
Abstract
Background:
Underlying muscle weakness and stiffness may increase the risk of developing rotator cuff tendinopathy. This systematic review aims to assess existing prospective studies to summarize whether muscle weakness and stiffness are risk factors for the development of rotator cuff tendinopathy in overhead athletes.
Methods:
A systematic search was performed using PRISMA guidelines. Prospective studies measuring muscle strength or stiffness and the incidence of rotator cuff tendinopathy were included. Quality assessment was performed with the Newcastle-Ottawa quality assessment scale.
Results:
The search yielded six studies, with a total of 523 trained overhead athletes followed up for one season. External rotation (ER) and internal rotation (IR) strength were described as protective factors against the development of rotator cuff tendinopathy. Athletes who did not sustain shoulder injuries had statistically stronger eccentric IR (p < 0.01) and ER (p < 0.05) strength in the pre-season assessment. Muscle stiffness indicated by limited range of motion of <106° for shoulder ER was described as a risk factor with an odds ratio of 1.12 (p < 0.001). Imbalance between ER and IR strength was reported as risk factors for shoulder injuries in two studies, with a relative risk of 2.57 (p < 0.05) reported in one study. Supraspinatus weakness was also reported as a risk factor for shoulder injuries in one study.
Conclusion:
Limited evidence support ER, IR weakness, limited ER range of motion, and very limited evidence support imbalance in ER/IR strength, and supraspinatus weakness as risk factors for rotator cuff tendinopathy in overhead athletes. No existing studies investigated the general population on this topic. Future cohort studies may improve on existing evidence with investigations on the general public, a longer follow-up time, clearly documented injury history, and a stringent diagnosis to rotator cuff tendinopathy.
Background
Rotator cuff tendinopathy is an umbrella term describing pain and loss of function in the rotator cuff tendons. Entities including tendinosis, tendinitis, subacromial impingement, and subacromial bursitis are often regarded under the term rotator cuff tendinopathy. 1 As reported in previous studies, rotator cuff tendinopathy is common among athletes,2,3 having severe impacts on their performance and athletic career.4,5
The pathogenesis of tendinopathy is believed to involve a failed healing process with a multifactorial etiology. 6 Overuse of the rotator cuff tendons was suggested to be one of the factors leading to developing rotator cuff tendinopathy. To explain the association of tendinopathy with overuse, previous studies have demonstrated that tendon loading, in terms of compression or tensile loads, would induce apoptosis and inflammation in tendon cells.7,8 An increased activity level would increase tendon loading. However, the fact that athletes with similar training load present inconsistently with tendinopathy suggest that some factors may play a role in the modulation of tendon loading under given training load.
Muscle weakness may be a factor modulating tendon loading. This is a relative term referring to the failure to generate a desired or expected force. 9 The mechanism of how weakness in rotator cuff muscles may lead to rotator cuff tendinopathy has been hypothesized by multiple groups. As suggested by previous literature, rotator cuff muscles counteract the deltoid to prevent humeral head elevation. 10 Without the rotator cuff, humeral head elevation will decrease the size of subacromial space, increasing the risk of supraspinatus impingement. 11 The reduction of subacromial space in patients with rotator cuff tendinopathy was also demonstrated by a previous retrospective study. 12 Another study suggested that external rotation strength is crucial for the deceleration of arm swinging movements. 13 Its weakness in athletes with repetitive forceful arm swings was hypothesized to lead to strains and tears in the tendon. 14
Muscle stiffness was also suggested to lead to muscle weakness via reciprocal inhibition from a tight antagonist. 10 Stiffness of the upper trapezius muscle was demonstrated in patients with rotator cuff tendinopathy. 15 There is a possibility that muscle stiffness of the shoulder may be one of the causes leading to muscle weakness and the development of rotator cuff tendinopathy. Muscle stiffness could be detected with ultrasound elastography, or by physical examination demonstrating a limited range of motion of the shoulder.15,16 However, it has to be acknowledged that other causes such as osteoarthritis or frozen shoulder may also lead to reduced range of motion. 16
In summary, expert opinion suggests that muscle weakness and stiffness may lead to an increased risk of developing tendinopathies.17,18 This suggestion has been supported by several authors reviewing retrospective and cadaveric studies.12,19–22 However, as these parameters are readily influenced by the presence of pain, the association between muscle weakness or stiffness and the development of tendinopathy is yet to be established.
Purpose of this review
This review aims to examine existing prospective studies on identifying the association between muscle weakness or stiffness, and rotator cuff tendinopathy in athletes. Muscle weakness would be identified by direct measurements of muscle strength, while associated factors like muscle stiffness may suggest a cause to the underlying muscle weakness.
Methods
A systematic search was carried out in PubMed, CINAHL, and Scopus from inception to 13 May 2020. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statements was used as a guideline in the performance of the systematic review. 23 Our study was registered to the PROSPERO database, under the registration number CRD42020197927. The searched keywords are shown in Table 1. Supplementary searches were carried out by hand searching the reference lists of the included studies.
Search terms used.

Eligibility criteria
Clinical studies were included if all of the following criteria are met: (a) prospective data containing the measurement of muscle strength or muscle stiffness were documented; (b) Incidence of tendinopathy was documented; and (c) Patients were described to have rotator cuff tendinopathy/tendinosis/tendinitis/tear, or subacromial impingement/bursitis. A study was excluded if (a) patients were treated with any interventions, or (b) the study was an animal study.
Study selection and data collection
Studies from the systematic search were merged in EndNote X9 (Thomson, New York, NY, USA), with duplicates removed. Application of exclusion and inclusion criteria was performed by screening the titles and abstracts, followed by retrieval of full texts of included studies. Two reviewers (CKK and MCK) independently screened all the titles, abstracts, and reviewed the studies for inclusion. Disagreements were resolved by consensus between two reviewers. A third reviewer (FSC) was available to resolve further disagreements. A PRISMA-flowchart of the selection process is shown in Figure 1.
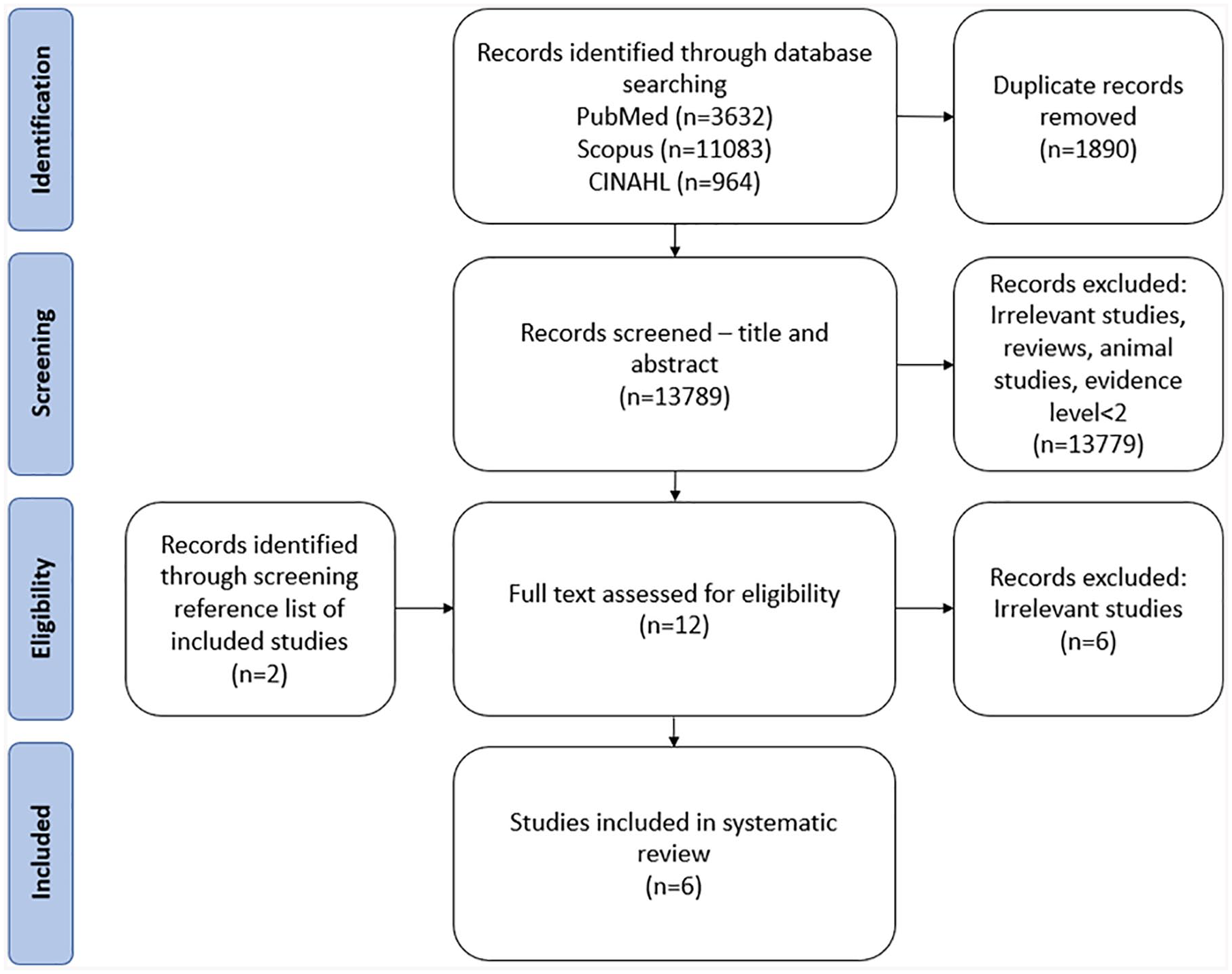
PRISMA flow diagram of the search strategy is shown.
Assessment of study quality and risk of bias in individual studies
The Newcastle-Ottawa quality assessment scale was used to assess the quality of included studies. Out of a full score of 9, studies scoring ⩾7 indicates high methodological quality, 6 indicates intermediate quality, and ⩽5 indicates low quality. The assessment of study quality was performed in a standardized manner independently by two reviewers (CKK, MCK). Disagreements were resolved by consensus between the two reviewers. A third reviewer (FSC) was available to resolve further disagreements. Inter-rater reliability with Cohen’s kappa was calculated using SPSS Version 20 for Windows (SPSS Inc., Chicago, IL, USA).
Results
Studies included
The systematic search resulted in 13,789 studies, which 663 were suitable for abstract review. Results were further screened down to 12 studies for full text review; 6 studies were included while the remainder were excluded as the topic of investigation was not rotator cuff tendinopathy, or prospective measurements of muscle weakness or stiffness were not documented.
The six included studies prospectively documented muscle weakness or stiffness, and the incidence of rotator cuff tendinopathy in 523 participants (Table 2). By the end of follow up, 105 participants developed shoulder injuries, of which 70 were diagnosed as rotator cuff tendinopathy. However, statistical association between muscle weakness or stiffness, and the incidence of tendinopathy was only calculated in two out of the six studies.24,25 The remaining studies demonstrated the association between muscle weakness or stiffness against shoulder injuries in general.26–29 The documentation of previous injuries was also inconsistent. Of the two studies which documented previous injuries, 19 out of 24 cases of shoulder injuries had an injury history. All included studies had a follow-up period of one season, approximately 6 months depending on the schedule of specific leagues. The studied population of all six studies were trained overhead athletes participating in either volleyball,24,28 baseball,25,29 or handball.26,27 Exact training load, in terms of hours per week, was not comparable due to inconsistent documentation among studies. Participants were free of shoulder pain at the beginning of studies, but other aspects of the past medical history were not documented. The diagnosis of tendinopathy also varied among the studies. Four studies did not provide the diagnostic criteria of rotator cuff tendinopathy,26–29 while two studies described the diagnosis to be made clinically and confirmed with radiological evidence.24,25
Summary of extracted data.

All studies included athletes with a training load of >7 h/week.
Age: 18–30 young adult, 30–40 adult, 40–60 middle age, >60 elderly.
Cases of tendinopathy are included in the “total shoulder injuries” column.
+, factor is reported to be a significant risk factor; −, factor is reported to be an insignificant factor; ER, external rotation; IR, internal rotation; n/a, factor not assessed in the study.
Methodological quality assessment
The results of quality assessment with the Newcastle-Ottawa scale for cohort studies are included in Table 3. Among six included studies, there were four of high methodological quality, and two with low quality. The criteria regarding the “demonstration of an absence of the outcome of interest at the start of the study” was not fulfilled in any included studies, as the absence of rotator cuff tendinopathy was only recorded from self-reporting questionnaires, without the support of clinical or radiological testing. Inter-Rater Reliability with Cohen’s Kappa was calculated as 0.899, indicating excellent inter-rater agreement between the two reviewers.
Methodological quality assessment using the Newcastle-Ottawa scale for cohort studies. a

+, point given for this category; −, point not given for this category.
The Newcastle-Ottawa Scale for cohort studies:
1. Representativeness of the exposed cohort
2. Selection of the non exposed cohort
3. Ascertainment of exposure
4. Demonstration that outcome of interest was not present at start of study
5. Study controls for the most important factor
6. Study controls for additional factors
7. Assessment of outcome
8. Was follow-up long enough for outcomes to occur
9. Adequacy of follow up of cohorts
The Newcastle-Ottawa scale for case control studies:
1. Is the case definition adequate?
2. Representativeness of the cases
3. Selection of controls
4. Definition of controls
5. Study controls for the most important factor
6. Study controls for additional factors
7. Ascertainment of exposure
8. Same method of ascertainment for cases and controls
9. Non-response rate
Studies reporting rotator cuff strength or stiffness as risk factors to the development of rotator cuff tendinopathy
One included study discussed isometric internal rotation (IR) and external rotation (ER) strength, as measured with an isokinetic dynamometer, as a protective factor to the development of rotator cuff tendinopathy. 24 It was reported that athletes who did not sustain shoulder injuries had statistically stronger eccentric IR (p < 0.01) and ER (p < 0.05) strength in the pre-season assessment. Upon further analysis with univariate logistic regression models, each 1 N/m increase of eccentric IR and ER strength decreased the risk of shoulder pain by 1% [odds ratio (OR) = 0.946, p = 0.01 and 0.940, p = 0.05]. 24 The significance of muscle stiffness, suggested by limited ER range of motion, hand measured with a goniometer, was reported in one study. 25 An OR of 1.12 (p < 0.001) was reported for a dominant arm ER range of <106°.
Studies reporting rotator cuff strength or stiffness as risk factors to the development of shoulder injuries
Five studies discussed isometric rotator cuff strength, measured with an isokinetic dynamometer, as a possible risk factor to the development of shoulder injuries, of which 70 out of 105 cases were diagnosed as rotator cuff tendinopathy.
In addition to the factors mentioned in the previous section, imbalance between ER and IR strength was mentioned in two studies. However, the definition for muscle imbalance varied. In one study, imbalance was defined as a significant difference between IR and ER strength, with no relative risk (RR) or OR provided. 28 In the other study, a cut off of <69% of ER/IR ratio was adapted, and RR of 2.57 (p < 0.05) was reported for athletes with muscle imbalance. 27
ER and supraspinatus weakness was reported in one study, with no OR or RR provided. 29
Discussion
According to our systematic search, IR weakness, ER weakness, and limited ER range of motion at the glenohumeral joint have been reported to be associated with the development of rotator cuff tendinopathy. Supraspinatus weakness, and imbalance in ER/IR strength have also been reported as a risk factor in the development of shoulder injuries.
Limited evidence support that weakness or stiffness of the rotator cuff muscles are risk factors to the development of rotator cuff tendinopathy
Our findings showed the significance of pre-injury muscle strength and stiffness on the incidence of rotator cuff tendinopathy. The reported risk factors include weakness of the shoulder external rotators, weakness of the internal rotators, and a limited range of motion in external rotation at the glenohumeral joint. It was demonstrated in previous studies that these muscle changes, in the absence of pain, may increase the risk of newly developing rotator cuff tendinopathy in the upcoming season.
Other risk factors such as a low ER/IR ratio and supraspinatus weakness were also mentioned in included studies. Although the significance of these factors was associated with shoulder injuries, rotator cuff tendinopathy made up 70 out of 105 total cases of shoulder injuries included. There is a possibility that the risk factors may also be valid for the development of rotator cuff tendinopathy, but the calculations were unfortunately not commenced in our included studies.27–29
Risk factors were classified into five evidence levels in a previous systematic review on rotator cuff tendinopathy.30,31 Using the same method, limited evidence support weakness or stiffness of rotator cuff muscles as risk factors. Very limited evidence support that a low ER/IR ratio and supraspinatus weakness are risk factors to the development of rotator cuff tendinopathy.
Hypothesis on how muscle weakness may lead to rotator cuff tendinopathy
Tendon loading, in terms of tension or compression to the tendon, is one of the risk factors leading to the development of tendinopathy. This suggestion is supported by previous in vitro studies, demonstrating that tension or compression of tendon cells leads to apoptosis and increased expression of inflammatory markers.7,8,32 As mentioned previously, several mechanisms have been proposed by various groups to explain how muscle weakness may lead to increased loading. Strength in the rotator cuff muscles are crucial in counteracting the deltoid muscle, keeping the humeral head adhered to the glenoid. 10 With weakened or fatigued rotator cuff muscles, humeral head elevation occur, decreasing the size of sub-acromial space, leading to compression of the supraspinatus tendon.11,12 Another possible mechanism was described in a previous study, suggesting that eccentric ER strength play a key role in the deceleration of arm swinging movements. 13 It was illustrated that the requirement for ER strength is increased to effectively decelerate an arm from forceful IR. Muscle imbalance in athletes with repetitive arm swings is hypothesized to cause strains and tears in the tendon. 14
Muscle weakness may not be an isolated problem
Associated factors such as muscle stiffness, posture, and movement patterns may provide more insight into the causes of muscle weakness. Unfortunately, it was demonstrated in our systematic search that the association of these factors to the development of rotator cuff tendinopathy is under-investigated, with only one existing study discussing the significance of shoulder range of motion in the development of rotator cuff tendinopathy. 33 This study demonstrated that limited ER range of the shoulder is associated with the development of rotator cuff tendinopathy. However, whether range of motion was active or passively measured was not described. Limited range in ER may imply stiffness of internal rotators such as pectoralis major, teres major, subscapularis, latissimus dorsi, and deltoid muscles. Considering the concept of reciprocal inhibition, tightness in this muscle group would lead to weakness in muscles for ER, which is also consistent with our results demonstrating that a low ER/IR strength ratio is associated with the development of rotator cuff tendinopathy. 10 This finding provide evidence that muscle weakness is not the only muscle change that may lead to the development of rotator cuff tendinopathy.
Could history of a previous injury be a confounding factor
As shown in Table 1, the history of previous injuries was recorded inconsistently in the included studies. Of the two studies that documented injury history, 19 out of 24 cases of shoulder injury also had a history of previous shoulder injury. However, current evidence is inconclusive whether history of a previous shoulder injury may act as a confounding factor between rotator cuff weakness and the development of rotator cuff tendinopathy.
Rotator cuff tendinopathy was described to be persistent and recurring. 34 However, a previous systematic review on risk factors of rotator cuff tendinopathy have not been able to identify whether a previous injury history is a risk factor for future rotator cuff tendinopathy. 30 Also, rotator cuff tendinopathy is well known to present as shoulder weakness, 35 but little is known on whether a previous injury would lead to residual weaknesses.
One of our included studies attempted to address this issue. 26 According to this latter study, 47% of 108 athletes were documented to have had previous shoulder injury. However, it was shown in the study that previous injury was not a significant risk factor in the development of new injury (p = 0.28). There was also no significant difference in isokinetic results between players with and without previous injuries (p > 0.05). 26
Clinical relevance
Rotator cuff tendinopathy affects a large population, leading to disability and heavy socioeconomic impacts. 36 The results from this study provided an insight on how we may attempt to decrease such burden via primary prevention. It was demonstrated that not only absolute strength, but imbalance in ER and IR strength of the shoulder may contribute to the development of rotator cuff tendinopathy. Therefore, screening programs can be conducted in high risk groups, such as athletes competing in overhead sports. By identifying individuals at a greater risk of developing rotator cuff tendinopathy, specific exercises programs attempting the correction of muscle imbalance could be suggested. There is a possibility that correction of muscle imbalance in existing cases of tendinopathy may also improve symptom control by modifying mechanical load to the tendon. However, its effectiveness on symptom control is yet to be investigated.
Regarding the method to correct muscle imbalance, it is to be acknowledged that a successful protocol would include, but is not limited to, training of the weak muscle. As mentioned in previous sections, muscle tightness would lead to reciprocal inhibition of the antagonist muscle. Attempts to relieve muscle stiffness may augment the effectiveness of training to restore muscle imbalance. This provides a rationale to some existing treatments for tendinopathy, which include eccentric exercises to train weak muscles, and soft tissue release to relax tightened muscles. Systematic reviews on the effectiveness of these treatments alone have shown promising but inconclusive results on symptom relief of tendinopathy.17,37,38 However, the effectiveness of combined treatment of muscle relaxation followed by training have not been investigated in rotator cuff tendinopathy, which opens a direction for future clinical trials.
Limitations
All included studies recruited patients in the athletic population participating in various sports. The situation is not ideal as muscle weakness of stiffness of the rotator cuff may have a varying impact on the development of tendinopathy depending on the specific activity. However, due to the limited number of existing studies, not only that sub-group analysis could not be performed for each sport, whether our finding could apply to the general public is also unclear.
Rotator cuff tendinopathy observed in the included studies presented in a rather sub-acute manner, developing during one season. In comparison, tendinopathy in the general public is more known as a chronic degenerative disease with failed healing. 6 One explanation can be that weakness in the rotator cuff leads to an unfavorable mechanical environment, causing subclinical microtraumas over time. Tendinitis would then develop as an acute on chronic condition from triggers such as an intense competitive season.
This hypothesis is particularly relevant as participants in the included cohort studies were pain-free at the beginning of follow up, but no confirmatory imaging tests were done to confirm the absence of tendinopathy. Muscle weakness or stiffness could therefore be a result of adaptation to painless cases of tendinopathy, which its existence was previously described in a magnetic resonance imaging (MRI) study. 39 The diagnostic criteria of rotator cuff tendinopathy was also not clearly documented in several included studies,26–29 providing a potential source of inconsistency.
Athletes in the included studies also varied in age, gender, and sports participated. These factors may explain the inconsistencies between the results of our included studies.
Future study
With the goal of developing screening programs and to lower injury risk, future studies could further investigate the profile of muscle weaknesses that may lead to rotator cuff tendinopathy. The significance of muscle weakness or stiffness have been investigated only on rotator cuff muscles, while there have been hypothesis that muscles of the spine, chest, and back may also have an impact on shoulder injuries. 40 Results from this review have also pointed out several limitations in the existing cohort studies, and that a future cohort could further improve on the existing evidence with longer follow-up times, clearly documented injury history, and a stringent diagnosis to rotator cuff tendinopathy.
Prospective investigations on muscle stiffness, posture, and movement patterns may also be fruitful, as it may provide a cause for the existing muscle imbalance, and provide insights into how this problem could be corrected more effectively.
Conclusions
Limited evidence supports the view that weakness of the ERs, weakness in the IRs, and limited range of motion in shoulder ER are risk factors for the development of rotator cuff tendinopathy in overhead athletes. Very limited evidence supports imbalance in ER and IR strength, and supraspinatus weakness are risk factors for rotator cuff tendinopathy in overhead athletes. No existing cohort studies investigated the association between muscle weakness and the risk of rotator cuff tendinopathy in the general public. Existing evidence on whether muscle weakness is a risk factor in the development of rotator cuff tendinopathy is limited, despite having great potential in providing insight into the development of screening programs to lower the risk of this condition. Future cohort studies may improve on existing evidence with investigations in the general public, more muscle groups, longer follow-up times, clearly documented injury history, and a stringent diagnosis of rotator cuff tendinopathy.
Footnotes
Authors’ contributions
CKK designed the study with supervision from SCF. CKK and MCK performed data collection and analysis with supervision from SCF. CKK drafted the text with supervision from SCF. SKKL, HTL, JHO, and PSHY read and approved the various drafts up to the final manuscript
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.