
Abstract
Background:
Little is known about the treatment outcomes of secukinumab in clinical practice, which differ from those in clinical trials. The effectiveness of biologics may differ in psoriasis patients with previous biologics exposure. The objective of this study was to investigate the real-world effectiveness and safety of secukinumab therapy and analyze subgroups stratified by reimbursement or prior biologic failure.
Methods:
This retrospective multicenter study collected data from a cohort of 118 consecutive patients who received secukinumab treatment between December 2015 and March 2018. Effectiveness was evaluated by degree of improvement in the Psoriasis Area and Severity Index (PASI) scores. Adverse events and reasons for discontinuation were also recorded.
Results:
The mean PASI improvement rate at weeks 4, 12, 24, and 36 was 63.5%, 77.7%, 78.7%, and 76.0%, respectively. Compared with reimbursed patients, nonreimbursed patients had a significantly lower baseline PASI and a shorter mean disease duration of psoriasis; they were more frequently biologic-naïve, had used less prior traditional antipsoriatic drugs and were more likely to be treated with secukinumab 150 mg. The effectiveness of secukinumab in nonreimbursed patients was superior despite higher discontinuation rates. Compared with patients without prior biologic failure, patients with prior biologic failure had a significantly lower mean PASI improvement at weeks 12, 24, 36, and 48. The decline in response rates to secukinumab tended to be more pronounced for patients who failed ustekinumab than tumor necrosis factor-α inhibitors. Moreover, the number of prior biologic failures was associated with a decreased response rate and increased likelihood of secondary loss of effectiveness of secukinumab therapy.
Conclusion:
In a real-life clinical setting, the characteristics of nonreimbursed patients receiving secukinumab treatment differed from those of reimbursed patients. The PASI improvement for secukinumab was substantial but lower than that in clinical trials. The number and classes of prior biologic failures impact the treatment response to secukinumab.
Keywords
Introduction
Several pivotal phase III randomized controlled trials (RCTs) have demonstrated a promising efficacy of secukinumab for the treatment of moderate-to-severe plaque psoriasis.1–3 However, daily clinical practice is much different from the strictly regulated setting of RCTs, which are conducted in selected patients fulfilling strict inclusion and exclusion criteria to maximize internal validity. Thus, trial results might have limited external validity in daily practice. Patients who failed or exposed some kinds of biologics and have significant comorbidities are usually excluded from RCTs.4–7 Up to 30% of patients in a real-world setting would be ineligible for RCTs. 4 A washout period of topical and systemic therapies is required in RCTs, whereas combination therapies, commonly seen in daily practice, are usually not allowed. The aforementioned discrepancy might affect real-world treatment outcomes of secukinumab.
Moreover, switching of biologics, which is tightly associated with prior exposure to or failure of biologics, occurs commonly in daily practice. Registry data (PSOLAR and BADBIR) have also suggested that the discontinuation of a prior biologic therapy was a predictor of lower drug survival with subsequent biologics.8,9 However, a study investigating the impact of previous biologic use, including interleukin (IL) 12/23 and tumor necrosis factor-α inhibitor (TNFi), on the effectiveness and safety of secukinumab treatment in a real-world clinical setting is lacking. Moreover, in the real world, a certain proportion of biological treatment cases are nonreimbursed. 10 Nonreimbursed psoriasis patients who receive biologics may differ in some respects (e.g. comorbidities, prior treatments) from those who are eligible for reimbursement, and this has been rarely studied. Data of secukinumab treatment in an Asian population in a real-world setting are limited by small numbers of cases. 11 Thus, we conducted this multicenter study to assess the real-world effectiveness and safety of secukinumab therapy. A further subgroup analysis was also performed to compare the characteristics of nonreimbursed and reimbursed patients with psoriasis and investigate the impact of different types of prior biologic therapy on subsequent secukinumab treatment effectiveness.
Materials and methods
Study population
This retrospective study reviewed the clinical records of patients with moderate to severe plaque psoriasis who received secukinumab treatment between December 2015 and March 2018 at four dermatology centers in different regions of Taiwan. Based on the Bureau of National Health Insurance reimbursement policy in Taiwan, secukinumab treatment is reimbursed for psoriasis patients who have a Psoriasis Area and Severity Index (PASI) ⩾ 10 and inadequate response, contraindication, or intolerance to at least two of the three conventional systemic agents including methotrexate (⩾15 mg/week), acitretin (0.3–1 mg/kg/day), and cyclosporine (3.5–5 mg/kg/day) in addition to narrow-band ultraviolet B or psoralen ultraviolet A phototherapy at least twice weekly for 3 months.10–14
Prior to secukinumab treatment, all patients underwent screening for the presence of hepatitis B virus (HBV) surface antigen (HBsAg), hepatitis C virus (HCV) antibody, and latent tuberculosis (TB) by chest X-ray and QuantiFERON®-TB Gold (QFT-G) (Cellestis, Melbourne, Victoria, Australia).5,15,16 A 9-month isoniazid prophylaxis was recommended for patients with positive QFT-G results.15,16 Patients were also referred to respiratory specialists if there was a suspicion of TB on clinical or laboratory findings. HBV and HCV viral loads were checked regularly and antiviral treatment was provided as indicated.5,17,18
Ethical approval was obtained from the local Institutional Review Board of National Taiwan University Hospital (201207080RIC); National Taiwan University Hospital, Hsin-Chu branch (103-082-E, 104-008-F); and Chang Gung Memorial Hospital, Linkou and Taipei branches (201801101BOD001). Written informed consent was obtained from all participants.
Treatment protocol and efficacy assessment
In Taiwan, secukinumab 300 mg is reimbursed for patients weighing > 60 kg, whereas secukinumab 150 mg is given to patients weighing ⩽ 60 kg. Subcutaneous secukinumab was administrated once weekly at weeks 0, 1, 2, 3, and 4 and every 4 weeks thereafter. 11 Nonreimbured patients who weighted > 60 kg but received secukinumab treatment at a dose of 150 mg were excluded. efficacy analyses were conducted throughout the study by assessment of PASI score improvement calculated at each visit. Prior biologic failure was defined as primary failure to reach a 50% improvement in PASI (PASI 50) compared with baseline or secondary loss of PASI 50 during previous biologic therapy for psoriasis. Patients were also asked to report all adverse events (AEs) since the last visit and report changes in comorbidities and concomitant medication.
Statistical analysis
The effectiveness of the different dosages was compared between the two treatment groups. These analyses were conducted using the Wilcoxon rank sum test for continuous variables and the chi-squared test or Fisher’s exact test for discrete variables. In addition, logistic regression analyses with adjustment for covariates collected at study entry were performed to identify factors associated with achieving a maximum PASI improvement ⩾ 75 (PASI 75) on secukinumab treatment. The statistical analysis of the data was performed using the SPSS 21 statistical package (IBM Corporation, Chicago, IL, USA). In all cases, a p value < 0.05 (two-tailed) was considered statistically significant.
Results
A total of 118 psoriasis patients (88 men [74.6%], 30 women [25.4%]) treated with secukinumab were included. The mean ± SD baseline PASI was 18.5 ± 10.0. The mean ± SD duration of secukinumab treatment was 10.6 ± 4.5 months (range, 3–24 months) (Table 1). The mean PASI improvement rates at weeks 4, 12, 24, and 36 were 63.5%, 77.7%, 78.7%, and 76.0%, respectively.
Patient demographic and baseline clinical characteristics and efficacy and safety outcomes following secukinumab treatment.

PASI, Psoriasis Area and Severity Index; SD, standard deviation; *p < 0.05; **p < 0.01; ***p < 0.001.
Reimbursed versus nonreimbursed patients
A total of 94 patients (79.4%) received reimbursed secukinumab, whereas the other 24 patients (20.3%) received nonreimbursed secukinumab. Compared with reimbursed patients, the nonreimbursed patients had a significantly lower baseline PASI and a shorter mean disease duration of psoriasis. Moreover, a higher percentage of nonreimbursed patients were biologic-naïve, and fewer prior traditional antipsoriatic drugs had been used compared with reimbursed patients. The effectiveness of secukinumab in nonreimbursed patients was superior to that in reimbursed patients, although the proportion of secukinumab 150 mg used was higher in nonreimbursed than in reimbursed patients (Supplementary Table S1). The discontinuation of secukinumab therapy was reported in higher proportions of nonreimbursed patients than reimbursed patients. The most common reason for discontinuing treatment was financial reasons and almost full clearing of lesions in nonreimbursed patients versus secondary loss of efficacy in reimbursed patients (Supplementary Table S2).
Patients without prior failure versus with prior failure of biologic
Of 118 patients included, 53 (44.9%) had not failed any biologics previously, whereas 65 (55.1%) patients had experienced at least one biologic failure before the start of secukinumab therapy. In real-world practice, patients with prior failure of biologic tended to have a longer disease duration, weigh more, be exposed to more traditional antipsoriatic drugs, have a higher proportion of concomitant psoriatic arthritis, and have a higher PASI score at baseline than patients without prior biologic failure (Table 1 and Supplementary Table S3). Mean PASI improvement was higher in patients without prior biologic failure than in those with biologic failure at week 4 (65% versus 62%, p = 0.43), week 12 (83% versus 74%, p = 0.04), week 24 (83% versus 75%, p = 0.06), week 36 (85.4% versus 71.2%, p = 0.007), and week 48 (82.4 versus 67.2%, p = 0.009) (Figure 1(a)). The response rates of PASI 50 at weeks 12 and 24, PASI 75 at weeks 12 and 24, and PASI 90 at week 36 in patients without prior biologic failure were also significantly greater than those with prior biologic failure (Supplementary Table S4). We found a similar result regarding absolute PASI score. The percentage of patients who reached an absolute PASI score ≦2, ≦3, and ≦5 tended to be higher in patients without prior biologic failure than those with prior biologic failure (Supplemental Figure 1)
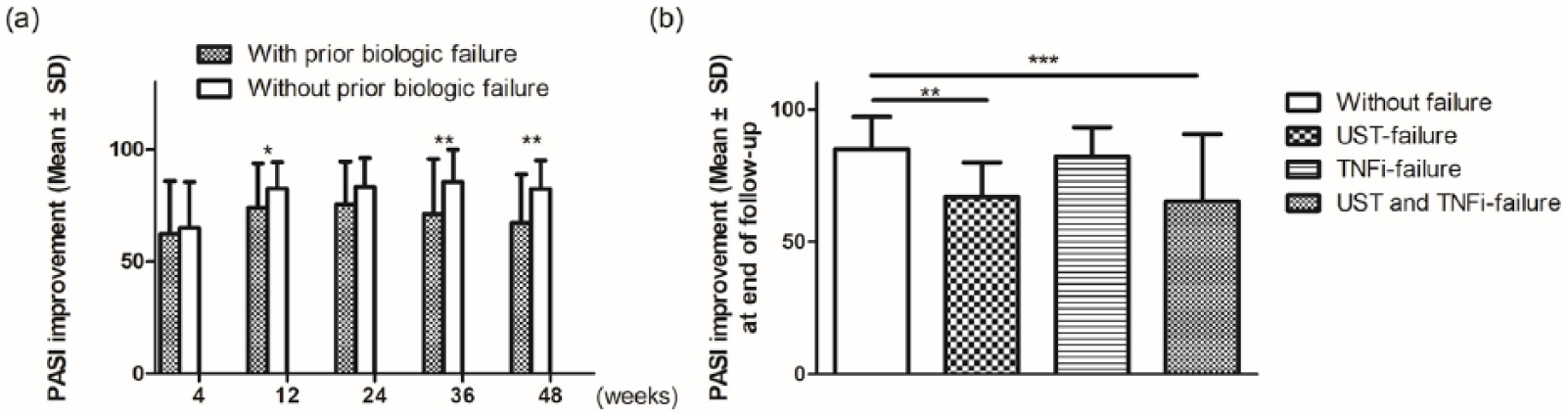
Impact of previous biologic failure on secukinumab therapy. (a) Comparison of mean PASI improvement between patients without and with prior biologic failure. (b) Difference in PASI improvement among patients without prior bioloigc failure and those who failed different biologics. *p < 0.05, **p < 0.01, ***p < 0.001 for comparison between patients with and without prior biologic failure. PASI, Psoriasis Area and Severity Index.
To examine whether the relationship of previous biologic failure and response to subsequent secukinumab therapy was different for TNFi than ustekinumab (UST), which has different mode of action (MOA), we subdivided our population of patients into those without prior biologic failure, those who failed UST, those who failed TNFi, and those who failed both UST and TNFi. Compared with those without prior biologic failure, those who failed both UST and TNFi had the least PASI improvement (65.2%) at the end of follow up, followed by those who failed UST (67.0%) and then those who failed TNFi (82.1%) (Figure 1(b)). The decline in response rates to secukinumab treatment tended to be more pronounced for patients who failed UST than for those who failed TNFi.
Moreover, we found that the number of prior biologic failures was significantly associated with effectiveness and loss of effectiveness of secukinumab treatment. The more prior biologic failures patients experienced, the less PASI improvement they had. Moreover, the likelihood of losing 20% of maximum PASI improvement to secukinumab treatment increased in parallel with an increasing number of prior biologic failures (Figure 2).
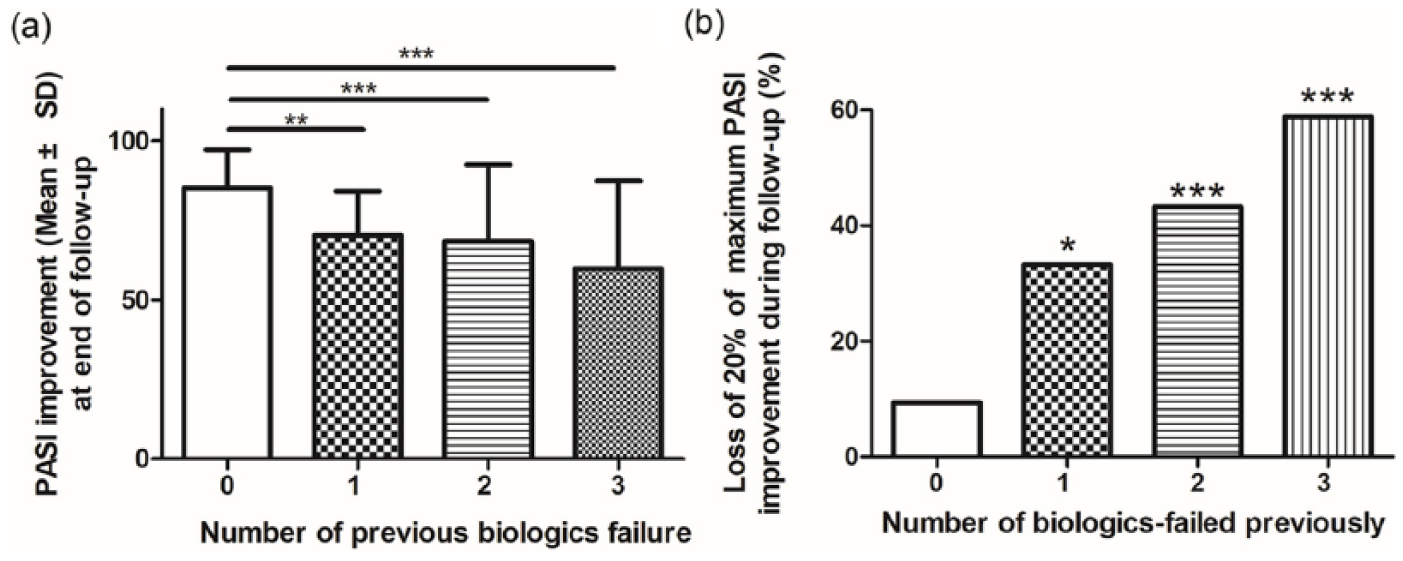
The relationship between number of prior biologic failures and PASI improvement at end of follow up (a) and loss of 20% of maximum PASI improvement during secukinumab treatment (b). *p < 0.05, **p < 0.01, ***p < 0.001 for comparison between patients with and without prior biologic failure.
Factors affecting secukinumab effectiveness
Multivariate analysis using Cox regression showed the absence of prior biologic failure (odds ratio [OR] = 18.8; p = 0.006), and female (OR = 13.40; p = 0.04) was the significant variable associated with achieving maximum PASI improvement ⩾ 75 on secukinumab treatment after the adjustment for confounding variables.
Safety
A total of 72 AEs were reported, most of which were similar to those reported in previous studies.1–3 Commonly reported treatment-induced AEs included upper respiratory tract infection (16.1%), nasopharyngitis (7.6%), arthralgia (6.7%), inflamed epidermal inclusion cyst (4.2%), and diarrhea (4.2%).
Sensitivity analysis
In sensitivity analysis that restricted the study population to reimbursed patients, the results were similar. As compared with patients who had not failed any biologics previously, those with history of failure with previous biological drugs had a worse response and also worse maintenance of the response in the medium and long term. The number of prior biologic failures remained associated with a decreased response rate and increased likelihood of secondary loss of effectiveness.
Discussion
Several multicenter RCTs have suggested the promising efficacy of secukinumab as a treatment for patients with moderate-to-severe psoriasis.1–3,19 Previous pivotal studies demonstrated that 67.0–71.6% and 77.1–91% of patients achieved their PASI 75 response at week 12 in the secukinumab 150 mg and 300 mg treatment groups, respectively.1–3 A PASI 90 response at week 12 was achieved by 39.1–41.9% of patients in the secukinumab 150 mg group and 54.2–73% of patients in the 300 mg group.1–3 A subanalysis of Taiwanese patients in a phase III global clinical trial (ERASURE) also showed that the proportions of PASI 75 achievement at week 12 were 87.5% with secukinumab 300 mg and 70% with secukinumab 150 mg. 20 Recent studies have investigated the effectiveness and safety of secukinumab in daily practice, which showed effectiveness seems to be less well maintained in real life.21–29 PASI75 response was observed in 52.90–80% of patients treated with secukinumab at week 12 and 68.30–80% had PASI 75 response at week 52.21–29 However, studies investigating the treatment outcomes of secukinumab for Asian populations in real-world clinical practice are lacking. Our study showed that in this real-life setting, about 64% and 28% of patients achieved a PASI 75 and 90 response after 12 weeks of secukinumab treatment, respectively (Supplementary Table S4), which was lower than those shown in previous trials.1–3 The lower response rate to secukinumab could be partially attributed to a higher proportion of patients who had previous biologics exposure (75% versus 11.6–29.8%) or failure (65% versus 2.8–10.7%) in real-world practice than in clinical trials.1–3,20 Similarly, a real-world report from Denmark showed a very high proportion of patients (86%) had previously been treated with a biologic before the start of secukinumab treatment. 30
Although treating psoriasis patients with prior biologic exposure is now commonplace in daily practice, there is a paucity of studies investigating the impact of prior biologic use on the effectiveness of subsequent biologics.31–35 Leman et al. had suggested that the failure of one biologic does not preclude response to another biologic. 32 Nevertheless, previous studies have suggested that failure with prior biologics was predictive of lower drug survival with subsequent biologics.8,9 A retrospective study also showed that PASI 75 response rates to UST at week 24 were significantly better in patients with no prior exposure to TNFi (85% versus 50%, p = 0.0235). 36 A pooled subanalysis of four phase III clinical trials in psoriasis revealed that PASI 90 response rates were lower in subjects with prior exposure to biologics or with prior biologic treatment failure on secukinumab 300 or 150 mg treatment. Galluzzo et al. reported that biologic-naïve patients tended to achieve PASI75, PASI90 and PASI100 with secukinumab treatment faster than biologic-experienced patients (60% versus 41.2%; 42.0% versus 17.0%; 25.5% versus 9.8% at week 4). This finding is in line with our results. 21 We found that patients with prior biologic treatment failure had worse treatment responses to secukinumab than those without prior biologic treatment failure. This result was further corroborated by multivariate regression analysis, which showed that absence of prior biologic failure remained associated with treatment response after the adjustment for confounding variables.
Interestingly, our data showed that among patients with one previously failed biologic, those with previous UST failure had worse PASI improvement than patients with prior TNFi failure when receiving secukinumab treatment. This may be due to the fact that UST, which targets IL 12/23, also inhibits the type 17 T helper/IL17 pathway. Thus, UST and secukinumab at least partially shared a similar MOA to exert their effect at treating psoriasis.33,37 However, large-scale studies are needed to determine whether the prior failure of biologic drugs with the same MOA leads to a greater reduction in efficacy than that with a different MOA.
Our study also found that an increase in the number of prior biologic failures predicted a decreasing response to subsequent secukinumab therapy. Qiang et al. demonstrated that patients with two previously failed biologics were half as likely to respond to the present treatment compared with subjects with just one failed biologic (OR = 0.474; 95% confidence interval [CI] 0.23–0.96; p = 0.04). 38 However, Clemmensen et al. found no difference in the PASI 75 response to UST between the subjects exposed to one, two, or three TNFi. 39
Notably, we also found that the likelihood of secondary loss of effectiveness of secukinumab increased as the number of prior biologic failures increased. Similarly, a recent study by Galluzzo et al. also showed the proportion of patients achieving PASI75, PASI90, and PASI100 was inversely proportional to the number of biological drugs received by patients before secukinumab. 21 Lost effectiveness was commonly observed after the induction phase period. 40 It could be due to the fact that patients with previous failure to biologics have genetic, pharmacokinetic, or extracutaneous factors (i.e. obesity) that could justify a higher chance of failure.
A major limitation of the present study was mainly related to its retrospective nature, which led to the absence of a washout period prior to the start of treatment; the noncomparative study design; the fact that all patients were not treated for the same period of time; and that the patient treatments were not randomized, standardized, or blinded. In addition, the study included a considerable percentage of nonreimbursed patients who have some characteristics (i.e. more frequent use of secukinumab at a dose of 150 mg and higher proportion of treatment discontinuation due to remission of the disease) that are different from those of the main study papulation eligible for reimbursement. This might penalize the survival of the drug, probably leading to potential bias in evaluation of long-term effectiveness. However, in the real world, the stringent local reimbursement criteria limited the access to biologic medication for all patients with psoriasis. The high annual cost of secukinumab treatment (NT$ 643,260 (first year); NT$ 514,608 (subsequent year) for secukinumab 300 mg) also facilitated treatment interruption or intermittent use for nonreimbursed patients, which was in line with a recent study indicating affordability of the biologic drug was the major reason for choosing intermittent, repetitive therapy. 41 Nevertheless, the results of sensitivity analysis which excluded nonreimbursed patients were consistent with those in primary models
Conclusion
Our results complement the data outlined by RCTs and provide efficacy and safety outcomes of secukinumab for psoriasis in a heterogeneous clinically relevant patient population. The number and classes of prior biologic failures affect the effectiveness of secukinumab.
Supplemental Material
Supplemental__Figure_1 – Supplemental material for Effectiveness and safety of secukinumab for psoriasis in real-world practice: analysis of subgroups stratified by prior biologic failure or reimbursement
Supplemental material, Supplemental__Figure_1 for Effectiveness and safety of secukinumab for psoriasis in real-world practice: analysis of subgroups stratified by prior biologic failure or reimbursement by Tzong-Yun Ger, Yu-Huei Huang, Rosaline Chung-yee Hui, Tsen-Fang Tsai and Hsien-Yi Chiu in Therapeutic Advances in Chronic Disease
Supplemental Material
Supplement_Table_S1 – Supplemental material for Effectiveness and safety of secukinumab for psoriasis in real-world practice: analysis of subgroups stratified by prior biologic failure or reimbursement
Supplemental material, Supplement_Table_S1 for Effectiveness and safety of secukinumab for psoriasis in real-world practice: analysis of subgroups stratified by prior biologic failure or reimbursement by Tzong-Yun Ger, Yu-Huei Huang, Rosaline Chung-yee Hui, Tsen-Fang Tsai and Hsien-Yi Chiu in Therapeutic Advances in Chronic Disease
Supplemental Material
Supplement_Table_S2 – Supplemental material for Effectiveness and safety of secukinumab for psoriasis in real-world practice: analysis of subgroups stratified by prior biologic failure or reimbursement
Supplemental material, Supplement_Table_S2 for Effectiveness and safety of secukinumab for psoriasis in real-world practice: analysis of subgroups stratified by prior biologic failure or reimbursement by Tzong-Yun Ger, Yu-Huei Huang, Rosaline Chung-yee Hui, Tsen-Fang Tsai and Hsien-Yi Chiu in Therapeutic Advances in Chronic Disease
Supplemental Material
Supplement_Table_S3 – Supplemental material for Effectiveness and safety of secukinumab for psoriasis in real-world practice: analysis of subgroups stratified by prior biologic failure or reimbursement
Supplemental material, Supplement_Table_S3 for Effectiveness and safety of secukinumab for psoriasis in real-world practice: analysis of subgroups stratified by prior biologic failure or reimbursement by Tzong-Yun Ger, Yu-Huei Huang, Rosaline Chung-yee Hui, Tsen-Fang Tsai and Hsien-Yi Chiu in Therapeutic Advances in Chronic Disease
Supplemental Material
Supplement_Table_S4 – Supplemental material for Effectiveness and safety of secukinumab for psoriasis in real-world practice: analysis of subgroups stratified by prior biologic failure or reimbursement
Supplemental material, Supplement_Table_S4 for Effectiveness and safety of secukinumab for psoriasis in real-world practice: analysis of subgroups stratified by prior biologic failure or reimbursement by Tzong-Yun Ger, Yu-Huei Huang, Rosaline Chung-yee Hui, Tsen-Fang Tsai and Hsien-Yi Chiu in Therapeutic Advances in Chronic Disease
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Taiwan University Hospital, Hsin-Chu branch [grant numbers 108-HCH064 and 107-HCH057] and Chang Gung Memorial Hospital [grant numbers CMRPG2F0332 and CMRPG1F0061], and in part by Basic Research Award, Asia-Pacific La Roche-Posay Foundation 2014. The funders had no role in study design, data collection and analysis, interpretation of findings, manuscript writing, and target journal selection.
Conflict of interest statement
The author(s) declared following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the ICMJE uniform disclosure form available at ![]() , and declare that the following. Dr. Tsen-Fang Tsai has conducted clinical trials or received honoraria for serving as a consultant for Abbvie, Boehringer Ingelheim, Celgene, Eli-Lilly, Galderma, GSK, Janssen-Cilag, Leo Pharma, Merck-Serono, Novartis International AG, and Pfizer Inc. Dr. Hsien-Yi Chiu and Rosaline Chung-yee Hui have received speaking fees from AbbVie, Eli-Lilly, Novartis Pharmaceuticals Corporation, Janssen-Cilag Pharmaceutica, and Pfizer Limited. Dr. Yu-Huei Huang has conducted clinical trials for serving as a principal investigator for Galderma, Eli-Lilly, Novartis Pharmaceuticals Corporation, and Janssen-Cilag Pharmaceutica, received honoraria for serving as an advisory board member for Pfizer Limited, AbbVie, and Celgene, and received speaking fees from AbbVie, Eli-Lilly, and Novartis Pharmaceuticals Corporation. Dr. Tzong-Yun Ger and Dr. Chu-Ju Hung have no conflicts of interest to declare.
, and declare that the following. Dr. Tsen-Fang Tsai has conducted clinical trials or received honoraria for serving as a consultant for Abbvie, Boehringer Ingelheim, Celgene, Eli-Lilly, Galderma, GSK, Janssen-Cilag, Leo Pharma, Merck-Serono, Novartis International AG, and Pfizer Inc. Dr. Hsien-Yi Chiu and Rosaline Chung-yee Hui have received speaking fees from AbbVie, Eli-Lilly, Novartis Pharmaceuticals Corporation, Janssen-Cilag Pharmaceutica, and Pfizer Limited. Dr. Yu-Huei Huang has conducted clinical trials for serving as a principal investigator for Galderma, Eli-Lilly, Novartis Pharmaceuticals Corporation, and Janssen-Cilag Pharmaceutica, received honoraria for serving as an advisory board member for Pfizer Limited, AbbVie, and Celgene, and received speaking fees from AbbVie, Eli-Lilly, and Novartis Pharmaceuticals Corporation. Dr. Tzong-Yun Ger and Dr. Chu-Ju Hung have no conflicts of interest to declare.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.