
Abstract
A methodological approach to quality of life (QoL) assessment in Alzheimer’s disease (AD) is challenging and few clinical trials have included it among outcomes, with conflicting results. In this review an indirect appraisal of evidence has been performed, searching the literature for the effect of drug treatments on determinants of QoL in AD. Among clinical factors associated with QoL, possible targets of drugs include cognition, which seems to be associated with QoL in early disease and can be positively affected by cholinesterase inhibitors (CIs) in this stage; functional decline, the risk of which can be decreased by CIs and memantine (MEM); behavioral and psychological symptoms, which can be reduced by MEM and atypical antipsychotics. Long-term observational studies have associated CIs and MEM treatment with a reduced institutionalization risk. According to the evidence, drug treatment of depression associated with AD should not be first choice from a QoL perspective, while treatment of pain can have beneficial effects on wellbeing indicators also in the late stages of the disease. Possible drug-related adverse events can affect QoL and should always be weighed against expected benefits from the patient’s perspective. For this reason antipsychotic treatment is often problematic in AD and should be limited to severe psychosis and aggression, using the lowest effective doses for the shortest possible period. Conversely titration of CIs is necessary to reach the most effective dosages, although dose-related risk of adverse events has to be taken into account. Finally, CIs and MEM have been shown to reduce caregiver burden in randomized trials, possibly affecting caregivers’ QoL.
Keywords
Introduction
In recent years, the study of diseases has been increasingly spreading out from objective assessment of clinical, radiological and biological features to patients’ individual experience of their own health status. Therefore, contemporary assessment of social and health interventions places an increasing emphasis on quality of life (QoL), which is considered today as one of the main outcomes of any pharmacological and non-pharmacological treatment.
Due to methodological difficulties of QoL assessment in Alzheimer’s diseases (AD), inherent to the characteristics of the illness and discussed below, only few studies have directly assessed the effects of pharmacological treatment on this outcome. Therefore the present paper, after discussing preliminary issues related to QoL assessment and determinants in AD, will be focused on available evidence regarding the effects of specific drug treatment on QoL and on its clinical correlates in AD.
Quality of life: how the concept applies to patients with Alzheimer’s disease
QoL has been defined in a broad sense as an individuals’ perception of their position in life, in the context of culture and value systems in which they live and in relation to their goals, expectations, standards and concerns [WHOQOL Group, 1995]. Specifically, the concept of health-related QoL embraces aspects of QoL which pertain specifically to a person’s health, and can be defined as perceived health status, including physical symptoms, level of functioning, psychological status, social interactions and general health perception [Wilson and Cleary, 1995].
Self-rating of health status has obvious potential limitations in dementia, due to cognitive deficit that induces amnesia, reduced insight of disease and awareness of impairments, and decreased critical judgment. Therefore, the use of specific instruments, rather than generic measure of health-related QoL, has been advocated for patients with AD [Ettema et al. 2005]. Different approaches to assess QoL in dementia have been adopted: self-rating, which is generally preferred if deemed possible according to disease severity; caregiver rating, which can be related to carer judgment per se or to the rating the carer believes the patient would give of his own status (substitute judgment) [Bosboom et al. 2012; Karlawish et al. 2001]; direct observation of behavior [Lawton et al. 1991].
Moreover, QoL assessment includes both objective indicators – describing the physical and environmental condition of the subject- and subjective factors – which include the personal experience of the individual. For example, in the model proposed by Lawton and colleagues, regarding older subjects in general [Lawton et al. 1991] and specifically adapted to dementia [Lawton, 1997], behavioral competence and living environment are assessed among objective factors, while psychological wellbeing and perceived competence are assessed in the subjective sector. When QoL has to be measured in the dementia setting, several life domains should be assessed, including affect, self esteem, general health perception, appraisal of physical functioning, social interaction and environment (enjoyment of activities, privacy etc.) [Ettema et al. 2005]. The concurrent assessment of such domains is intended to provide a global picture, which is necessary to evaluate the outcome of different interventions in dementia care.
In this conceptual framework, several scales have been proposed and validated by different authors which adopt different perspectives [Schölzel-Dorenbos et al. 2007a]. One of the main determinants of the choice among different instruments is patient cognitive level, which may obviously interfere with the ability of the patient to understand the items of the scale and to be able to rate own life condition according to them. Beyond stage of the disease the instrument may be applied in, available scales differ for the way of collection (interview or observation) and the subject who is intended to complete the rating (patient, proxy, clinician or professional carer) (Table 1). A brief summary of the peculiarities of each instrument is provided below.
Dementia-specific instruments validated for quality of life (QoL) assessment in Alzheimer’s disease (modified from Schölzel-Dorenbos et al. [2007a]).
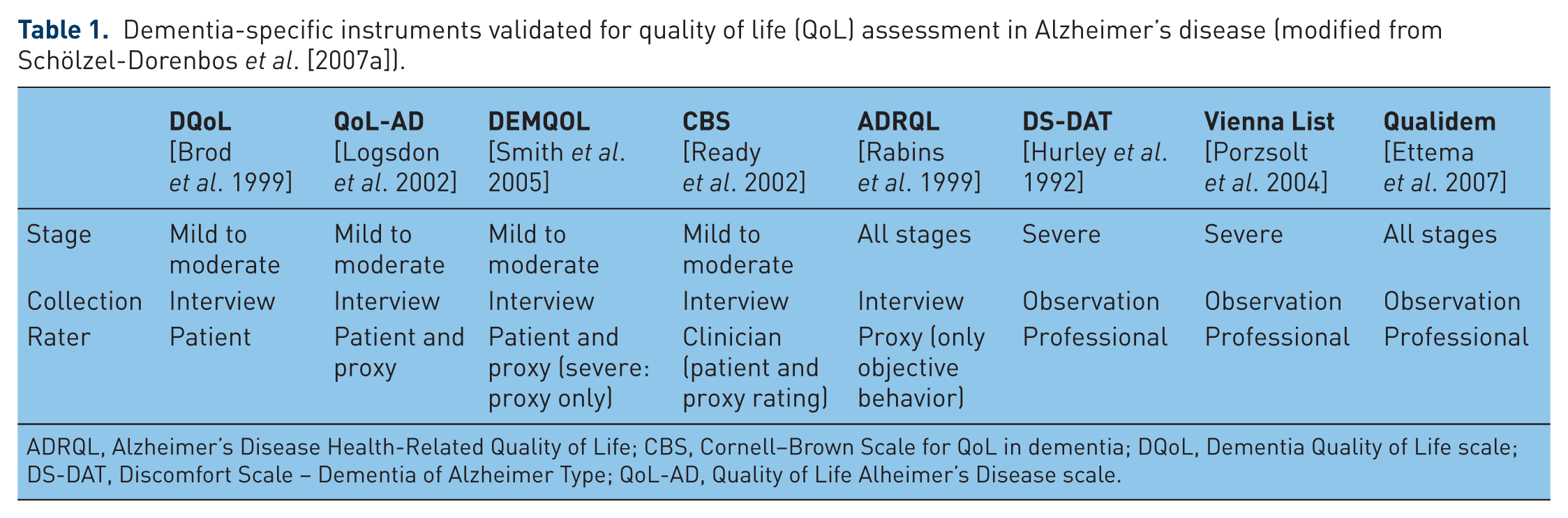
ADRQL, Alzheimer’s Disease Health-Related Quality of Life; CBS, Cornell–Brown Scale for QoL in dementia; DQoL, Dementia Quality of Life scale; DS-DAT, Discomfort Scale – Dementia of Alzheimer Type; QoL-AD, Quality of Life Alheimer’s Disease scale.
The Dementia Quality of Life scale (DQoL) is an interview including 29 items, each one rated on a 1–5 Likert scale, to be completed by patients with mild to moderate dementia [Brod et al. 1999].
The Quality of Life Alzheimer’s Disease scale (QoL-AD) is a self-report questionnaire including 13 items, each one rated on a 1–4 Likert scale, which can be completed both by patients with mild to moderate dementia and by informal caregivers, and yields a single score which weights patient’s score twice as much as the caregiver’s one. It also includes a caregiver’s QoL subscale.
DEMQOL is a self-report questionnaire administered to both patients affected by mild-to-moderate dementia (28 items) and to carers independently of disease severity (DEMQOL-Proxy, 31 items) [Smith et al. 2005].
The Cornell–Brown Scale (CBS) includes the clinical rating of 19 bipolar items on a five-point scale, after a brief interview with both patient and caregiver [Ready et al. 2002].
Alzheimer’s Disease Health-Related Quality of Life (ADRQL) is an interview including 47 items rated by proxy according only to observable behaviors, which is applicable irrespectively of disease severity [Rabins et al. 1999].
The Discomfort Scale – Dementia of Alzheimer Type (DS-DAT) encompasses nine behavioral indicators of discomfort in patients with severe dementia and language disorders, rated by professional caregivers [Hurley et al. 1992].
The Vienna list includes the rating of five factors describing the behavior of patients with severe dementia, performed by professional carers [Porzsolt et al. 2004]
Qualidem is a 49-item observation scale of patients with severe dementia in institutions, rated by professional carers, able to provide a profile of patients’ behavior on nine subscales [Ettema et al. 2007].
Different instruments allow comparison between different perspectives on QoL, as it is reported by patients and by caregivers, which show only a limited correlation. For example, in a study conducted in the Memory Clinic of Hamburg (Germany), which enrolled 100 patients affected by dementia [Alzheimer’s disease 58%, Mini Mental State Examination (MMSE) ≥ 11] and their caregivers, both were asked two questions: ‘How would you describe your quality of life/the quality of life of your relative?’ and ‘How satisfied are you with your current health status/with the current health status of your relative?’. In both cases, caregivers rated patients’ QoL significantly lower than patients themselves [Arlt et al. 2008]. Similar results were obtained in a cross-sectional study of 236 patients using a specific instrument such as QoL-AD, which has confirmed that patients have a better perception of QoL compared with caregivers, especially children [Conde-Sala et al. 2009]. A possible explanation of this difference is linked to loss of impairment awareness in patients, as it has been shown that lower awareness of memory function is associated with higher QoL ratings [Trigg et al. 2011]. Conversely, the discrepancy may be explained by a possible underestimate of patients’ QoL in caregivers’ rating, as the latter results appear to be significantly associated with assistance burden and carers’ own health status [Beer et al. 2010; Fuh and Wang, 2006; Karlawish et al. 2001]. Finally, ‘adaptation to disability’ may improve patients’ perception of own status, helping them to change standard of evaluation and relative importance of life goals, as it has been generally shown in older subjects with functional decline [Rothermund and Brandtstadter, 2003].
Clinical determinants of quality of life in dementia
The above cited multidimensional approach to QoL shows similarities with the comprehensive assessment which, especially in the geriatric setting, is typically adopted for the care of patients with dementia. Several studies have searched for potential predictors of QoL among multiple clinical parameters describing health status in dementia, including cognitive impairment, disability, behavioral and psychological symptoms (BPSDs), depression, care setting, presence of pain, physical illness.
Earlier data show that the correlation between QoL and cognitive impairment is weak, more frequent in caregivers’ than in patients’ reports, and more evident in the early stages of the disease in comparison with later stages [Banerjee et al. 2009]. Yet recent data confirm an independent association between cognitive function and proxy-rated QoL, both in institutionalized patients with moderate to severe AD [Barca et al. 2011] and in community-dwelling patients with a mild to moderate stage of the disease [Bosboom et al. 2012]. Moreover AD is a chronic disorder, and the relationship between QoL and cognitive symptoms may change as the disease progresses. This hypothesis was tested in a multicenter AD study, which assessed the relationship between Alzheimer’s Disease Assessment Scale – Cognitive Subscale (ADAS-Cog), a widely used measure of cognitive function, and patients’ reported QoL within mild and moderate dementia subgroups. While no correlation was found in the moderate stages, a direct correlation between cognitive function and QoL was observed in patients with mild dementia, supporting the importance of maintaining cognitive performance also from the patient’s perspective, at least in early phases of the disease [Hurt et al. 2010].
Moreover, a moderate correlation between QoL and disability has been observed, more significant in caregivers’ than in patients’ reports, and more evident in later stages of the disease compared with earlier stages [Banerjee et al. 2009; Barca et al. 2011; Hoe et al. 2006], although the association has also been recently reported in milder cases [Karttunen et al. 2011].
BPSDs are strongly correlated with caregivers’ reports of patients’ QoL, while this association is weak in patients’ self reports. This possibly reflects decreased insight associated with dementia, or a differential appraisal of the impact of emerging BPSDs in patients compared with carers [Banerjee et al. 2009]. This association has been reported both for family caregivers of community-dwelling patients [Hoe et al. 2007], including those with mild forms [Karttunen et al. 2011], and for nursing home residents with QoL rating performed by staff [Beer et al. 2010; Hoe et al. 2006].
The severity of depressive symptoms has shown a strong reverse association both with self-assessed and for proxy-rated QoL in all stages of dementia [Barca et al. 2011; Bosboom et al. 2012; Hoe et al. 2006; Hoe et al. 2007; Karttunen et al. 2011], although the observation is less consistent in more severe cases [Banerjee et al. 2009].
Moreover, although the data are sparse, the setting of care is a plausible determinant of QoL in dementia. In particular living at home, rather than in nursing home, is an independent predictor of higher QoL rated both by the patient and by the caregiver [Hoe et al. 2007].
Finally, physical illness is a frequently overlooked factor potentially affecting QoL in AD patients. For example in institutionalized patients pain, assessed with a validated instrument, is significantly related to self-rating and not proxy-rating of patients QoL [Beer et al. 2010].
Specific drug treatments and quality of life in Alzheimer’s disease
Randomized clinical trials of specific pharmacologic treatments for AD have proven the efficacy of cholinesterase inhibitors (CIs) and memantine (MEM) in reducing cognitive impairment, delaying functional decline, and improving clinical global rating versus placebo. However, only few trials have included QoL as a specific outcome (see the next paragraph). Owing to the scarcity and inconsistency of such data, an indirect appraisal of drug effects in this regard has been performed. Therefore, the remaining part of this section is devoted to a reasoned analysis of the evidence regarding the effect of drug treatment on possible clinical correlates of QoL, including cognition, disability, care setting, adverse events and BPSDs. In the last paragraph an alternative, goal-oriented approach to outcome assessment is introduced, as it takes into account the subjective relevance of symptoms and personal expectations regarding treatments, which seem conceptually related to QoL.
Direct assessment
Only four randomized clinical trials comparing donepezil with placebo have included a measure of QoL among their outcomes [Burns et al. 2011; Rogers et al. 1998b, 1998a; Rogers and Friedhoff, 1996] – in all cases a secondary one. The results were inconsistent as donepezil’s effect was found to be superior to placebo in one study [Rogers et al. 1998b], comparable to placebo in two other studies [Burns et al. 2011; Rogers and Friedhoff, 1996] and slightly worse than placebo in another [Rogers et al. 1998a]. Of note, none of the studies had adopted assessment instruments which are validated in patients with AD; therefore, no clear conclusion can be drawn from them [Takeda et al. 2006]. Conversely, some observational studies have reported an independent association between patient-rated QoL, measured with appropriate instruments, and treatment with antidementia agents [Bosboom et al. 2012], especially CIs [Hoe et al. 2007].
Cognition
As discussed above, cognitive impairment is a first potential determinant of QoL in AD, at least during the early phases. Meta-analyses of studies have shown a significant cognitive benefit of the CIs donepezil, rivastigmine and galantamine over placebo after 6 months in mild to moderate AD [Birks, 2006]. Similar data are available for MEM, although the effect is more evident in moderate to severe stages of the disease compared with earlier stages [McShane et al. 2006], in agreement with the approved indication of the drug.
Disability
Similarly disability – another important determinant of QoL, at least in caregivers’ reports – has been shown to decline less in subjects treated with CIs and MEM in comparison with placebo [Hansen et al. 2007]. The extent of such benefit, although significant, is difficult to quantify due to the number of different scales used for assessment. To clarify the meaning of these data, some review articles have reanalyzed the results of clinical trials using the risk of global cognitive and functional decline as a composite outcome of obvious meaning for daily life. Such data are available for donepezil, which in a meta-analysis of three randomized trials showed a reduced risk of such transition, both in mild stages of the disease and in moderate stages, with less than half of treated patients reaching the endpoint in the active drug versus placebo group [Wilkinson et al. 2009]. Similar results have been obtained in meta-analyses of three clinical trials of rivastigmine in mild to moderate AD [Raskind et al. 2000] and of six clinical trials of MEM in moderate to severe AD [Wilkinson and Andersen, 2007].
Care setting
As stated before, care of setting, in particular living at home versus in an institution, is a potential determinant of QoL in AD. Therefore, the ability of long-term drug treatment to prevent institutionalization may be considered as an outcome relevant to patient’s QoL. The only randomized clinical trial which had sufficient duration to include institutionalization risk among its outcomes was AD2000, which showed no significant difference between donepezil and placebo after 3 years in this respect [Schneider, 2004]. Yet, in a subsequent Cochrane review several study limitations were pointed out, including reduced statistical power due to low enrolment and high dropout rate, and the review concluded that the study failed to meet its objectives [Birks, 2006]. Therefore, only observational studies are available to assess the long-term effects of available drugs, with obvious methodological limitations. In these studies, use of CIs has been associated with a decreased risk of nursing home admission compared with no specific drug treatment after a mean follow-up period of 3 years [Lopez et al. 2002], data which were separately confirmed both with donepezil [Geldmacher et al. 2003] and with rivastigmine [Beusterien et al. 2004]. Moreover, in a subsequent study, with a mean follow up of 62 months, combination with CIs and MEM was associated with a reduced institutionalization risk compared with treatment with CIs only, and the latter was associated in turn with a reduced risk compared with no specific treatment [Lopez et al. 2009].
Adverse events risk versus efficacy
From a QoL perspective, symptomatic efficacy has to be balanced against risk of drug-related adverse events, especially in a chronic condition such as AD. This approach seems relevant for CIs, which have shown a greater risk of adverse events compared with placebo, especially gastrointestinal symptoms (nausea, vomiting, diarrhea) and, less frequently, syncope, fatigue, insomnia, headache and tremor [Birks, 2006]. Of note, the risk of such events is clearly dose dependent (as seems to be the case for efficacy), and this was shown, at least for donepezil and rivastigmine, in a meta-analysis of randomized clinical trials [Ritchie et al. 2004]. The clinical benefit of reaching higher doses from a QoL perspective is supported by a large 3-year, prospective, observational study of 880 patients with AD treated with CIs, in which a higher dose of CIs (donepezil >6.9 mg/day, oral rivastigmine >6 mg/day, galantamine >16 mg/day) was independently associated with a lower institutionalization risk [Wattmo et al. 2011]. The risk of gastrointestinal side effects leading to treatment withdrawal is particularly high for the oral formulation of rivastigmine, both in clinical trials [Birks et al. 2009] and in clinical practice [Mossello et al. 2004]. In this regard, the introduction of a transdermal formulation of rivastigmine has represented a relevant advantage, allowing the administration of higher, more efficacious doses with a reduction of adverse events by two-thirds in comparison with capsules [Winblad et al. 2007].
The balance between efficacy and adverse events seems to be a minor issue for MEM, which has been associated with no increased risk of adverse events in placebo-controlled studies [McShane et al. 2006].
Behavioral and psychological symptoms
Another important determinant of QoL, although limited to caregivers report, is the presence of BPSDs. In agreement with data supporting a delay of disease progression, treatment with CIs has been associated with a decreased risk of developing BPSDs requiring antipsychotic treatment, as has been shown for rivastigmine in a pharmacoepidemiological study [Suh et al. 2004] and subsequently confirmed in the subset of nursing home residents [Narayanan et al. 2006]. With regard to BPSD treatment, a meta-analysis of six randomized clinical trials of CIs, including the Neuropsychiatric Inventory (NPI) as a secondary outcome, has found a small but significant benefit compared with placebo [1.72 points, 95% confidence interval (CI) 0.87–2.57] [Trinh et al. 2003]. Yet, in the cited studies all patients had mild to moderate disease and mean baseline NPI score at baseline was 9.2–13.9, suggesting that patients with significant BPSDs were few, and therefore making clinical meaning of such results unclear. In a pooled analysis of patients with moderate to severe AD enrolled in clinical trials, showing a greater prevalence of BPSDs, aggressiveness (present in 60% of the sample) was significantly reduced in the rivastigmine arm compared with those receiving placebo [Burns et al. 2004]. In a similar subanalysis of patients with moderate to severe AD enrolled in clinical trials of donepezil, a significant effect of the drug in comparison with placebo was observed on apathy, depression and anxiety, but not on agitation/aggression items of NPI. Only a few randomized clinical trials have targeted BPSDs as a primary outcome and the results have been inconsistent and generally negative. In the largest of those studies, which enrolled 272 patients with moderate to severe AD with clinically significant agitation, no significant benefit of donepezil was observed on the Cohen Mansfield Agitation Inventory after 12 weeks in comparison with placebo. More positive data are available regarding the effect of MEM on BPSDs. A Cochrane meta-analysis has reported a mean benefit of 2.76 NPI points (95% CI 0.88–4.63) in patients with moderate to severe AD (mean basal score 13.5–20.5) [McShane et al. 2006], thus suggesting a greater benefit in patients with a high prevalence of clinically relevant BPSDs in comparison with a CIs meta-analysis [Trinh et al. 2003]. Moreover, in a pooled analysis of 593 patients with moderate to severe AD with delusions, hallucinations or agitation at the NPI, the cumulative score of the three symptoms decreased significantly in the MEM group versus the placebo group after 6 weeks and 26 weeks [Wilcock et al. 2008].
From problem-oriented to goal-oriented approaches
Although available literature has clearly demonstrated the statistical efficacy of available drug treatments on rating scales in AD, there is much debate on the clinical meaning of the observed effects [Raina et al. 2008], including the extent to which they affect patients’ QoL [Schölzel-Dorenbos et al. 2007b]. Moreover, often the clinical impression is not fully consistent with the results of rating scales.
For this reason, in addition to the traditional problem-oriented assessment of clinical response, it has been proposed to combine a goal-oriented approach, which focuses on outcomes relevant to individuals and not on standardized impairment rating scales. One of the instruments used for this purpose is the Goal Attainment Scaling (GAS), in which the clinician identifies personalized goals with the patient and caregiver before the start of therapy, with the aim of assessing the extent to which the goals are reached after treatment [Bouwens et al. 2008]. This kind of assessment has been adopted in a pilot clinical trial of galantamine for AD, in which the clinician-rated GAS, completed together with patients and caregivers, has shown an increased goal attainment in patients receiving galantamine versus placebo after 4 months of treatment, thus paralleling the results of cognitive and global assessment [Rockwood et al. 2006]. A more widespread use of this promising approach seems to be advisable to understand how much treatments adopted in patients with AD can help reaching goals which are relevant for patients’ and caregivers’ daily life.
Other drug treatments and quality of life in Alzheimer’s disease
Psychotropic medications
In the pharmacological treatment of BPSDs, atypical antipsychotics have been studied extensively. Reviews of several randomized controlled trials have concluded that risperidone, olanzapine and aripiprazole have a limited but definite efficacy in reducing aggression and psychotic symptoms [Ballard and Howard, 2006]. Yet their use is associated with a significant increase in severe adverse events, including extrapyramidal symptoms, drowsiness and falls. Moreover, in clinical trials which have included patients with dementia a small but significant increased risk of cerebrovascular events and total mortality versus placebo has been observed [Schneider et al. 2005]. For these reasons, atypical antipsychotics should only be used when symptoms are severe and distressing or when they pose a risk to the patient or others [Ballard and Howard, 2006]. Also, these drugs have to be used at the lowest effective dose for the shortest possible period, attempting to taper down and withdraw the treatment early after the control of symptoms.
In the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) study, which compared risperidone, olanzapine and quetiapine with placebo with a pragmatic design resembling clinical practice, olanzapine and risperidone resulted in an amelioration of clinical symptoms (including hostility and psychosis) at the expense of a significant increase of adverse events, with a net effect of no change in proxy-rated QoL [Schneider et al. 2006; Sultzer et al. 2008]. These data can be explained by the fact that the therapeutic effects are offset by drug-related adverse events, which make the effect of these drugs on QoL uncertain, possibly depending on individual response.
Depressive symptoms have consistently been identified as predictors of QoL in AD. However, data demonstrating the effect of antidepressants on mood in AD are still limited and inconsistent. In fact, while a previous meta-analysis of small-scale clinical trials concluded that antidepressants in AD were efficacious and safe [Thompson et al. 2007], a recent randomized clinical trial comparing sertraline, mirtazapine and placebo showed no significant difference between active comparators and placebo after 13 and 39 weeks, both in the change of depressive symptoms, which decreased in all groups over time, and in the change in health-related QoL rated with DEMQOL and DEMQOL-Proxy [Banerjee et al. 2011]. The evidence for cognitive effect of antidepressant drugs is even weaker. Observational data support a reduced cognitive decline associated with antidepressants in patients with AD treated with CIs [Mossello et al. 2008] and a pilot clinical trial has shown a beneficial effect of the association between selective serotonin reuptake inhibitors and CIs on functional status and clinical global impression [Mowla et al. 2007]. However, taking into account the increased risk of adverse events linked to antidepressant treatment and the high response rate observed with placebo, the use of antidepressants in patients with AD has little support from a QoL perspective, except in the case of severe symptoms.
Analgesics
The treatment of pain in older patients is often neglected, and this is particularly frequent in patients with dementia. In a sample of Italian older home-care patients, reporting chronic daily pain, 34% received any analgesic drug, while only 26% of subjects with dementia received the treatment, with an adjusted odds ratio of 0.80 (95% CI 0.69–0.93) [Landi et al. 2001]. However, analgesia is associated with better proxy-rated QoL, measured with ADRQL, in nursing home patients with advanced dementia [Cordner et al. 2010]. This is in agreement with the results of a randomized, double-blind, placebo-controlled, crossover trial, which has shown that the administration of paracetamol 3 g/day to patients with moderate to severe AD in nursing homes results in increased social interaction and engagement with environment versus patients who received placebo [Chibnall et al. 2005].
Caregivers’ quality of life and drug treatments
AD involves not only patients but also has a high impact on their families; thus, the issue of caregivers’ QoL should not be neglected in assessing the efficacy of treatments. Determinants of caregiver QoL include both personal factors, such as female sex, depressive symptoms, physical health, care burden, and patient factors, including disease duration, BPSDs and QoL of patients themselves [Thomas et al. 2006]. Therefore, addressing patients’ QoL is per se a way to ameliorate the impact of the disease on their caregivers.
Treatment with CIs has possible positive effects on caregivers’ QoL: in a randomized clinical trial, donepezil was shown to reduce caregiver burden in moderate to severe AD, decreasing by 52 min per day the time of care in basal and instrumental activities of daily living compared with placebo [Feldman et al. 2003]. Similar data were obtained in a randomized clinical trial of MEM, which, after adjustment for baseline between-group difference, showed a decrease of time of care of 92 min per day [Wimo et al. 2003].
Finally, in regard to BPSDs, the recent results of the CATIE study have shown that treatment with atypical antipsychotics, although not associated with an increase in patient’s QoL, might be associated with a small but significant benefit on caregivers’ burden [Mohamed et al. 2012]. These data pose a possible ethical problem in daily clinical practice, suggesting a case-by-case approach, which weighs carefully the possible harms and benefits for the patient and takes into account caregivers’ wellbeing too.
Conclusion
The definition of QoL in AD has several shortcomings due to cognitive deficits and lack of insight typically associated with the disease, which can limit assessment reliability. However, caregivers’ rating of patients’ QoL is systematically worse than patients’ self rating, and is influenced by different factors. For example, patient-rated QoL seems to correlate with cognitive performance only in milder cases, while the association of proxy-rated QoL with cognitive and functional performance seems stronger in more advanced stages. Moreover, a strong inverse association exists between BPSDs and proxy-rated, but not patient-rated QoL, while both ratings are inversely correlated with depressive symptoms.
Only a few clinical trials have directly assessed the effect of drug treatment on QoL in AD, and the results are inconsistent. Therefore, an indirect appraisal has been performed, searching the literature for the effects of drugs on clinical determinants of QoL in AD.
Randomized trials have shown a beneficial effect of CIs on cognition, which seems to be relevant for QoL in the early phases of the disease, and on risk of functional decline, while MEM has shown a decreased risk of functional decline and a positive effect on BPSDs, which have been associated with proxy-rated QoL in moderate to severe disease. Conversely atypical antipsychotics, which have been proven to be beneficial for psychosis and aggression, can negatively affect QoL due to the risk of severe adverse events. The risk of adverse events does not seem to be an issue for MEM, while for CIs the risks and benefits, which both increase with dosage, have to be assessed during drug titration. Observational studies suggest that CIs and MEM can decrease the risk of care setting. There is no strong evidence of a beneficial effect of antidepressants on QoL in AD, as recent data have shown a high response to placebo and a possible risk of drug-related adverse events for these patients. Treatment of physical illness should never be neglected from a QoL perspective, with a special focus on pain, the treatment of which seems to be associated with increased indicators of wellbeing also in the late stages of the disease. CIs and MEM have been shown to decrease caregiver stress.
A careful choice of drug treatment seems to be relevant for QoL in AD. The patient perspective should be adopted to balance expected efficacy of symptomatic treatment against the possible risk of adverse events. However, non-pharmacological treatments, including psychosocial approaches, environment modification and caregivers’ education, can greatly affect QoL as well [Olazaran et al. 2010] and have a key role in the care management of these patients.
Footnotes
Funding
The present paper is based on a lecture sponsored by Novartis, held by EM at the VII European International Congress of the International Association of Gerontology and Geriatrics.
Conflict of interest statement
EM has received lecture honoraria from Novartis, Lundbeck and Pfizer.