
Abstract
Background:
Carotid intima–media thickness (cIMT) is considered a risk factor for and predictor of cerebrovascular disease. In this study, we explored the contribution of cIMT to cognitive impairment (CI) in dialysis patients and the role of cerebral small vascular disease (CSVD) and brain atrophy in this process.
Methods:
Cognitive function was assessed using a comprehensive cognitive test battery. CSVD and brain volume were assessed by magnetic resonance imaging, and cIMT was measured by ultrasonography. Multivariable analysis and mediation were used to explore the relevant relationships among cIMT, CI, CSVD and brain volume.
Results:
Seventy-three dialysis patients were enrolled. Approximately 54.8% were diagnosed with increased cIMT. The increased cIMT group was older and had lower serum albumin and creatinine levels than the normal cIMT group. There was no difference in the CSVD prevalence between the different cIMT groups. Patients in the normal, unilaterally and bilaterally increased cIMT subgroups demonstrated a gradual decrease in brain-matter volume and degenerate cognitive function. cIMT was related to cognitive function and gray-/white-matter volume. Increased cIMT was associated with a significantly increased risk of a reduced Mini Mental State Examination/Montreal Cognitive Assessment score and Trail A/B time delay. Mediation analysis showed that CI was mediated by brain-matter volume but not by CSVD.
Conclusion:
Increased cIMT was an independent risk factor for impairment of global cognitive function, memory, and executive function. The impact of cIMT on cognition was not induced by CSVD but by brain atrophy. cIMT may be a useful tool for screening patients at high risk of CI in the dialysis population.
Keywords
Introduction
Dialysis patients (end-stage renal disease, ESRD-5D) suffer from a higher prevalence and worse outcome of cerebrovascular disease than the general population.1,2 In addition to stroke, dialysis patients also have a higher prevalence of cerebral small vessel disease and cognitive decline.3,4
Cerebrovascular disease and carotid-artery disease are both risk factors for cognitive impairment (CI) in the general population.5,6 Carotid intima–media thickness (cIMT) is widely used as a noninvasive index to assess carotid atherosclerosis. The results from the Cardiovascular Health Study showed that in patients without clinically evident cerebrovascular disease, cognitive decline was associated with severe stenosis of the left internal carotid artery. 6 In an animal model, it was shown that relief of bilateral carotid stenosis could improve cognitive function. 7 However, the mechanisms of cognitive impairment in patients with asymptomatic carotid stenosis are still not well understood, with one possible explanation being the absence of a good model. Chronic kidney disease (CKD) is considered an independent risk factor for carotid atherosclerosis. 8 A recent study demonstrated decreased cerebral blood flow (CBF) during the dialysis procedure, 9 which may magnify the influence of carotid atherosclerosis on brain lesions in ESRD patients. Thus, the ESRD population would be an optimal model for discovering the relationships among carotid atherosclerosis, cognitive function, and CSVD.
Therefore, we hypothesized that carotid atherosclerosis is partly responsible for CI in dialysis patients and that subclinical CSVD and brain atrophy may be involved in the pathogenesis of this process.
Materials and methods
Study design
This is a retrospective study. The present study was approved by the Ethics Committee of Peking Union Medical College Hospital (PUMCH; IRB number S564). Written informed consent was obtained from each participant.
Participants
In the 2013–2014 CSVD-CI study, 416 maintenance dialysis patients from our dialysis center were screened from July 2013 to July 2014 10 with the following criteria: age 18 years or older and regular dialysis for at least 1 month. Patients with the following criteria were excluded from the study: systemic infection, acute cardiovascular or stroke events, cancer, surgery, or trauma in the month prior to the study; metabolic encephalopathy, mental disorders, emotional disorders, epilepsy requiring long-term treatments, or diagnosis of dementia; history of nonatherosclerotic arterial disease, such as Anti-neutrophil cytoplasmic antibody (ANCA) vasculitis; metal prosthesis; and inability to complete the cognitive assessment.
We recruited patients from the original study who had at least one carotid-artery ultrasound record with cIMT measurement results within a year before or after the brain magnetic resonance imaging (MRI) procedure based on the Hospital Information System at PUMCH.
According to cIMT measurements, patients were divided into a normal cIMT group and an increased cIMT group. In the increased cIMT group, patients were further categorized by dividing them into unilaterally and bilaterally increased cIMT subgroups.
Clinical and laboratory data
Demographics, comorbid conditions, dialysis parameters and physical examination results including dialysis modality, dialysis vintage, smoking status, history of hypertension, diabetes mellitus, hyperlipidemia, self-reported stroke, ischemic heart disease, and related medications were recorded. Laboratory data from blood examinations conducted during the same period as the brain MRI evaluation were evaluated. For hemodialysis (HD) patients, the blood sample was taken at the first HD session in a week.
Imaging and analyses
Carotid-artery ultrasound
Philips iU22 (Bothell Everett Highway, Bothell, USA) color Doppler ultrasonic diagnostic instruments with a probe frequency of 7.5 MHz were used for carotid ultrasonography. Using the carotid bulb as an anatomic reference, measurements were performed 10 mm below the carotid bifurcation in the common carotid arteries, at the bifurcation level, and 10 mm after the carotid bifurcation in the internal carotid arteries. The intima–media thickness of the common carotid artery was defined as the mean of the maximum intima–media thicknesses of the near and far walls. The greater value of the right or left common cIMT (CAA-IMT) was used for analysis. Values of cIMT ⩾1 mm were defined as increased cIMT; 11 otherwise, they were defined as normal cIMT. The sonographers were blinded to the clinical information.
Brain MRI and CSVD
The participants underwent brain magnetic resonance (MR) examinations on a 3.0 T MR scanner (DISCOVERY MR750; General Electric, Milwaukee, WI, US) using an eight-channel head coil. Imaging sequences included T1-weighted and T2-weighted sequences, fluid-attenuated inversion recovery and susceptibility-weighted imaging MR sequences. One radiologist and one neurologist blinded to the clinical information independently assessed the presence and location of different signs of recent lacunar infarcts, lacunes (similar to the definition for chronic lacunar infarcts), white-matter hyperintensities (WMHs), and cerebral microbleeds (CMBs).10,12–14 Discrepancies were resolved by consensus after discussion.
Brain volume measurement
Structural three-dimensional (3D) T1-weighted MRI images were acquired using a 3.0-T Siemens Vision scanner. VBM8, a toolbox of SPM8 software (https://www.fil.ion.ucl.ac.uk/spm/software/spm8/), was used for the morphometric analysis, which was applied with the DARTEL algorithm. First, the structural images were segmented into gray matter (GM), white matter (WM), and cerebrospinal fluid (CSF) using a standard unified segmentation model in SPM8. The sum of GM and WM was defined as brain matter (BM), while the whole-brain volume was the total volume of BM and CSF. The percentage of the GM volume in the whole brain was defined as the GM fraction; the percentage of WM volume in the whole brain was defined as the WM fraction; and the percentage of the BM volume in the whole brain was defined as the BM fraction. After that, the DARTEL approach was performed for registration, normalization, and modulation in the DARTEL space. In detail, a new DARTEL template was constructed based on the deformation fields from the segmentation procedure, and all the individual deformation field maps were registered to the new template. Then, the GM images were normalized to a study-specific template in the Montreal Neurological Institute space. All the brain region volumes were measured by calculating the total number of voxels in each image’s data, with resampling voxel size of 1 cm isotropic and spatially smoothed with 8 mm full width at half-maximum Gaussian kernel. 15
Cognitive assessments
Medical staff members from our dialysis center were trained by neurologists to administer the cognitive tests. Cognitive assessments were performed on an intradialysis day for HD patients and during clinical visits for peritoneal dialysis patients.
In the cognitive test battery, global cognitive function was assessed with the Chinese versions of the Mini Mental State Examination (MMSE) and the Montreal Cognitive Assessment (MoCA). 4 The specific domains of cognitive function were evaluated by the Chinese version of the 12-word Philadelphia Verbal Learning Test (czP(r)VLT-12) 16 to assess immediate, short-delayed and long-delayed verbal memory, the Boston Naming Test 17 to assess language ability, and Trail-Making Tests A and B 18 to assess executive function (Trail B is more complicated than Trail A). The scores of czP(r)VLT-12 ranged from 0 to 12, with higher scores denoting better performance. Higher scores on the Boston Naming Test represent higher ability. The time taken to complete the Trail A/B test performance was recorded.
Statistical analysis
Continuous data with a normal distribution are presented as the means ± standard deviation and were analyzed by Student’s t-test and one-way analysis of variance. The data with high skew are presented as the median and interquartile range and were analyzed by the Mann–Whitney test and the Kruskal–Wallis test. Categorical data are presented as proportions and were analyzed by the chi-square test and Fisher’s exact test. Correlations between variables were assessed by Pearson’s coefficient test. The differences in various cognitive scores and brain volumes in the normal, unilateral and bilateral cIMT increased subgroups were compared with the trend test. Variables with p < 0.05 in the univariate analyses were selected as candidate variables for the multivariable regression analyses, which were performed to investigate whether cIMT was associated with impaired cognitive function. The SPSS 21.0 statistical package (IBM Corporation, Armonk, NY, US) was used for all analyses, and a value of p < 0.05 was considered statistically significant. In addition, the fit curve of age and cIMT with various cognitive functions was performed with Origin (Originlab Corporation, Northampton, MA, US), R (http://www.R-project.org), and EmpowerStats software (www.empowerstats.com, X&Y solutions, Inc. Boston, MA, US).
Mediation of the association of cIMT with cognitive function by CSVD and brain volume
Mediation analysis was performed using the template described by Baron and Kenny and the method described by Vanderweele and Vansteelandt. 19 Figure 1 illustrates the hypothetical causal model. To perform mediation analysis, it is necessary to test three pathways: step 1, the association of cIMT with CSVD or BM (a); step 2, the association of CSVD or BM with cognitive function (b); and step 3, the association of cIMT with cognitive function (c’). If all three associations are confirmed, mediation can be established in a fourth step through pathway (c). According to Baron and Kenny, the mediation of the relationship is full when (c) is not significant and partial when (c) is significant. Mediation is absent when not all steps are satisfied. All pathways were tested using univariable and multivariable regression analysis.

Model of the hypothetical causal pathway from cIMT to cognitive function in dialysis patients.
Results
From our dialysis-CSVD-CI study cohort, 73 dialysis patients had undergone carotid-artery ultrasonography within 1 year before or after the brain MRI scan and thus were recruited in this study.
In our cohort, 54.8% (40/73) of patients were diagnosed with increased cIMT, and 13/73 patients had unilateral cIMT increments (10 were left carotid arteries, 3 were right carotid arteries). All our patients were right handed. A total of 37.0% (27/73) were male, and the average age was 57.9 years. Furthermore, 67.1% (49/73) of them were on HD, and the rest were on peritoneal dialysis. The median dialysis vintage was 56.0 months. Of the patients, 94.5% were hypertensive, 28.8% were diabetic, 45.2% had hyperlipidemia, and 8.2% had a history of stroke (Table 1).
Clinical characteristics of patients with normal and elevated cIMT.

The p value is for the comparison between the normal and increased cIMT groups.
Bolded numerals indicate statistical significance.
BMI, body mass index; cIMT, carotid intima–media thickness; DBP, diastolic blood pressure; HD, haemodialysis; HDL-C, high-density lipoprotein cholesterol; hs-CRP, high-sensitivity C-reactive protein; LDL-C, low-density lipoprotein cholesterol; MAP, mean arterial pressure; Med_RAASI, renin–angiotensin–aldosterone-system-inhibitors medication use; Med_PLT, antiplatelet medication use; PTH, parathyroid hormone; SBP, systolic blood pressure.
Between the normal and increased cIMT groups (Table 1), sex, education level, combined diseases, dialysis modality and vintage, average blood pressure, RAASI (renin–angiotensin–aldosterone-system inhibitors) medication use, serum phosphorus levels, parathyroid hormone, and lipid profiles were comparable. However, those in the increased cIMT group were older (62.4 ± 9.6 years versus 52.5 ± 11.3 years) and had lower serum albumin (37.4 ± 4.4 g/l versus 39.4 ± 3.8 g/l) and lower serum creatinine levels (860.7 ± 261.9 μmol/l versus 1007.8 ± 204.4 μmol/l) than the normal cIMT patients.
CSVD and brain volume in different cIMT groups
There was only a tendency for more CSVD lesions (lacunes, WMH, and CMB) in the increased cIMT group than in the normal cIMT group, but none of the three types of CSVD reached statistical significance (Table 2).
CSVD and brain volume of patients in different cIMT groups.

n indicates the number of patients with the relevant characteristics.
The p value is for the comparison between normal and increased cIMT groups.
p for trend, comparison of normal, unilateral and bilateral cIMT increased subgroups.
Bolded numerals indicate statistical significance.
cIMT, carotid intima–media thickness; CMB, cerebral microbleed; CSVD, cerebral small vascular disease; WMH, white-matter hyperintensity.
Between the normal and increased cIMT groups, there was no difference in whole-brain volume, but the increased cIMT group showed significant decreases in GM, WM, and BM volume and corresponding fractions (Table 2). Moreover, there was a significant gradually declining trend in the normal, unilateral and bilateral increased cIMT subgroups.
We also analyzed the relationship between cIMT and different brain volumes. The cIMT was negative relative to the GM volume (r = −0.412, p < 0.001), WM volume (r = −0.290, p = 0.014), BM volume (r = −0.376, p = 0.001), and corresponding fractions but not relative to whole-brain volume (Supplemental Table S1).
Cognitive function and cIMT
Cognitive function in different cIMT groups
The patients with increased cIMT showed poorer global cognitive performance on the MMSE and MoCA than the normal cIMT participants, and more patients were diagnosed with CI (Table 3). The increased cIMT group also had poorer memory function on the czP(r)VLT-12, especially for immediate- and long-delayed memory; they also showed worse executive function in Trail B. The two different cIMT groups exhibited a similar language ability regarding the Boston Naming score and executive function in Trail A. We further compared patient cognitive function in the normal, unilaterally and bilaterally increased cIMT subgroups, showing a trend of more carotid-artery involvement and more severe CI in global cognitive function, memory, and executive function (Figure 2).
Cognitive function of patients with normal and elevated cIMT.

Data are presented as n, number of patients included (and percentage) in the prevalence section; data are presented as median (and interquartile range) in non-prevalence setion.
The p value is for the comparison between normal and increased cIMT groups.
Bolded numerals indicate statistical significance.
CI-MMSE, cognitive impairment evaluated by MMSE; CI-MoCA, cognitive impairment evaluated by MoCA; cIMT, carotid intima–media thickness; czP(r)VLT-12, Philadelphia Verbal Learning Test; MMSE, Mini Mental State Examination; MoCA, Montreal Cognitive Assessment.

Performances of various cognitive functions by cIMT groups.
As people age, cognitive function declines. The patients in the increased cIMT group demonstrated a steeper slope of deterioration in all aspects of cognitive function with age than those in the normal cIMT group (Figure 3).
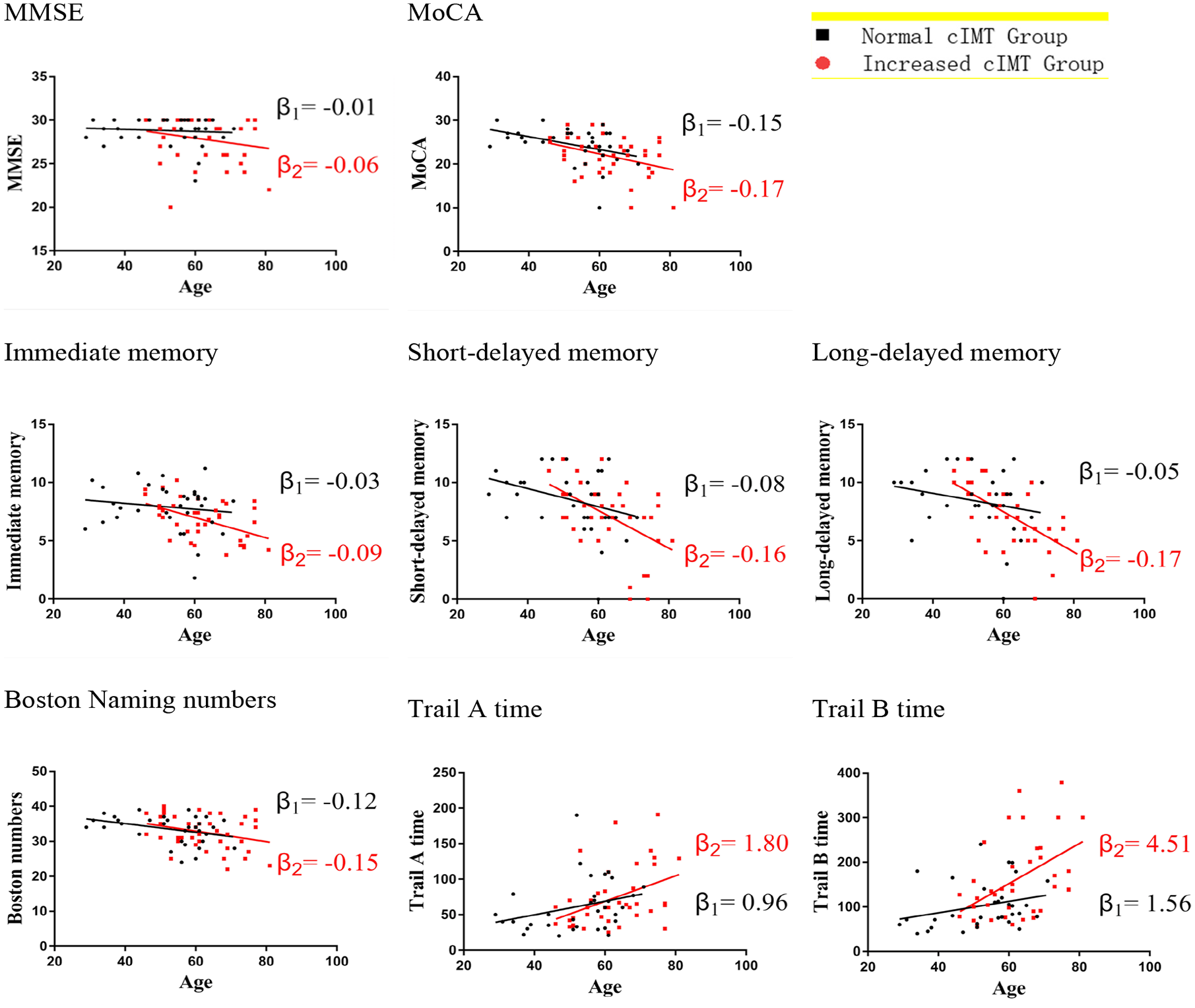
Linear fit chart of age with various cognitive function grouping by normal and increased cIMT.
Effect of cIMT on cognitive function
As cIMT increased, a declining tendency was seen in global cognitive function in the whole cohort and the domains of memory and executive function, as shown in Figure 4.
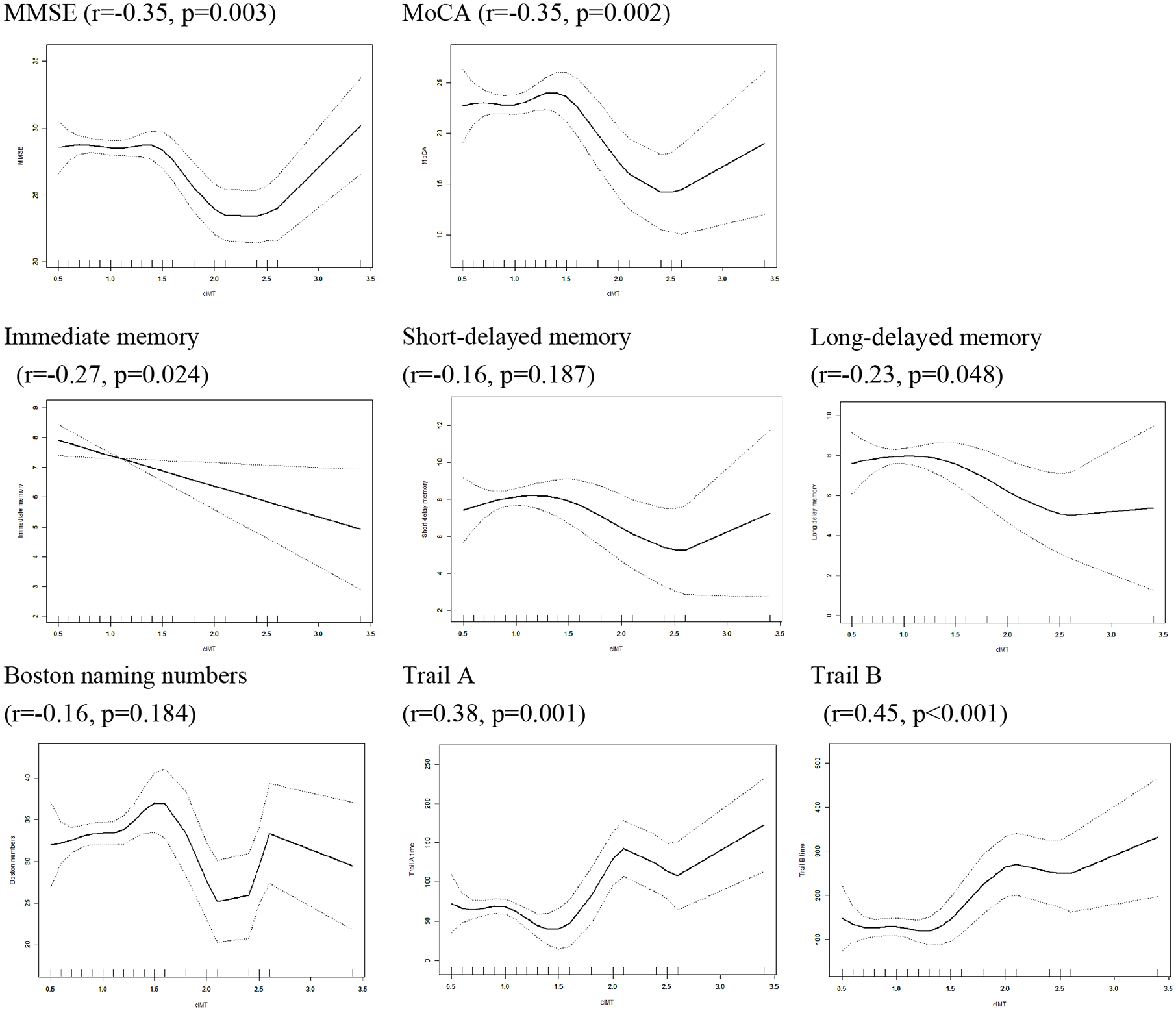
Fit curve of cIMT with various cognitive functions adjusted for age.
To investigate the effect of carotid-artery stenosis on global and different domains of cognitive function, we further built several models to analyze the relationship between carotid-artery stenosis and cognitive testing scores in the whole cohort (Table 4). In the crude model, both the global cognitive assessment score and each specific aspect of cognitive function showed negative relevance to the thickness of the cIMT. In model 1, after adjusting for age, education level, antiplatelet medication, dialysis modality, and serum albumin and creatinine levels, cIMT still showed an effect on global cognitive function [for the MMSE, β = −1.28 (95% confidence interval −2.23 to −0.33); for the MoCA, β = −2.29 (95% confidence interval −4.17 to −0.40)] and executive function [for Trail A, β = 24.14 (95% confidence interval 6.73–41.55); for Trail B, β = 60.91 (95% confidence interval 26.31–95.52)]. In model 2, we adjusted for three types of CSVD based on model 1; the influence of cIMT on cognitive function remained the same as in model 2. Based on model 2, we further adjusted for BM volume in model 3. In this model, the influence of cIMT on different domains of cognition was decreased compared with that in model 2.
Multiple linear regression analysis of cIMT associated with impaired cognitive function.

Model 1: adjusted for age, education level, antiplatelet medication, dialysis modality, serum albumin and serum creatinine.
Model 2: adjusted for the variables entered into model 1 and lacunes, cerebral microbleeds, and white-matter hyperintensity.
Model 3: adjusted for the variables entered into model 2, gray-matter volume, and white-matter volume.
CI, confidence interval; cIMT, carotid intima–media thickness; czP(r)VLT-12, Philadelphia Verbal Learning Test; MMSE, Mini Mental State Examination; MoCA, Montreal Cognitive Assessment.
To provide deeper insight into the possible pathway from cIMT to CI, we also analyzed the mediation effect of the association between cIMT and cognitive function by CSVD and brain volume (Supplemental Table S2). Considering brain structure, cIMT could generate global cognitive and memory, language, and executive function impairment by full or partial mediation through GM, WM, and BM, but none of these cognitive impairments was mediated through CSVD.
Discussion
In this retrospective study, we focused on a specific population of dialysis patients who had a high burden and increased comorbidity of cardiovascular and cerebrovascular disease. CKD was shown to be an independent risk factor for carotid atherosclerosis, 8 and increased cIMT is associated with early-stage 20 and advanced CKD. 21 cIMT is considered a surrogate for cardiovascular disease and is a variable predictor of stroke and cardiovascular events.22–24 Our original cohort also showed a high prevalence of cognitive function decline and CSVD in dialysis patients.4,10 Thus, ESRD-5D patients would be an appropriate population in which to explore the relationship between vascular factors (e.g. cIMT, carotid stenosis) and brain lesions.
In our cohort, patients with increased cIMT had worse performance in global cognitive function, memory, and executive function. The severity of increased cIMT was relative to cognitive function. Figure 2 shows more carotid-artery involvement and worsened cognitive performance. This trend was statistically significant in global function and the domains of memory and executive function. Figure 3 shows that patients with cIMT increases had a faster rate of decline in all domains of cognitive function. After adjusting for age, the thickness was still relative to the MMSE/MoCA, memory, and executive function.
To further illustrate the possible mechanism of the relationship between cIMT and cognitive function from the perspective of brain lesions, we introduced cerebrovascular disease and brain volume for analysis. Our results showed that the increased cIMT group had a significantly decreased BM volume and that these BM volumes were negative relative to cIMT. However, there was no difference in the three typical CSVD features between the two different cIMT groups.
In the cognitive function comparison, greater cIMT was significantly associated with worse performance on all cognitive tests in the unadjusted regression model. After adjustment for demographics, clinical risk factors and CSVD, cIMT remained negatively associated with global function and executive function. These findings were similar to those of several longitudinal studies.25–27 There is no doubt that CSVD is related to cognitive function. CSVD may be caused by microembolisms due to carotid plaque rupture. However, Frazier et al. 26 found that the relationship between executive function decline and cIMT was independent of WM injury and cerebral infarct. Beyond their findings, we found that lacune and microbleed CSVDs did not affect the impact of cIMT on cognitive function. Carotid atherosclerosis might lead to brain hypoperfusion and atrophy. Our finding that the BM volumes were negative relative to cIMT just provided evidence for it. In the adjusted models, after adjusting for BM volumes, the relationship between cIMT and cognitive tests shrank or disappeared. These results indicated that brain atrophy may be an important mediator from cIMT to cognition. We performed a further mediation analysis. These models proved that GM, WM, and total BM mediated the association of cIMT with cognitive function in all domains, while CSVD was not involved in this process.
A study on ESRD showed that CBF was increased in patients with ESRD compared with healthy controls; however, the CBF of dialysis patients was lower than that of nondialysis ESRD patients. 28 In contrast, a recent study in HD patients showed decreased CBF during the HD procedure and demonstrated a possible link between the dialysis-induced CBF decrease and cognitive decline, in which CSVD WMHs and brain atrophy may be involved. 9 It seems to be controversial in CBF changes in ESRD patients. In fact, at the early stage of carotid stenosis, blood flow may accelerate, while at the late stage, blood flow decreases. In the general population, the autoregulation of CBF could compensate for the change in blood supply. However, in dialysis patients, regardless of the stage of carotid stenosis, there might be dysfunction of CBF autoregulation, which will decrease the total brain blood supply and eventually result in brain atrophy. Our findings about the role of CAA-IMT in brain volume and cognitive function specifically support the long-term influence of CBF changes in brain lesions in dialysis patients.
The treatment of carotid stenosis in dialysis is conservative. Carotid revascularization in ESRD showed a low risk–benefit ratio with higher rates of in-hospital mortality and moderate-to-severe disability. 29 However, our results show a relationship between cIMT and BM volume/cognitive decline. From this point of view, monitoring the increase in cIMT and preventing it from developing carotid stenosis would be more appropriate in ESRD patients. Control of CAA-IMT might contribute to preventing cognitive decline in dialysis patients. Currently, strict control of hypertension and hyperglycemia, smoking cessation, and prevention of CKD progression are central therapies for carotid atherosclerotic disease23,30 and related brain lesions.
To the best of our knowledge, this is the first study about cIMT and cognitive function that focuses on brain volume and CSVD at the same time. However, this study still has some limitations. Our findings are based on a retrospective observational study, and further follow up on cognitive function is needed to make the results more convincing. Second, although very few studies have focused on cIMT and brain imaging changes in dialysis patients, our sample size was still relatively small compared with studies in the general population. Finally, we assessed only CAA-IMT, and assessment of the internal carotid artery may provide more information.
Conclusion
Our study supports a role for CAA-IMT in cognitive function impairment in dialysis patients, especially in global cognitive function, memory and executive function. In the relationship between cIMT and cognitive decline, BM atrophy demonstrated a more important effect than CSVD. Furthermore, dialysis patients with increased cIMT need to be more closely monitored for cognitive decline.
Supplemental Material
Supp_Material_cIMT_and_CSVD_cognitive_function20200623 – Supplemental material for Carotid intima–media thickness relative to cognitive impairment in dialysis patients, and their relationship with brain volume and cerebral small vessel disease
Supplemental material, Supp_Material_cIMT_and_CSVD_cognitive_function20200623 for Carotid intima–media thickness relative to cognitive impairment in dialysis patients, and their relationship with brain volume and cerebral small vessel disease by Ke Zheng, Yujun Qian, Tiaye Lin, Fei Han, Hui You, Xixi Tao, Bo Hou, Jing Yuan, Haiyun Wang, Dingding Zhang, Ke Lv, Feng Feng, Yicheng Zhu and Xuemei Li in Therapeutic Advances in Chronic Disease
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: the contributing study was funded by the 12th National Science and Technology Support Program (2011BAI10B02) and CAMS Innovation Fund for Medical Sciences (CIFMS) (2017-I2M-2-001).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.