
Abstract
Diaphragmatic hernias that are diagnosed in adulthood may be traumatic or congenital in nature. Therefore, respiratory specialists need to be aware of the presentation of patients with these conditions. In this report, we describe a case series of patients with congenital and traumatic diaphragmatic hernias and highlight a varied range of their presentations. Abnormalities were noted in the thorax on the chest radiographs, but it was unclear as to the nature of the anomaly. The findings on thoracic ultrasound conducted by a pulmonologist helped to direct appropriate investigations avoiding unnecessary interventions. Instead of pleural effusions, consolidation or collapse, thoracic computed tomography demonstrated diaphragmatic hernias which were managed either conservatively or by surgery. There is increasing evidence that pulmonary specialists should be trained in thoracic ultrasonography to identify pleural pathology as well as safely conducting pleural-based interventions.
Keywords
Introduction
The diaphragm is a major muscle of respiration and it plays a vital role in spontaneous respiration. Diaphragmatic excursion and chest wall expansion produce negative intrathoracic pressure and are responsible for the inspiratory phase of respiration. The causes of diaphragmatic dysfunction range from neuromuscular disorders and trauma to congenital anomalies [Laghi and Tobin, 2003]. Diaphragmatic herniation may be congenital or acquired and may manifest as respiratory failure [Puri and Nakazawa, 2009]. Congenital diaphragmatic hernias occur due to embryonic defects in the diaphragm while blunt and penetrating traumas are responsible for most of the acquired diaphragmatic hernias [Williams, 1982]. It has been reported that the incidence of congenital diaphragmatic hernias is 1 in 2000–3000 live births and accounts for 8% of all major congenital anomalies [Butler and Claireaux, 1962].
Here we report four cases of diaphragmatic hernias due to different aetiologies. Moreover, we evaluate the role of thoracic ultrasound in the initial assessment of some of these cases by the pulmonologist, thus highlighting its safety in diagnosing or ruling out chest radiograph changes which may be suggestive of pleural effusion, or collapse or consolidation of the lung.
Case 1
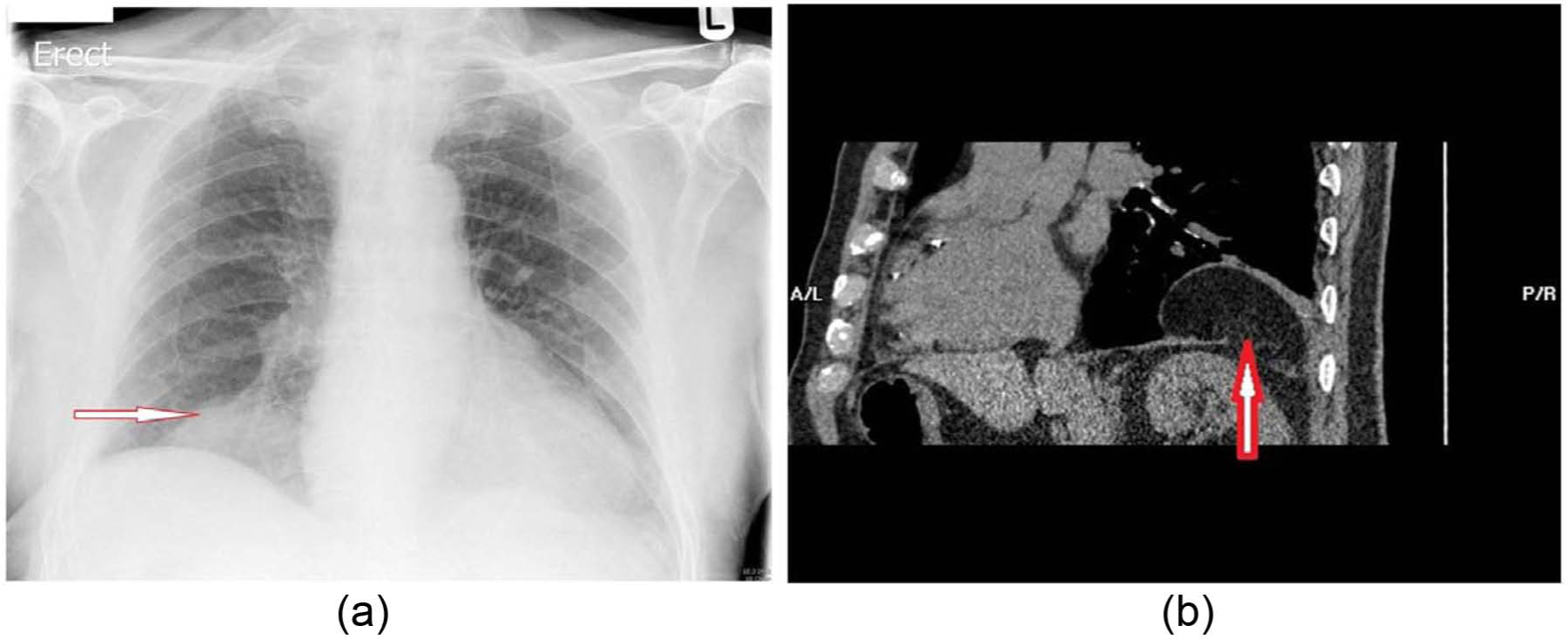
An 80-year-old man with history of orthopnoea and a non-productive cough was referred for further assessment as his chest radiograph was suggestive of a possible right lower zone consolidation or pleural effusion (Figure 1(a)). He was a tobacco smoker (30 pack years) and recently underwent a dual chamber pacemaker insertion for trifasicular heart block. Thoracic ultrasound showed no obvious fluid collection; hence a computed tomography (CT) scan of the thorax was performed revealing a diaphragmatic hernia (Figure 1(b, c)). He could not recall having any chest or abdominal trauma, making it difficult to ascertain whether the diaphragmatic hernia was congenital or acquired. The patient was offered a surgical repair, which he declined. Apart from the orthopnoea, he remains asymptomatic at 9 months of detection of the hernia.

(a) Chest radiograph mimicking right lower zone consolidation and effusion. (b) Thoracic ultrasound of right chest. The arrow depicts an abnormal finding and no evidence of pleural effusion/consolidation. (c) Computed tomography scan showing an arrow pointing at a defect in the anterior part of the diaphragm through which the colon, small bowel and mesentery have herniated.
Case 2
A 43-year-old woman presented with a 6-week history of a non-productive cough and breathlessness. Her chest radiographs performed over a period of 5 weeks were suggestive of a persistent right middle lobe consolidation. She had a past medical history of polycystic ovarian syndrome, hypertension and was an ex-smoker (10 pack years). The repeat chest radiograph remained unchanged (Figure 2(a)) and thoracic ultrasound did not reveal any pleural fluid (Figure 2(b)). A thoracic CT scan (Figure 2(c)) showed a Morgagni hernia on the right, with fat in the thoracic cavity. Subsequently, she was referred for surgical correction of the hernia.

(a) Chest radiograph mimicking right middle lobe consolidation. (b) Thoracic ultrasound of right chest. The arrow depicts an abnormal finding and no evidence of pleural effusion/consolidation. (c) Computed tomography scan showing an arrow pointing at a defect in the anterior part of the diaphragm with omentum and omental vessel extending through.
Case 3
A 59-year-old man presented with intermittent right chest wall dull aches that started 2 years previously following a fall off a ladder. He was referred to a pulmonologist as his chest radiograph revealed homogeneous opacification of the right hemithorax suggestive of a pleural effusion (Figure 3(a)). The patient had no relevant past medical history of note. He had an exercise tolerance of one mile and was a tobacco smoker (40 pack years). Clinical examination confirmed decreased air entry at the right lung base on auscultation and dullness to percussion. A bedside thoracic ultrasound showed no evidence of pleural fluid. Thoracic CT revealed a right diaphragmatic hernia containing part of his liver, spleen, pancreas, stomach, large and small bowel (Figure 3(b)). He underwent a right thoracotomy, laparotomy and diaphragmatic hernia repair and remains well at 7 months post surgery.

(a) Chest radiograph depicting a right basal homogenous abnormality suggestive of a pleural effusion. (b) Computed tomography scan showing arrows at the margins of the defect in the diaphragm. Linear transverse lines anterior and posterior to the markers are the diaphragm. The scan also demonstrates the contents of the diaphragmatic hernia, which includes the liver, small bowel and small bowel mesentery with vessels herniating through.
Case 4
An 85-year-old fit and independently mobile man was admitted to hospital after having a fall onto the right side of his chest while carrying his shopping. His past medical history comprised rate-controlled atrial fibrillation for which he received warfarin, hypertension and a hip replacement. The clinical examination revealed anterior chest wall tenderness on the right but no visible bruising. The chest radiograph (Figure 4(a)) showed a right-sided homogenous opacity and thoracic ultrasound demonstrated no evidence of fluid; this was confirmed on a thoracic CT scan to represent a Bochdalek hernia (Figure 4(b)). He was managed conservatively due to his multiple co-morbidities and being symptom free. He remains asymptomatic from the diaphragmatic hernia at 6 months.
(a) Chest radiograph showing a right basal homogenous, well circumscribed opacity. (b) Computed tomography scan showing arrows pointing to a defect in the diaphragm through which retroperitoneal fat has herniated.
Discussion
The first traumatic diaphragmatic hernia was reported by Sennertus in 1541 and the first two deaths as a result of these hernias were described by Ambrose Pare in 1578. A high level of suspicion is required to diagnose acquired diaphragmatic hernias and guide investigations appropriately [Turhan et al. 2008]. Patients can be asymptomatic in up to 53% and 44% of acquired hernias due to blunt and penetrating trauma respectively. Around 5% of people hospitalized following a trauma have a ruptured diaphragm; most presenting in their 30s with a male to female ratio of 4:1. More than two-thirds of acquired diaphragmatic hernias are left sided, one-quarter are right sided and about 1.5% are bilateral [Hanna et al. 2008]. Road traffic accidents account for a great majority of diaphragmatic hernias due to blunt injury, whereas a gunshot and stab wounds account for the majority of penetrating injuries. Other rare described causes included barotrauma during underwater diving in patients who have had previous Nissen’s fundoplication [Hayden et al. 1998] or cases of recurrence of previously repaired diaphragmatic hernia during labour [Hamoudi et al. 2004]. There are a number of possible explanations for the underlying mechanisms of rupture of the diaphragm following blunt trauma, including shearing of a stretched membrane, avulsion of the diaphragm from its point of attachment or a sudden increase in the trans-diaphragmatic pleuroperitoneal pressure gradient [Bekassy et al. 1973; Lucido and Wall, 1963; Probert and Havard, 1961]. Our case series reports how viscera could herniate through the diaphragm and lead to a whole plethora of symptoms, ranging from asymptomatic incidental findings to herniated organ-dependent symptoms.
In two of our cases diaphragmatic hernias were congenital in nature, including a Morgagni and Bochdalek’s hernia. A Morgagni hernia is caused by a defect between the costal margin of the diaphragm and the septum transversum in the anterior midline [Harrington, 1951]. Organs herniating through may include the stomach, omental fat, liver and small or large intestine. Frequently patients are asymptomatic, but can present with a variety of symptoms. Despite their rarity, they account for 2–3% of all diaphragmatic hernias [Harrington, 1951] and can be repaired laproscopically. The majority (90%) of these hernias occur on the right side [Bragg et al. 1996]. Bochdalek hernias are the most common form of congenital hernias and account for 0.17–6.0% of all diaphragmatic hernias [Mark et al. 2001]. They result due to a posterolateral defect in the diaphragm and are more common on the left side as the pleuroperitoneal canal closes late on this side [Nyhus and Condon, 1995]. Since the advent of CT scanning their incidence has increased. In children they may manifest with respiratory distress, however in adults they may manifest with a variety of symptoms with some being asymptomatic [Ahrend and Thompson, 1971]. Owing to improved techniques in antenatal ultrasound assessment a large proportion of congenital diaphragmatic hernias can nowadays be diagnosed in utero [Dillon et al. 2000]. However, some patients, as described in our case series, remain asymptomatic and the diagnosis of diaphragmatic hernia is established incidentally while investigating for other conditions.
In three of our cases there was no history of trauma, making it difficult to ascertain whether the diaphragmatic hernias were congenital or acquired. In contrast, in case 3 there was a clear history of trauma. Importantly, the appearances of the chest radiographs might have been mistaken for a pleural effusion rather than a traumatic diaphragmatic rupture or herniation, and therefore a thoracocentesis could have been undertaken. The use of thoracic ultrasound prevented this inappropriate intervention. There is good evidence to suggest that thoracic ultrasound can be used routinely by pulmonologists and its application has been shown to improve safety of pleural procedures such as thoracocentesis [Koenig et al. 2011; Weingardt et al. 1994]. Thoracic ultrasound-guided thoracocentesis, compared with that performed without it, is associated with very few complications. Thoracic ultrasound scanning not only allows for an accurate location of pleural fluid, but also facilitates assessment of its size and detection of abnormalities that may be mistaken for pleural effusions radiographically or on clinical examination. Thus the current national British Thoracic Society guidelines recommend the use of thoracic ultrasound for the investigation and management of patients with pleural disorders [Havelock et al. 2010]. For this reason, pulmonary specialists have been increasingly acquiring thoracic ultrasound skills and have started to incorporate this procedure into their routine clinical practice [Koenig et al. 2011; Weingardt et al. 1994]. The routine use of thoracic ultrasound by pulmonary specialists may result in reduction of inappropriate pleural procedures as well as contributing towards more accurate guidance of further radiological investigations [Koenig et al. 2011; Weingardt et al. 1994]. This was evident in the cases described in this report. Some of the anomalies may prove difficult to be accurately characterized using thoracic ultrasound, requiring therefore further radiological assessment such as CT scan of the thorax. Similarly, when the chest radiograph may be suggestive of pleural effusion and the thoracic ultrasound examination fails to identify the presence of any pleural fluid, our experience and current practice recommend that additional radiological assessment in the form of thoracic CT scanning is essential. As described in this case series, thoracic ultrasound findings prompted further investigations in the form of a CT scan of the thorax, which is the most appropriate method of diagnosing diaphragmatic hernias and assessment of their contents.
The characteristics of diaphragmatic hernia on chest radiograph can be mistaken for other pleural abnormalities, such as pleural effusion. Thoracic ultrasound imaging provides very good characterization of pleural disorders, such as pleural effusion, pleural thickening, empyema or malignancy [Havelock et al. 2010]. In addition, there are specific characteristic findings on thoracic ultrasound imaging that suggest the presence of diaphragmatic hernia [Eren and Ciris, 2005]. Ultrasound imaging can visualize diaphragmatic continuity, the presence of herniated organs as well as distinguishing between fatty tissue and the liver. Congenital hernias such as Morgani hernia may contain liver or omentum and the ultrasonographic appearances of the liver or fat are distinct from those of pleural effusion or thickening [Megremis et al. 2005]. Similarly, if the diaphragmatic hernia content includes the bowel, ultrasound imaging may be able to visualize peristaltic movement or fluid filled stomach following ingestion of a small amount of fluid by the patient prior to imaging. In addition, thoracic ultrasound can detect motion of the hemi-diaphragm, which may be abnormal in cases of diaphragmatic hernia. More recent studies suggest the use of M mode to evaluate the paralyzed diaphragm [Summerhill et al. 2008]. Occasionally, Bochdalek hernia may contain the kidney and when this occurs ultrasonography may reveal the absence of a kidney in the renal space within the abdomen and the presence of intrathoracic kidney [Fiaschetti et al. 2010].
Conclusion
Diaphragmatic hernias are commonly congenital, however they may be acquired due to trauma. These hernias are usually diagnosed very early in childhood, but some may manifest later in life. Ideally, treatment for diaphragmatic hernias is surgical correction; however, those diagnosed incidentally in later life who are asymptomatic may be managed conservatively. With the increased use of thoracic ultrasonography in pulmonology, not only will pleural procedures be safer, but also they will help identify other pleuro-pulmonary pathology.
Footnotes
Acknowledgements
IA, SP, UBL, GRA, JAK and JBM contributed to writing the manuscript. GRA reviewed and provided the edited images for the manuscript. JAK conducted the thoracic ultrasound scans.
Funding
JBM received honoraria for speaking and financial support to attend meetings/advisory boards from Wyeth, Chiesi, Pfizer, MSD, Boehringer Ingelheim, Teva, GSK/Allen & Hanburys, Napp, Almirall and Novartis.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this manuscript.