
Abstract
Background:
The purpose of this study was to examine the prevalence and effects of current smoking on adverse outcomes among hospitalized COVID-19 patients.
Methods:
A systematic review of the literature (PubMed) identified 18 (from a total of 1398) relevant studies. Pooled current smoking prevalence was compared with the gender-adjusted and gender and age-adjusted, population-based expected prevalence by calculating prevalence odds ratio (POR). The association between current, compared with non-current and former, smoking and adverse outcome was examined. A secondary analysis was performed by including 12 pre-publications (30 studies in total). All analyses were performed using random-effects meta-analysis.
Results:
Among 6515 patients, the pooled prevalence of current smoking was 6.8% [95% confidence interval (CI): 4.8–9.1%]. The gender-adjusted POR was 0.20 (95% CI: 0.16–0.25, p < 0.001), and the gender and age-adjusted POR was 0.24 (95% CI: 0.19–0.30, p < 0.001). Current smokers were more likely to have an adverse outcome compared with non-current smokers [odds ratio (OR): 1.53, 95%CI: 1.06–2.20, p = 0.022] but less likely compared with former smokers (OR: 0.42, 95% CI: 0.27–0.74, p = 0.003). When pre-publications were added (n = 10,631), the gender-adjusted POR was 0.27 (95% CI: 0.19–0.38, p < 0.001) and the gender and age-adjusted POR was 0.34 (95% CI: 0.24–0.48, p < 0.001).
Conclusion:
This meta-analysis of retrospective observational case series found an unexpectedly low prevalence of current smoking among hospitalized patients with COVID-19. Hospitalized current smokers had higher odds compared with non-current smokers but lower odds compared with former smokers for an adverse outcome. Smoking cannot be considered a protective measure for COVID-19. However, the hypothesis that nicotine may have a protective effect in COVID-19 that is partially masked by smoking-related toxicity and by the abrupt cessation of nicotine intake when smokers are hospitalized should be explored in laboratory studies and clinical trials using pharmaceutical nicotine products.
Introduction
The coronavirus pandemic has generated an understandable concern about the effects of smoking on disease susceptibility and severity. Smoking is an established risk factor respiratory infections. 1 Media reports and opinion pieces have made reasonable suggestions that smoking may be detrimental in case of infection with SARS-CoV-2, assuming that the gender differences in COVID-19 vulnerability and mortality may be due to the increased prevalence of smoking among Chinese men compared with women.2,3 However, until recently, clinical data were lacking. A study of 78 COVID-19 patients found that history of smoking increased the risk for disease progression by more than 14-fold. 4 However, the association was weak and with a wide 95% confidence interval (CI) since only five smoking patients were included, of whom three progressed to severe disease. A meta-analysis of five case series from China found that current smokers had a statistically insignificant increase in the odds of progressing to severe COVID-19. 5 However, another systematic review reported that smokers were more likely to be admitted to an intensive care unit (ICU), need mechanical ventilation, or die compared with non-smokers. 6
Smoking is an established risk factor for a variety of diseases, including cardiovascular disease and chronic obstructive pulmonary disease (COPD), which appear to be risk factors for severe COVID-19 and adverse outcome. 7 Thus, it would be expected for smokers to be over-represented among COVID-19 patients. Still, in a recent meta-analysis of 13 studies of hospitalized COVID-19 patients in China, an unexpectedly low prevalence of smoking, approximately one-fourth the population smoking prevalence, was found. 8 To further explore this issue, we performed a systematic review of case series presenting data on the smoking status of hospitalized COVID-19 patients in order to:
Calculate the pooled prevalence of smoking among hospitalized COVID-19 patients and compare it with the expected prevalence based on population smoking rates.
Examine the association between current, compared with non-current and former, smoking and adverse outcome in COVID-19.
Methods
Studies included
A systematic search of the literature (PubMed) was performed for studies published until 25 April 2020 using the terms “(SARS-CoV-2 OR COVID-19 OR 2019-nCoV) AND (Clinical OR Mortality OR Outcome)” in the title or the abstract. Studies were included in the analysis if they satisfied all of the following criteria:
Present hospitalized patients with COVID-19
Classify patients according to disease severity, irrespective of the severity definition
Present data on the smoking status, separately for each severity classification.
Out of a total of 1398 studies, 19 studies fulfilling the previously mentioned criteria were found.4,9–26 One study was excluded because of unreliable data since the sum of current and former smokers did not correspond to the numbers presented in different severity subgroups. 26 Thus, 18 studies were analyzed. All of the studies were retrospective observational case series. The PRISMA flow diagram is presented in the Supplemental Figure S1. Most of the studies were from China (n = 15), while two studies presented patients from the United States (US) and one from South Korea. Four of the studies recorded separately current and former smokers and were used to examine the association between current, rather than former, smoking and adverse outcome.9,13,20,21 The rest of the studies reported the smoking status as “smoking” or “history of smoking” and may have included former smokers. Three studies had missing smoking data on 14 of 1099, 44 of 645, and 22 of 476 patients.9,16,23 The number of patients with available smoking data (1085, 601 and 454, respectively) were used in the calculations. Another study reported unknown smoking history for 13 out of 487 patients (all with mild disease) 17 ; they were also excluded from the analysis.
In addition, we sought to identify pre-publications (not peer-reviewed) on the pre-print server Medrxiv. The terms “smoking” and “COVID-19” were sought in the title or abstract. A total of 123 pre-publications were found, with 12 fulfilling the previously mentioned criteria.27–38 All of the studies were retrospective observational case series. Of these, nine were from China, two from the US, and one from Japan. Two of the studies recorded current and former smokers separately.27,31 The rest of the studies reported smoking status as “smoking” or “history of smoking” and may have included former smokers. One study from the US reported never smokers or unknown history of smoking as one group, without clarifying how many patients had missing data. 27 Another study reported the smoking status and outcomes for 170 of 200 patients. 29 In total, 30 studies (published and pre-publications) were used in the secondary analysis, whereas 6 studies were used to examine the association between current versus former smoking and adverse outcome.
Analysis
A cross-sectional analysis was performed. In two studies, both outpatients and hospitalized patients were presented.20,27 In one of them, 7162 patients were presented in total, of whom 5143 were ambulatory, 1037 were hospitalized in non-ICU units, 457 were hospitalized in ICU units, and for 525 patients the hospitalization status was unknown. 20 Only hospitalized patients (n = 1494) were included to the analysis. In the other study, 2104 patients were ambulatory and 1999 were hospitalized. 27 Of those hospitalized, 1582 were included in the analysis since 932 were classified as “discharged with no critical illness” and 650 as having “critical illness.” In studies where former smokers were not separately presented, all patients with a positive smoking history were classified as current smokers. When presented separately, former smokers were included in the non-current smoking group.
The pooled prevalence of current smoking was calculated using random-effects meta-analysis. Smoking prevalence in each study was compared with the expected prevalence based on gender-specific population smoking rates. The expected prevalence of smoking in each study was calculated using the gender distribution of patients in each study and the gender-specific population smoking prevalence. The following formula was used:

where SPE = expected smoking prevalence; PM = male prevalence among patients; SPP–M = population smoking prevalence in males; PF = female prevalence among patients; and SPP–F = population smoking prevalence in females.
The observed smoking prevalence was compared with the expected smoking prevalence by calculating prevalence odds ratio (POR). 39 The population smoking rates used to calculate the gender-adjusted expected number of smokers in each study were (males and females, respectively): 50.5% and 2.1% for China, 40 15.6% and 12.0% in the US, 41 35.8% and 6.5% in South Korea, 42 and 29.3% and 7.2% in Japan. 43
The studies analyzed did not include data on the patients’ age distribution. Therefore, age-adjustment in the expected smoking prevalence calculation was performed by assuming that all patients were ⩾65 years old. This represents a worst-case scenario considering that people aged ⩾65 years have the lowest smoking rates compared with other adult age groups while the mean or median age of hospitalized COVID-19 patients was by far lower than 65 years in the studies examined (Table 1). Thus, this approach underestimates the expected smoking prevalence. The population smoking rates used to calculate the age and gender-adjusted expected number of smokers in each study were (males and females, respectively): 44.0% and 4.1% for China, 40 10.1% and 7.7% in the US, 44 17.9% and 1.9% in South Korea, 45 and 21.2% and 5.4% in Japan.46,47 The formula mentioned previously was applied to calculate the gender and age-adjusted expected smoking prevalence. We report both gender-adjusted and gender and age-adjusted POR. The association between current (versus non-current) smoking and adverse outcome was performed by calculating the odds ratio (OR). In addition, the association between current smoking (versus former smoking) and adverse outcome was calculated using the studies that presented data for former smokers separately; never smokers were excluded from the latter analysis. All analyses were performed with random-effects meta-analyses using MetaXL v5.3, with heterogeneity evaluated through I2 and publication bias examined by visual assessment of funnel plots.
Characteristics of the studies included in the analysis.

Blank cells represent non-available data or multiple age groups.
IQR, interquartile range; SD, standard deviation; US, United States.
Results
Study characteristics
The characteristics of the studies included in this analysis are presented in Table 1. Published studies included 6515 hospitalized patients, of whom 440 were current smokers. Together with the pre-publications, 10,631 patients, with 961 of them being smokers, were examined. Adverse outcomes ranged from non-specific “severe” to specific definitions based on clinical criteria or death. No publication bias was obvious from the funnel plot. Outcome definitions for each study are presented in Supplemental Table S1.
Primary analysis (published studies)
In published studies, the random-effects pooled prevalence of current smoking was 6.8% (95% CI 4.8–9.1%). The gender-adjusted POR, displayed in Figure 1, was 0.20 (95% CI: 0.16–0.25, p < 0.001) with substantial heterogeneity being observed (I2 = 68%). The gender and age-adjusted POR, displayed in Figure 2, was 0.24 (95% CI: 0.19–0.30, p < 0.001) with substantial heterogeneity being observed (I2 = 66%). In Chinese studies only, the gender-adjusted POR was 0.20 (95% CI: 0.16–0.26, p < 0.001) and the gender and age-adjusted POR was 0.22 (95% CI: 0.18–0.28, p < 0.001).

POR of current smoking among hospitalized patients with COVID-19 (gender-adjusted). Data from 18 published studies.
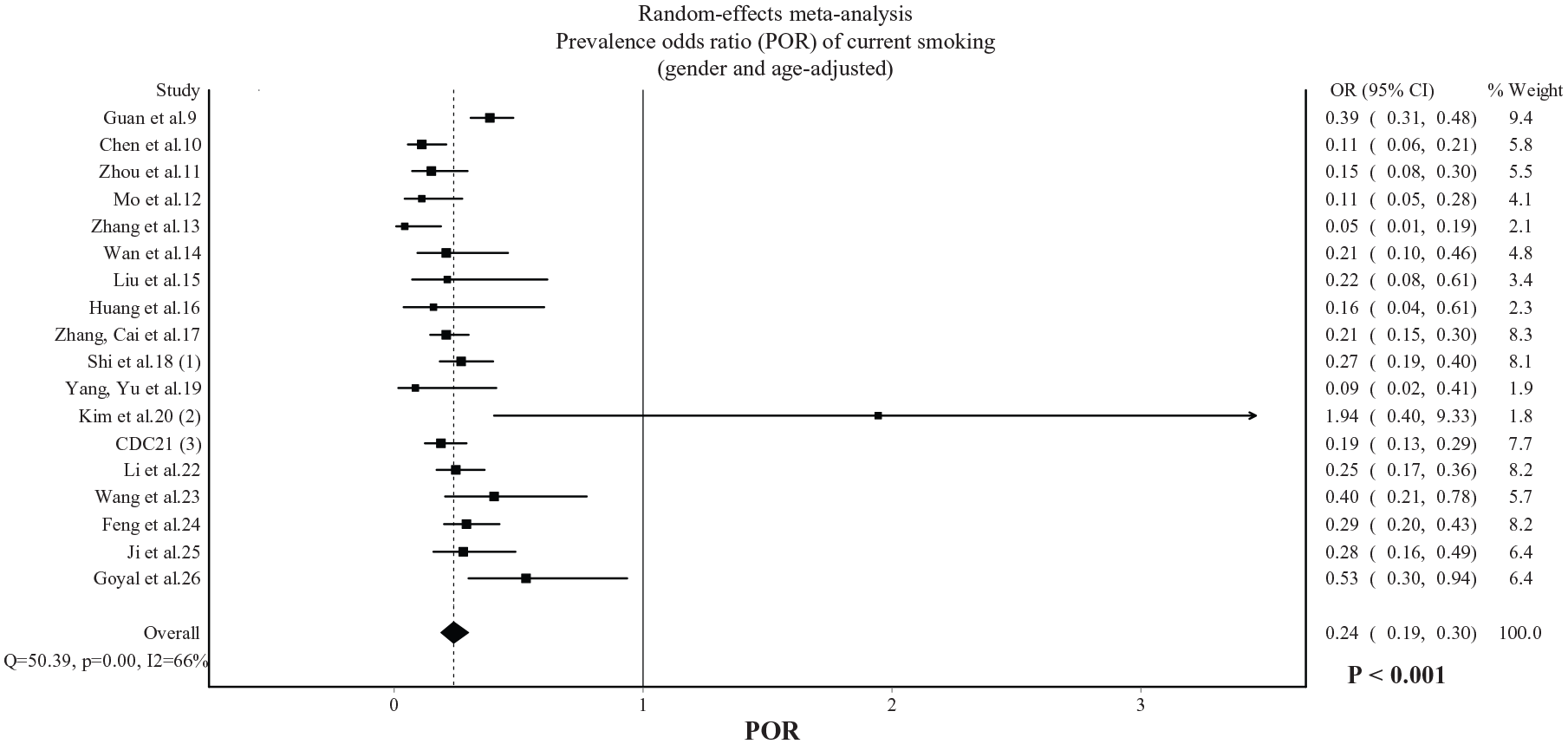
POR of current smoking among hospitalized patients with COVID-19 (gender and age-adjusted). Data from 18 published studies.
Current smokers were more likely than non-current smokers to experience an adverse outcome (OR: 1.53, 95% CI: 1.06–2.20, p = 0.022), with moderate heterogeneity being observed (I2 = 43%, Figure 3). Compared with former smokers, current smokers were less likely to experience an adverse outcome (OR: 0.42, 95% CI: 0.24–0.74, p = 0.003), with no heterogeneity being observed (I2 = 0%, Figure 4).

Association between current (versus non-current) smoking and adverse outcome in COVID-19. Data from 18 published studies.

Association between current (versus former) smoking and adverse outcome in COVID-19. Data from 4 published studies.
Secondary analysis (published studies and pre-publications)
From the secondary analysis, which included both published studies and pre-publications, the random-effects pooled prevalence of current smoking was 9.0% (95% CI: 6.5–11.8%). The gender-adjusted POR, displayed in Supplemental Figure S2, was 0.27 (95% CI: 0.19–0.38, p < 0.001), with considerable heterogeneity being observed (I2 = 93%). The gender and age-adjusted POR, displayed in Supplemental Figure S3, was 0.34 (95% CI: 0.24–0.48, p < 0.001), with considerable heterogeneity being observed (I2 = 93%). In Chinese studies only, the gender-adjusted POR was 0.24 (95% CI: 0.17–0.33, p < 0.001) and the gender and age-adjusted POR was 0.27 (95% CI: 0.20–0.38, p < 0.001).
Current smokers were more likely than non-current smokers to experience an adverse outcome (OR: 1.59, 95% CI: 1.15–2.21, p = 0.006) with moderate heterogeneity being observed (I2 = 67%, Supplemental Figure S4). Compared with former smokers, current smokers were less likely to experience an adverse outcome (OR: 0.61, 95% CI: 0.36–1.02, p = 0.056) with moderate heterogeneity being observed (I2 = 54%, Supplemental Figure S5).
Discussion
The main finding of this systematic review was the unusually low prevalence of current smoking among hospitalized COVID-19 patients. Smoking prevalence was less than one-fourth the expected prevalence based on gender-adjusted population smoking rates. Even when age-adjustment was performed by calculating expected prevalence based on the age group with the lowest population smoking rates (age ⩾ 65 years), smoking prevalence in hospitalized COVID-19 patients was still approximately one-third the expected prevalence (66% lower). Current smokers had higher odds for adverse outcome compared with non-current smokers. In contrast, current smokers were less likely to have an adverse outcome compared with former smokers.
An important limitation is that the analysis was unadjusted for confounding factors such as comorbidities that appear to be associated with higher risk for an adverse outcome in COVID-19. 48 Sociodemographic factors may also be associated with reduced access of smokers to hospital care. Older age is usually associated with lower current smoking and higher former smoking prevalence, which could explain the lower odds for adverse outcome in current compared with former smokers. However, China has a high smoking prevalence even in older age groups. Liu et al. reported a prevalence of >50% in smoking males aged 60–69 years and >40% in those >70 years.40,49 Moreover, we performed age-adjustment by calculating the expected prevalence based on the adult age group with the lowest population smoking prevalence. Still, the difference between observed and expected smoking prevalence was substantial. There were no available data to further adjust expected prevalence based on geographically-specific population smoking rates. The possibility for inaccurate recording, false-reporting, or inability to report the smoking status due to critical condition of patients admitted to the hospitals, as well as the lack of an objective assessment of the smoking status, should also be considered. Still, the findings that smokers are under-represented by approximately 3- to >4-fold compared with population smoking rates could be explained only by unusually extensive under-reporting of the current smoking status. Finally, many studies reported smoking history instead of current smoking, which might include former smokers and thus overestimate current smoking prevalence among hospitalized COVID-19 patients.
Low prevalence of current smokers among hospitalized COVID-19 patients has been observed in case series outside China too.20,25,27,50 While it is highly unlikely for the majority of cigarette smoke compounds to have any potential benefit considering their toxic characteristics and oxidative stress and inflammation-promoting properties, some researchers have hypothesized that these findings might imply a protective effect of nicotine.50–53 It was recently reported that many of the clinical manifestations of COVID-19 could be explained by a dysfunction of the nicotinic cholinergic system, and it was hypothesized that nicotine could modulate the immune response by restoring the function of the cholinergic anti-inflammatory pathway. 52 Severe COVID-19 appears to represent a hyper-inflammatory response that could result from dysregulation of the immune system and a failure to return to homeostasis after being activated to combat viral invasion. SARS-CoV-2 activates the innate immune system, which, if left unregulated, can increase vascular permeability, cause migration of fluid and blood cells into the alveoli, and result in respiratory failure. 54 This is commonly called “cytokine storm”, and is characterized by the release of several pro-inflammatory cytokines such as tumor necrosis factor (TNF), interleukin (IL)-1, and IL-6. Elevated levels of these cytokines have been associated with poor prognosis in COVID-19 patients.11,55 The importance of this process in severe COVID-19 has been recognized by the scientific community, and clinical trials of immunosuppressants and cytokine inhibitors are already underway based on biological plausibility and despite warnings and precautions against the use of such medication in the presence of active infection.56–60 The cholinergic anti-inflammatory pathway, mediated mainly through the vagus nerve and alpha 7 nicotinic acetylcholine receptors, has well-established immunomodulatory effects that are present in a variety of cells such as macrophages and bronchial epithelial and endothelial cells.61–64 It represents a reflex mechanism based on a bi-directional communication between the immune and nervous systems. Activation of the cholinergic anti-inflammatory pathway through electrical stimulation of the vagus nerve has been shown to reduce levels of pro-inflammatory cytokines and control the acute hyper-inflammatory response in animal models.65,66 Therefore, dysregulation of the cholinergic nervous system could explain the clinical manifestations of severe COVID-19 and the inability to suppress and control the inflammatory response. Notably, risk factors for severe COVID-19 such as diabetes, heart disease, ageing and obesity are characterized by autonomic nervous system imbalance.67–70 These patients are expected to be more sensitive to further compromise of the cholinergic nervous system due to SARS-CoV-2 infection.
Nicotine is an agonist of the nicotinic cholinergic system and has been shown to prevent acute respiratory distress syndrome, the hallmark of severe COVID-19, in animal models. 71 Therefore, we present the hypothesis that nicotine intake could be the reason for the low prevalence of smoking among hospitalized COVID-19 patients. This would seemingly be in disagreement with the higher odds of adverse outcomes among hospitalized COVID-19 smokers. However, it should be emphasized that smokers experience abrupt cessation of nicotine intake after hospital admission and are unlikely to receive pharmaceutical nicotine replacement therapies while hospitalized. As a result, the effects of nicotine will rapidly wean off within hours after admission considering that the plasma half-life of nicotine is 1–2 h. Therefore, the higher odds for adverse outcome in current, compared with non-current, smokers are not contradictory to the hypothesis that nicotine may be beneficial for COVID-19. In addition, any hypothesized benefits of nicotine are expected to be masked by the well-established adverse effects of smoking and smoking-related comorbidities, which could also explain the higher odds for adverse outcome in hospitalized smokers. Thus, it is possible that COVID-19 severity and outcome may differ between smokers without and with smoking-related disease. Therefore, smoking cannot be recommended or used as a protective or therapeutic measure. However, pharmaceutical nicotine products have been available for years and have been used therapeutically even in non-smokers for longer periods of time compared with the few days that would be needed for a clinical trial of nicotine in COVID-19 patients.72,73 The safety profile and lack of dependence potential that has been observed in these studies, with pharmaceutical nicotine being administered to elderly non-smokers at high doses and for several weeks, offers a rationale for future clinical trials of nicotine in COVID-19 patients. In addition, such a clinical trial would not need to administer nicotine as a substitute for other standardized therapeutic measures.
Another concern in relation to nicotine and COVID-19 refers to its effects on angiotensin converting enzyme 2 (ACE2) expression, since this enzyme is used as a receptor by SARS-CoV-2 for cell entry. 74 Recent data support that nicotine upregulates ACE2, which is suggested as a potential mechanism to increase susceptibility and severity of COVID-19.75,76 However, this is in contrast with previous data that nicotine and smoking down-regulate ACE2. 77 Moreover, up-regulation of ACE2 does not necessarily imply more fulminant disease. Concerns that up-regulation of ACE2 by ACE-inhibitors and angiotensin receptor blockers could be linked to adverse prognosis in hypertensive COVID-19 patients were raised early in the COVID-19 pandemic. 78 However, recent studies found either no adverse effect or a protective effect associated with the use of these medications.79,80 In fact, down-regulation of ACE2 immediately after viral cell entry is proposed as an important mechanism favoring the progression and severity of disease. 81 ACE2 deficiency has been observed with ageing, in diabetes mellitus, and in heart disease, all of which appear to be risk factors for severe COVID-19.82–84 In addition, children and young women, who usually experience mild COVID-19, were found to have higher levels of ACE2 than older people. 85 Thus, it is possible that ACE2 upregulation is protective against severe COVID-19,78,86 and the contradictory data about the effects of nicotine on ACE2 expression need to be clarified in future experimental studies.
In conclusion, this systematic review and meta-analysis of retrospective, observational case series identified a low prevalence of current smoking among hospitalized COVID-19 patients but higher odds of adverse outcome for current compared with non-current smokers. Smoking cannot be considered a protective measure against COVID-19 (or any other condition) due to associated risk for cardiovascular, respiratory and cancer morbidity and mortality. Thus, smokers should still be encouraged to quit. While limitations are applicable to this analysis and other unknown reasons or confounding factors could, at least partially, explain these findings, the hypothesis that nicotine may be protective against severe COVID-19 is biologically plausible and should be explored through laboratory and, eventually, clinical trials using pharmaceutical nicotine products.
Supplemental Material
PRISMA_checklist-filled – Supplemental material for Current smoking, former smoking, and adverse outcome among hospitalized COVID-19 patients: a systematic review and meta-analysis
Supplemental material, PRISMA_checklist-filled for Current smoking, former smoking, and adverse outcome among hospitalized COVID-19 patients: a systematic review and meta-analysis by Konstantinos Farsalinos, Anastasia Barbouni, Konstantinos Poulas, Riccardo Polosa, Pasquale Caponnetto and Raymond Niaura in Therapeutic Advances in Chronic Disease
Supplemental Material
Supplementary_file – Supplemental material for Current smoking, former smoking, and adverse outcome among hospitalized COVID-19 patients: a systematic review and meta-analysis
Supplemental material, Supplementary_file for Current smoking, former smoking, and adverse outcome among hospitalized COVID-19 patients: a systematic review and meta-analysis by Konstantinos Farsalinos, Anastasia Barbouni, Konstantinos Poulas, Riccardo Polosa, Pasquale Caponnetto and Raymond Niaura in Therapeutic Advances in Chronic Disease
Supplemental Material
Supplementary_file_TAJ – Supplemental material for Current smoking, former smoking, and adverse outcome among hospitalized COVID-19 patients: a systematic review and meta-analysis
Supplemental material, Supplementary_file_TAJ for Current smoking, former smoking, and adverse outcome among hospitalized COVID-19 patients: a systematic review and meta-analysis by Konstantinos Farsalinos, Anastasia Barbouni, Konstantinos Poulas, Riccardo Polosa, Pasquale Caponnetto and Raymond Niaura in Therapeutic Advances in Chronic Disease
Footnotes
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KF is a non-paid, external associate at the Laboratory of Molecular Biology and Immunology of the University of Patras. Concerning the current work, he participates in a patent application for pharmaceutical cholinergic agonists, monoclonal antibodies and diagnostic tests for COVID-19.
KP participates in a patent application for pharmaceutical cholinergic agonists, monoclonal antibodies and diagnostic tests for COVID-19. He is the principle investigator in NOSMOKE, an institute located at Patras Science Park, which has received in the past a grant by the Foundation for a Smoke-Free World.
RP is full tenured Professor of Internal Medicine at the University of Catania (Italy) and Medical Director of the Institute for Internal Medicine and Clinical Immunology at the University of Catania. In relation to his recent work in the area of respiratory diseases, clinical immunology, and tobacco control, RP has received lecture fees and research funding from Pfizer, GlaxoSmithKline, CV Therapeutics, NeuroSearch A/S, Sandoz, MSD, Boehringer Ingelheim, Novartis, Duska Therapeutics, and Forest Laboratories. Lecture fees from a number of European EC industry and trade associations (including FIVAPE in France and FIESEL in Italy) were directly donated to vaping advocacy nonprofit organisations. RP has also received grants from European Commission initiatives (U-BIOPRED and AIRPROM) and from the Integral Rheumatology and Immunology Specialists Network (IRIS) initiative. RP has served as a consultant for Pfizer, Global Health Alliance for treatment of tobacco dependence, CV Therapeutics, Boehringer Ingelheim, Novartis, Duska Therapeutics, ECITA (Electronic Cigarette Industry Trade Association, in the UK), Arbi Group Srl, and Health Diplomats. RP has served on the medical and scientific advisory board of Cordex Pharma, CV Therapeutics, Duska Therapeutics, Pfizer, and PharmaCielo.
RP is also founder of the Center for Tobacco prevention and treatment (CPCT) at the University of Catania and of the Center of Excellence for the acceleration of HArm Reduction (CoEHAR) at the same University, which has received support from the Foundation for a Smoke Free World to conduct eight independent investigator-initiated research projects on harm reduction. RP is currently involved in a patent application concerning a smartphone app tracker for smoking behavior developed for ECLAT. RP is also involved in the following pro bono activities: scientific advisor for Lega Italiana Anti Fumo, the Consumer Advocates for Smoke-free Alternatives, and the International Network of Nicotine Consumers Organizations; and Chair of the European Technical Committee for standardisation on “Requirements and test methods for emissions of electronic cigarettes” (CEN/TC 437; WG4).
PC is paid by the University of Catania as an external part-time researcher and adjunct professor of clinical, addiction, and general psychology. In 2015 he won an unrestricted grant from Pfizer, GRAND, Global Research Award for Nicotine Dependence. He has been affiliated to the CoEHAR since December 2019 in a pro bono role. He is coauthor of a protocol paper supported by an Investigator-Initiated Study award program established by Philip Morris International in 2017.
AB and RN have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.