
Abstract
Alpha-1 antitrypsin (AAT) augmentation is effective in slowing the progression of emphysema due to AAT deficiency (AATD) but cannot prevent eventual progression to end-stage lung disease and complete respiratory failure, which is the leading cause of death for individuals with severe AATD. When patients develop end-stage lung disease, lung transplantation is the only treatment option available, and this can improve lung physiology and patient health status. The available data suggest that survival rates for lung transplantation are significantly higher for patients with AATD-related chronic obstructive pulmonary disease (COPD) compared with non-AATD-related COPD, but, conversely, there is a higher risk of common post-lung transplant complications in patients with AATD versus non-AATD COPD. Nevertheless, lung transplantation (single and bilateral) is favorable for patients with AATD. After respiratory failure, the second leading cause of death in patients with AATD is liver disease, for example, cirrhosis and hepatocellular carcinoma, caused by the accumulation of mutant forms of AAT retained within the liver. As with lung disease, the only treatment option for end-stage liver disease is liver transplantation. Survival rates for patients with AATD undergoing liver transplantation are also favorable, and patients, particularly pediatric patients, have benefitted from advancements in peri-/post-surgical care. As the majority of AAT is produced by the liver, the AAT phenotype of the recipient becomes that of the donor, meaning that AAT serum levels should be normalized (if the donor is AAT-replete), halting further lung and liver disease progression. However, post-liver transplant respiratory function may continue to decline in line with normal age-related lung function decline. In the most severe cases, where patients have simultaneous end-stage lung and liver disease, combined lung and liver transplantation is a treatment option with favorable outcomes. However, there is very little information available on this procedure in patients with AATD.
Keywords
Introduction
Alpha-1 antitrypsin (AAT) deficiency (AATD) is a genetic disorder that predisposes patients to lung and liver disease. 1 In addition, there are a spectrum of other pulmonary and extra-pulmonary manifestations associated with AATD, which are the focus of the chapter in this series by Stoller and Tejwani. 2 Respiratory failure is the leading cause of death in patients with severe AATD, followed by liver disease, 3 which is often undetected until cirrhosis or hepatocellular carcinoma is evident (for a more detailed overview of AATD-associated liver disease, please refer to the chapter in this series by Patel and Teckman). 4 AAT augmentation, which is discussed in detail within the chapter by Barjaktarevic and Campos, 5 is effective in slowing the progression of emphysema related to AATD6,7; however, lung density may still continue to decline to the point of respiratory failure (20 g/l has been posited as the threshold for this), 7 and lung transplantation is the only treatment option for those who develop end-stage lung disease. Although only a minority of patients with AATD require lung transplantation (around 5%), AATD remains the fourth most common indication for lung transplantation worldwide, following non-AATD chronic obstructive pulmonary disease (COPD), idiopathic pulmonary fibrosis, and cystic fibrosis. 8 Compared with patients undergoing lung transplantation due to non-AATD COPD, patients undergoing lung transplantation due to AATD are, on average, 10 years younger and have had less exposure to tobacco smoke, 9 making them more suitable for lung transplantation. However, there is conflicting data on post-lung transplant survival in AATD compared with other transplant indications. Similarly, for AATD patients with end-stage liver disease, which may be necessary in children as well as adults, the only effective treatment is liver transplantation.
The transplant-related healthcare burden associated with AATD appears to be disproportionate compared with its status as a rare disease, and transplantation is a rarely discussed area of AATD care, as guidelines focus more on the treatment and monitoring of patients up to lung transplantation. However, it is important to be aware of outcomes in AATD post-lung and liver transplantation so that patients can be provided with all the necessary information before deciding whether or not to go ahead with these treatment options. This chapter of the AATD review series discusses both types of transplantation and the associated outcomes in patients with AATD, as well as combined lung and liver transplantation, which may be the only treatment option for patients with end-stage emphysema complicated by cirrhosis, or for those with cirrhosis and advanced emphysema who would not be expected to survive lung or liver transplantation alone. 10
Lung transplantation
As a result of the efforts of transplant centers worldwide, there is now substantial information available regarding the incidence – and associated outcomes – of lung transplantation related to AATD. Despite being a rare disease, AATD accounts for a substantial proportion of all lung transplantation cases. Between 1995 and 2015, the primary indication for 50,002 adult lung transplantations in the United States (US) was COPD (n = 18,241; 36.5%), and 2568 of these cases (5.1%) were as a result of AATD-related COPD. 11 In Sweden between 1987 and 2015, out of 14,644 patients who required long-term oxygen therapy due to COPD, a higher proportion of patients with AATD-related COPD underwent lung transplantation (19%) than patients with non-AATD-related COPD (1%). This is likely due to AATD patients having more impaired diffusion capacity than non-AATD COPD patients, possibly as a result of a more emphysema-predominant phenotype compared with non-AATD COPD patients. 12 This may account for the high representation of AATD patients within lung transplant statistics.
In the UK, a study from the Antitrypsin Deficiency Assessment and Programme for Treatment (ADAPT) registry between 1996 and 2011 reported favorable post-lung transplant survival rates in patients with AATD of 81.3%, 74.2%, 52.9%, and 45.2% at 90 days, 1 year, 5 years, and 10 years, respectively. 13 Notably, these rates were no better than those of matched control patients who did not undergo lung transplantation. 13 However, patients that did undergo lung transplantation showed significant improvement in forced expiratory volume in 1 s (FEV1) and all domains of the St. George’s Respiratory Questionnaire (both p < 0.002), demonstrating beneficial effects of transplantation outside of survival. 13
Outcomes in AATD versus non-AATD COPD
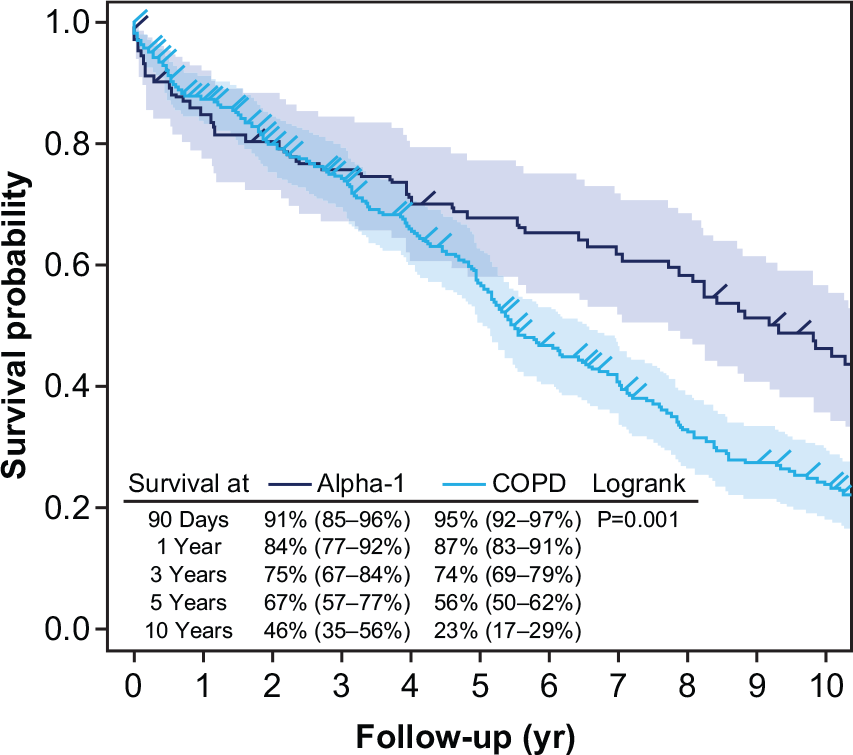
There are several studies reporting that outcomes of lung transplantation in patients with AATD differ from those with non-AATD COPD (Table 1). Studies by Tanash et al. and Fakhro et al. report superior short- and long-term survival in patients with AATD undergoing lung transplantation compared with those with non-AATD COPD,14,15 whereas Spratt et al., Gulack et al., and Riley and Lascano report worse short-term survival but better long-term survival (Table 1; Figure 1).16 –18 There are also differences in survival reported between single lung versus bilateral lung transplantation within these two patient cohorts, with higher survival reported for bilateral lung transplantation irrespective of whether the transplantation was due to AATD or non-AATD COPD (Table 1).17,18 Nevertheless, reducing the incidence of post-transplant infection remains a major challenge to lung transplant survival for any etiology. 15 When compared with non-AATD COPD, lung transplant patients with AATD are reported to have increased post-transplant mortality due to infection and liver disease. 18
Reported outcomes of lung transplantation in patients with AATD and non-AATD COPD.

AAT, alpha-1 antitrypsin; AATD, AAT deficiency; COPD, chronic obstructive pulmonary disease; GI, gastrointestinal; HPB, hepatopancreatobiliary; IQR, interquartile range; LAS, lung allocation score; SD, standard deviation; Tx, transplant.
More recently, however, the above differences in post-transplant survival between patients with AATD versus non-AATD COPD have not been observed in the US, which likely results from implementation of the lung allocation score (LAS) in 2005. 17 The LAS was devised to prioritize patients awaiting lung transplantation based on disease severity and patient health, rather than prioritizing patients based upon time on the transplant waiting list. Therefore, patients with AATD may now receive lung transplants at an older age. The reason for the change in post-transplant survival observations following LAS implementation may be multifactorial, but could be due to the fact that the LAS does not differentiate between diagnosis with regards to COPD; both AATD-related and non-AATD-related COPD are grouped together as a “Group A” Diagnosis. 17 Therefore, it is possible that there were differences in the severity of illness by diagnosis prior to LAS implementation that led to reduced early survival for patients with AATD. 17 Alternatively, the increasing use of AAT augmentation may be responsible for reducing the differences in lung transplant statistics in AATD versus non-AATD COPD, 17 with patients potentially surviving longer before lung transplantation is required. These observations may also be due to overall improvements in the approach to lung transplantation, which may have impacted some specific disease processes more than others. 17
There are, therefore, conflicting reports on the overall value of lung transplantation in AATD, with early studies suggesting longer survival in patients with AATD, but with worse short-term survival. These differences are less apparent in recent studies in the US, which may be attributed to the more widespread use of AAT augmentation and the LAS. Further studies could investigate whether patients with AATD today have significantly worse clinical state than those with non-AATD COPD at the time of lung transplantation.
Outside of survival, the decline in FEV1 pre-lung transplantation is highly variable for patients with AATD and non-AATD COPD,19,20 and, following single lung transplantation, the rate of decline in FEV1% predicted appears to be no different between AATD and non-AATD COPD patients. 21 However, a faster rate of decline in FEV1% predicted has been observed in AATD patients undergoing a double lung transplantation. 21 Prior to lung transplantation, other surgical intervention approaches, such as endobronchial lung volume reduction (ELVR) and endobronchial coil treatment, may be suitable treatment options for patients with AATD-associated lung disease, and are discussed in more detail in the chapter by Barjaktarevic and Campos. 5
Impact of AAT augmentation
Treatment of AATD with intravenous infusion of exogenous AAT protein (AAT augmentation) aims to slow the progression of lung destruction and has demonstrated significant slowing of emphysema progression related to AATD, prolonging the time to terminal respiratory failure.5 –7,22 Registry data also suggests that AAT augmentation confers a survival advantage compared with no treatment, 23 which is supported by an extrapolation analysis of the lung densitometry data from the RAPID clinical trial program.6,7 AAT augmentation plays an important role in postponing lung transplantation, but its role following lung transplantation is unclear and needs to be explored.24,25 Indeed, most reports of transplantation outcomes in the previous section do not provide information on the use of AAT augmentation post-lung transplantation in patients with AATD. In the US study that compared outcomes of AATD-related COPD and non-AATD-related COPD lung transplant recipients, only three double lung transplant patients with AATD (n = 45) received AAT augmentation within 3 years following transplantation, and the effects of AAT augmentation on post-transplant survival were not investigated. 21 However, AAT augmentation use post-lung transplantation was reported to help reverse what seemed to be impeding chronic rejection in one patient. 21
In the post-lung transplant period, there is excessive inflammation and neutrophil activity (with an increase in neutrophil elastase) in patients with AATD, which can further increase during periods of infection and/or transplant rejection. 26 Therefore, treatment with AAT, which has been shown to assist in the resolution of chronic inflammation in the lung endothelium, 27 may be beneficial to AATD patients following lung transplantation. In line with this, there has been interest in the utility of AAT augmentation for transplant indications including graft-versus-host disease and lung transplantation in general, with several pre-clinical and early-phase studies conducted in this area.28 –32 Pre-clinical animal models have also shown a potential benefit of AAT augmentation in terms of reducing allograft injury, 33 but this needs to be confirmed in human trials. Regarding AAT augmentation utilization pre-transplantation, one study in Germany has reported differences in post-transplant survival in patients who had previously received AAT between 1999 and 2012, compared with those who had not received the therapy. 34 At 1 year post-transplant, there was a trend towards lower survival in patients who received AAT augmentation prior to transplantation. This difference became statistically significant in the long-term (between 3 and 10 years post transplantation; p ⩽ 0.01). 34 The results were unexpected and the authors had no definitive explanation, although it was postulated that patients who had previously received AAT augmentation may have had more severe disease prior to transplantation, which could have impacted the post-transplant outcome. Alternatively, given that AAT augmentation is considered to be an immunomodulatory therapy, sudden therapy discontinuation could have an adverse effect on post-lung transplant survival, 34 which could suggest that a tapering approach is indicated in the period immediately after transplantation. However, more research is required in this area.
Although resolution of emphysema as a result of lung transplantation necessitates discontinuation of AAT augmentation, the underlying genetic deficiency remains unresolved. Indeed, the reoccurrence of emphysema in patients with AATD has been documented twice in the literature; in a patient 11 years post lung transplantation, 35 and in another 2 years post lung transplantation. 36 In both cases, patients had recommenced smoking. In these cases, the reintroduction of AAT augmentation is justified if patients abstain from smoking. In contrast, AAT augmentation is not recommended following liver transplantation related to AATD, as transplantation of a donor liver from an AAT-replete individual will result in the normal production and secretion of endogenous AAT. 37
Liver transplantation
The background to the pathophysiology and progression of liver disease in AATD is covered in an earlier chapter of this series of reviews. 4 However, as previously mentioned, although supportive care and symptomatic treatment is warranted for patients with AATD, liver transplantation is the only available curative treatment for end-stage liver disease related to AATD. 38 In adults, liver disease is often undetected until cirrhosis or hepatocellular carcinoma is evident, which are treatable through liver transplantation. 39 In children with AATD, some may experience jaundice and have no further complications, whilst some may develop liver cirrhosis and require liver transplantation. 39 Therefore, the American Thoracic Society/European Respiratory Society recommend liver assessment through liver function testing in all individuals most at risk of AATD-associated liver disease (patients with the PI*ZZ genotype). 1 However, additional testing may be necessary as testing serum liver enzymes alone may not be sufficient; in a study of 403 patients with AATD (PI*ZZ), liver enzymes were increased in only a minority of patients [19.1% for alanine aminotransferase, 12.7% for aminotransferase (AST), 23.7% for γ-glutamyl transferase and 8.6% for alkaline phosphatase]. 40 Non-invasive liver assessments, as for other causes of chronic liver disease, such as the liver stiffness measurement and the AST to platelet ratio index, may be useful to identify those at risk of AATD-associated liver disease.40,41
In AATD, disease progression to end-stage liver disease requiring liver transplantation occurs more commonly in males, with 73% of those requiring liver transplantation being male, despite rates of liver disease diagnosis being similar between men and women.39,42 Increased body mass index has also been found to be a risk factor for end-stage liver disease requiring liver transplantation in AATD. 43 The course of pulmonary disease after liver transplantation in both adults and children is poorly understood, but, recently, pulmonary hypertension and pulmonary embolism were reported more frequently in adult patients with AATD compared with those undergoing liver transplantation without AATD. 44 However, further studies are required to clarify the impact of liver transplantation on pulmonary function. 45 Nevertheless, liver transplantation is associated with favorable survival rates in both adults and children with AATD.
Outcomes
Liver transplantation is associated with favorable survival rates for a variety of diagnoses, including AATD. In one large study of survival rates from 5180 liver transplantations (116 of which were related to AATD) in 37 different centers in the US between 1982 and 1991, the 5-year survival rate for patients undergoing liver transplantation related to AATD was 72.9%. 46 This was slightly higher than the overall average 5-year survival rate of 69.2%, and similar to survival rates for primary (71.0%) and secondary biliary cirrhosis (81.4%), primary sclerosing cholangitis (73.5%), and Wilson’s disease (79.2%), but substantially higher than for hemochromatosis (43.1%), liver cancer (33.6%), and hepatitis B (31.9%). 46 In another US study evaluating liver transplantation over a later period (1995–2004), a higher survival rate at 5 years post-liver transplantation in patients with AATD was reported (83%; Figure 2). 47 The improvements in post-transplant survival in this study may reflect advances in supportive treatments and peri-/post-surgical care over time.

In children with AATD, liver transplantation is also associated with favorable long-term outcomes in terms of survival, growth, and quality of life.48 –51 A study using the United Network for Organ Sharing (UNOS) database reported a 5-year survival rate of 90% in pediatric liver transplant recipients with AATD, somewhat higher than the rate of 83% reported among adult liver transplant recipients with AATD. 47 A study from another US center analyzing survival following liver transplantation in pediatric patients with AATD highlighted the importance of novel treatments in determining post-transplant outcomes. 49 The 5-year survival rate increased from 33% in the period of 1969–1984 to 77% following the introduction of cyclosporine in 1985, and 100% following the introduction of tacrolimus in 1995. 49 More recently, in a study of 32 adults and 58 children with the AATD undergoing liver transplantation between 1982 and 2017 in Europe, overall patient survival rates were 97.8%, 95.5%, 95.5, 92.0% and 89.1% at 1, 5, 10, 15, and 20 years, respectively. 52
The AATD genotype may have a minor influence on survival rates post liver transplantation, with one study, predominantly in adults, reporting respective 3-, 5-, and 10-year survival rates of 83%, 80%, and 72% for PI*ZZ patients, compared with 86%, 79%, and 79% for PI*SZ patients. 53 Despite these minor differences, the survival rate following liver transplantation for both adult and pediatric patients with severe AATD is considered excellent.
Normalization of AAT production
A specific benefit of liver transplantation is that it should normalize the secretion of AAT, potentially reducing further disease-related decline in lung function and liver disease. This premise is supported by studies where liver transplantation was associated with a rise in serum AAT levels,53,54 as well as findings from a small US study conducted between 1999 and 2003, which collected lung function data from seven patients with AATD from before and after liver transplantation. 55 Despite an expected decline in FEV1 of 250 ml during the 3-year period post-liver transplant, there was no significant change in lung function in these liver transplant recipients. 55 The authors concluded that liver transplantation likely prevented progression of pulmonary disease in these patients. 55 However, another US study has reported variable results. 53 In a small group of PI*ZZ patients following liver transplantation, the majority of patients (n = 11) experienced a decline in FEV1 whereas others (n = 6) showed an improvement in FEV1. 53 These data suggest that further studies are required to fully understand the impact of liver transplantation on lung function. It is important to note that, although liver transplantation normalizes AAT levels and there have been some reports of lung function improvement, lung function may continue to decline at a rate comparable with that of normal age-related decline in lung function following liver transplantation. 56
Complete normalization of AAT production following liver transplantation will occur only if the donor liver is from an AAT-replete (PI*MM) individual. However, as not every center routinely tests donors for AATD, it is possible for a liver transplant recipient to receive a liver with a severe AATD genotype. Indeed, cases of PI*MZ, PI*ZZ, and PI*SZ liver transplantation have been reported.45,57,58 The recipient of an affected liver may initially go unnoticed, as testing AAT levels post-liver transplantation is not performed routinely. 45 Testing should therefore be considered for unexplained liver function test abnormalities post-liver transplantation, or if periodic acid-Schiff and D-globules are found on donor organ biopsies. 45 Alternatively, non-invasive genetic testing should be performed, which would identify patients with borderline serum AAT levels.
Combined lung and liver transplant
Combined lung and liver transplant is a viable treatment option for patients with both end-stage lung and liver disease who would otherwise not survive with either transplantation alone. 10 This type of combined transplant is not commonly performed due to the complexity of the procedure, and so there are currently no recipient selection criteria reported in the literature. There is also no listing criteria for patients with AATD-related lung and liver disease, and there is limited information regarding patient characteristics and outcomes, particularly in patients with AATD. In one study of eight patients undergoing combined lung and liver transplantation between 2009 and 2012 in one US center, overall survival at 1 year was 71.4%, but only one combined transplant was related to AATD. 10 In a German study with 13 patients undergoing combined lung and liver transplant between 1999 and 2003, two combined transplants were related to AATD and overall survival rates at 1, 3, and 5 years were 69%, 62%, and 49%, respectively, for the seven patients that did not succumb to post-operative complications. 59 Although combined transplant is more commonly performed in patients with cystic fibrosis, the limited data available suggest that it can be performed successfully with favorable outcomes in carefully selected patients with AATD. Infectious complications are the most common cause of death related to this procedure, but improvements in surgical technique, treatment in the intensive care unit, and medical and immunosuppressive therapy have helped to make combined lung and liver transplantation a viable procedure when performed at experienced centers. 59
Conclusions
Lung and liver transplantation are viable treatment options for end-stage lung and liver disease in patients with AATD, and data shows that post-lung and -liver transplant survival is favorable. Patients show improved lung function and quality of life post lung transplantation, and although some differences have been reported in the past, recent data in the age of the LAS and AAT augmentation suggest that outcomes of lung transplantation in patients with AATD are similar to those with non-AATD-related COPD. The effect of prior AAT augmentation on survival following lung transplant requires further investigation.
Liver transplantation in patients with AATD is associated with favorable long-term survival rates and is the only available intervention for addressing severe liver disease related to AATD. Survival rates are very good for both adult and pediatric transplant recipients and has increased over the past decades as better supportive treatments and care have become available. A specific benefit of liver transplantation in patients with AATD is that physiological AAT levels are restored with the introduction of a liver expressing wild-type AAT, which should theoretically slow the progression of AATD-related lung disease, and preclude the reoccurrence of AATD-related liver disease. In the most severe cases of AATD, where patients have end-stage lung and liver disease simultaneously, a combined lung and liver transplant may be a feasible treatment option, but more data on this procedure is required for patients with AATD.
Footnotes
Acknowledgements
Medical writing assistance was provided by Ben McDermott and Steven Foster of Meridian HealthComms Ltd., Plumley, UK, in accordance with good publication practice (GPP3), funded by CSL Behring.
Author contributions
Both authors contributed to the writing of the manuscript, reviewed the manuscript, and approved the manuscript for submission.
Conflict of interest statement
The authors declare that there is no conflict of interest.