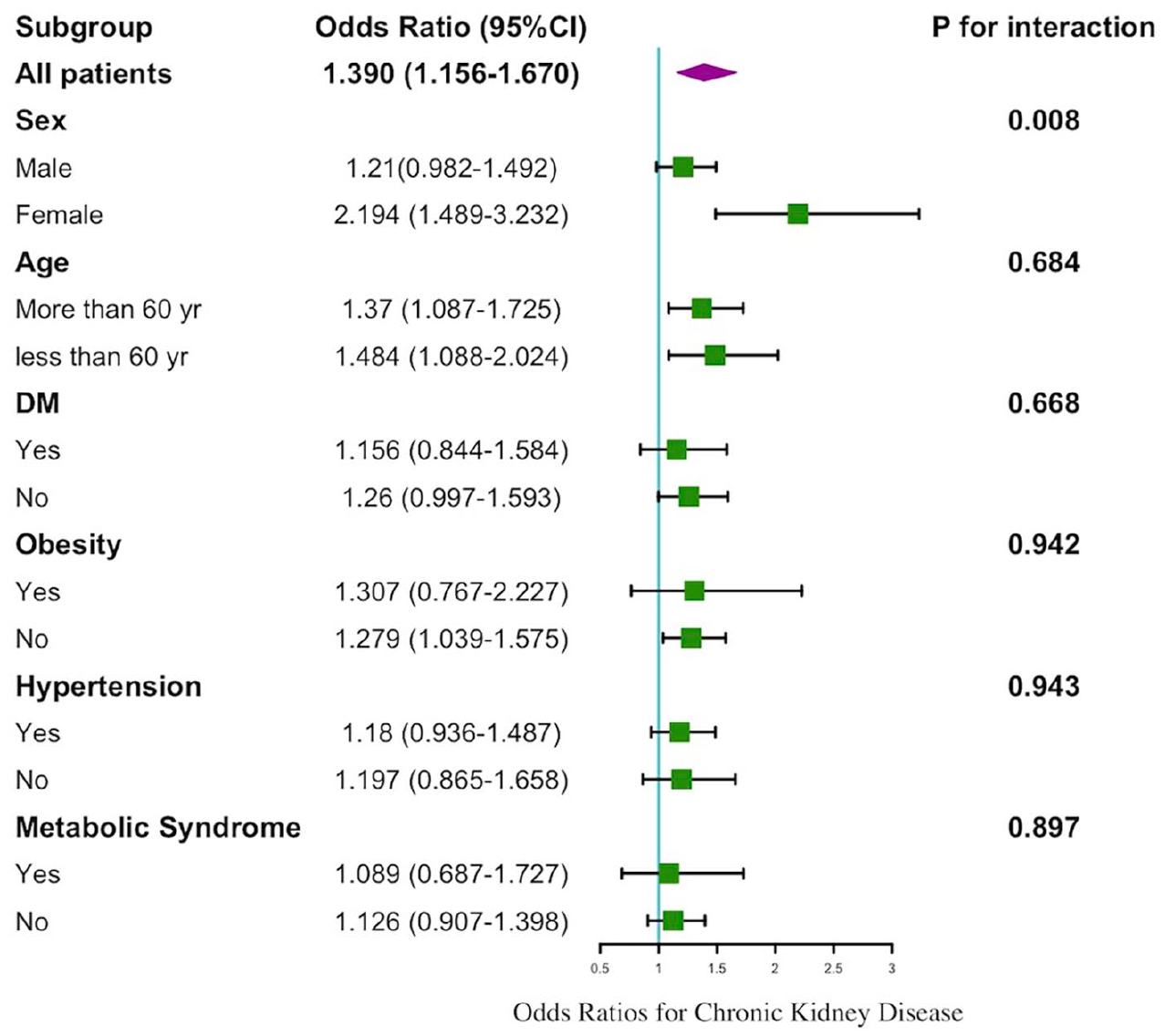
Odds ratios for prevalent CKD comparing participants with NAFLD with those without NAFLD in different subgroups.

Odds ratios for abnormal albuminuria (increased ACR) comparing participants with NAFLD with those without NAFLD in different subgroups.
NAFLD severity and risk of prevalent CKD and presence of abnormal albuminuria
As shown in Figure 4, the prevalence of CKD stage ⩾ 1 or CKD stage ⩾ 3 and the presence of abnormal albuminuria gradually increased in accordance with the severity of NAFLD.

Comparison of prevalence of CKD (panel a, c) and presence of abnormal albuminuria (panel b, d) between subjects with NAFLD and those without NAFLD stratified by NAFLD fibrosis score (NFS) and Fibrosis 4 score (FIB-4).
As shown in Table 4, the unadjusted ORs of prevalent of CKD stage ⩾ 1 or CKD stage ⩾ 3 or abnormal albuminuria for NAFLD severity assessed by NFS or FIB-4 scores were statistically significant (all p < 0.05). After adjustment for age and sex, the ORs for prevalent CKD stage ⩾ 1 or CKD stage ⩾ 3 or abnormal albuminuria for NAFLD severity assessed by NFS or FIB-4 scores were almost statistically significant (all p < 0.05, except the prevalent CKD stage ⩾ 3 for NAFLD severity assessed by FIB-4 scores). After adjustment for age, sex, and DM, the ORs for prevalent of CKD stage ⩾ 1 or CKD stage ⩾ 3 or abnormal albuminuria for NAFLD severity assessed by NFS were almost statistically significant (all p < 0.05), only the prevalent of CKD stage ⩾ 1 for NAFLD severity assessed by FIB-4 scores remained statistically significant (p = 0.026). Univariable logistic regression analyses stratified by the severity of NAFLD were performed to further understand the association between NAFLD and kidney damage. The ORs of prevalent CKD stage ⩾ 1 for increasing levels of NFS were 1.00 (reference), 2.14 (1.65–2.77), and 2.49 (1.76–3.54). Similarly, the ORs of prevalent CKD stage ⩾ 1 for increasing FIB-4 score were 1.00 (reference), 1.36 (1.05–1.76), and 1.46 (1.08–1.98). The ORs of prevalent of CKD stage ⩾ 3 or abnormal albuminuria for NAFLD severity regardless of NFS or FIB-4 scores showed similar trends.
Associations of NAFLD severity (stratified by NFS scores and FIB-4 scores) with CKD (defined as either CKD stage ⩾ 1 or CKD stage ⩾ 3) and abnormal albuminuria (defined as ACR ⩾ 3 mg/mmol). 17

ACR, albumin/creatinine ratio; 95% CI, 95% confidence interval; CKD, chronic kidney disease; DM, diabetic mellitus; FIB-4, fibrosis 4 score; NAFLD, nonalcoholic fatty liver disease; NFS, NAFLD fibrosis score; OR, odds ratios.
Discussion
This study suggested that the prevalence of NAFLD was 49.2% among the general population in Beijing, China. The prevalence of CKD and abnormal albuminuria was higher in individuals with NAFLD than in those without NAFLD. The comorbidities of NAFLD, including DM, hypertension, and MetS, increased the risk of CKD and abnormal albuminuria. The prevalence of CKD and abnormal albuminuria were significantly different in subgroup analyses stratified by age and subgroups of individuals with and without the presence of comorbidities such as DM, obesity, hypertension, and MetS. NAFLD was associated with a moderately increased risk of CKD and abnormal albuminuria, independently of traditional cardiometabolic risk factors. In addition, a greater severity of NAFLD was strongly associated with a higher risk of CKD and abnormal albuminuria. To our knowledge, this is the first cross-sectional study to investigate the association between NAFLD and CKD or abnormal albuminuria, and to analyze the association between the severity of NAFLD and CKD or abnormal albuminuria based on a health checkup of a population from Beijing, China.
Several large cross-sectional and case-control studies have reported that the prevalence of CKD in patients with NAFLD is between 4% and 42%.18–23 A cross-sectional analysis of 37,825 cases from health checkup centers in Taiwan showed that the percentage of CKD was 17.5% in individuals with NAFLD and a significantly positive association between moderate to severe NAFLD and CKD even after adjustment for potential confounders such as age, sex, smoking, components of MetS, and the ALT level. 24 Their results were similar to those of our study. Another important observation of our study was that NAFLD remained a risk factor for CKD regardless of age, sex, and DM. The results of subgroup analysis confirmed that NAFLD was positively related to CKD even in female, younger individuals, and patients without comorbidities, suggesting that more attention should be paid to renal impairment in patients with NAFLD.
A previous meta-analysis of 11 longitudinal studies (involving a total of 28680 individuals) reported that NAFLD was associated with an almost 80% increased risk of incident CKD [random-effects hazard ratio (HR) = 1.79, 95% CI = 1.65–1.95]. 25 An updated meta-analysis that incorporated nine observational studies with 96,595 adult individuals (34.1% with NAFLD) found that NAFLD was associated with an increased incidence of CKD (HR = 1.37, 95% CI = 1.20–1.53) and patients with more advanced NAFLD or fibrosis were more likely to develop incident CKD (HR = 1.50, 95% CI = 1.25–1.74). 26 Another largest and most updated meta-analysis of 13 studies with 1,222,032 individuals (28.1% with NAFLD) and 33,840 cases of incident CKD stage ⩾ 3 over a median follow-up of 9.7 years indicated that NAFLD is significantly associated with ~1.45-fold increased long-term risk of incident CKD stage ⩾ 3, and the risk seems to parallel the severity of NAFLD, especially the severity of liver fibrosis. 8 To date, convincing evidence suggests that NAFLD could be a driving force for the development and progression of CKD.
In our study, the prevalence of NAFLD with obesity or DM was 28.8% and 29.4%, respectively. Obesity, a component of MetS, is the most common risk factor for NAFLD and an independent risk factor for CKD. Diabetes mellitus (DM) is the leading cause of CKD. Patients with NAFLD commonly develop DM. Targher et al. 21 reported that in NAFLD patients with DM, the prevalence of CKD reached 40%. A previous study showed that metabolic abnormality was associated with a significantly increased risk of CKD progression. 27 In this study, we also found that individuals with NAFLD and coexisting MetS had a higher prevalence of CKD and abnormal albuminuria. Our study benefits from understanding the implications of both NAFLD and traditional risk factors for CKD. CKD shares similar risk factors with NAFLD, such as increasing age, obesity, hypertension, DM, and MetS. The relationship between NAFLD and CKD is complex and has not been definitively demonstrated. Three observational cohort studies have reported the influence of NAFLD on the risk of all-cause mortality, incidence of non-fatal cardiovascular events (CVEs), or progression of kidney disease within the CKD population.9,28,29 Only one study showed a strong association between NAFLD and non-fatal CVEs in patients with CKD. 28 The results were conflicting for all-cause mortality and progression of renal disease. Additional larger prospective studies are needed to further examine this association.
Some studies have further analyzed the possible pathophysiological mechanisms by which NAFLD may contribute to the development and progression of CKD. Accumulating evidence suggests that NAFLD (especially with advanced fibrosis) exacerbates hepatic insulin resistance, promotes atherogenic dyslipidemia, induces hypertension, and causes the release of multiple proinflammatory cytokines and hepatokines that may contribute to the development and progression of CKD.7,30,31 Adipose tissue has an endocrine function and can secrete many biologically active adipokines. These cytokines affect the metabolism of adipose tissue and the entire body of the organism. Several studies have reported the potential role of adipokines and other inflammatory mediators in the etiopathogenesis of both NAFLD and CKD. Higher levels of circulating leptin have been found to be associated with increased severity of NAFLD and contribute to the development and progression of CKD.32,33 Adiponectin enhances glucose and fatty acid oxidation, improves insulin sensitivity, attenuates plaque formation, and increases aldosterone production. 34 Decreased adiponectin levels are inversely related to the severity of steatosis, necroinflammation, and fibrosis.35,36 Similarly, decreased adiponectin levels were also associated with a higher risk of end-stage renal disease independent of conventional risk factors, BMI, and metabolic syndrome. 37
Therapeutic interventions for the treatment of both NAFLD and CKD are currently under investigation, and shared common risk factors such as obesity, insulin resistance, inflammation, and underlying pathophysiology suggest that medications and behavioral modifications may be applicable to both diseases. Lifestyle interventions, including exercise, weight loss, and bariatric surgery, can decrease hepatic fat content and inflammation, result in regression of fibrosis, and also have beneficial effects on renal functions, which are associated with improvements in glomerular hemodynamics.38,39 A recent cross-sectional study determined that CKD-NAFLD patients taking angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) had a lower degree of liver stiffness than patients not on medications. 40 Some NAFLD studies suggest that ARBs can attenuate steatosis, insulin resistance, inflammation, necroinflammation, NAFLD activity score, fibrosis stage in NASH, and microalbuminuria.41–43 Glucagon-like peptide-1 receptor (GLP-1R) analogs and dipeptidyl peptidase-4 (DPP-4) inhibitors are all incretin mimetics, which have a potential role in improving NASH and CKD through multiple mechanisms. 44 Both GLP-1R agonists and DPP-4 demonstrated nephroprotection in diabetic nephropathy.45,46 Recent clinical trials reported that liraglutide induced significant weight loss and NASH resolution and improved markers of lipotoxicity, inflammation, and metabolic dysfunction. 47 However, sitagliptin did not induce weight loss or improved radiological and biochemical markers of steatosis, liver fibrosis, and insulin resistance in diabetic NAFLD patients. 48 Given the disease burden imposed by NAFLD and CKD worldwide, it is necessary to identify NAFLD patients with higher risk of incident CKD to prevent early renal damage. Further research is needed to clearly illustrate the mechanism and provide effective treatment for liver and kidney disease in NASH-related CKD.
There are several limitations to our study that need to be noted. First, this is a cross-sectional design; in comparison with a longitudinal design, cross-sectional study is more prone to bias. Furthermore, our findings determined simple associations between NAFLD and CKD, which are inherently inapt to establish a clear causal or consequential nexus. Further intensive studies remain to be conducted to determine the precise relationship between the two. Second, the study population only included Chinese individuals who underwent annual physical examinations at the outpatient clinic. This population might not be representative of other ethnic groups and inpatients. Third, only liver ultrasonography (US) was used to diagnose the fatty liver. It is well known that US can miss milder fatty liver (<25%). However, the overdiagnosis of fatty liver on ultrasound is not common. Liver biopsy is still the gold standard for the diagnosis of NAFLD or NASH with liver fibrosis. Our population was physically examined, considering the risks and costs associated with liver biopsy or other non-invasive assessments such as Fibroscan or MRE (magnetic resonance elastography) and their inappropriateness for widespread use. NFS and FIB-4 score were used instead to assess liver fibrosis in this study. These scores were mainly designed to rule out advanced fibrosis and are not specifically useful for assessing liver fibrosis. In addition, our study enrolled individuals with different BMI statuses, and a recent study 49 that analyzed several non-invasive NAFLD markers including NFS, concluded that their reliability depends on BMI status. The non-invasive markers used to evaluate liver fibrosis in clinical practice should be further explored. Despite these limitations, the results of this study are important in raising awareness of CKD among Chinese individuals with NAFLD.
Conclusion
In conclusion, NAFLD was associated with a higher prevalence of CKD regardless of traditional risk factors, and the severity of NAFLD assessed by non-invasive methods was also positively associated with the prevalence of CKD. Our findings suggest that NAFLD with comorbidities may be associated with a higher risk of CKD and abnormal albuminuria. It is recommended that patients with NAFLD, especially those with coexisting comorbidities, should be carefully accessed for the development of CKD. Future studies should focus on the mechanisms and therapeutic targets for both NAFLD and CKD in a comorbid setting.
Footnotes
Acknowledgements
Ying Cao and You Deng contributed equally to this work. We thank all physicians who participated in the management of the subjects included in this study.
Author contributions
Wen Xie conceived and designed the study; Ying Cao, You Deng, Jingjing Wang, and Jingyu Zhang collected the data; Ying Cao and You Ddeng carried out the statistical analysis, discussed the results, and drafted the first manuscript. Hong Zhao and Wen Xie discussed the results and revised the manuscript. Wen Xie supervised the data collection and interpreted the data. All authors read and approved the final manuscript for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the National Natural Science Foundation Youth Fund Project (81600454), National Natural Science Foundation of China (81770577), and the Clinical Medicine Development Project of Beijing Municipal Administration of Hospitals (ZYLX201828).
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.