
Abstract
Background:
To investigate the efficacy and safety of biologics in the perioperative management of severe aortic valve regurgitation (AR) caused by Behçet syndrome (BS).
Methods:
We retrospectively analyzed 20 patients with severe AR caused by BS who were all treated with biologics during the perioperative period of cardiac surgeries in our center between February 2016 and October 2020.
Results:
A total of 20 patients with severe AR were enrolled, including 19 males and 1 female, with a mean age of 39.1 ± 8.8 years and a median course of 8 [interquartile range (IQR) 5.25–10.00] years. Before biologic administration, 92.9% of the patients who underwent aortic valve replacement had failed conventional therapy and developed postoperative paravalvular leakage (PVL) at a median interval of 4 months. Biologics were administered with background glucocorticoids (GCs) and immunosuppressants during the perioperative period for 22 aortic valve surgeries, including preoperatively with a median interval of 3.5 (IQR 2.75–4.25) months in 13 cases and within 3 months postoperatively in 9 cases. After a median follow up of 21 (IQR 15–32) months, 2 out of 13 cases (15.4%) preoperatively, and 1 out of 9 cases (11.1%) postoperatively treated with biologics developed PVL, and the rest were event free. The Behçet’s Disease Current Activity Form score improved significantly (7 versus 0, median, p < 0.0001). Decrease of erythrocyte sedimentation rate [25.0 (IQR 11.00–36.25) mm/h versus 6.5 (IQR 4.0–8.8) mm/h, p < 0.001], and C-reactive protein [20.77 (IQR 7.19–29.58) mg/l versus 1.53 (IQR 0.94–2.92) mg/l, p = 0.001] were achieved rapidly and effectively. The GC dosage tapered from 40 (IQR 30–60) mg/d to 10 (IQR 5–11.25) mg/d, p < 0.0001. Immunosuppressants were tapered in number and dosage in 6 (30%) and 20 patients (100%), respectively. No serious adverse event was observed.
Conclusion:
Our study suggests that biologics were effective and well tolerated for the perioperative management of severe and refractory AR caused by BS, which significantly reduced the occurrence of postoperative PVL and had favorable GC- and immunosuppressant-sparing effect.
Introduction
Behçet syndrome (BS) is a chronic, relapsing, systemic inflammatory disorder of unknown etiology, characterized by recurrent oral and/or genital ulcers, skin lesions, and multi-organ involvement.1,2 Vasculitis is the underlying patho-logical manifestation involving both venous and arteries of any sizes.3,4 Cardiovascular involvement in BS is rare, whereas it is associated with poor prognosis, and accounts for the leading cause of BS mortality.5,6 Among the spectrum of cardiac involvements, perioperative management of severe aortic valve regurgitation (AR) caused by BS has always been a major challenge. The pathophysiology of AR caused by BS has yet to be understood. 7 Most patients with AR fail to fulfill the diagnostic criteria of BS before undergoing aortic valve (AV) surgery.8,9 Moreover, AR caused by BS is associated with a high incidence of severe postoperative complications, especially paravalvular leakage (PVL) due to the fragilities of aortic lesions and tissue inflammation, leading to a significantly in-creased risk of re-operation, and potentially life-threatening conditions.10–12
Perioperative immunosuppressive therapies with glucocorticoids (GCs) combined with immunosuppressants have been indicated in preventing postoperative PVL.8,12–14 However, many patients are delayed to timely treatment or respond inadequately to these conventional therapies. More rapid and efficient control of inflammation is critical in preserving cardiac function and preventing complications after surgery, which remains an unmet need. In 2018, the European League Against Rheumatism
In this study, we explored the efficacy and safety profile of biologics in the perioperative management of severe AR caused by BS. This study addressed the effects of biologics concerning postoperative PVL prevention, overall disease activity, and GC- and immunosuppressant-sparing effects.
Methods and materials
Study design and patients
We retrospectively studied BS patients from Peking Union Medical College Hospital (PUMCH) between February 2016 and October 2020. Adult BS subjects diagnosed with severe AR caused by BS and treated with biologics during the perioperative period of cardiac surgery were included. The diagnosis of BS was made according to the 2014 International Criteria for BD (ICBD). 16 Patients who did not fulfill ICBD criteria were clinically diagnosed with BS by consensus determination of cardiologists, rheumatologists, pathologists, and cardiac surgeons. Confirmation of AR due to BS was based on subjects’ clinical manifestations, imaging findings (echocardiography and computed tomography angiography), and pathology of surgical specimens. 17 Multiple characteristic echocardiographic manifestations of AR caused by BS were observed, including aneurysmal aortic valve changes, vegetation-like lesions, and aortic lesions, as previously reported.11,18–20
Patients with the presence of other known causes of AV diseases were excluded, such as rheumatic fever, Marfan syndrome, congenital heart disease, infective endocarditis, syphilis, and AV degeneration. Other key exclusion criteria were severe liver and kidney insufficiency, current or prior active tuberculosis, hepatitis B or hepatitis C infection, any persistent or severe infection, and history of malignancy. Patients with evidence of latent tuberculosis were initiated a 1-month or longer course of tuberculosis prophylaxis before receiving biologics.
Patients were evaluated and followed up with the collaboration of rheumatologists, cardiologists, and cardiac surgeons. The cardiac surgeons determined the surgical approach, and rheumatologists mainly guided the perioperative therapy. Surgical procedures included aortic valve replacement (AVR) and aortic root replacement with a composite graft (i.e. Bentall procedure and Cabrol procedure). All patients received treatment with biologics, including adalimumab (ADA), golimumab (GOL), infliximab (IFX), and tocilizumab (TCZ), along with concomitant treatment of maintained or decreased GCs and immunosuppressants during the perioperative period. IFX was administered at a dose of 5 mg/kg intravenously at 0, 2, and 6 weeks, followed by every 8 weeks. Patients received TCZ intravenously at a dose of 8 mg/kg every 4 weeks. ADA was administered at 40 mg subcutaneously every 2 weeks. GOL was injected subcutaneously at a dose of 50 mg every 4 weeks. During follow up, the dose and frequency of biologics were adjusted, and further tapering was tailored to each patient’s clinical needs. During the perioperative period, biologics were generally paused at least 2 weeks before the operation based on their median terminal half-life,21–24 and were continued at least 4 weeks after the cardiac operation if infection was excluded.
The following data were collected and analyzed: demographic characteristics, medical history, disease duration between the first clinical manifestation and AV involvement of BS, the main clinical manifestations, lab examinations [inflammatory markers (erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)], imaging findings (echocardiography, computed tomography angiography), treatment regimen, surgical intervention and pathology results. BS disease activity was evaluated by the Behçet’s Disease Current Activity Form (BDCAF) 2006 (http://www.Behçet.ws/pdf/BehçetsDiseaseActivityForm.pdf). Imaging examinations, especially echocardiography, was routinely performed every 3–6 months during follow up to assess PVL after AV surgery. PVL was graded as mild, mild–moderate, moderate, moderate–severe, and severe, in accordance with the American Society of Echocardiography recommendations.25,26 Moderate-to-severe PVL, suggested by the previous meta-analysis that affected short- and long-term survival mortality, and required further surgical interventions, were included in our outcome assessment. 27
This study complied with the Declaration of Helsinki and was approved by the Institutional Review Board of PUMCH (approval number: S-443). Written informed consent was obtained from all patients. Patients’ records/information were anonymized and de-identified before analysis.
Outcome assessment
The primary aim was to evaluate the effectiveness of biologics in reducing postoperative complications of AV surgery, especially PVL, in BS patients with AR. The secondary outcomes were the clinical changes of BS disease activity (including BDCAF score, ESR, and CRP), GC- and immunosuppressant-sparing effect, and adverse events.
Statistical analysis
Data with Gaussian distribution were presented as mean value ± standard deviation. Data with non-Gaussian-distributed data were described as median value and interquartile range (IQR). Qualitative variables were expressed as an absolute number and percent number (%). The continuous variables were analyzed by the paired- or unpaired-sample t test, as appropriate. A two-sided test with p values < 0.05 was considered a statistically significant difference. Statistical analyses were performed using the SPSS (version 23.0, IBM Corp, Armonk, NY, USA).
Results
Characteristics of patients with AR caused by BS
A total of 20 BS patients (19 males and 1 female) with severe AR were enrolled as described in Table 1. Among them, 16 BS patients (80%) fulfilled the 2014 ICBD criteria, and 4 BS patients (20%) were clinically diagnosed based on clinical, surgical and pathological findings. The mean age was 39.1 ± 8.8 (range 23–57) years, and the median disease duration of BS was 8 (IQR 5.25–10) years. The mean interval between BS onset and the detection of AR was 8.9 ± 5.8 (range 0–20) years. AR was observed in 19 patients at the time of BS diagnosis, among whom 13 cases were diagnosed after recurrent PVL after AVR surgeries. One patient developed AR 2 years after diagnosed with BS.
Clinical and outcome data of patients treated with biologics for severe aortic regurgitation due to Behçet syndrome.

A, arthritis; AR, aortic regurgitation; AZA, azathioprine; COL, colchicine; CTX, cyclophosphamide; G, genital aphthosis; GCS, glucocorticoids; GOL, golimumab; IFX, infliximab; LEF, leflunomide; MMF, mycophenolate mofetil; MR, mitral regurgitation; MTX, methotrexate; O, oral aphthosis; P, positive pathergy test; PVL, paravalvular leakage; S, skin involvement; SASP, sulfasalazine; TCZ, tocilizumab; THD, thalidomide; TR, tricuspid regurgitation; U, uveitis; V, vascular involvement.
Cardiac manifestations
Among the 20 patients, 6 patients (30%) were asymptomatic of cardiac manifestations, and their AV lesions were detected by physical examination. Ten patients (50%) initially complained of cardiac failure or aortic insufficiency symptoms, including exertional dyspnea, hemoptysis, and paroxysmal nocturnal dyspnea. Two patients (10%) showed recurrent fever with or without dyspnea before AV lesions were identified.
All 20 patients presented with severe AR on preoperative echocardiography, with dilation of the aortic root or ascending aorta in 8 patients (40%), aneurysm of the aortic sinus in 8 patients (40%), mitral regurgitation and tricuspid regurgitation in 8 patients (40%), an echocardiographic-free space mimicking paravalvular abscess in 7 patients (35%), aortic dissection in 3 patients (15%), and vegetation-like mobile lesions were presented in 2 patients (who had been misdiagnosed with infective endocarditis; 10%), respectively (Table 1).
BS manifestations
Except for cardiac valve involvement, oral ulceration was presented in all 20 patients, followed by skin lesions (90%; including pseudo-folliculitis, erythema nodosa, and pathergy), genital ulcers (60%), arthritis (30%), ocular involvement (5%). Additionally, extra-cardiac arterial occlusions/stenosis were presented in two (10%) patients.
Previous cardiac surgeries
Previous studies have suggested that BS patients with AR have a significantly high risk of PVL after cardiac valve operation. The occurrence of PVL is associated with insufficient preoperative immunosuppressive therapy and elevated preoperative ESR. 12
In this study, 11 patients had undergone 14 cardiac surgeries before biologic administration, including 3 treatment-naïve patients who had undergone reoperation due to severe PVL or aneurysm after their first operation. The recorded preoperative inflammatory markers, ESR [41 (IQR 26.00–82.43) mm/h] and CRP [19.65 (IQR 11.65–38.50) mg/l], were both significantly elevated. Severe cardiac complications occurred after all 14 cardiac valve surgeries. Thirteen of them (92.9%) developed moderate-to-severe PVL at a median interval of four (IQR 2–5) months postoperatively. Ascending aortic anastomosis aneurysm occurred in one patient 7 months after surgery.
Histologic findings of AV tissue from four patients were characterized by chronic inflammation, cellulose-like necrosis, and local inflammatory cell infiltration.
Perioperative biologic treatment
Perioperative biologics were introduced for the following indications: (a) the urgency to perform cardiac surgery for patients with uncontrolled disease progression (such as severe heart failure, progressing of the aneurysm or aortic dilation) or occurrence of moderate-to-severe PVL after previous surgeries despite intensive conventional therapy; therefore, biologics were administrated in eleven patients shortly before the operation for rapid and effective control of inflammation and GCs tapering; (b) the other nine patients treated with conventional therapies (GCs and multiple immunosuppressants [two (range 1–4) types] perioperatively showed uncontrolled disease activity after cardiac surgeries, indicated by significantly elevated postoperative inflammatory markers. Additionally, five of them had developed PVL in previous surgeries, leading to a high risk of leak recurrence. After ruling out infection, biologics were initiated postoperatively at a median interval of 1 (range 1–3) month for suppressing inflammation and reducing disease activity.
With GCs and immunosuppressants as concomitant therapy, all patients received perioperative biologics, including TCZ in nine cases, GOL in five cases, ADA in two cases, and IFX in one case. Three cases had their biologics switched, one from TCZ to GOL because of gastrointestinal bleeding, one from TCZ to IFX due to the development of PVL, and one from ADA to TCZ for financial concerns. The mean duration of biologic treatment was 16.9 ± 11.2 months.
Outcomes
Effective control of inflammation and disease activity
Treatment with biologics was associated with rapid resolution of clinical symptoms. The BDCAF score of 20 patients decreased significantly [7 (IQR 7–8) versus 0 (IQR 0–3), p < 0.0001]. Fifteen (75%) patients had complete resolution of clinical symptoms at the last visit, five (25%) patients had minor oral ulcers or skin lesions occasionally. No other major organ involvement was observed during follow up. All patients achieved rapid and effective suppression of inflammation indicated by significant decrease of ESR [baseline: 25.0 (IQR 11.00–36.25) mm/h versus last visit: 6.5 (IQR 4.0–8.8) mm/h, p < 0.001] and CRP [baseline 20.77 (IQR, 7.19–29.58) mg/l versus last visit 1.53 (IQR 0.94–2.92) mg/l, p = 0.001] (Figure 1).

Effectiveness of biologics for patients with Behçet syndrome (BS).
Perioperative biologics decreased occurrence of PVL
A total of 20 patients had 22 cardiac surgeries after enrollment. Postoperative complications of patients treated with perioperative biologics during follow up are summarized in Figure 2.
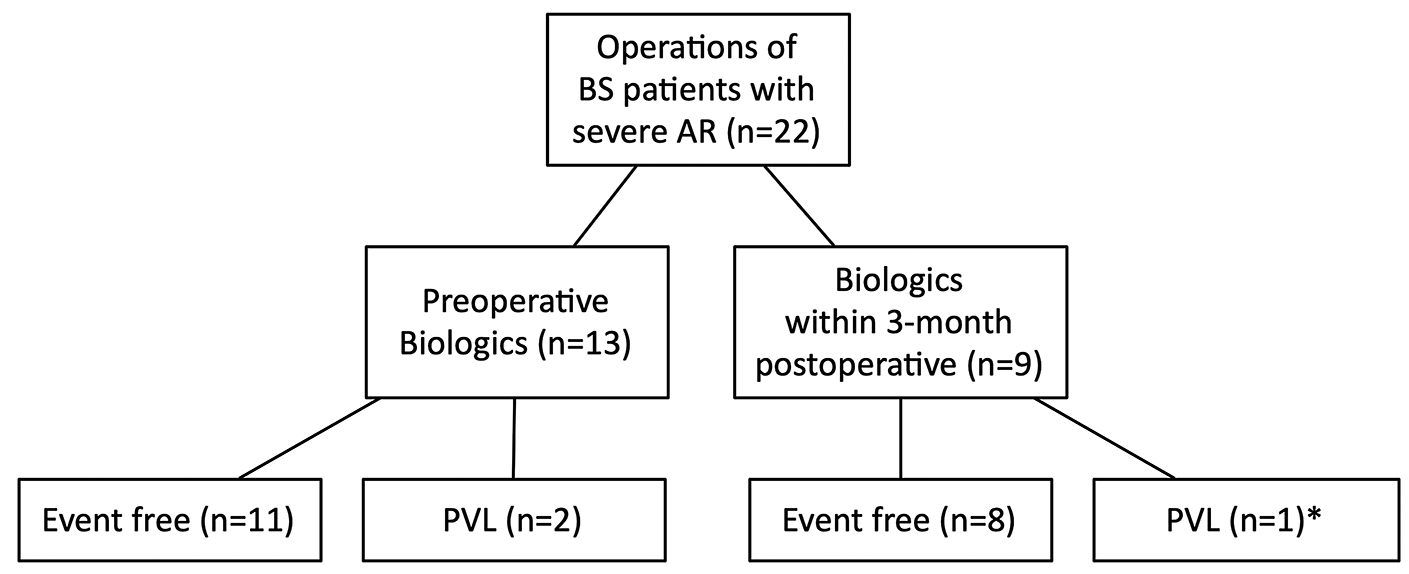
Summary of the clinical outcomes of aortic regurgitation (AR) in Behçet syndrome (BS) treated with biologics during the perioperative period.
Thirteen cases (59%) started biologics 3.5 (IQR 2.75–4.25) months before the cardiac operation. Among them, 11 cases (84.6%) were PVL free during follow up, no new-onset cardiovascular events occurred, and ESR and CRP levels remained normal during the entire perioperative period. Moderated PVL was observed in the other two cases (15.4%) 3–4 months after surgeries with TCZ treatment. Both had elevated inflammatory markers at surgery (ESR 30 mm/h and 75 mm/h, CRP 20.43 mg/l and 82.51 mg/l) and 3 months’ postoperation (ESR 77 mm/h and 93 mm/h, CRP 29.07 mg/l and 31.49 mg/l). One of them switched to IFX and the other continued TCZ treatment without dose adjustment. Both achieved freedom from surgical complications for subsequent cardiac surgeries, with normal perioperative inflammatory markers. No PVL was observed after 21–28 months of follow up.
Nine cases (41%) started biologics within 3 months postoperatively, and ESR and CRP levels decreased to normal ranges 3 months after surgeries. During follow up, eight cases (88.9%) were event free. One case developed moderate PVL within 1 month post-surgery, who then started treatment with biologics. The patient remained stable on biologics during 32 months of follow up without reoperation.
Given that PVL generally develops 3.5–4 months after surgery in active BS, 12 we collected ESR and CRP levels at the last visit before surgery, and at 1 month and 3 months after surgery. A summary of the clinical manifestations, laboratories, and outcomes of all cases throughout the perioperative period is shown in Figure 3.

Summary of the clinical outcomes and level of inflammatory markers of patients treated with biologics during the perioperative period.
Collectively, PVL developed in 3 out of 22 (13.6%) cardiac surgeries with perioperative biologic treatment. The 19 surgeries without PVL had inflammation effectively controlled with biologic treatment, either initiated preoperatively or postoperatively. Meanwhile, the other three surgeries that developed postoperative PVL showed significantly elevated ESR and CRP levels throughout the 3 months postoperative period. (With PVL versus without PVL: preoperative ESR, 48 ± 23.8 versus 10.5 ± 9.4, p < 0.001; 3-month postoperative ESR, 59 ± 45.7 versus 6.4 ± 6.1, p < 0.01; preoperative CRP, 43.1 ± 34.2 versus 6.5 ± 12.8, p < 0.01. 3-month postoperative CRP, 20.4 ± 17.1 versus 3.4 ± 6.0, p < 0.05.)
Sparing effect of GCs and immunosuppressants
The dosage of GCs was significantly tapered [baseline: 40 (IQR 30–60) mg/d versus last visit: 10 (IQR 5.00–11.25) mg/d, p < 0.0001]. Immunosuppressants were tapered in number and dosage in 6 (30%) and 20 patients (100%), respectively.
Safety
One patient experienced gastrointestinal bleeding due to terminal ileal ulcers after 8 months of TCZ treatment and achieved mucosal healing after switching to GOL. No other serious adverse event occurred in the other patients. One patient (no. 4) was diagnosed with latent tuberculosis (TB) and initiated prophylaxis with isoniazid 1 month before using GOL and continued isoniazid therapy during GOL treatment. No TB reactivation was observed during follow up.
Follow up
Overall, with a median follow up of 21 (IQR 15–32) months, 9 out of 20 patients (45%) have discontinued biologics, and no indication of relapse was observed on echocardiography of all patients.
Discussion
Our findings suggest that perioperative treatment with biologics in patients with AR caused by BS, both initiated preoperatively and within 3 months postoperatively, could significantly decrease the incidence of postoperative PVL and the risk of reoperation. We demonstrated that perioperative biologics could effectively reduce GC and immunosuppressant doses in a short period. To the best of our knowledge, this is the first study reporting the effectiveness and safety of biologics for the treatment of AR caused by BS during the perioperative period.
AR is one of the most commonly reported cardiac manifestations caused by BS with unknown pathophysiology, especially in Asian patients.11,19,28 It is associated with a significantly high incidence of life-threatening postoperative complications, leading to an increased risk of reoperation and mortality. Jeong et al. 13 showed that the overall mortality rate in BS patients with severe AR who underwent surgical intervention was high (47.3%) during the mean follow-up period of 77.4 ± 68.1 months, which is consistent with the low 5-year survival rate (45%) reported in BS patients who underwent cardiovascular surgery without postoperative immunosuppression. 14 The treatment of AR caused by BS is challenging due to the high risk of surgical complications, and the difficulties in early diagnosis.
Severe AR can be the initial manifestation in one third of patients with BS. 29 Thus, most patients with AR attributable to BS failed to meet the classification criteria of BS before surgery,16,30 leading to delayed diagnosis and treatment.8,9 Many patients were diagnosed after experiencing multiple surgical complications (65% in our study). Meanwhile, some patients with AR due to BS are asymptomatic, or their cardiovascular manifestations are insidious. Therefore, echocardiography may play a critical role in the early identification of AR caused by BS. 20
PVL is one of the major, severe, postoperative complications developed in 47–51.4% of patients with severe AR due to BS after cardiac surgical intervention, which results in reoperation according to previous reports.12,17 The rate is much higher than the 1.0% incidence of 2-year PVL in patients with infective endocarditis who underwent AV replacement. 31 More than 70% of patients who developed PVL after cardiac surgery progressed to reoperation or fatal events, 32 and the risk is even higher in patients with BS. Therefore, there is calling for the improvement of the management strategy for patients with AR due to BS.
The etiopathogenesis of the high incidence of PVL in AR due to BS remains unclear. Our histopathological findings and other reports revealed the infiltration of inflammatory cells, myxoid degeneration, micro-abscess formation, and extensive endothelial loss, indicating vasculitis and aortitis that causes fragility and vulnerability of the AV and aortic wall, which contributed to the development of PVL.13,14 Meanwhile, elevated preoperative inflammatory markers (ESR and CRP) and CRP to albumin ratio are associated with increased risk of PVL and mortality in patients with AR after cardiac surgery,12,14,17 further enhancing that it is critical to control inflammation during the perioperative period.
There is no firm evidence on the management strategy of AR in BS so far. Some studies have indicated that perioperative usage of GCs and immunosuppressants, such as azathioprine and cyclophosphamide, might effectively prevent postoperative PVL and reoperation.8,12,13 Theoretically, surgery should be postponed until inflammation is under control. However, the disease progression of AR in BS may occur in an emergent or urgent condition that requires urgent or semi-elective surgery. However, conventional immunosuppressive therapy takes months to induce remission. Also, postoperative immunosuppressants are ineffective in controlling disease activity due to the short interval between surgical intervention and the development of PVL (median 3.5 months).12,17
Our previous studies and other studies in the literature reported series of vascular BS patients successfully treated with biologics, including TNFα inhibitors (IFX, ADA, GOL) and interleukin-6-receptor antagonist (TCZ).33–38 However, the use of biologics on cardiac involvement in patients with BS and the management strategy during surgical intervention has not been clarified and requires further investigation. Our study explored the efficiency of perioperative biologics in preventing postoperative complications and improving the prognosis of AR caused by BS.
For preoperative immunosuppressive therapy, previous studies showed that the median interval of starting conventional immunosuppressants and the first cardiac operation for patients with AR caused by BS was 6 months. 12 Considering the progressive disease, waiting for the treatment to take effect and delaying surgery might add great risk to patients. In our study, the median interval of initiating preoperative biologic treatment and operation was 3.5 months, with effectively decreased inflammatory markers indicating successfully controlled BS disease activity, accompanied by successful short-term GC and immunosuppressant tapering, and decreased postoperative PVL risk. Together, these results suggested that preoperative biologics, concomitant with conventional immunosuppressants, shortened cardiac surgery preparation for patients with AR caused by BS, and lowered the risk of postoperative PVL. Notably, many patients with acute heart failure or other emergency conditions, or diagnosed postoperatively, do not have the chance of receiving preoperative immunosuppressants. Given that insufficient postoperative immunosuppression is associated with the incidence of PVL in AR attributable to BS, 14 effective and rapid control of inflammation with postoperative biologics might be essential for those patients.
Many studies suggest that BS patients with active inflammation have more delayed wound healing at surgical sites than patients without BS. 39 Concerns have arisen regarding the controversial effect of GC and immunosuppressant use during surgical treatment, since they delay the wound-healing process and increase susceptibility to infection.40–42 In this case, with a favorable GC- and immunosuppressant-sparing effect, biologics could effectively and rapidly suppress inflammation and promote the wound-healing process after cardiac surgery.
According to previous reports, the median duration of the development of PVL after surgery was 3.5 months. 12 Therefore, we examined postoperative levels of inflammatory markers (ESR and CRP) at 1 month and 3 months after surgery. As indicated in Figure 3, our results showed that patients with elevated postoperative ESR and CRP had a higher risk of developing PVL, which is consistent with the previous study. 13 Whereas, biologics concomitant with conventional therapies started within 3 months postoperatively normalized ESR and CRP rapidly, and 87.5% of patients were event free during follow up. Thus, biologics should be considered for patients with consistently elevated postoperative ESR and CRP to prevent severe postoperative complications. Together, our study revealed that perioperative biologics efficiently and rapidly suppressed inflammation, which prevented disease recurrence and improved the prognosis of AR caused by BS.
In our study, ileal ulcers and gastrointestinal bleeding were observed in one patient treated with TCZ for 8 months. TCZ has been reported to elevate the risk of lower intestinal perforations in patients with rheumatoid arthritis, compared with treatment with other biologics or conventional immunosuppressants. 43 It was difficult to differentiate whether it was caused by the side effect of TCZ or newly developed intestinal involvement, as the terminal ileum is the most commonly affected area in intestinal BS, 44 and the patient achieved mucosal healing after switching to GOL. The biologics were well tolerated in other patients, and no severe adverse event was observed.
We acknowledge some limitations in this study. First, the number of enrolled patients was relatively small due to the scarcity of AR due to BS treated with biologics. However, this study is already the largest cohort to date. Second, this was started as a retrospective study from a single center that may lead to potential selection bias. Finally, long-term follow up is lacking for some patients recently included. Therefore, a prospective study to confirm the therapeutic benefit of biologics in managing AR caused by BS is warranted.
Conclusion
In conclusion, our study suggests that perioperative biologics concomitant with GCs and immunosuppressants might be a novel strategy for preventing postoperative complications and improving the prognosis of AR due to BS. Perioperative inflammatory markers, ESR and CRP, might be useful indicators in determining the timing of biologic treatment and predicting cardiac surgery prognosis in patients with BS.
Footnotes
Acknowledgements
We gratefully acknowledge all patients who participated in our study.
Authors’ contributions
All authors made substantial contributions to this study. Luxi Sun, Jinjing Liu, Wei Bai, Yunjiao Yang, and Chanyuan Wu acquired the data. Luxi Sun performed the data analysis and drafted the manuscript. Jinjing Liu and Wenjie Zheng provided critical revisions to the manuscript. Zhimian Wang, Jun Zheng and Shangdong Xu also reviewed the manuscript and provided valuable feedback. All authors read and approved the final manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the National Natural Science Foundation of China (grant number 81871299, 81571598); The Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (grant number CIFMS2017-I2M-1-008, CIFMS2016-I2M-1-013); National Key Research and Develop-ment Program: ‘Precise Medical Research’ (grant number 2016YFC0906201).
Ethics approval
The study was approved by the Institutional Review Board of PUMCH. All patients from our center provided written informed consent in accordance with the Declaration of Helsinki.