
Abstract
Recently, autoimmune pancreatitis has been classified into two subtypes. Type 1 is related to immunoglobulin G4 and type 2 is related to granulocytic epithelial lesions, but pathogenetic mechanisms in both still remain unclear. Apart from type 2 autoimmune pancreatitis, the pathological features of type 1 autoimmune pancreatitis with increased serum immunoglobulin G4/immunoglobulin E levels, abundant infiltration of immunoglobulin G4+plasmacytes and lymphocytes, fibrosis, and steroid responsiveness are suggestive of abnormal immunity such as allergy or autoimmunity. Although pathophysiological conditions seem to be different in each, both respond well to steroid drugs. After remission, the patients with type 1 autoimmune pancreatitis show high relapse rates (30–50% within 6–12 months), whereas those with type 2 autoimmune pancreatitis seldom relapse. After remission, the steroid maintenance therapy and therapeutic strategy for relapsing patients with type 1 is different among local expertise. In this paper, recent advances in pathogenesis and clinical guidance for therapy are discussed.
Keywords
Introduction
In 1961, Sarles and colleagues first observed a particular case of pancreatitis with hypergammaglobulinemia [Sarles et al. 1961]. Yoshida and colleagues first proposed the concept of autoimmune pancreatitis (AIP) [Yoshida et al. 1995]. Hamano and colleagues reported increased serum levels of immunoglobulin (Ig) G4 in Japanese patients with AIP [Hamano et al. 2001]. The histopathological findings of AIP in Japanese patients are characterized by the periductal localization of predominantly cluster of differentiation (CD) 4 positive T cells, IgGt4-positive plasma cells, storiform fibrosis with acinar cell atrophy frequently resulting in stenosis of the main pancreatic duct, storiform fibrosis and obliterative phlebitis [Okazaki and Chiba, 2002, 2011; Pickartz et al. 2007], which is also called lymphoplasmacytic sclerosing pancreatitis (LPSP) [Kawaguchi et al. 1991]. Recently, the International Consensus Diagnostic Criteria for AIP classified two distinct subtypes; type 1 and type 2 AIP [Chari et al. 2010]. Type 1 AIP is classified as a pancreatic manifestation of IgG4-related disease, probably a systemic disease with an autoimmune process, whereas type 2 AIP is supposed to be a specific pancreatic disease with occasional coexistence alongside ulcerative colitis [Chari et al. 2010; Shimosegawa et al. 2011]. Although pathogenesis or pathophysiology remains unclear, we will discuss the most recent advances in the concept and therapeutic guidance of AIP.
Recent advances in the concepts of autoimmune pancreatitis subtypes
Recent studies have suggested that AIP manifests as two distinct subtypes, type 1 and type 2 AIP (Table 1) [Chari et al. 2010; Shimosegawa et al. 2011; Klöppel et al. 2010]. In type 1 AIP, whose histologic description is called LPSP, the pancreatic histopathology shows the following characteristic features: (a) abundant infiltration of plasma cells (IgG4+ cells; >10/hpf, 40% > IgG4/IgG cells) and lymphocytes, (b) peculiar storiform or swirling fibrosis, and (c) perivenular infiltration with lymphocytes and plasma cells often leading to obliterative phlebitis. Clinically, type 1 AIP seems to be the pancreatic manifestation of the recently proposed IgG4-related disease [Kamisawa et al. 2006; Yamamoto et al. 2006; Masaki et al. 2009; Umehara et al. 2012], characterized by swelling of the pancreas, elevated serum IgG4 levels and extrapancreatic lesions (e.g. sclerosing cholangitis, sclerosing sialadenitis and retroperitoneal fibrosis) associated with infiltration of abundant IgG4+plasma cells. Although it is not certain that all of them can be related to AIP, extrapancreatic lesions are prevalent in the systemic organs, suggesting that type 1 AIP, but not type 2 AIP, may be a pancreatic manifestation of IgG4-related disease. Elderly male patients with type 1 AIP often have obstructive jaundice, and the pancreatic and extrapancreatic manifestations respond to steroid therapy [Chari et al. 2010; Shimosegawa et al. 2011].
Subtypes of autoimmune pancreatitis.

AIP: autoimmune pancreatitis, GEL: granulocytic epithelial lesion, LPSP: lymphoplasmacytic sclerosing pancreatitis, IDCP: idiopathic duct-centric pancreatitis, USA: United States of America, EU: European Union, NS: not significant.
Type 2 AIP [Chari et al. 2010; Shimosegawa et al. 2011] was proposed by American and European pathologists from histological examinations of the resected pancreas of patients with chronic nonalcoholic pancreatitis, and they reported another histopathological pattern named as idiopathic duct-centric pancreatitis (IDCP) or AIP with granulocytic epithelial lesion (GEL) [Notohara et al. 2003; Zamboni et al. 2004; Klöppel et al. 2010]. The most characteristic feature of type 2 AIP is GEL, often with destruction and obliteration of the pancreatic duct. Type 2 AIP has swelling of the pancreas but none, or very few, IgG4-positive plasma cells, and clinical features show a distinctly different profile associated with no serum IgG4, IgG elevation, presence of autoantibodies, or other organ involvement except for inflammatory bowel disease (approximately 30%). Patients with type 2 AIP differ from those with type 1 AIP as they have no serological markers of autoimmunity, but deposition of C3c and IgG at the basement membrane of pancreatic ducts and acini suggests immune complex-mediated destruction of ducts and acini in type 2 AIP as well as in type 1 AIP [Detlefsen et al. 2010]. Although it is still in debate as to whether type 2 AIP should be classified as one clinical entity of AIP or not, the nomenclature of the two subtypes and international diagnostic criteria were proposed at the consensus meeting of the International Association of Pancreatology held at Fukuoka in 2010 [Shimosegawa et al. 2011].
Pathophysiological conditions in autoimmune pancreatitis
IgG4 and humoral immunity
The pathogenesis and pathophysiology of AIP have been studied mainly from immunological approaches and focused for the most part on IgG4-related type 1 AIP, because few incidences of abnormal immunity have been reported in type 2 AIP. In healthy subjects, the ratios for each IgG subclass are 65% of IgG1, 25% of IgG2, 6% of IgG3, and 4% of IgG4 [Roitt, 1997]. In IgG4-related diseases, total IgG, IgG1, IgG2, IgG4 and IgE are usually increased compared with healthy subjects, while IgM, IgA, and the ratios of IgG to IgM or IgA, are decreased compared with normal or other control diseases [Hamano et al. 2001; Yamamoto et al. 2006; Masaki et al. 2009; Taguchi et al. 2009]. Although the association of IgE-mediated allergy and IgG4 antibodies is well known [Robinson et al. 2004], IgG4 characteristics are still poorly understood. Basically, IgG4 has nonacting characteristics for immune responses involved in a continuous process referred to as ‘Fab-arm exchange’ by swapping a heavy chain and attached a light chain with a heavy-light chain pair from another molecule as monovalent antibodies [van der Neut Kolfschoten et al. 2007]. Another aspect of IgG4 mimics IgG rheumatoid factor activity by interacting with IgG on a solid support [Kawa et al. 2008]. In contrast to conventional rheumatoid factor, which binds via its variable domains, the activity of IgG4 is located in its constant domains, but is inefficient in activating potentially dangerous effector systems due to its low affinity for C1q and the classical Fcγ receptors. As the patients in active stages of AIP occasionally show decreased complement (C3, C4) with elevated circulating immune complex [Hamano et al. 2001; Cornell et al. 2007], the classical pathway of complement activation through IgG1 may be involved in the development of AIP rather than mannose-binding lectin or alternative pathways through IgG4 [Muraki et al. 2006]. Moreover, IgG4 bound to other isotypes such as IgG1, 2, and 3 with an Fc–Fc interaction immune complex in patients with AIP [Kawa et al. 2008], suggests that IgG4 may contribute to the clearance of immune complexes or termination of the inflammatory process by preventing the formation of large immune complexes with blocking Fc-mediated effector functions of IgG1. Patients with type 1 AIP generally show several nonspecific antibodies, such as an antinuclear antibody, in addition to increased IgG and IgG4 [Okazaki et al. 2001, 2011]. From the view of IgG4 function, the big mystery is whether type 1 AIP is an autoimmune or an allergic disease. The occasional coexistence of other organ involvement leads us to the concept that there may be common target antigens in the involved organs such as the pancreas, salivary glands, biliary tract, lungs, renal tubules, and so on. Although disease-specific antibodies have not been identified at this moment, several disease-related antibodies such as antilactoferrin (anti-LF) [Uchida et al. 2000; Okazaki et al. 2000], anticarbonic anhydrase-II (anti-CA-II) [Uchida et al. 2000; Okazaki et al. 2000; Nishi et al. 2007; Aparisi et al. 2005], anti-CA-IV [Nishimori et al. 2005], antipancreatic secretory trypsin inhibitor (anti-PSTI) [Asada et al. 2006], antiamylase-α [Endo et al. 2009], anti-HSP-10 [Takizawa et al. 2009], and antiplasminogen-binding protein (anti-PBP) peptide autoantibodies [Frulloni et al. 2009] have been reported. Although the patients show increased serum levels of IgG4, the major subclass of these autoantibodies is not necessarily IgG4, but often IgG1 [Asada et al. 2006], CA-II [Uchida et al. 2000; Okazaki et al. 2000], CA-IV [Nishimori et al. 2005], LF [Uchida et al. 2000; Okazaki et al. 2000] and PSTI [Frulloni et al. 2009] which are distributed in the ductal cells of several exocrine organs, including the pancreas, salivary glands, biliary duct, lungs and renal tubules [Uchida et al. 2000; Okazaki et al. 2000]. Although not all peptides have been studied, immunization with CA-II or LF induced systemic lesions similar to human AIP, such as pancreatitis, sialadenitis, cholangitis and interstitial nephritis, in the mice models [Nishimori et al. 1995]. The high prevalence of the above antibodies suggests that they may be candidates for the target antigens in AIP [Ueno et al. 1995]. Molecular mimicry among microbes and target antigens may be a possible mechanism for breaking down immune tolerance. The hypothesis is based on the concept that infectious agents share one or more epitopes with self-components, or that infectious agents cause bystander activation of immune cells with autoaggressive potential [Kountouras et al. 2005; Guarneri et al. 2005]. Guarneri and colleagues showed significant homology between human CA-II and α-CA of Helicobacter pylori, a fundamental enzyme for bacterial survival and proliferation in the stomach [Kountouras et al. 2005; Guarneri et al. 2005]. Moreover, the homologous segments contain the binding motif of DRB1*0405, which confers a risk for AIP development. The PBP peptide identified in European patients with AIP shows homology with an amino acid sequence of the PBP of H. pylori and with the ubiquitin-protein ligase E3 component, n-recognin 2, an enzyme highly expressed in acinar cells of the pancreas, while European patients with AIP did not necessarily show LPSP as the typical histopathology of type 1 AIP in IgG4-related diseases [Frulloni et al. 2009]. These findings suggest that gastric H. pylori infection might trigger AIP in genetically predisposed subjects [Kountouras et al. 2005; Guarneri et al. 2005].
Th1 and Th2 immune balance
The presence of autoantibodies, the predominant infiltration of CD4+ and CD8+T-cells, and the expression of HLA-DR antigens in the pancreas [Uchida et al. 2000; Okazaki et al. 2011; Pickartz et al. 2007], suggest that an immunological mechanism may be involved in the development of AIP as well as the infiltration of plasmacytes and B cells. CD4+T cells differentiate from naïve T cells (Th0) to Th1, Th2, Th17, and regulatory T cells (Treg) [Kountouras et al. 2005]. Interleukin (IL)-12 induces Th1 cells, which produce IL-2, tumor necrosis factor-alpha (TNF-α) and interferon-gamma (IFN-γ), mediate cellular immunity, macrophage activation, cytotoxicity and help with B cell production of opsonizing and complement fixing antibodies [Okazaki et al. 2001]. IL-4 induces Th2 cells which produce IL-4, 5, 6 and 10, promoting humoral and allergic responses [Okazaki et al. 2001]. Transforming growth factor-beta (TGF-β), IL-6 IL-21 and IL-23 induce Th17 cells, which secrete IL-17, and may induce inflammation in mice [McGeachy and Cua, 2007; Oukka, 2007]. Although Th1-immune responses derived from the peripheral blood cells have been reported to be predominant over Th2 in some patients [Okazaki et al. 2000; Yamamoto et al. 2005], Th2 type immune responses are dominated in the local tissues in IgG4-related sclerosing cholangitis patients [Zen et al. 2007]. Mice models with depletion of Tregs by neonatally thymectomy (nTx) showed Th1 cells act mainly as effectors in the initial early stage [Okazaki et al. 2011]. Taken together, Th1 cytokines may be essential in the induction of AIP, while Th2 cytokines are involved in the progression of the disease process, especially the maturation and proliferation of local B cells and plasmacytes [Okazaki et al. 2011].
Regulatory T cells and innate immunity
From naïve Th0 cells, TGF-β can induce CD4+CD25+ Tregs, which have a potent inhibitory function via the transcription factor Foxp3 to CD4+ T-cell-mediated immune responses such as Th1, Th2 and Th17 [Oukka, 2007]. Foxp3 is a member of the forkhead/winged-helix family of transcriptional regulators, and functions as the master regulator in the development and function of Tregs. This suppressive function is mediated by both TGF-β and IL-10, and cell-to-cell contact via ligation of cytotoxic T lymphocyteantigen-4. Naturally occurring CD4+CD25+ Tregs (nTregs) from the thymus decreased in the peripheral blood of patients with AIP, whereas inducible memory Tregs (iTregs) (CD45RA-)-Tregs in major populations are significantly increased [Zen et al.2007]. In addition, prominent infiltration of Tregs with upregulation of IL-10 is observed in the liver of IgG4-related sclerosing cholangitis patients [Uchida et al. 2002]. These findings suggest that iTregs in the periphery and local tissues may be inhibitory immune responses against inflammation in the patients with AIP, although decreased nTregs may be pathogenetic. In AIP, increased peripheral iTregs are positively correlated with serum levels of IgG4 [Miyoshi et al. 2008]. These findings suggest that IgG4 or IgG4-immune complexes do not act as a pathogenetic factor but as an anti-inflammatory factor in IgG4-related diseases [Kawa et al. 2008].On the other hand, recent studies suggested that abnormal innate immunity may be involved in production of IgG4 by upregulating B-cell activation factor family (BAFF) [Watanabe et al. 2012, 2013]. Further studies are necessary to clarify the role of IgG4 in type 1 AIP as an IgG4-related disease. Our recent hypothesis for the pathogenesis of type 1 AIP is shown in Figure 1. The basic concept is the biphasic mechanism of ‘induction’ and ‘progression.’ An initial response to self-antigens (LF, CA-II, CA-IV, PSTI, amylase-α, PBP peptide of H. pylori, etc.) might be induced by decreased naïve Tregs followed by a Th1 type immune response with the release of proinflammatory cytokines (IFN-γ, IL-1β, IL-2, TNF-α). In progression, Th2 type immune responses to producing IgG, IgG4 and autoantibodies may be involved in pathophysiology. IgG4 and fibrosis may be regulated by increased IL-10 and TGF-β secreted from iTregs, with inducible T-cell co-stimulator molecules, respectively. The classical pathway of the complement system may be activated by the IgG1 immune complex. Recently, another mechanism of upregulation of IgG4 may be mediated by increased BAFF secreted from monocyte or basophils, which suggests that abnormal innate immunity may be involved in the development of IgG4-related disease [Watanabe et al. 2012, 2013].

Hypothesis for the pathogenesis of AIP and IgG4-related disease.
Recent therapeutic strategy for AIP
About 10% of AIP patients improve spontaneously without steroid therapy; thus, steroid therapy in AIP is recommended in patients who have symptoms such as obstructive jaundice, abdominal and back pain, and the presence of symptomatic extrapancreatic lesions. A distinct difference from type 2 AIP patients is that type 1 AIP patients rarely have the severe abdominal pain that occurs in acute pancreatitis, but persistent abdominal or back pain in type 1 AIP appears to be an indication for steroid therapy. Associated symptomatic extrapancreatic lesions, such as retroperitoneal fibrosis, interstitial pneumonia, tubulointerstitial nephritis, and hepatic or pulmonary pseudotumor are indications for steroid therapy. A facile steroid trial to diagnose AIP is permitted only after negative work-up for malignancy by histological examinations under endoscopic ultrasound-fine needle aspiration/core biopsy [Okazaki et al. 2009; Kamisawa et al. 2010].
Before steroid therapy, biliary drainage for obstructive jaundice should be performed and blood glucose levels should be controlled in patients with diabetes mellitus. For the initial oral prednisolone dose for induction of remission, 0.5–0.6 mg/kg/day is recommended. The initial dose is administered for 2–4 weeks and then gradually tapered. After 2–4 weeks at the initial dose, the dose is tapered by 5 mg every 1–2 weeks over 3–4 months, based on changes in the clinical manifestations, biochemical blood tests, and repeated imaging studies [Okazaki et al. 2009; Kamisawa et al. 2010].
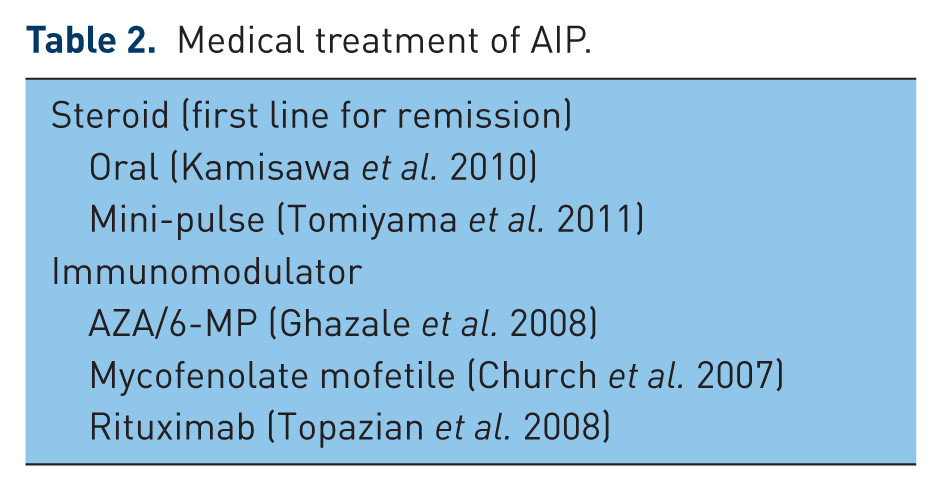
Most AIP patients (more than 90%) respond well to initial steroid therapy and achieve a remission state. After remission, the patients with type 1 AIP show a high rate of relapsing (30–50% within 6–12 months), whereas those with type 2 AIP seldom relapse. After remission in type 1 AIP, steroid maintenance therapy is still controversial, although the relapsing rate of 18–32% in maintenance therapy is relatively low (53%) in cases without maintenance therapy [Okazaki et al. 2009; Kamisawa et al. 2010]. To prevent relapse, maintenance therapy (2.5–5 mg/day) within 3 years is recommended in the Japanese consensus guidelines (Figure 2) [Okazaki et al. 2009; Kamisawa et al. 2010], but not in Western countries (Europe and the United States). Similarly, the therapeutic strategy for relapsing patients with type 1 AIP is different among local expertise. In Japan, re-administration or increased dose of steroid is recommended for the second line in relapsing AIP patients, whereas immune-modulators such as thiopurine (azathioprine/6-mercaptoethanol) [Ghazale et al. 2008; Church et al. 2007] or a molecular targeting agent (rituximab) [Topazian et al. 2008] is commonly used in Western countries (Table 2). At this moment, molecular biological mechanism of the treatments, such as steroid and immunomodulator still remains unclear.

Proposal of steroid treatment of autoimmune pancreatitis (AIP) in Japan.
Medical treatment of AIP.
Conclusion
The pathophysiological conditions in the two subtypes of AIP seem to be different, although both of them respond well to steroid treatment. After remission, the steroid maintenance therapy and therapeutic strategy for relapsing patients with type 1 AIP are different among local expertise. As Tregs seem to take important roles in progression as well as induction of the disease, further studies are necessary to clarify the pathogenesis of AIP, including genetic backgrounds, disease specific antigens, and the role of IgG4.
Footnotes
Funding
This study was partly supported by a grant-in-aid for Scientific Research from the Ministry of Culture and Science of Japan (23591017), a grant-in-aid for ‘Research for Intractable Disease Program’ from the Ministry of Health, Labor and Welfare of Japan, grants-in-aid from CREST Japan Science and Technology Agency, and MEXT-Supported Program for the Strategic Research Foundation at Private Universities.
Conflict of interest statement
The author declares that there is no conflict of interest.