
Abstract
Behçet disease is a chronic inflammatory systemic disorder, characterized by a relapsing and remitting course. It manifests with oral and genital ulcerations, skin lesions, uveitis, and vascular, central nervous system and gastrointestinal involvement. The main histopathological finding is a widespread vasculitis of the arteries and veins of any size. The cause of this disease is presumed to be multifactorial involving infectious triggers, genetic predisposition, and dysregulation of the immune system. As the clinical expression of Behçet disease is heterogeneous, pharmacological therapy is variable and depends largely on the severity of the disease and organ involvement. Treatment of Behçet disease continues to be based largely on anecdotal case reports, case series, and a few randomized clinical trials.
Introduction
Behçet’s disease (BD) is a multigenetic inflammatory systemic disorder of unknown etiology. Clinical features include oral and genital ulcers, ocular inflammation, skin lesions, as well as articular, vascular, neurological, pulmonary, gastrointestinal, renal, vascular and genitourinary manifestations. The disease may start with one or more of the above symptoms but other symptoms may gradually appear over the years [Arayssi and Hamdan, 2004]. Outside the eye, its course is characterized by recurrent self-limiting episodes of acute inflammation that can lead to significant disability [Sakane et al. 1999].
The disease is present worldwide but its prevalence is the highest in the Middle East, Mediterranean region and Asia. The usual age of onset is around 30 and the male to female ratio varies with the ethnic background [Sakane et al. 1999] (range of male/female patients 1:1–3:1) [Hamdan et al. 2006]. The disease burden of BD is confined to the early years (around 15 years) of its course, and in many patients the syndrome burns out over the years [Kural-Seyahi et al. 2003]. Major vessel disease and central nervous system (CNS) involvement account for most of the deaths seen in this condition and can rarely appear for the first time relatively late in the course of the disease [Kural-Seyahi et al. 2003].
As in most complex diseases, both genetic and environmental factors are implicated in the pathogenesis of BD. Although detailed discussion of the pathogenesis of BD is beyond the scope of this paper, it is important to note the significant strides that have been made in the last decade in understanding its complex genetic architecture. HLA-B51 is by far the strongest associated genetic factor with reported odds ratio (OR) in patients with BD compared with controls ranging from 3.49 to 5.78 [Remmers et al. 2010; Meguro et al. 2010; de Menthon et al. 2009]. Recent data, however, from Italian and Turkish BD cohorts suggest that this association may be explained by a variant located between the HLA-B and MICA genes (OR = 3.88) and not by the HLA-B51 [Hughes et al. 2013].
In addition to HLA-B51, several susceptibility genes within and outside the major histocompatibility complex have been described and are thought to play a role in this complex disease. These include HLA-A26, PSORS1C1 [Hughes et al. 2013], HLA-Cw1602 [Hughes et al. 2013], GIMAP [Lee et al. 2013], UBAC2 [Sawalha et al. 2011], IL10 and IL23-IL12RB2 [Remmers et al. 2010; Mizuki et al. 2010], CCR1/CCR3 [Hou et al. 2012], MEFV and TLR4 [Kirino et al. 2013]. As further understanding of the functional relevance of those genes emerge, new therapeutic targets may be developed to treat the disease in a more specific manner.
Therapeutic options in Behçet’s disease
The main goal of therapy in patients with BD is to induce and maintain remission and improve patients’ quality of life. Selecting treatment is based on the organ involved and the assessment of the severity of the disease. The choice of therapy, however, is limited by the scarceness of high-quality therapy trials and is based largely on case reports, case series and several randomized clinical trials (RCTs) (Table 1).
Randomized controlled trials in Behçet’s disease.
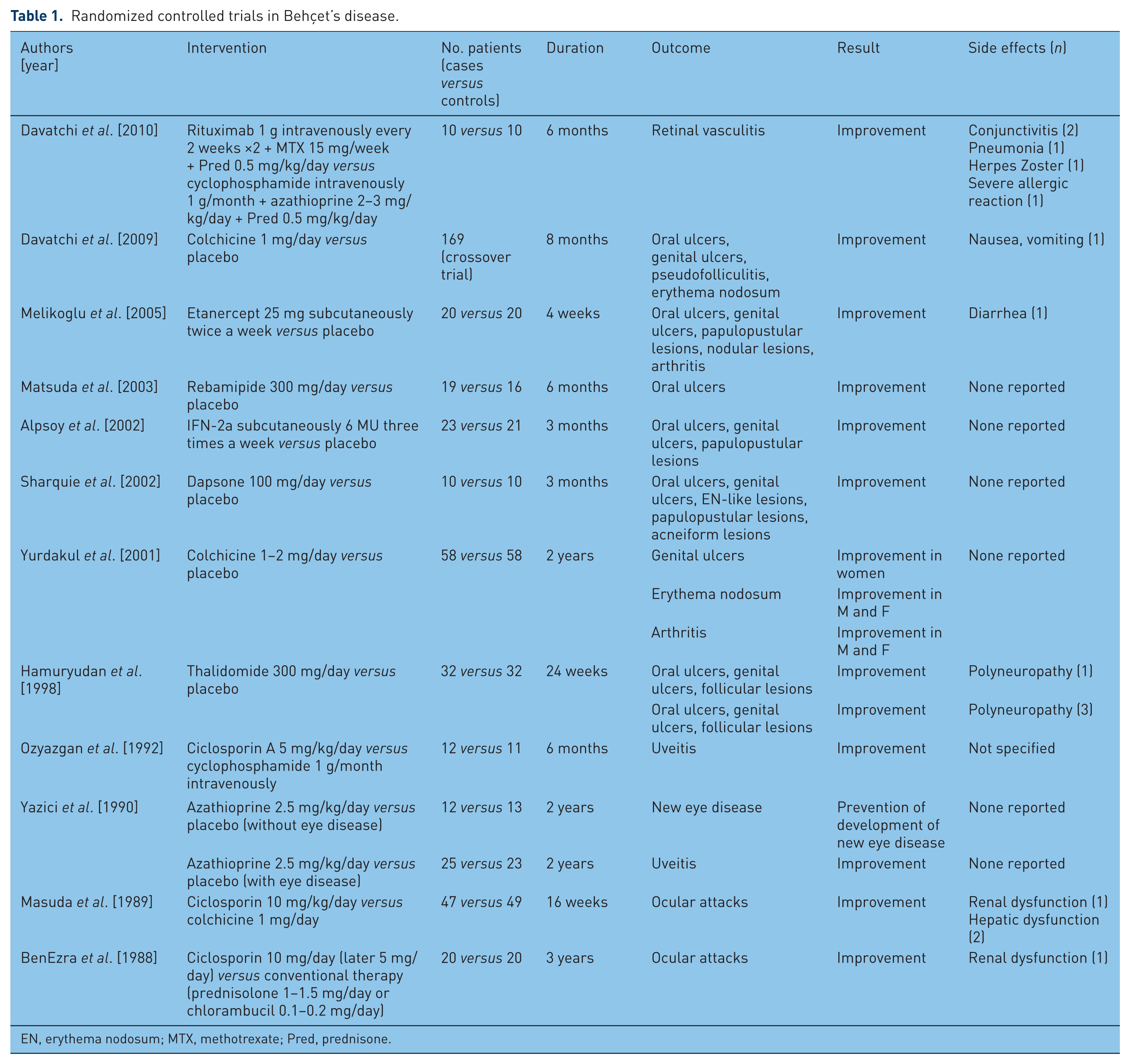
EN, erythema nodosum; MTX, methotrexate; Pred, prednisone.
In this section, we review the different drug classes utilized in the care of patients with BD with special emphasis on the use of biologic agents that provided an important therapeutic advancement for patients with severe or resistant disease (Table 2).
Indications for the use of common therapeutic agents in Behçet’s disease.

EULAR, European League Against Rheumatism; GI, gastrointestinal; RCT, randomized controlled trial.
Biologics and monoclonal therapy
Tumor necrosis factor α inhibitors
Over the last decade, a considerable amount of literature has been published regarding the use of tumor necrosis factor (TNF) inhibitors in BD. Beneficial effects have been noted with infliximab, etanercept, and adalimumab.
Infliximab
Although there are no controlled trials, the existing evidence suggests efficacy of infliximab in treating patients with BD with refractory uveoretinitis, entero-Behçet, neuro-Behçet, vascular BD, and arthritis.
In uveoretinitis, a large number of case reports/series [Munoz-Fernandez et al. 2001; Sfikakis et al. 2001; Capella and Foster, 2012; Alokaily et al. 2010; Olivieri et al. 2008; Takamoto et al. 2007; Merino et al. 2006; Lindstedt et al. 2005; Lanthier et al. 2005; Wechsler et al. 2004; Sayarlioglu et al. 2004a; Rosenbaum, 2004; Giansanti et al. 2004; Falappone et al. 2004; Morris et al. 2003; Gulli et al. 2003; Triolo et al. 2002; Takayama et al. 2013], open-label clinical trials [Okada et al. 2012; Handa et al. 2011; Giardina et al. 2011; Tanaka et al. 2010; Adan et al. 2010; Al-Rayes et al. 2008; Tognon et al. 2007; Niccoli et al. 2007; Accorinti et al. 2007; Tugal-Tutkun et al. 2005; Benitez-del-Castillo et al. 2005; Arayssi et al. 2005; Abu El-Asrar et al. 2005; Sfikakis et al. 2004; Ohno et al. 2004; Cantini et al. 2012; Keino et al. 2011], and nonrandomized comparative studies [Tabbara and Al-Hemidan, 2008; Yamada et al. 2010; Markomichelakis et al. 2011] showed that intravenous infliximab, as single therapy, is effective in inducing prompt suppression of ocular inflammation, decreasing the frequency of uveitis attacks and allowing gradual tapering of corticosteroids (CS). As would be expected, vision of eyes with permanent lesions due to irreversible retinal damage does not improve. The most commonly used dose is 5 mg/kg every 6–8 weeks and repeated infusions are required to maintain long-term remission. The combination of infliximab with azathioprine or cyclosporine A (CsA) or methotrexate (MTX) appears to be superior to infliximab monotherapy for sustained ocular remission [Arida et al. 2011]. Side effects of its use have been reported as mild. Some serious adverse events described include a case of pyomyositis [Morris et al. 2003], one with perianal abscess [Tabbara and Al-Hemidan, 2008] and another with non-Hodgkin’s lymphoma [Giardina et al. 2011].
None of the long-term prospective studies compared treatment with infliximab with any other treatment. However, two retrospective studies compared infliximab with cyclosporine in patients with refractory uveoretinitis [Tabbara and Al-Hemidan, 2008; Yamada et al. 2010]. Both studies found infliximab to be safe and more effective in reducing the number of uveitis flares.
Recently and in a prospective, 4-week, noncomparative pilot study, a single intravitreal injection of infliximab (1 mg/0.05 ml) was given to 15 patients with relapsing posterior uveitis at the onset of a unilateral attack [Markomichelakis et al. 2012]. Eleven patients were receiving additional immunosuppressive treatment or CS and their condition remained stable during follow up. Thirteen patients were naïve to anti-TNF treatment, whereas two patients had received intravenous treatment with infliximab for relapsing ocular inflammation in the past. A beneficial effect was seen on best-corrected visual acuity, anterior chamber cells, vitreous haze, and posterior eye segment inflammation. Ocular or extraocular side effects were not observed. This trial suggested that intravitreal infliximab may be an option for BD-associated relapsing uveitis when systemic TNF inhibitors are contraindicated.
In entero-Behçet, one prospective study evaluated the efficacy of infliximab in patients with severe intestinal involvement [Iwata et al. 2011]. In this trial, 10 patients received infliximab (3-5 mg/kg) administered at 0, 2, and 6 weeks and every 8 weeks thereafter in combination with MTX. All patients had improvement of gastrointestinal symptoms within 4 weeks and in 9 out of 10 ileocecal ulcerations disappeared at 12 months of therapy. No severe adverse effects were observed during the 24 months of follow up. Similar findings were found in several published case series [Maruyama et al. 2012; Lee et al. 2007; Ju et al. 2007; Kram et al. 2003; Travis et al. 2001; Hassard et al. 2001; Naganuma et al. 2008]. Currently, infliximab is approved in Japan for the treatment of entero-Behçet disease.
Infliximab was also administered in patients with neuro-Behçet refractory to high doses of steroids combined with cyclosporine, azathioprine, or MTX [Giardina et al. 2011; Licata et al. 2003; Ribi et al. 2005; Sarwar et al. 2005; Fujikawa et al. 2007; Borhani Haghighi and Safari, 2008; Kikuchi et al. 2008; Pipitone et al. 2008; Abalos-Medina et al. 2009]. The infliximab dose most commonly used was 3–5 mg/kg administered at 0, 2, and 6 weeks and every 6–8 weeks. Overall, results were favorable as most patients had a satisfactory clinical remission and regression of parenchymal lesions on magnetic resonance imaging (MRI).
Similarly, published experience with infliximab for vascular involvement is limited to case reports [Schreiber et al. 2011; Yoshida et al. 2012]. Adler and colleagues reported the largest cohort of vascular BD responding to infliximab [Adler et al. 2012]. They analyzed seven patients, three with aortic involvement, one with recurrent venous thrombosis of the pelvic veins, one with recurrent venous and arterial thromboses of the thigh, and two with retinal vasculitis. Control of inflammation was seen 1–5 days after infliximab induction in all patients. The authors concluded that infliximab is effective in inducing and maintaining remission of vasculitic activity.
Additionally, inflximab was shown to be beneficial in the treatment of BD arthritis. Most of the information regarding its therapeutic efficacy derives from prospective studies evaluating its use for ocular involvement. Arida and colleagues reviewed the efficacy of TNF inhibitors for the treatment of several manifestations of BD, including joint involvement, in 369 patients. They found that joint involvement improved with infliximab in 94%, and remission was sustained in 91% [Arida et al. 2011].
In a similar manner, infliximab was shown to be effective in reducing the various mucocutaneous manifestations of the disease [Chan and Lee, 2012; Aikawa et al. 2011; Kasugai et al. 2010; Lestre et al. 2009; Olivieri et al. 2008; Almoznino and Ben-Chetrit, 2007; Connolly et al. 2005; Takayama et al. 2013; Gulli et al. 2003].
Etanercept
Etanercept is the only TNF inhibitor evaluated in an RCT that demonstrated its efficacy in suppressing most of the mucocutaneous manifestations of BD [Melikoglu et al. 2005]. In this 4-week study, 20 patients received etanercept 25 mg twice a week and 20 received placebo injections. Without suppressing the pathergy reaction, etanercept decreased the frequency of oral ulcers, papulopustular lesions and arthritis with a moderate effect size, and the frequency of genital ulcers and nodular lesions with a small effect size. This trial did not address the effect of etanercept on more serious clinical manifestations of BD.
Only two case reports describe patients with ocular BD treated with etanercept. In the first report, one patient with refractory papillitis and retinal vasculitis despite treatment with azathioprine, cyclosporine, colchicine, and prednisone was reported to have no active disease on fluorescein angiography after 2 months of etanercept treatment. He remained asymptomatic after 1 year on continued treatment with etanercept and low-dose prednisone [Curigliano et al. 2008]. In the second report, the efficacy of etanercept (25 mg twice a week for 6 months) was evaluated in 10 patients with refractory uveitis. All patients had severe ocular inflammation despite combination treatment with CS, azathioprine, and CsA. The addition of etanercept had a beneficial effect in maintaining visual acuity with a concomitant decrease of CS dose. This effect lasted during the whole treatment period but was not sustained in the 6 months post treatment follow up [Sfikakis, 2002].
Adalimumab
Based on case reports [Mushtaq et al. 2007; Takase et al. 2011; Adan et al. 2010] and retrospective case series [Bawazeer et al. 2010], adalimumab 40 mg subcutaneously every 2 weeks appears to be effective in BD uveitis. In the largest study published to date regarding the use of adalimumab in ocular BD [Bawazeer et al. 2010], 17 out of 21 eyes had improvement of visual acuity by more than three lines. This improvement was noticed after an average period of 4 weeks. Adalimumab was also found to have a CS-sparing effect. The steroid dose was reduced by 43% in 10 of 11 patients and was stopped completely in three patients. Similarly, the doses of azathioprine and cyclosporine were reduced in most of the patients and discontinued in 6 out of 10 patients.
Information on the response of extraocular manifestations is provided by a number of case reports [Atzeni et al. 2010; Olivieri et al. 2009; De Cassan et al. 2011; Ariyachaipanich et al. 2009; Belzunegui et al. 2008; Lee et al. 2010] and retrospective chart reviews [Perra et al. 2012]. Overall, the results were favorable. Adalimumab was beneficial in treating leg and recalcitrant genital ulcers [Atzeni et al. 2010; Olivieri et al. 2009; Perra et al. 2012], steroid-dependent ileocolitis [De Cassan et al. 2011; Ariyachaipanich et al. 2009], cerebral vasculitis [Belzunegui et al. 2008], and life-threatening bilateral pulmonary artery aneurysms [Lee et al. 2010]. Adalimumab use also allowed the reduction in the number and dose of standard immunosuppressive agents in most of these cases.
Data on the efficacy of switching amongst anti-TNF inhibitors is only available for patients transitioning from infliximab to adalimumab. In those patients, adalimumab was effective in maintaining disease remission and visual acuity in patients who had to switch due to difficulty in attending infusions (three patients) [Mushtaq et al. 2007], anaphylactoid infusion reaction (one patient) [Takase et al. 2011], relapse after discontinuation of infliximab (two patients) [Adan et al. 2010] or lack of response to infliximab (one patient) [Bawazeer et al. 2010].
Additionally, a prospective, longitudinal, observational study showed that switching from infliximab to adalimumab, due to lack or loss of efficacy or infusion reactions, was successful regardless of the reason for switching [Olivieri et al. 2011].
Rituximab
Sadreddini and colleagues reported the first case of retinal vasculitis in BD treated successfully with rituximab [Sadreddini et al. 2008]. Prior to rituximab, the patient had developed an allergic reaction to etanercept and had no significant amelioration in visual acuity after 2 months of treatment with azathioprine and steroids. Treatment with two doses of rituximab 1 g/dose given 15 days apart led to significant improvement in ophthalmic vasculitis and visual acuity during 6 weeks with no relapse after the steroid-tapering period.
More recently, a pilot randomized, single-blind study compared rituximab with cytotoxic therapy for patients with refractory ocular BD [Davatchi et al. 2010]. Patients in the rituximab arm received two infusions of 1 g, 15 days apart, along with methotrexate and prednisolone. The cytotoxic combination therapy arm received intravenous cyclophosphamide 1000 mg monthly, azathioprine, and prednisolone. Ten patients were enrolled in each arm. The total adjusted disease activity index, the primary endpoint, improved significantly in the rituximab group, but not in the cytotoxic therapy group. In terms of secondary endpoints, posterior uveitis, retinal vasculitis, and the total inflammatory activity index improved in both groups, but more so in the rituximab group than in the cytotoxic therapy group. Mean visual acuity declined slightly in both groups (though not statistically significantly). These results are promising but long-term study on a larger series of patients comparing rituximab with proven efficacious therapy for ocular BD is warranted.
Other biologics
Interleukin 1β (Il-1β) inhibition therapy has been evaluated in the treatment of various manifestations of BD.
An open-label pilot study evaluated the efficacy of a single infusion of gevokizumab, a recombinant humanized anti-IL-1β antibody, in seven patients with acute posterior or panuveitis, or retinal vasculitis [Gul et al. 2012]. These patients had disease that failed to respond to azathioprine or CsA, and were receiving 10 mg/day or less of prednisolone. Gevokizumab was associated with rapid and durable clinical response in all patients. Complete resolution of intraocular inflammation was achieved in 4–21 days, with a median duration of response of 49 days.
Canakinumab, a fully human anti-IL-1β antibody, was effective in treating one patient with BD with resistant panuveitis and retinal vasculitis [Ugurlu et al. 2012]. The patient’s condition had failed to respond to multiple immunosuppressive and biologic agents that included azathioprine, CsA, interferon (IFN), infliximab, adalimumab, and anakinra. Following a single dose of subcutaneous canakinumab 150 mg, eye inflammation resolved and the patient remained attack free for 8 weeks.
In another report, canakinumab was administered for the treatment of resistant fevers, recurrent oral and genital aphtosis, arthritis, ileocolic ulcers, and persistently elevated inflammatory markers in one patient who was unresponsive or intolerant to prednisone, several disease-modifying antirheumatic drugs (DMARDS), etanercept, infliximab, and anakinra. Canakinumab 150 mg every 8 weeks proved efficacious in achieving a prompt and complete disease response without evidence of any adverse events. At 6-month follow up, the patient was fever and symptom free, and serum amyloid A concentration remained stable within the normal range [Cantarini et al. 2012].
Anakinra was also reported to be successful in treating one patient with BD with recurrent fevers, oral and genital ulcers, colonic involvement, arthralgia, and elevated inflammatory markers [Botsios et al. 2008] who was unresponsive to prednisone and several immunosuppressive agents. Within 7–10 days of initiation of anakinra 100 mg/day, there was dramatic resolution in fever, marked improvement in oral and genital ulcers, and decrease in inflammatory markers. After 20 months of using anakinra (100 mg/day) and prednisone (5 mg/day), the patient remained disease free.
Data on the efficacy of IL-6 inhibition using tocilizumab are conflicting. It has been reported to be effective in the treatment of two patients with refractory neuro-Behçet [Urbaniak et al. 2012; Shapiro et al. 2012]. The first patient presented with progression of myelitis despite 4-weekly infusions of infliximab in combination with glucocorticoids and azathioprine. The second patient presented with recurrent meningo-encephalitis manifested by headaches and fever, and had disease resistant to several DMARDS, IFN, daclizumab, cyclophosphamide, and infliximab. Treatment with tocilizumab 8 mg/kg every 4 weeks resulted in a satisfactory increase in the walking distance in the first case and in total remission of symptoms in the second case.
Similarly, in one patient with recurrent oral ulcers, erythema nodosum, and posterior uveitis resistant to DMARDS and infliximab, tocilizumab 8 mg/kg every 4 weeks [Hirano et al. 2012] was effective. The treatment, as monotherapy, suppressed the patient’s clinical manifestations, including ocular attacks, for 1 year and improved her visual acuity.
However, tocilizumab did not show any benefit in two patients with BD with mouth and genital ulcers [Diamantopoulos and Hatemi, 2013]. In both patients, treatment with prednisone, colchicine, several immunosuppressive agents, etanercept, and infliximab led to either short efficacy or side effects. One patient had a deterioration of mouth and genital ulcers after the first infusion of tocilizumab. The other patient had recurrence of the painful genital ulcers immediately after her third infusion necessitating treatment with steroid and high doses of opioid analgesics.
Although both IL-6 and IL-1β are intimately involved in the pathogenesis of BD [Zhou et al. 2012], the routine use of their inhibitors in clinical practice should be guided by future studies.
Interferon α
IFNα has shown benefit in treating mucocutaneous, articular, and ocular manifestations of BD.
One RCT [Alpsoy et al. 2002] and several open studies [Boyvat et al. 2000; O’Duffy et al. 1998; Georgiou et al. 1998; Azizlerli et al. 1996; Alpsoy et al. 1994] showed IFNα to be effective for the management of the mucocutaneous lesions. The 3-month RCT showed that IFNα-2a at a dose of 6 MU subcutaneously three times weekly significantly decreased the duration and pain of oral ulcers, and the frequency of genital ulcers and papulopustular lesions compared with placebo. It also reduced the severity and rate of recurrence of attacks of eye disease. All symptoms, however, returned to pretreatment level after stopping the drug.
There are no RCTs evaluating the efficacy of IFNα in eye involvement. In an uncontrolled, prospective study, 50 patients with refractory ocular BD were each treated with 6 MU of IFNα-2a tapered according to a preset schedule [Kotter et al. 2003]. The ocular response was 92%. Retinal infiltrates resolved after 2–4 weeks in all patients, and remission in affected eyes was reached by week 24. Forty percent of the patients remained disease free of all medications at 30 months of follow up. The same study showed that, whereas extraocular manifestations such as genital ulcerations, arthritis, and skin lesions remitted with IFNα, only 36% of the oral ulcers responded [Kotter et al. 2004b]. Similarly, several other open and retrospective studies showed IFNα to be beneficial in ocular BD [Onal et al. 2011; Sobaci et al. 2010; Deuter et al. 2010; Bodaghi et al. 2007; Tugal-Tutkun et al. 2006; Deuter et al. 2004; Krause et al. 2003; Calguneri et al. 2003; Hamuryudan et al. 2002; Wechsler et al. 2000; Yalcindag and Uzun, 2012].
A systematic review conducted in 2004 included data on IFNα treatment published between 1986 and 2002 [Kotter et al. 2004a]. In 32 articles and 4 abstracts analyzed, 338 patients were treated with IFNα. Eighty-six percent of the patients with mucocutaneous symptoms, 96% with arthritis, and 94% with uveitis exhibited a partial or complete response. Long-term remission after cessation of IFNα therapy was noted in almost 60% of patients.
Finally, IFNα has been used in severe cases of parenchymal neurologic involvement, although the data for its efficacy in such conditions are limited to case reports [Nichols et al. 2001; Kuemmerle-Deschner et al. 2008; Chroni et al. 2008; Calguneri et al. 2005; Monastirli et al. 2010].
Side effects of this drug include an influenza-like syndrome occurring within several hours after administration, myelosuppression, transaminitis, alopecia, and interstitial nephritis. Patients should be screened for depression prior to initiation of therapy.
Apremilast
In a recent double-blind placebo-controlled trial [Melikoglu et al. 2013], apremilast, an oral phosphodiesterase 4 inhibitor used at 30 mg orally twice daily, was effective in reducing oral ulcers in patients with BD compared with placebo. For the few patients with genital ulcers (n = 16), aprelimast was superior to placebo. Side effects noted included one case of reversible diplegia and one case of anal fissure with hemorrhoids out of 50 patients treated with apremilast.
Traditional treatments
Corticosteroids
Although high-quality placebo-controlled trials with CS are lacking, these agents are commonly used in BD. In the only controlled study of CS, 86 patients with BD who had active disease with genital ulcers were randomized to receive either intramuscular CS injections (40 mg methylprednisolone acetate) or placebo every 3 weeks for 27 weeks [Mat et al. 2006]. At the end of the trial, no significant differences in the mean number of genital and oral ulcers, or folliculitis between groups were found. However, the mean number of erythema nodosum lesions was significantly less in the corticosteroid group. The side effects described as a response in the questionnaire at each visit were similar in the CS and placebo arms and these events were mild. The mean body weights of corticosteroid- and placebo-treated patients were 65.1 ± 10 and 65.6 ± 10 kg respectively at the last visit, which were not different from the baseline in both groups.
Despite the absence of RCTs, the European League Against Rheumatism (EULAR) recommends early initiation of CS for the management of severe or life-threatening manifestations, such as ocular, vascular, gastrointestinal, or neurologic disease [Hatemi et al. 2008]. In such instances, pulse dose steroids (1 g intravenous methylprednisolone infusions daily) are often used for 3 days, followed by 1 mg/kg/day prednisolone tapered slowly.
Nonsteroidal anti-inflammatory drugs
Nonsteroidal anti-inflammatory drugs (NSAIDS) are commonly used by rheumatologists to treat joint pains in patients with BD. One RCT compared the NSAID azapropazone 900 mg/day given for 3 weeks with placebo in patients with BD presenting with acute arthritis of less than 10 days’ duration [Moral et al. 1995]. Although the visual analogue scale for pain during the first week was less in the azapropazone group, at the end of the trial the arthritis persisted in 53.5% (15/28) of the patients on azapropazone and in 41.3% (12/29) of those on placebo, which was not statistically significant.
In an open-label study, 30 patients with BD were treated with oral indomethacin 25 mg four times daily for 3 months [Simsek et al. 1991]. At the initiation of therapy, 28 patients had oral aphthous lesions, 23 had joint involvement, 13 had genital ulcerations, 8 had cutaneous lesions, and 4 had eye involvement. Eighty-eight percent of patients with skin lesions, 80% with joint involvement, 43% with oral aphthous lesions, and 38% with genital ulcerations responded to indomethacin therapy. No serious adverse reactions were observed. Only three patients developed nausea, anorexia, and abdominal pain that resolved when indomethacin was changed to a suppository form. Thus, NSAIDS may be effective in treating pain in some patients who have BD-related arthritis.
Colchicine
Colchicine is the most frequently prescribed medication for the treatment of mucocutaneous manifestations of BD. Three RCTs have evaluated this agent. The first study was a 6-month, placebo-controlled study including 14 male patients in each group. Colchicine improved arthralgias and erythema nodosum in young male patients, but had no effect on mucocutaneous lesions [Aktulga et al. 1980]. The second study was a 2-year study that randomized 116 patients to either colchicine or placebo. Colchicine was shown to reduce recurrence of genital ulcers in female patients with BD, in treating arthritis, and preventing erythema nodosum lesions in both men and women [Yurdakul et al. 2001]. Neither study showed beneficial effect of colchicine on oral ulcers. In the third randomized, double-blind, placebo-controlled crossover trial, 169 patients with BD without major organ involvement were selected consecutively. The overall disease activity as well as the oral and genital aphthosis, pseudofolliculitis, and erythema nodosum improved significantly with colchicine but not with placebo [Davatchi et al. 2009].
Based on the above randomized controlled trials, colchicine is effective in the treatment of joint symptoms as well as in the management and prevention of erythema nodosum. Clinical observations, however, suggest that there might be a subgroup of patients with oral ulcers who might benefit from this treatment [Mizushima et al. 1977] and thus the drug should be considered for this indication. The lack of confirmation of colchicine’s efficacy for treatment of mucocutanous lesions could be related to relative lack of power of the studies or to inappropriate study design. A subgroup of BD with oral ulcers might indeed be responsive to colchicine, and a withdrawal study among the responders is helpful to show whether colchicine is beneficial for the treatment of oral ulcers in this subset [Hatemi et al. 2009].
Azathioprine
Ocular disease
There is only one RCT that evaluated azathioprine in BD [Yazici et al. 1990]. In this 2-year trial, 73 patients with and without ocular involvement were treated with glucocorticoids and either azathioprine or placebo. Azathioprine proved to be superior to placebo in decreasing the number of uveitis attacks [number needed to treat (NNT) = 4; 95% confidence interval (CI) 2.1–16.3] and in preserving visual acuity. It also decreased the development of new eye disease among patients with BD without eye involvement (NNT = 2; 95% CI 1.2–4.4) and was effective in preventing the development of new genital ulcers, arthritis, and thrombophlebitis. A 7-year follow up of these patients [Hamuryudan et al. 1997] demonstrated that patients originally allocated to the azathioprine group had less blindness (NNT = 4; 95% CI 1.9–43.9) and less development of new eye disease (NNT = 3; 95% CI 1.3–3.3). More recently, a retrospective study [Saadoun et al. 2010] evaluated the efficacy of azathioprine combined with prednisolone in 157 consecutive patients with BD with active posterior uveitis or panuveitis. After a mean follow up of 71.5 months, 93% of the patients had either partial or complete response.
Thus, azathioprine and CS are recommended as the initial therapy for all patients with BD with inflammation of the posterior segment of the eye [Hatemi et al. 2008]. Testing for thiopurine methyltranferase activity should be considered prior to initiating treatment with azathioprine [Zhou, 2006].
Vascular disease
There are no controlled trials evaluating the efficacy of azathioprine in patients with vascular manifestations of BD. Nevertheless, patients in the treatment group of the above-mentioned RCT [Yazici et al. 1990] developed less vascular disease compared with the placebo group, suggesting that the drug may be beneficial in the treatment of this complication. Thus Hatemi and colleagues suggest the use of azathioprine 2.5 mg/kg/day for the treatment of acute venous thrombosis of the extremities and for maintenance therapy in the management of patients with peripheral and pulmonary artery aneurysms [Hatemi et al. 2008].
Entero-Behçet and neuro-Behçet
The largest series on the use of azathioprine in entero-Behçet is reported from a multidisciplinary BD clinic in Turkey. In the 51 patients who were diagnosed with entero-Behçet, the presenting symptoms were perforation in 4, massive bleeding in 8, and abdominal pain or diarrhea in 39 patients. Thirty-three patients were prescribed azathioprine (2–2.5 mg/kg/day) as first-line therapy. Twenty-two of these 33 patients (67%) had complete remission and no relapses during a mean follow-up period of 44.3 ± 46.9 months. Also, three-quarters of patients who used azathioprine after nonresponse to 5-aminosalicylic acid derivatives went into remission [Hatemi et al. 2013], suggesting that azathioprine may be efficacious in the management of the various manifestations of entero-Behçet.
In a similar manner, there are no RCTs evaluating the use of azathioprine in patients with CNS involvement. Large series suggest a beneficial effect when the prognosis of patients treated in the pre versus post azathioprine era is compared [Kurtuncu et al. 2008].
Mycophenolate mofetil
Only one study evaluated prospectively the efficacy and safety of mycophenolate mofetil (MMF) in mucocutaneous manifestations of BD. The trial was discontinued due to lack of efficacy in the first six patients [Adler et al. 2001]. More recently, a case series reported on four patients with parenchymal neuro-Behçet treated with MMF at a dose of 2 g/day [Shugaiv et al. 2011]. While treated with MMF, all patients remained relapse free during 3–7 years of follow up. These results suggest that MMF could be an alternative drug in parenchymal neuro-Behçet but not in mucocutaneous disease. Large controlled studies are needed for verification of these results.
Cyclosporine A
Several trials suggested that cyclosporine may have a beneficial effect on the ocular manifestations of BD. Three RCTs have been published comparing CsA with cyclophosphamide in one [Ozyazgan et al. 1992], colchicine in the second [Masuda et al. 1989], and conventional therapy (steroid or chlorambucil) in the third [BenEzra et al. 1988]. In the first trial, CsA produced a rapid and significant improvement in visual acuity over the first 6 months [Ozyazgan et al. 1992]. However, this effect was not sustained at 2 years. When CsA was compared with colchicine, the frequency and severity of ocular attacks decreased [Masuda et al. 1989] in the CsA group compared with colcichine. In the third RCT, the visual acuity improved in most patients after 1-year follow up and remained stable or improved from baseline after 3 years [BenEzra et al. 1988]. All other noncontrolled trials also supported the efficacy of CsA in eye disease [Ermakova, 2003; Ozdal et al. 2002; Fujino et al. 1999; Sullu et al. 1998; Whitcup et al. 1994; Sajjadi et al. 1994; Pacor et al. 1994; Hayasaka et al. 1994; Atmaca and Batioglu, 1994; Chavis et al. 1992; Nussenblatt et al. 1985; Diaz-Llopis et al. 1990; Binder et al. 1987; Wechsler et al. 1986; Muftuoglu et al. 1987]. Currently, cyclosporine is considered one of the therapeutic options for refractory or severe eye disease defined as more than two lines of drop in visual acuity on a 10/10 scale or retinal disease (retinal vasculitis or macular involvement) [Hatemi et al. 2009].
For physicians taking care of patients with BD, the decision to use cyclosporine has to be counterbalanced with the risk of developing neurotoxicity. Three case–control studies reported an increased frequency of neurologic involvement among patients with BD treated with CsA [Kotter et al. 2006; Kotake et al. 1999; Kato et al. 2001]. Compared with nonusers, those who used cyclosporine had an OR for developing serious neurological involvement of 9.9 (95% CI 3.9–25.2) [Kotter et al. 2006], over 79 (95% CI 7.9–620) [Kotake et al. 1999], and 6.8 (95% CI 0.8–60) [Kato et al. 2001]. It is unclear whether these findings are confounded by indication [Hatemi et al. 2013], as there is an association between neurologic involvement and eye involvement, the main indication for the use of cyclosporine in BD. However, a large retrospective series compared patients, matched for severity of eye involvement, who used CsA (group 1, 92 patients) with those who used other immunosuppressants (group 2, 132 patients), and colchicine (group 3, 45 patients) and did not use CsA. The frequency of parenchymal neurologic involvement was significantly higher in the first group (eight cases) compared with the other two groups (one case in each), suggesting that cyclosporine is truly associated with an increased risk of neurologic disease. EULAR guidelines recommend that CsA not be used in patients with BD with CNS involvement unless necessary for intraocular inflammation [Hatemi et al. 2008].
In addition to its efficacy in eye disease, CsA might be beneficial for the management of acute deep vein thrombosis (DVT). In one open-label study [Cantini et al. 1999], seven patients with venous thrombosis had complete remission of thrombophlebitis within 2 months without residual venous insufficiency and no recurrences as long as treatment was continued. Oral aphthous ulcers, dermal lesions, and genital ulcerations may also be reduced with the use of CsA [Masuda et al. 1989].
Tacrolimus
Tacrolimus (FK506), a calcineurin inhibitor similar to cyclosporine, may have similar efficacy, but the drug was not tested in an RCT in BD. Open studies showed some benefit for eye involvement.
A multicenter open-label clinical trial assessed the effect of FK506 on 26 patients with BD with refractory uveitis. Uveitis decreased in 60% and visual acuity improved in 32% of the eyes, and did not change in 50%. The effect of FK506 was dose dependent. Renal toxicity was present in four cases, all treated with cyclosporine previously. Thus, special care should be considered with patients treated previously with cyclosporine in whom tacrolimus is to be prescribed [Mochizuki et al. 1991].
Two other clinical trials studied the efficacy of FK506 in BD uveitis and uveitis in other medical conditions. A total of 13 patients (both studies combined) received doses ranging from 0.05 to 0.2 mg/kg/day. A trend showed improvement of the visual acuity, although clinical significance could not be shown due to the small number of patients. The studies also showed that the efficacy as well as the toxicity profile of FK506, like cyclosporine, is dose dependent [Ishioka et al. 1994; Mochizuki et al. 1992].
Cyclophosphamide
The main indications for cyclophosphamide in BD are major vascular and parenchymal neurologic involvement.
There are no RCTs directly addressing the treatment of vessel wall inflammation in BD. Two retrospective studies, published 10 years apart, showed that monthly pulses of cyclophosphamide up to 2 years followed by maintenance treatment with azathioprine resulted in significant decrease in mortality in patients with pulmonary artery aneurysms [Hamuryudan et al. 1994, 2004]. In 2008, the EULAR guidelines suggested that cyclophosphamide be used preferentially for thrombosis of the superior vena cava or Budd–Chiari syndrome that are usually treated more aggressively than peripheral artery aneurysms for which systemic immunosuppressives such as azathioprine could be used [Hatemi et al. 2008].
A 2012 retrospective series described 40 patients with severe neuro-Behçet who presented with meningoencephalitis (48.8% of cases), cerebral deep venous thrombosis (43.6% of cases), and myelopathy (7.7% of cases). All patients were treated with cyclophosphamide 600 mg/m2 of body surface area on day 1, 2, 4, 6, and 8 followed by a bolus of 600 mg/m2 of body surface area every 2 months for 2 years. The 40 patients evolved positively with clinical improvement and good tolerance for cyclophosphamide [Ait Ben Haddou et al. 2012].
A systematic review from the Cochrane database illustrated the lack of efficacy of cyclophosphamide for ocular disease [Saenz et al. 2000]. Currently, the EULAR does not recommend the use of this drug for treatment of any of the ocular manifestations associated with BD [Hatemi et al. 2008].
Thalidomide
Thalidomide is effective in the treatment of orogenital ulcerations in patients with BD. In a 24-week RCT, thalidomide was superior to placebo in decreasing oral and genital ulcers in men with BD [Hamuryudan et al. 1998]. A complete response occurred in 2 of the 32 patients receiving thalidomide, 100 mg/day; in 5 of the 31 patients receiving thalidomide, 300 mg/day; and in none of the 32 patients receiving placebo. The suppressive effect of thalidomide with either dosage was evident at 4 weeks for oral ulcers and at 8 weeks for genital ulcers and follicular lesions. The use of the drug was associated with an increase in erythema nodosum in the first 8 weeks of the study. Four patients developed polyneuropathy as a complication of the treatment. Thus, thalidomide at 100 mg/day is effective for the treatment of orogenital ulcers.
Three other open-label studies using thalidomide showed similar efficacy on orogenital ulcers [Gardner-Medwin et al. 1994; Hamza, 1986; Saylan and Saltik, 1982]. Paresthaesias, somnolence, nausea, vomiting, and skin rash were reported in few of these patients.
Additionally, thalidomide has been reported in several case reports to be helpful in the treatment of BD colitis. Three patients presented with ileocolitis that was resistant to treatment with azathioprine, sulfasalazine, methylprednisolone, cyclophosphamide, or surgical debridement. Thalidomide 100–300 mg/day resulted in complete resolution of their symptoms within a few weeks [Sayarlioglu et al. 2004b; Larsson, 1990; Postema et al. 1996].
Methotrexate
An observational report with MTX showed some benefit in patients with eye involvement [Davatchi et al. 2003]. Weekly high- and low-dose MTX was effective in reducing ocular inflammation in patients with BD, but high doses were more effective.
Two open successive studies involving a small number of patients receiving MTX from the same center suggested beneficial effects in neuro-Behçet [Kikuchi et al. 2003; Hirohata et al. 1998]. In the first study, in which patients were followed for 12 months, there were six patients and in the extension study another four patients were added and treated for up to 4 years. MTX showed stabilization of neuropsychiatric findings, intelligence test, brain MRI scans, and decreased cerebrospinal fluid IL-6 levels. However, patients experienced significant exacerbations 6 months after discontinuation of MTX.
Dapsone
A double-blind placebo-controlled clinical trial, assessed the effect of dapsone in the treatment of mucocutaneous lesions in 20 patients [Sharquie et al. 2002]. Patients were randomly allocated to receive either dapsone 100 mg daily or placebo for 3 months. After 3 months, patients crossed over and followed up for another 3 months. The frequency and duration of oral ulcers and the number and frequency of genital ulcers were significantly decreased in the dapsone group, but not in the placebo group.
Anticoagulation
There are no controlled data to guide on whether anticoagulants should be used in the management of patients with BD with DVT or cerebral venous thrombosis (CVT).
A retrospective study of 37 patients with BD with venous thrombosis compared anticoagulation treatment, immunosuppressive agents, and the combination of immunosuppressive agents and anticoagulation treatment [Ahn et al. 2008]. The most commonly involved sites were the superficial and common femoral veins. Three of the four patients in the anticoagulant-treated group developed new thromboses, compared with 2 of 16 patients in the immunosuppressive agent-treated group and 1 of 17 patients in the combination-treated group, suggesting that immunosuppressive therapy is essential and that anticoagulation therapy may not be required.
In CVT, anticoagulants may be more helpful. In one of the largest series, 62 of 64 patients with BD and CVT were anticoagulated [Saadoun et al. 2009]. Forty-eight of these 62 patients received treatment with steroids (prednisone or equivalent 1 mg/kg/day). This resulted in regression or disappearance of neurologic symptoms within 1 month in 56 of 64 patients. Four patients experienced hemorrhagic complications [psoas hematoma (two cases), leg hematoma (one case), and subdural hematoma (one case)] that recovered without sequelae. This study favored anticoagulation as a safe and effective therapy in patients with BD and CVT.
Additionally, a systematic review identified 290 patients with BD and CVT [Aguiar de Sousa et al. 2011]. This review found that the most frequent therapy used was the association of both immunosuppressant and anticoagulation therapies. Around 90% of these patients were prescribed CS with or without immunosuppressives and 74% were prescribed anticoagulants.
Interestingly, a physician’s decision to use anticoagulants seems to be mostly related to the prevalence of the disease in the country where the physician is practicing. Around 87% of physicians practicing in countries with low to intermediate prevalence of BD anticoagulate their patients with DVT in comparison to only 44% in whom the prevalence is much higher [Tayer-Shifman et al. 2012].
Currently, due to the lack of evidence of benefit with anticoagulant in the management of DVT or arterial lesions in BD, the EULAR does not recommend the use of anticoagulant for this indication [Hatemi et al. 2009]. Further studies attempting to determine the need for anticoagulation for the treatment of venous and arterial thrombosis in patients with BD are clearly needed.
Other therapies
Rebapamide, although rarely used, is an alternative for reducing oral ulcers pain in patients with BD [Matsuda et al. 2003]. Topical treatment with CS, topical anesthetics, antimicrobial mouthwashes, sucralfate [Keogan, 2009] and topical granulocyte colony-stimulating factor [Bacanli et al. 2006] can be helpful in the management of mucocutanous lesions. Additionally, a number of antibiotics and antivirals, based on the possible role of herpes and Streptococcus sanguinis in the pathogenesis of the disease, have been used primarily for the treatment of mucocutaneous manifestations with variable responses [Calguneri et al. 1996a, 1996b; Davies et al. 1988] and thus are not part of the routine care of patients with BD.
Conclusion
The management of patients with BD has evolved considerably over the last decade, with more insight into the better use of older agents and the development of newer remedies such as biologics. Despite that, treatment remains challenging as it continues to be largely based on case reports, case series, and only a few randomized clinical trials. Large, well designed, multicenter trials are still needed to advance our knowledge of this complex syndrome. Newer therapeutic options, including alemtuzumab and hematopoetic stem cell transplantation, are currently being investigated. These efforts will undoubtedly provide insight into optimal treatment.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.