
Abstract
Acute diverticulitis of the colon represents a significant burden for national health systems, in terms of direct and indirect costs. Past guidelines claimed that recurrent episodes (two or more) of diverticulitis need surgery, but revised guidelines recommend an individualized approach to patients after an attack of acute diverticulitis. For these reasons, conservative treatment has become the preferred choice after an episode of diverticulitis. Thus, significant efforts are now being focused to identify the correct therapeutic approach to prevent diverticulitis relapses. Nonabsorbable antibiotics, 5-aminosalicylic acid and probiotics are currently being investigated in this way. The effectiveness and the future perspectives of these treatments are discussed herein.
Keywords
Introduction
Diverticular disease is characterized by the presence of sac-like protrusions (diverticula) which form when colonic mucosa and submucosa herniate through defects in the muscle layer of the colon wall [Tursi and Papagrigoriadis, 2009]. Diverticular disease is commonly found in developed countries, slightly more frequently in the USA than in Europe, and is a rare condition in Africa. However, some indication is available that the prevalence of colonic diverticulosis is increasing throughout the world, probably because of changes in lifestyle [Weizman and Nguyen, 2011].
Acute diverticulitis on the colon represents a significant burden for National Health Systems so far, in terms of direct and indirect costs [Sandler et al. 2002]. Moreover, this disease seems to relapse more frequently than previously thought. In fact, a recent study found that overall disease relapse during a 10-year follow up is up to 40% [Lahat et al. 2013].
Until recently the guideline was based on the assumption that recurrent episodes (two or more) of diverticulitis will lead to complicated diverticulitis and higher mortality [Stollman and Raskin, 1999]. However, multiple episodes of diverticulitis do not seem to be associated with increased mortality or an increased risk of complicated diverticulitis. The overall mortality rate for patients with a prior history of diverticulitis was 2.5%, comparing favorably with a mortality rate of 10% for patients with a first presentation of complicated diverticulitis [Chautems et al. 2002]. In addition, 78% of patients with perforated diverticulitis had no prior history of diverticulitis [Chapman et al. 2006]. Elective sigmoid resection for diverticulitis is associated with risks of mortality and colostomy as high as 2.3% and 14.2% respectively [Hart et al. 2002; Richards and Hammitt, 2002; Salem et al. 2004]. Furthermore, the risk of recurrent diverticulitis is not eliminated after sigmoid resection, with recurrence rates between 2.6% and 10.4% [Salem et al. 2004]. In this way, the American Society of Colon and Rectal Surgeons revised their recommendations in 2006 and recommended an individualized approach to patients after an attack of acute diverticulitis [Rafferty et al. 2006].
For all these reasons, conservative treatment has become the preferred choice after an episode of diverticulitis. So, significant effort is now being made to identify the correct therapeutic approach to prevent diverticulitis relapses.
Medical strategies in preventing diverticulitis recurrence
Specifics around the diagnosis and treatment of diverticular disease of the colon are based on single papers in most cases; few high-quality randomized trials, systematic reviews or meta-analyses have been published. Despite the lack of evidence from these high-quality studies, there is some evidence to support approaches to treatment.
High-fiber diet
Once the acute episode has resolved, patients are generally advised to maintain a high-fiber diet in order to optimize their bowel movements [Stollman and Raskin, 1999]. However, the collective literature investigating the role of dietary modification in preventing diverticular disease or a recurrence of diverticulitis is inconsistent. Looking at more recent studies, the results are conflicting [Crowe et al. 2011; Peery et al. 2012; Ünlü et al. 2012], and there is no consistent support for recommending a high-fiber diet (Table 1). Despite this lack of evidence, a high-fiber diet is still commonly recommended to reduce the likelihood of diverticulitis recurrence [Murphy et al. 2007].
Use of high-fiber diet in diverticulitis.

Another interesting point is related to the classical advice to avoid consuming seeds, popcorn, and nuts, which is based on the assumption that such substances could theoretically enter, block or irritate a diverticulum and result in diverticulitis, and possibly increase the risk of perforation [Stollman et al. 1999]. There is, however, no evidence to date to support this practice [Strate et al. 2008].
Nonabsorbable antibiotics
Given the potential involvement of microbial imbalance in the pathogenesis of diverticular disease [Tursi, 2010], the literature is now proposing the use of nonabsorbable antibiotics, namely rifaximin. Cyclic treatment with rifaximin has been proposed as a therapeutic tool in preventing diverticulitis relapses and diverticulitis complications [Bianchi et al. 2011] (see Table 2).
Rifaximin in diverticulitis.
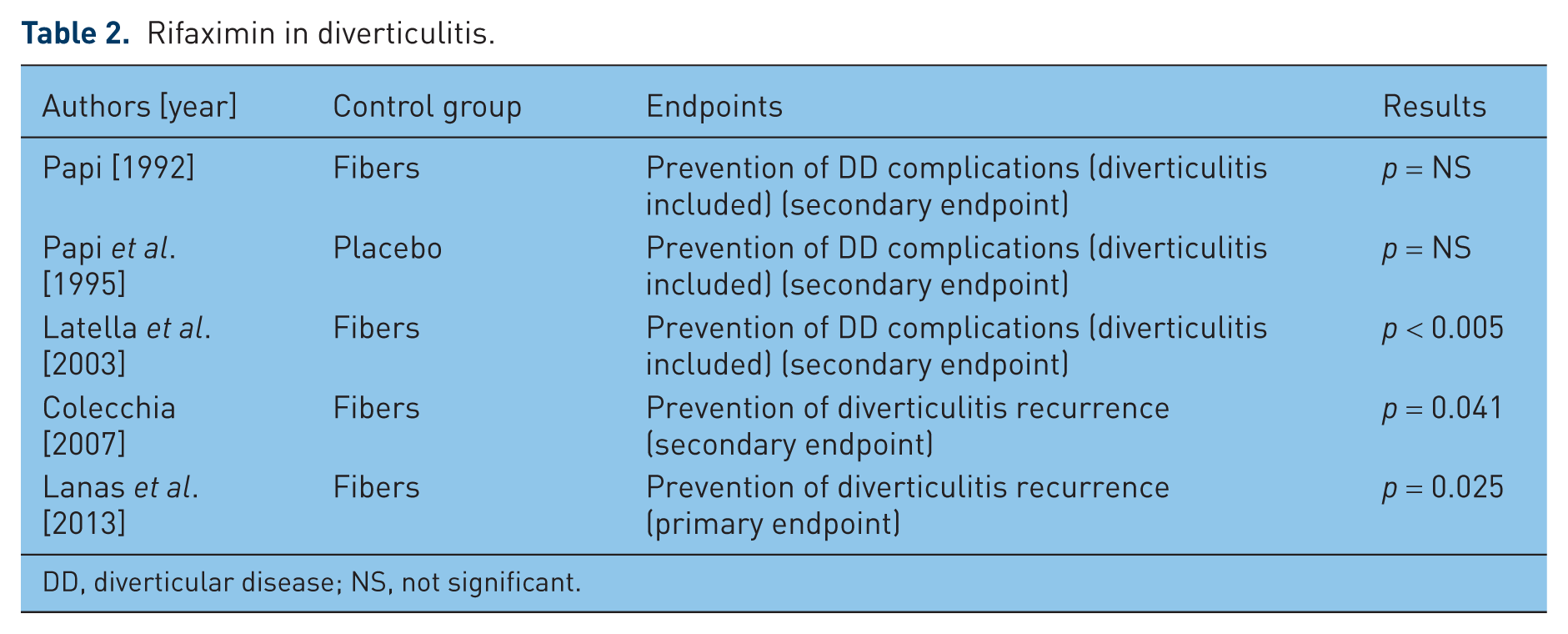
DD, diverticular disease; NS, not significant.
A recent, proof-of concept multicentre, randomized, open controlled study in patients with a recent episode of colonic diverticulitis currently in remission investigated the role of the rifaximin in preventing diverticulitis recurrence [Lanas et al. 2013]. Patients received 3.5 g of high-fiber supplementation twice a day with or without 1 week per month of rifaximin 400 mg twice a day for 12 months. Diverticulitis recurrence occurred in 10.4% of patients given rifaximin plus fiber versus 19.3% of patients receiving fiber alone. After performing an adjusted statistical analysis, the authors found a significant treatment effect (odds ratio 3.20; 95% confidence interval 1.16–8.82; p = 0.025). Safety was similar in both groups [Lanas et al. 2013]. This study is very interesting because it was the first designed for this specific endpoint using rifaximin. Unfortunately the study was interrupted since the recruitment rate was largely below the minimum anticipated and it was therefore switched from evidence gathering to proof of concept. However, the main limitation of this study was probably the open-label design, which did not add anything to data already published. This confirmed the findings of three systematic reviews that found the current data on rifaximin use in preventing diverticulitis recurrence inconclusive [Ünlü et al. 2012; Zullo et al. 2010; Maconi et al. 2011].
From a pathophysiological perspective, repeated oral administration of an antibiotic, which reaches very high concentrations within the gastrointestinal lumen, may have profound influence on the intestinal flora [Scarpignato and Pelosini, 2006]. As expected, fecal bacterial counts fall down during oral treatment with rifaximin, but the effect is short lasting. In fact, the bacterial population (mostly Escherichia coli, Bacterioides spp. and anaerobic cocci) has been shown to recover within 1–2 weeks after the end of treatment [Scarpignato and Pelosini, 2006]. The recent proof-of-concept study from Lanas and colleagues found rifaximin plus fiber better than fiber alone in preventing diverticulitis recurrence [Lanas et al. 2013]. However, this study had a lot of limitations, ranging from its open design to the failure to enroll the planned number of patients to the absence of a placebo-controlled group. In this way, this study did not add anything than was already known from other older studies [Papi et al. 1995; Latella et al. 2003] (Table 2). Of course, some attempt may be performed to improve the efficacy of rifaximin in preventing diverticulitis relapses. One possibility may be to give rifaximin twice a month. For example, two 10-day courses with a 10-day interval between the two antibiotic courses may cover the entire month, preventing the bacterial population recovery. Another possibility may be to increase rifaximin dosage up to 1200 mg/day, as recently advised in treating irritable bowel syndrome [Jolley, 2011], or to give rifaximin for a longer period, as recently advised in treating Crohn’s disease [Prantera et al. 2006; Shafran and Burgunder, 2010]. However, we do not know whether and how this profound modification of colonic microflora may alter the immune system, and all the cited hypotheses should be confirmed by well designed randomized studies.
5-Aminosalicylic acid
Another hypothesis is to try to control chronic inflammation arising from the acute episode. It is currently known that the mechanisms that underlie the development of inflammation in diverticulitis may be similar to those that drive the inflammation in inflammatory bowel disease [Lahat et al. 2013]. This hypothesis is based on five findings:
Diverticular disease shows an inflammatory infiltrate linked to the severity of the disease [Tursi et al. 2008a, 2010].
Diverticular disease shows an enhanced expression of proinflammatory cytokines as tumor necrosis factor α [Tursi et al. 2012a, 2012b; Humes et al. 2012].
Obesity is a risk factor for diverticulitis recurrence due to the proinflammatory effect of the adipokynes and chemokynes [Batra and Siegmund, 2012].
Both persisting endoscopic and histological inflammation have recently been identified as important risk factors for diverticulitis recurrence [Tursi et al. 2013].
Up to 20% of patients complain of persistent abdominal pain after surgical treatment of diverticulitis, and quality of life of those patients is significantly worse after surgery [Bargellini et al. 2013]. It has been hypothesized that persistent symptoms are linked to increased neuropeptides in mucosal biopsies, which may reflect resolved prior acute inflammation and persistent chronic inflammation [Scarpa et al. 2009].
So, all of these conditions may be considered proinflammatory situations at higher risk of diverticulitis recurrence. Using mesalazine may be an interesting therapeutic tool in this way. Mesalazine action in diverticular disease is strictly linked to control of the proinflammatory pathway (reducing inflammatory infiltrate [Tursi et al. 2008b], decreasing proinflammatory cytokine expression [Tursi et al. 2012], reducing important inflammatory and pain genes, including those involved in response to bacterial ligands [Smith et al. 2012]).
Mesalazine and its prodrug balsalazide, alone or in combination with an antibiotic or probiotics, have been found effective in preventing diverticulitis recurrence [Tursi et al. 2002, 2007]. Open-label studies also found mesalazine to be superior to rifaximin because mesalazine seems to be able to reduce endoscopic and histological inflammation after an attack of acute diverticulitis [Lombardo and Lapertosa, 1991; Tursi et al. 2013].
Recent double-blind, placebo-controlled studies found mesalazine promising in providing pain relief and reducing gastrointestinal symptoms both in symptomatic uncomplicated diverticular disease [Smith et al. 2012; Kruis et al. 2013] and after and an episode of acute diverticulitis (Gaman et al. 2011). Unfortunately, data from double-blind, placebo-controlled studies about the effectiveness of mesalazine in preventing diverticulitis recurrence are still inconclusive (Table 3).
Double-blind, placebo-controlled studies on mesalazine in diverticulitis.

NS, not significant.
The DIVA trial evaluated the efficacy of delayed-release mesalazine (Eudragit L enteric coating) in reducing gastrointestinal symptoms after an acute attack of diverticulitis (author: insert ref). During a 1-year double-blind, randomized, placebo-controlled study, 117 patients with recent computed tomography (CT) scan confirmed acute diverticulitis received placebo, mesalamine or mesalamine plus Bifidobacterium infantis 35624 for 12 weeks and were followed for 9 additional months. Efficacy was assessed using a Global Symptom Score (GSS) of 10 symptoms (ranging from abdominal pain to dysuria), and in whom abdominal pain had to be scored over 2. GSS decreased in all groups during treatment, without a statistically significant difference between mesalazine and placebo (mesalazine versus placebo, p = 0.3781; combined mesalazine/probiotic versus placebo, p = 0.6285). However, scores were consistently lower for mesalazine at all timepoints. The rate of complete response (GSS = 0) was significantly higher with mesalazine than placebo at weeks 6 and 52 (p < 0.05), and was particularly high for rectosigmoid symptoms at weeks 6, 12, 26 and 52. Recurrence of diverticulitis was low and comparable across groups. Surprisingly, a probiotic in combination with mesalazine did not provide additional efficacy [Stollman et al. 2013].
The PREVENT 1 and 2 trials investigated the role of mesalazine MMX (Cosmo S.p.A., Milan, Italy) in preventing diverticulitis recurrence, enrolling about 600 patients for each trial and treating them with 1.2, 2.4, 4.8 g once daily or placebo during a 2-year follow-up. PREVENT 2 did not find mesalazine MMX effective in preventing diverticulitis recurrence (1.2, 2.4, 4.8 g versus placebo: p = 0.368, p = 0.159, p = 0.778 respectively) [ClinicalTrials.gov identifier: NCT00545103]. But, surprisingly, the PREVENT 1 trial found mesalazine MMX 4.8 g/day superior to placebo in preventing diverticulitis relapses (p = 0.047) [ClinicalTrials.gov identifier: NCT00545740].
Finally, two other trials published as abstracts investigated mesalazine in preventing diverticulitis. The first trial assessed mesalazine Eudragit L 2.4 g/day for 10 days/month in 105 patients with a recent attack of uncomplicated diverticulitis. The primary efficacy endpoints were diverticulitis recurrence at the intention-to-treat analysis and the time of relapse (TTR), and clinical evaluations were performed using the Therapy Impact Questionnaire (TIQ) for physical condition and quality of life at admission and at 3-month intervals. Treatment tolerability and use of additional gastrointestinal drugs were also evaluated at the baseline visit and every 6 and 3 months respectively. Relative risk (RR) of diverticulitis relapse in the mesalazine versus placebo group was 1.04, 0.87, 0.69 and 0.48 at 6, 12, 18 and 24 months respectively (p = not significant). The average TTR was 219 days for the mesalazine-treated group and 370 days for the placebo group (p = not significant). Mean values of TIQ for physical condition at 24 months were significantly better in the mesalazine group than in the placebo group (p = 0.021); average additional drug consumption was also significantly lower during mesalazine than placebo treatment (p = 0.028). No significant difference in the development of side effects or changes in the laboratory parameters were recorded in the two groups [Parente et al. 2011].
The second study assessed the role of mesalazine granules 514.7 ± 30.5 mg/day versus placebo in 120 patients with colonoscopy-confirmed diverticulosis in preventing diverticular disease complications during a follow up of 40.47 ± 1.28 months. At least one flare of diverticulitis occurred in 33.82% patients given mesalazine versus 53.84% from the placebo group (p = 0.044). Time to first flare was significantly higher in the mesalazine group versus the placebo group (mesalazine 37.39 ± 1.8 months; placebo 23.09 ± 1.75 month; p = 0.001). The estimated RR of diverticulitis occurring in the placebo group was 2.47 times higher than in the mesalazine group. The number of flares during follow up was also significantly lower in the mesalazine group (mesalazine 0.9 ± 0.17; placebo 3.25 ± 0.46; p = 0.001), while the need for surgery occurred in 14.7% of patients given mesalazine and in 34.6% of patients given placebo (p = 0.02) [Gaman et al. 2011].
A possible explanation of these disappointing results is linked to the trial design. If we consider inflammation as the key factor for disease relapse, it is advisable to take the drug every day rather than only for 3 months (as in the DIVA trial) [Stolman et al. 2013] or for 10 days/months (as in the DIV/09 trial) [Parente et al. 2011]. Another confounding factor may be that different endpoints may be used in these trials. For example, the PREVENT 1 and 2 trials used objective CT scan evidence of recurrent diverticulitis as an endpoint, whilst the DIVA trial used ongoing symptoms as response to treatment. In this regard, the results of the trials cannot be compared.
Finally, another confounding factor is that results seem to vary according to the different mesalazine formulation investigated. For example, mesalazine granules seem to be more effective than mesalazine Eudragit L [Parente et al. 2011; Gaman et al. 2011; Stollman et al. 2013], whilst mesalazine MMX seems to be ineffective [ClinicalTrial.gov, 2012]. Why this different behavior? It is hypothesized that the efficacy of the mesalazine granules may be linked to the extended release of 5-aminosalicylic acid and higher mucosal levels after discharging [Brunner et al. 2003]. But this cannot explain the failure of mesalazine MMX, which should be more effective in releasing mesalazine in the left colon [Prantera et al. 2005]. More probably, the choice of mesalazine in diverticular disease should be different to that performed in ulcerative colitis. In fact, inflammation significantly affects colonic motility in diverticular disease [Bassotti and Villanacci, 2012]; in this way, mesalazine formulations releasing drugs through the entire colon may be more effective than distal-releasing systems.
Probiotics
Probiotics are living microorganisms that, if consumed in sufficient numbers, can alter the host microflora and exert specific health benefits without increasing the risk of antibiotic resistance [Isolauri et al. 2001]. These microorganisms have been investigated for the treatment of various digestive disorders and prevention of antibiotic-related gastrointestinal side effects. They commonly include the bacteria Bifidobacterium spp., Lactobacillus spp. and certain strains of E. coli, and the budding yeast Saccharomyces cerevisiae [Isolauri et al. 2001]. Probiotic microorganisms appear to have multiple modes of action, including inhibition of pathogen adherence, improving mucosal defense by enhancing tight junction integrity, decreasing bacterial translocation, stimulation of immunoglobulin A secretion in Peyer’s patches and enhancement of immune system activity by controlling the balance of pro- and anti-inflammatory cytokines [Gionchetti et al. 2002]. Moreover, probiotics may also interfere with pathogen metabolism [Gionchetti et al. 2002], and have the ability to restore balance to enteric flora, primarily by decreasing numbers of pathogenic Gram-negative bacteria [Bengmark, 1998; Sheth and Floch, 2006].
In the last few years, some open-label studies evaluated the role of probiotics in the treatment of diverticular disease (Table 4).
Probiotics in diverticulitis.

NS, not significant.
The first study was conducted more than 10 years ago. Giaccari and colleagues found that when the nonabsorbable antibiotic, rifaximin, followed by a Lactobacillus spp. probiotic was administered in patients with postdiverticulitis colonic stenosis, 88% of the 79 patients remained symptom free for a 12-month period [Giaccari et al. 1993]. No repeated episodes of diverticulitis occurred during the follow-up period, and stenoses improved or remained stable in 50% of patients [Giaccari et al. 1993]. Although this observational study lacks a placebo arm, it is significant because it was the first study to suggest that probiotics may play a role in preventing inflammatory complications of diverticular disease.
As stated above, a more recent study investigated the combination of balsalazide, a 5-aminosalicylic acid prodrug, with the high-potency, probiotic mixture VSL#3 (VSL Pharmaceuticals Inc., Towson, MD, USA). It is composed of eight different bacterial strains: L. casei, L. plantarum, L. acidophilus, L. delbrueckii subsp. bulgaricus, B. longum, B. breve, B. infantis, Streptococcus salivarius subsp. thermophilus in preventing recurrence of diverticulitis. The authors found that the combination of balsalazide and VSL#3 was better than VSL#3 alone in preventing relapse of uncomplicated diverticulitis of the colon, even if without statistical significance (73.33% versus 60%, p < 0.1) [Tursi et al. 2007].
Finally, an interesting approach in preventing diverticulitis may be the use of bacterial lysate. We know that the intestine is well known as the largest human lymphoepithelial organ and, each day, produces more antibodies, mainly secretory immunoglobulin A (IgA), than all other lymphoid tissues. IgA has different immune and anti-inflammatory properties [Mestecky et al. 1999]. In 2004 a study assessed the efficacy of an oral immunostimulant, highly purified polymicrobial lysate (containing 80 × 109 E. coli strains 01, 02, 055 and 0111, and 1 × 109 Proteus vulgaris) in the prevention of recurrent attacks of diverticulitis and in the improvement of symptoms. Eighty-three consecutive patients with recurrent symptomatic acute diverticulitis and with at least two attacks in the previous year were randomly assigned to receive an oral polybacterial lysate suspension (5 ml twice a day for 2 weeks every month) (group A) or to a no-treatment clinical follow up as controls (group B) for a 3-month follow up. Statistical differences of the sums of the scores between group A and group B were recorded after 1 month (p < 0.05) and 3 months (p < 0.01) of treatment with the oral polybacterial lysate suspension [Dughera et al. 2004].
The use of probiotics in preventing diverticulitis recurrence is therefore intriguing. However, current data are too preliminary to draw any conclusion.
Conclusion
After this literature review, an empirical therapeutic approach can be suggested in preventing diverticulitis relapses (Figure 1). However, some questions remain unanswered.

Proposed treatment algorithm after acute diverticulitis. CT, computed tomography.
Why have the studies assessing medical treatment in preventing diverticulitis recurrence given divergent results? And what research questions remain unanswered? One of the possible explanations for the disappointing results is that most of the trials assessing prevention of diverticulitis recurrence fail to enroll an adequate sampling size. The DIVA trial [Stollman et al. 2013], the DIV/09 trial [Parente et al. 2011] and the Lanas trial [Lanas et al. 2013] failed to enroll the planned number of patients. This led to disappointing results that affected the importance of the study and increased the number of unanswered questions. What factors affect the inadequate sampling size in that disease? Underevaluation of the complication of the disease? Underevaluation of the burden of the disease to patients and the particular health system? Or, more simply, an overall underevaluation of diverticulitis that is still considered a little bit more than a ‘complex irritable bowel syndrome’ by several physicians?
Other important points to investigate in the future is whether a different mesalazine formulation may influence the response to treatment, as well as whether probiotics may be advised in treatment because of their ‘bacterial control’ and immune stimulation.
Can these somewhat conflicting data currently be used to guide a patient? Despite the fact that most currently available data are inconclusive for many reasons (lack of controlled studies, preliminary data published as abstract but not as full paper, different primary and secondary endpoints, etc.), the following points have clearly been shown:
A high-fiber diet, as well as cyclic nonabsorbable antibiotics, is ineffective in preventing diverticulitis recurrence, even in the absence of any controlled study.
Data from double-blind, placebo-controlled studies are inconclusive about the effectiveness of mesalazine in preventing diverticulitis recurrence; however, it seems to be effective in controlling symptoms after an acute episode.
The use of probiotics cannot be advised due to a lack of controlled trials.
In conclusion, current studies about conservative prevention of diverticulitis relapses lead to more questions than answers. Much more investigation is required before answers to these questions are found.
Footnotes
Funding
The author declares that this research did not received a grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The author declares no conflict of interest in preparing this article.