
Abstract
Objectives:
To investigate the chest high-resolution computed tomography (HRCT) findings in coronavirus disease 2019 (COVID-19) pneumonia patients with acute respiratory distress syndrome (ARDS) and to evaluate its relationship with clinical outcome.
Materials and methods:
In this retrospective study, 79 COVID-19 patients with ARDS were recruited. Clinical data were extracted from electronic medical records and analyzed. HRCT scans, obtained within 3 days before clinical ARDS onset, were evaluated by three independent observers and graded into six findings according to the extent of fibroproliferation. Multivariable Cox proportional hazard regression analysis was used to assess the independent predictive value of the computed tomography (CT) score and radiological fibroproliferation. Patient survival was determined by Kaplan–Meier analysis.
Results:
Compared with survivors, non-survivors showed higher rates of lung fibroproliferation, whereas there were no significant differences in the area of increased attenuation without traction bronchiolectasis or bronchiectasis. A HRCT score <230 enabled the prediction of survival with 73.5% sensitivity and 93.3% specificity, 100% negative predictive value (NPP), 83.3% positive predictive value (PPV) and 88.6% accuracy (Area Under the Curve [AUC] = 0.9; 95% confidence Interval [CI] 0.831–0.968). A multivariate Cox proportional hazards model showed that the HRCT score is a significant independent risk factor for mortality (Hazard Ratio [HR] 9.94; 95% CI 4.10–24.12). Kaplan–Meier analysis revealed that a HRCT score ⩾230 was associated with a higher fatality rate. Organ injury occurred less frequently in patients with a HRCT score <230 compared to those with a HRCT score ⩾230.
Conclusion:
Early pulmonary fibroproliferative signs on HRCT are associated with increased mortality and susceptibility to organ injury in COVID-19 pneumonia patients with early ARDS.
Key points
Pulmonary fibroproliferation occurs in the early stages of acute respiratory distress syndrome (ARDS) due to coronavirus disease 2019 (COVID-19) pneumonia, manifested by the areas of traction bronchiolectasis or bronchiectasis within increased attenuation on high-resolution computed tomography (HRCT) scans.
Compared with survivors, non-survivors showed a higher percentage of lung fibroproliferation, whereas there were no significant differences in the area of increased attenuation without traction bronchiolectasis or bronchiectasis.
The extent of fibroproliferative signs on HRCT at the diagnosis of ARDS due to COVID-19 pneumonia was an independent predictive factor for death and organ injury.
Introduction
Coronavirus disease 2019 (COVID-19) is caused by a new coronavirus called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which emerged in China in December 2019.1,2 Until 26 April 2020, there were 209 countries and 2,804,796 confirmed COVID-19 cases globally, including over 193,710 deaths. 3 Most cases infected with SARS-CoV-2 have mild symptoms and a good prognosis, the clinical symptoms of which are similar to those of regular human flu. However, similar to severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), COVID-19 could also develop into acute respiratory distress syndrome (ARDS), multiple organ failure or even death.4,5
Mortality from ARDS still remains above 50% despite the use of low tidal volume ventilation and conservative fluid strategies. 6 ARDS is pathologically classified into three stages, in which an initial inflammatory injury with protein-rich edema and hemorrhage is followed by fibroproliferation. The fibroproliferative phase of ARDS has traditionally been regarded as a late event. 7 However, previous studies found that fibroproliferation is initiated early in ARDS and could predict mortality in ARDS patients.8,9 Some previous studies have demonstrated that levels of procollagen 3 in bronchalveolar lavage was correlated with the severity of fibrosis on lung biopsy. A comparative study between computed tomography (CT) scan and procollagen 3 found a weak correlation between them for fibrosis diagnosis after ARDS, suggesting that procollagen 3 could be an earlier marker of diffuse alveolar damage at the exudative state than CT scan which shows installed and maybe less reversible fibroproliferation.10,11 In addition, Ichikado et al. reported that fibroproliferation characteristics in HRCT could predict mortality in ARDS patients caused by pneumonia, aspiration, sepsis, etc. 12 Bilateral areas of ground-glass attenuation and airspace consolidation as well as the involvement of multiple lung lobes were common chest CT finding in severe and critical COVID-19 pneumonia patients. 13 Recently, Zhang et al. observed diffuse alveolar damage (DAD) and alveolar interstitial fibrosis in a lung biopsy from a deceased COVID-19 pneumonia patient. 14 To our knowledge, no study has been performed to evaluate chest CT patterns, especially early fibroproliferative changes and their eventual prognostic value in COVID-19 pneumonia patients with ARDS. Thus, in this retrospective study, we proposed that early pulmonary fibroproliferative HRCT imaging characteristics were associated with increased mortality in COVID-19 pneumonia patients with early ARDS, and the extent of fibroproliferative signs on HRCT was an independent predictive factor for death.
Materials and methods
Study design and participants
This study was approved by the Institutional Review Board (IRB) of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (IRB ID: TJ-C0200108). Patient consent was waived because of the retrospective nature of the study and because of emerging infectious diseases. Patients were admitted from 5 January to 16 February 2020. The inclusion criteria were as follows: (a) real-time reverse transcription polymerase chain reaction (RT–PCR) assay detection of SARS-CoV-2 nucleic acid positive in throat swabs or nasopharyngeal swabs; (b) diagnosis of ARDS using the Berlin definition 15 and interim guidance for clinical management of severe COVID-19 published by the World Health Organization (WHO); 16 (c) CT scan of the chest performed within 3 days before clinical ARDS onset. Exclusion criteria were as follows: pre-existing chronic pulmonary fibrosis and bronchiectasis were strictly excluded by history taking, documented from a review of radiological reports and the initial CT imaging data on HRCT scans (Supplemental Figure 1). The clinical data and outcomes were monitored up to 17 April 2020, the final date of follow-up. According to the outcomes, patients were divided into survivors and non-survivors groups.
Data collection
Medical record information including demographic, clinical, laboratory, treatment and outcome data were collected and extracted by using data collection forms.
CT examination
All patients underwent HRCT scanning of the chest within 0–3 days before the onset of ARDS. CT was performed in the supine position during end-inspiration without intravenous contrast medium, with various CT scanners using standard-dose chest CT protocols (GE Healthcare, Philips, or Toshiba Medical Systems). Imaging parameters were as follows: 80–120 kVp tube voltage, automated tube current modulation (60–300 mA), rotation time of 0.5 s, pitch of 0.984:1, slice thickness of 1.25 mm, reconstruction matrix: 512 × 512, with selected differences according to machine types.
HRCT assessment
All CT images were reviewed respectively by three radiologists (MX, QJH, HXG with 10, 10 and 20 years of clinical experience, respectively), who were unaware of patient outcomes. Disagreements were resolved by consensus. Chest CT images assessed the presence and extent of areas for the following characteristics based on the recommendations in Fleischner Society terminologies and similar studies: ground-glass opacity (GGO), airspace consolidation, traction bronchiectasis, traction bronchiolectasis, and honeycombing.17,18 When bronchi were irregular in contour or larger than the adjacent pulmonary artery, the bronchus within areas of parenchymal abnormality was recognized as traction bronchiectasis. Traction bronchiolectasis was identified by means of the presence of dilated bronchioles within areas with parenchymal abnormality. Honeycombing was defined as small, stacked 2–20 mm cysts in the subpleural lung without intervening lung parenchyma.
Scoring of HRCT findings
The HRCT findings were graded on a scale of 1–6 based on the classification by Ichikado and colleagues,12,18 which was correlated with previously described pathology: score of 1, normal attenuation; score of 2, ground-glass attenuation; score of 3, consolidation; score of 4, ground-glass attenuation with traction bronchiolectasis or bronchiectasis; score of 5, consolidation with traction bronchiolectasis or bronchiectasis; and score of 6, honeycombing. The extent of involvement of each abnormality was assessed independently for each of three zones of each lung: upper (above the carina), middle (below the carina and up to the inferior pulmonary vein), and lower (below the inferior pulmonary vein) zones. The extent of each abnormality was visually estimated to the nearest 10% of parenchymal involvement in each zone, and was then obtained by averaging the six zones’ extent. The abnormality score for each zone was obtained by multiplying the extent of involvement by each grading score (the score of 1–6) and then the total CT score was calculated by adding the averages for each index of the six zones.
Statistical analysis
All statistical analyses were performed using SPSS 20.0 software. The quantitative data of normal distribution were presented as mean ± Standard Deviation (SD) (minimum–maximum), and those of abnormal distribution were expressed as median (Interquartile Range [IQR]). Normally distributed variables were compared by using the paired t-test; abnormally distributed variables were compared by using the Mann–Whitney U test. The qualitative data were presented as a percentage (%) and analyzed with Fisher’s exact test or the chi-square test. The missing data are classified as ‘missing completely at random’ in our study. The proportion of missing data was less than 10%, so missing data are automatically recognized as system-missing values by SPSS. The biggest value in the Youden index was chosen to determine the cut-off level of the HRCT score. Cox proportional hazards regression analysis was used to evaluate the influence of the CT score and radiological fibroproliferation on survival while adjusting for other clinical factors. According to clinical aspects and previous studies,5,19 age, pulse oxygen saturation/fraction of inspiration O2 (SPO2/FiO2) ratio, lymphocyte count, D-dimer, any comorbidity and quick sequential organ failure assessment score (qSOFA) were important confounding factors associated with disease outcomes. Therefore, those six variables were included in Cox proportional hazards regression analysis using the enter method. The HRCT score has close correlation with radiological fibroproliferation (GGO with traction bronchiectasis or traction bronchiolectasis, consolidation with traction bronchiectasis or traction bronchiolectasis and traction bronchiolectasis or bronchiectasis). Therefore, the HRCT score, GGO with traction bronchiectasis or traction bronchiolectasis as well as consolidation with traction bronchiectasis or traction bronchiolectasis, and traction bronchiolectasis or bronchiectasis were included in three different model of Cox analysis, respectively. Patient survival was determined by Kaplan–Meier analysis. For all statistical analyses, p < 0.05 was considered significant.
Results
Clinical and laboratory findings
The characteristics, laboratory findings, complications and treatment of patients are shown in Table 1. A total of 79 COVID-19 patients with ARDS were enrolled in the research, including 45 survivors and 34 non-survivors. The median age of the survivors and non-survivors was 64.0 and 66.5 years, respectively. Most patients were men in the two groups. The mean SPO2/FiO2 ratio of survivors and non-survivors was 222.0 and 146.7. The proportion of patients with qSOFA ⩾ 1 was 67% and 91% in survivors and non-survivors. Hypertension (49%) was the most common comorbidity followed by diabetes (16%). The most common complications were respiratory failure (42%) and heart injury (23%), followed by renal dysfunction (16%). The laboratory abnormalities noted were lymphopenia, elevated D-dimer concentration, increased C-reactive protein and procalcitonin level in patients. Most patients received antiviral (95%), antibacterial (97%) and glucocorticoid therapy (90%); 19% of patients received high oxygen flow support, and ventilation was given in 52% of patients.
Characteristics, laboratory findings, complications and treatment in non-survivors and survivors.

Data are expressed as median (IQR) or n (%). Laboratory findings were collected at the time of CT examination. p Values comparing survivors and non-survivors are from Student’s t-test, Mann–Whitney U test, χ² or Fisher’s exact test, as appropriate. Supplemental oxygen therapy had been given to all patients. The number of participants with cardiae troponin I, procalcitonin and C-reactive protein were 72, 72 and 76, respectively.
IQR, interquartile range; SPO2, pulse oxygen saturation; FiO2, Fraction of inspiration O2; qSOFA, quick sequential organ failure assessment score; CT, computed tomography.
HRCT findings for survivors and non-survivors
All patients underwent HRCT scanning of the chest within 0–3 days (median 1) before the onset of ARDS, and the difference within days before the development of ARDS between the two groups was not statistically significant. The extent of CT findings in survivors and non-survivors is summarized in Table 2. The average percentage of lung affected was 75.93% in non-survivors compared with 59.22% in survivors (p < 0.001). The areas of traction bronchiolectasis or bronchiectasis and honeycombing were indicative of radiological fibroproliferation. Similarly, the areas of traction bronchiolectasis or bronchiectasis were significantly smaller in survivors than in non-survivors (Figures 1 and 2), whereas the extent of increased attenuation without traction bronchiolectasis or bronchiectasis was not statistically significant between survivors and non-survivors (Table 2). A multivariate Cox proportional hazards model with adjustment for age, SPO2/FiO2 ratio, lymphocyte count, D-dimer, any comorbidity and qSOFA, the total areas of the traction bronchiolectasis or bronchiectasis remained independent risk factors for mortality (Hazard Ratio [HR] 4.56; 95% confidence Interval [CI] 1.32–15.69) (Table 3 and Supplemental Table 1).
Extent of each high-resolution CT finding in survivors and non-survivors of ARDS with COVID-19.
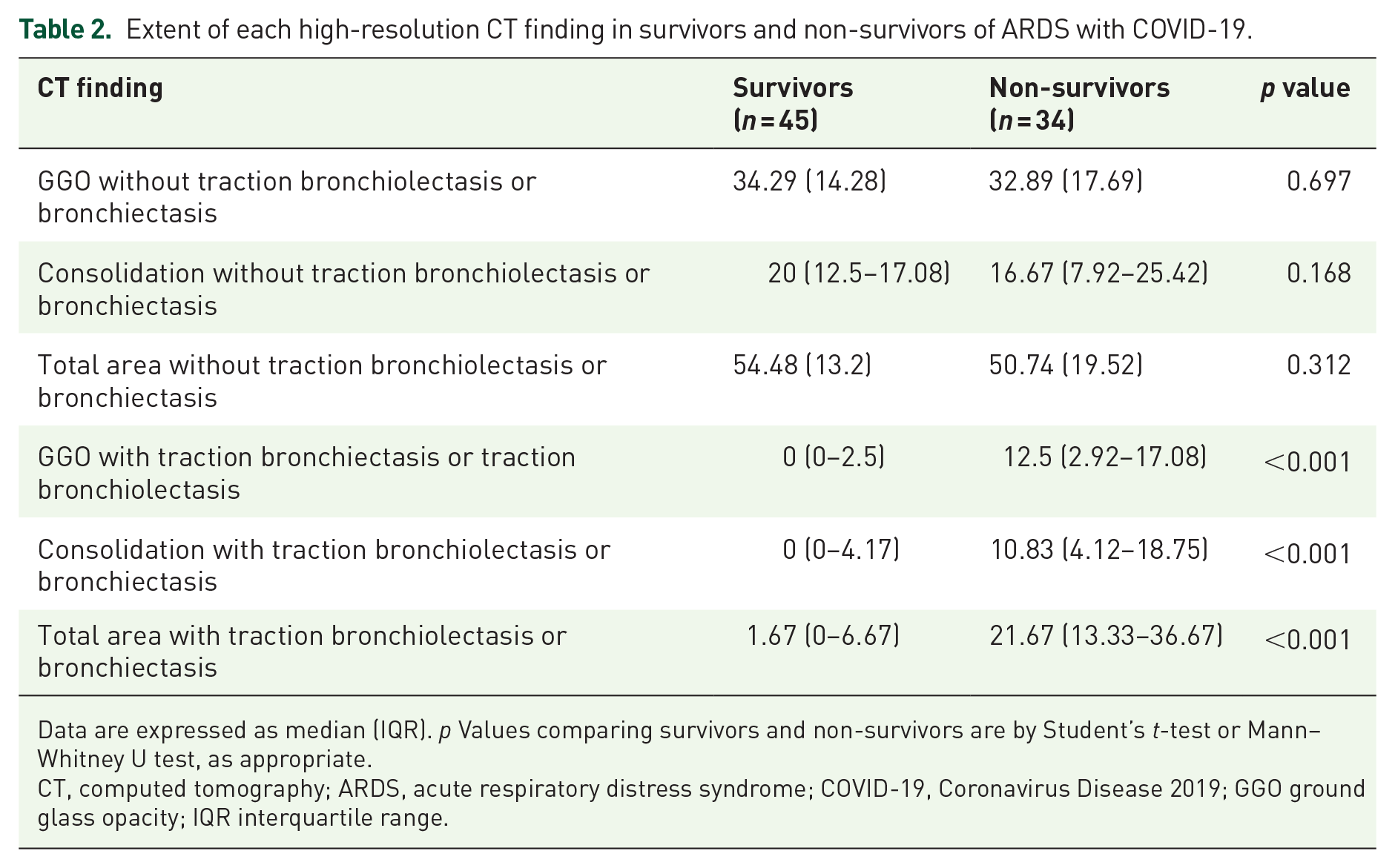
Data are expressed as median (IQR). p Values comparing survivors and non-survivors are by Student’s t-test or Mann–Whitney U test, as appropriate.
CT, computed tomography; ARDS, acute respiratory distress syndrome; COVID-19, Coronavirus Disease 2019; GGO ground glass opacity; IQR interquartile range.
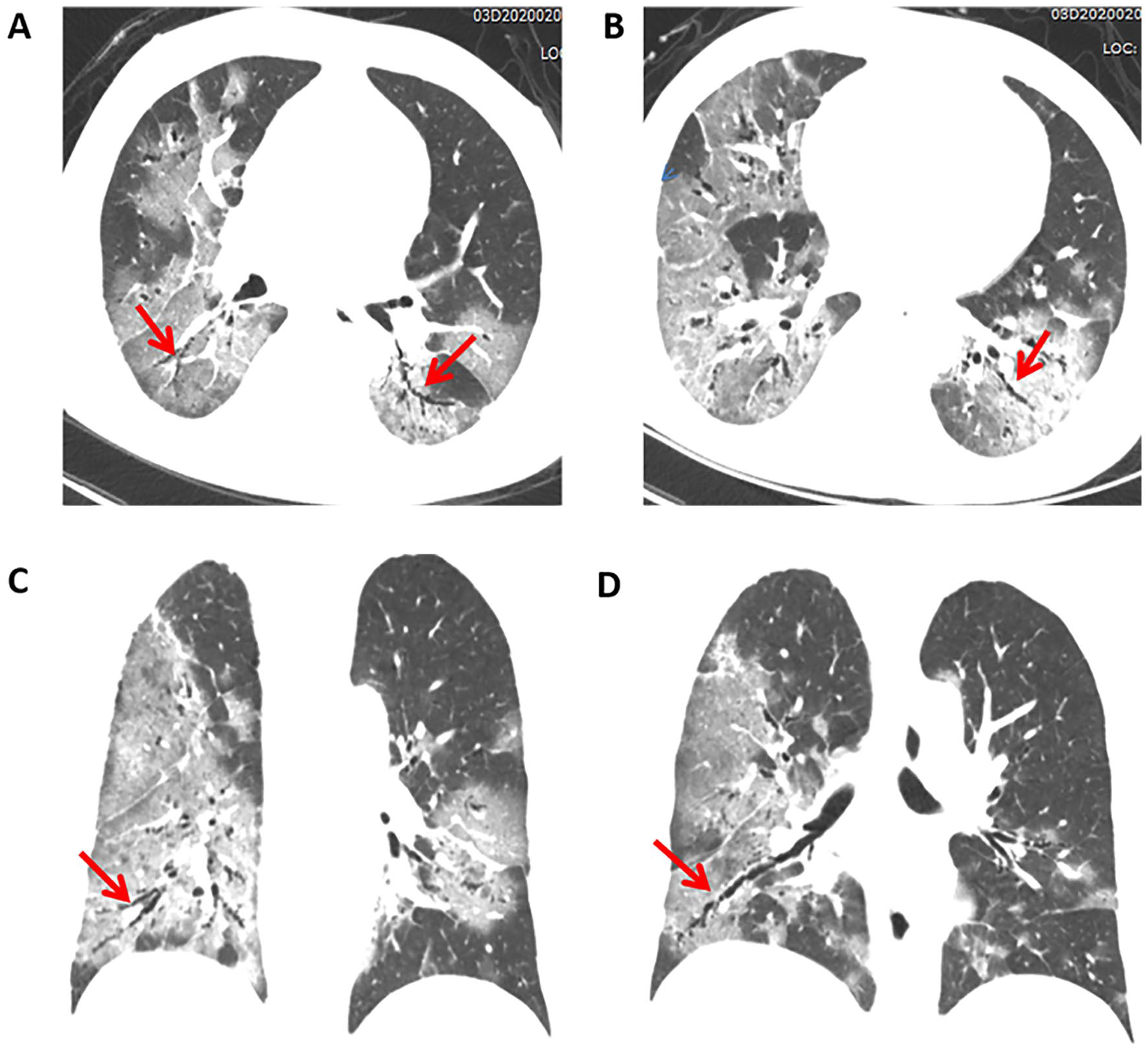
HRCT findings in a 55-year-old man with ARDS due to COVID-19 pneumonia who did not survive. HRCT scan shows bilateral areas of extensive ground-glass opacities associated with traction bronchiolectasis and bronchiectasis (arrows) and small consolidation in most lobes. (A) (B) axial images, (C) (D) coronal images.

HRCT findings in 40-year-old man with ARDS due to COVID-19 pneumonia who survived. HRCT scan shows extensive GGO predominantly and patchy consolidation without traction bronchiolectasis or bronchiectasis (arrows) involved multiple lung lobes. (A) (B) axial images, (C) (D)
Multivariate Cox regression analysis of HRCT findings and clinical characteristics associated with mortality in ARDS patients with COVID-19.

Cox proportional hazard regression models were applied to determine the potential risk factors associated with mortality, with the hazards ratio (HR) and 95% confidence interval (CI) being reported.
HRCT, high-resolution computed tomography; ARDS acute respiratory distress syndrome; COVID-19, Coronavirus Disease 2019; GGO, ground glass opacitye.
For more details please refer to Supplemental Table 2.
Prognostic value of the HRCT score
The overall HRCT score of survivors (mean 191.93 ± 29.47; range 146.67–273.33) was significantly lower than that of non-survivors (mean 255.78 ± 40.13; range 171.67–331.67). The sensitivity, specificity, likelihood ratio and Youden index for different thresholds of CT score are provided in Supplemental Table 2. A HRCT score <230 enabled the prediction of survival with 73.5% sensitivity, 93.3% specificity, 100% negative predictive value (NPP), 83.3% positive predictive value (PPV) and 88.6% accuracy (Area Under the Curve [AUC] = 0.9; 95% CI 0.831–0.968) (Figure 3). Multivariate Cox proportional hazards model analysis revealed that the HRCT score remained an independent risk factor for mortality (HR 9.94; 95% CI 4.10–24.12) (Table 3 and Supplemental Table 1). Kaplan–Meier analysis revealed that a higher CT score was associated with a higher fatality rate (Figure 4).

ROC curve of the CT score identified the optimal cut-off value of 230 for prediction of survival.
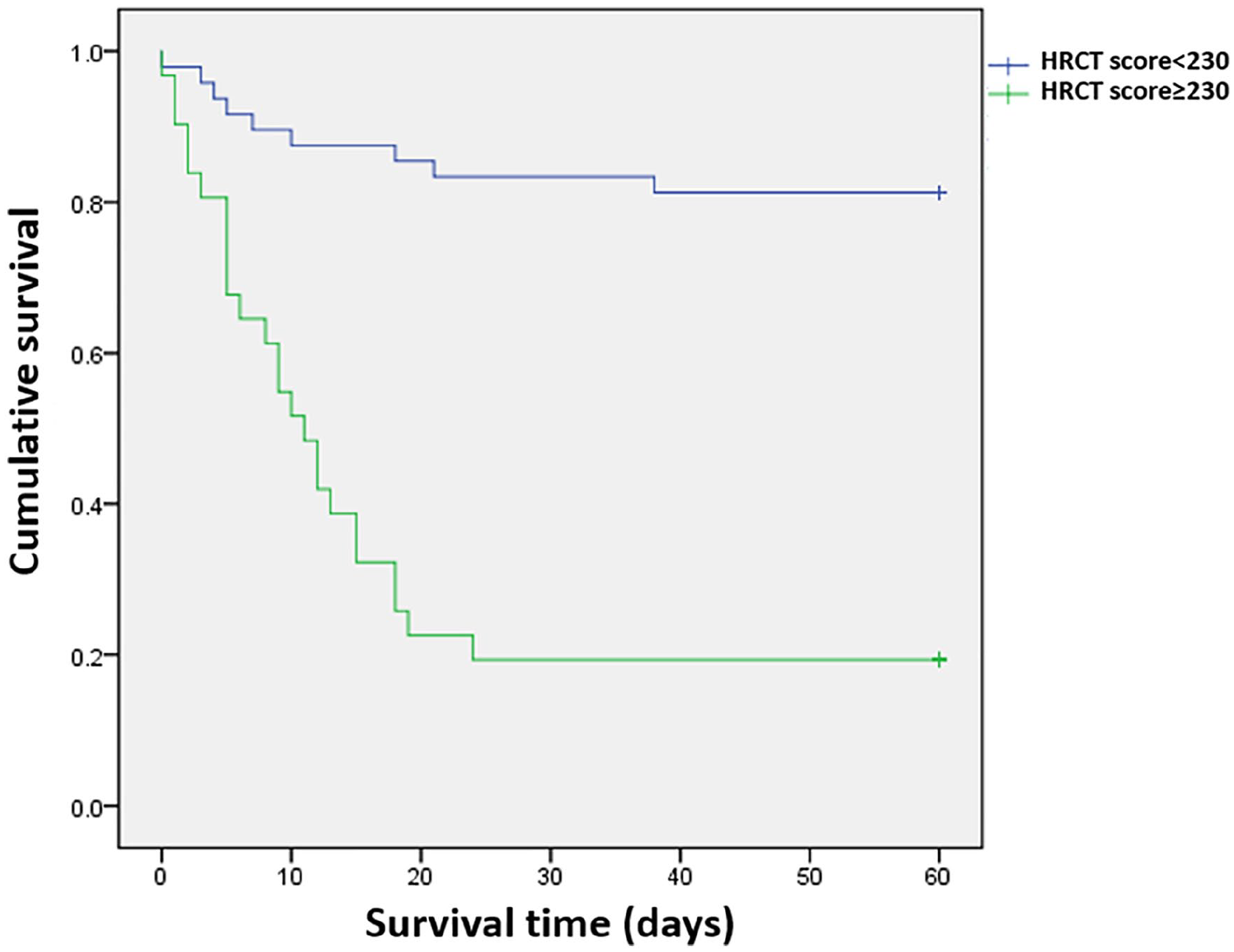
Kaplan–Meier analysis showed a significant difference for the survival ratio for a CT score cut-off of 230.
Discussion
In this retrospective cohort study, we comprehensively evaluated and analyzed the HRCT imaging characteristics of 79 COVID-19 pneumonia patients with ARDS. We found that pulmonary fibroproliferation occurs in the early stages of ARDS due to COVID-19 pneumonia, manifested by the areas of traction bronchiolectasis or bronchiectasis within increased attenuation on HRCT scan. Furthermore, we demonstrated the extent of fibroproliferative signs on HRCT, and a higher CT score at diagnosis of ARDS due to COVID-19 pneumonia was an independent predictive factor for death. Our observation suggested that pulmonary fibroproliferation at the early stage of COVID-19 ARDS is an important determinant of outcome. To our knowledge, this is the first study to evaluate whether fibroproliferation on HRCT in COVID-19 pneumonia patients with ARDS predicts mortality.
Traditionally, ARDS is divided into three stages in which an initial inflammatory phase is followed by fibroproliferation. 7 Interestingly, fibroproliferative pathways are activated early in ARDS, demonstrated by an increased fibrotic marker in bronchoalveolar lavage fluid (BALF). 9 HRCT scans of acute interstitial pneumonia showed more extensive areas of increased attenuation associated with traction bronchiectasis, which corresponded to fibroproliferative phases of DAD. 20 In the present study, traction bronchiolectasis or bronchiectasis within areas of increased attenuation, suggesting radiological fibroproliferation, was already detectable on HRCT scans obtained within 3 days (median 1 day) before the ARDS diagnosis in 49 patients (62.03%). Some investigations have shown that the typical findings of chest CT images in COVID-19 pneumonia patients are bilateral multiple lobular and subsegmental areas of consolidation and GGO, most commonly in the peripheral, subpleural area, or distributed diffusively.21–23 In addition, Li et al. reported that HRCT findings associated with severe and critical COVID-19 pneumonia were bilateral areas of ground-glass attenuation and consolidation in multiple lung lobes. 13 However, this new radiological evidence provided an innovative new method compared with previous investigations. Nevertheless, our study together with previous observations, suggests an alternative to traditional models of the lung injury response, whereby inflammatory and repair mechanisms occur in parallel rather than in series.
Several retrospective cohort studies have clarified clinical risk factors for death in patients with COVID-19 pneumonia.24–27 However, as we know, few studies have focused on the chest CT imaging appearance and COVID-19 pneumonia mortality. Our data suggested that extensive fibroproliferative HRCT imaging characteristics on HRCT in the early stages were associated with ARDS mortality in patients with COVID-19 pneumonia. Similarly, Ichikado et al. showed higher mortality in patients with areas of increased lung attenuation and varicoid bronchiectasis in the setting of clinically diagnosed ARDS caused by diverse diseases.12,18 These findings suggest that fibroproliferative signs on HRCT could be used for the assessment of direct and indirect ARDS severity.
The potential mechanisms by which fibroproliferative signs on HRCT might lead to poorer outcomes are unclear and are related to the pathological process. ARDS patients, who were in the acute exudative phase histologically had a better prognosis than did those who were in the fibroproliferative phase which was confirmed by lung biopsy. 9 On the basis of our evaluation of 79 COVID-19 pneumonia ARDS patients, some patients with fibroproliferative signs would be diagnosed with early ARDS if only the parameter of time elapsed since the onset of ARDS. Our present data suggest the discrepancy between the ‘clinically’ early phase of ARDS and ‘pathologically’ early phase of ARDS. However, it is difficult to distinguish the transition from exudative to fibroproliferative of these pathological phases without a lung biopsy in ARDS patients. Chest CT scan could be useful to distinguish these pathological phases and for the early diagnosis of lung injury.
High-volume ventilation initiates extracellular matrix remodeling in patients and experimental models. 28 This effect is likely to be due to repeated cyclic stretch and high tidal volume ventilation inducing the gene expression of several molecules related to the fibroproliferative processes. 29 In our study, some of the patients received lung protective mechanical ventilation. According to a previous study, lung protective ventilation strategies to prevent ongoing epithelial injury may drive fibroproliferation. 30 Given the benefit of lung protective mechanical ventilation, understanding and defining other factors that may drive the pathological fibroproliferative response in ARDS is vital as the optimal window for therapeutic intervention is most likely either to precede or coincide with the onset of fibroproliferation.
This study has several limitations. First, this study was retrospective and was conducted at a single-center hospital. Owing to limited medical resources, not all COVID-19 pneumonia patients received chest CT examination in the early period of ARDS. Second, the total number of patients was small, which limits the reliability of our study. More powerful studies with pooled data from multiple centers would be likely to be beneficial. Third, intubation could have been delayed for some patients due to limited medical resources during the peak period of the COVID-19 outbreak. Last but not least, this study only involved Chinese people. The results of this study may not be applicable to other ethnic groups.
The present study reported that fibroproliferative HRCT imaging characteristics occur early in COVID-19 ARDS, and the extent of fibroproliferative signs on HRCT with severity scores is a significant risk factor for the mortality of COVID-19 ARDS patients. Taken together, our findings suggest the potential of an early HRCT scan evaluation in patients with COVID-19 ARDS to identify individuals who may be at risk of poorer outcomes.
Supplemental Material
sj-docx-1-taj-10.1177_2040622320982171 – Supplemental material for Early fibroproliferative signs on high-resolution CT are associated with mortality in COVID-19 pneumonia patients with ARDS: a retrospective study
Supplemental material, sj-docx-1-taj-10.1177_2040622320982171 for Early fibroproliferative signs on high-resolution CT are associated with mortality in COVID-19 pneumonia patients with ARDS: a retrospective study by Zhilin Zeng, Min Xiang, Hanxiong Guan, Yiwen Liu, Huilan Zhang, Liming Xia, Juan Zhan and Qiongjie Hu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-pdf-1-taj-10.1177_2040622320982171 – Supplemental material for Early fibroproliferative signs on high-resolution CT are associated with mortality in COVID-19 pneumonia patients with ARDS: a retrospective study
Supplemental material, sj-pdf-1-taj-10.1177_2040622320982171 for Early fibroproliferative signs on high-resolution CT are associated with mortality in COVID-19 pneumonia patients with ARDS: a retrospective study by Zhilin Zeng, Min Xiang, Hanxiong Guan, Yiwen Liu, Huilan Zhang, Liming Xia, Juan Zhan and Qiongjie Hu in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
The authors would like to express their gratitude to Professor David A. Lynch (Department of Radiology, National Jewish Health, Denver, CO, USA) and Qihang Chen (Department of Radiology, Beijing Hospital, Beijing, China) for consultation on CT images. They are indebted to the frontline medical and nursing staff in Wuhan city who demonstrated selfless and heroic devotion to duty in the face of this COVID-19 outbreak despite the potential threat to their own lives and those of their family members.
Author contributions
ZLZ and MX contributed equally to this paper. JZ and QJH designed the study, had full access to all data in the study, and take responsibility for the integrity and accuracy of the data analysis. JMZ, YWL, HXG and LMX contributed to patient recruitment, data collection, data analysis, data interpretation and literature search. ZLZ and MX drafted the manuscript. JZ and QJH finally revised the manuscript. All authors contributed to data acquisition, data analysis, or data interpretation, and all reviewed and approved the final version of the manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Natural Science Foundation of China (NSFC) (grant number 81800041).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.