
Abstract
Background:
Solitary plasmacytoma (SP) is a rare plasmacytoma. Research on clinical characteristics and prognostic factors for SP is very limited.
Objective:
This study aimed to evaluate the clinical attributes and prognostic indicators for individuals afflicted with SP.
Design:
We retrospectively analyzed the clinical parameters and survival data of 49 patients diagnosed with SP from three centers between the year 2009 and 2024.
Methods:
The Kaplan-Meier curves were constructed to compare the survival outcomes. The independent risk factors were determined based on the Cox proportional hazards model.
Results:
Among the 49 patients with SP, 30 (61.2%) were classified as solitary bone plasmacytoma (SBP), while 19 (38.8%) had solitary extramedullary plasmacytoma (SEP). Anatomically, SEPs predominantly localized to the upper aerodigestive tract (47.4%), whereas SBPs exhibited a predilection for the axial spine (30.0%) and appendicular long bones (20.0%). Survival analysis revealed significantly reduced progression-free survival (PFS) in the SBP cohort compared to SEP patients (p = 0.0002), though no statistically significant difference in overall survival was observed between groups (p = 0.1012). Radiotherapy in conjunction with surgery or chemotherapy did not substantially enhance the outcome of the patients with SP. Multivariate Cox regression analysis identified SBP subtype (hazard ratio (HR) = 0.068, 95% confidence interval (CI): 0.008–0.537, p = 0.011) and elevated Ki67 expression (HR = 4.545, 95% CI: 1.005–20.542, p = 0.049) as independent prognostic factors for inferior PFS. Notably, SBP patients with Ki67 expression exceeding 35% demonstrated the poorest clinical outcomes.
Conclusion:
The prognosis of patients with SBP was poorer than that with SEP. Patients with SBP exhibiting Ki67 expression exceeding 35% had the poorest outcome.
Introduction
Solitary plasmacytoma (SP) is a single lesion composed of clonal plasma cells with or without plasma cell infiltration in the bone marrow and no other lesions outside the primary site. 1 Traditionally, there was no evidence of plasma cell proliferation in the bone marrow morphology or immunohistochemistry of patients with SP, but it is now believed that even a small amount of plasma cell proliferation in the bone marrow with a percentage of <10% is considered to be a status of SP, termed as solitary plasmacytoma with minimal marrow involvement.2,3 SP is classified as solitary bone plasmacytoma (SBP) and solitary extramedullary plasmacytoma (SEP) based on the lesion sites. SBP refers to a single osteolytic destruction infiltration of monoclonal plasma cells, while SEP is represented as soft tissue masses or organs formed by monoclonal plasma cells, respectively. SP is a rare disease constituting only 5% of all plasma cell diseases, with a male-to-female ratio of about 2:1. The median age at diagnosis of patients with SP is approximately 55–65 years old. 4 SBP accounts for 70% of all SP cases and involves any bone, especially the axial skeleton (83.1%–84.3%). 5 The main manifestations are bone pain, swelling, and fracture of the affected area. Some patients are asymptomatic in the early stage and are only visible through imaging examinations. SEP are frequently located in the head and neck region, especially in the upper respiratory tract, including the nasal cavity, oropharynx, salivary glands, and larynx. 6 Monoclonal immunoglobulins are detected in serum and/or urine in 60%–70% of patients with SBP and <25% of patients with SEP. Radiotherapy is currently the most sensitive treatment for SP. 7 Recommended radiotherapy dose is 35–50 Gy for 4–5 weeks. 8 The size of the lesion determines the efficacy of radiotherapy. The local remission rate of radiotherapy is more than 80%–90%, and the effect of radiotherapy is better for lesions <5 cm in size. 9 The role of chemotherapy and autologous hematopoietic stem cell transplantation (auto-ASCT) in the course of SP disease is controversial, and no reliable research demonstrate that chemotherapy affects the disease progression and survival of patients with SP. 10 Some studies suggest that chemotherapy is recommended for a maximal diameter ⩾5 cm. 11 For patients with SBP, indications for surgery are pathological fractures, neurological complications, and lesions at high risk of fracture, where surgical fixation of the fracture, decompression of the vertebral plate, and spinal stabilization are feasible. While surgery can help patients with SEP to remove a well-defined large mass, it should also be followed by standard radiotherapy.
Though those treatments result in a good response, patients with SP progress to multiple myeloma (MM) or additional solitary or multiple plasmacytomas inevitably. The risk factors for progression include an abnormal ratio of free light chain, larger tumor size, and persistence of M protein for more than 1 year after radiation.12–14 In our previous studies,15,16 we found that factors including age, gender, and sites were independently associated with survival of patients of SP based on the Surveillance, Epidemiology, and End Results (SEER) program. However, large and real-world data analysis focused on the entire cohort of patients with SP was very limited.
In this study, we retrospectively analyzed clinical data on 49 patients with SP from three centers. In addition, we investigated the prognostic roles of some baseline characteristics to identify risk factors of SP.
Materials and methods
Study population
Forty-nine patients from September 2009 to March 2024 diagnosed with SP from Jiangsu Province Hospital, Nanjing First Hospital, and Changzhou No. 2 People’s Hospital were enrolled in our study. Inclusion criteria: (i) A single bone lesion or a single soft tissue or bone-extravasated lesion was confirmed by the whole-body imaging examinations; (ii) the pathological examination of the lesion confirmed the presence of monoclonal plasma cells, with restricted expression of κ or λ light chains; (iii) no evidence of MM. Exclusion criteria: (i) Previous or current coexistence of MM or other malignant hematological diseases; (ii) previously received systemic anti-myeloma treatments; (iii) post-diagnosis treatment plans were unknown. Parameters, including age, gender, serum/urine immunofixation electrophoresis, lesion sites, and treatment therapies, were recorded. We categorized the nasopharyngeal lesions of SEP patients as the upper respiratory tract, the trachea and lungs as the lower respiratory tract, tonsils, palatal regions, and gingiva as the oral cavity, and other lesions, including the mesentery, thyroid, and lymph nodes. In addition, for SBP patients, we categorized the humerus, tibia, femur, etc., as long bones, while the clavicle, ilium, etc., are categorized as others.
All patients who received radiotherapy were treated with the same radiotherapy techniques. The radiotherapy techniques employ both Intensity-Modulated Radiation Therapy (IMRT) and Volumetric-Modulated Arc Therapy (VMAT), which are three-dimensional conformal intensity-modulated radiotherapy and volumetric modulated arc therapy. Mean doses of 40–50 Gy in 25 fractions are usually achievable in localized tumors using radiotherapy. A representative figure shows an SBP in a 45-year-old man with a lump in the left chest wall (Supplemental Figure 1). The clinical target volume was determined from contrast-enhanced CT images, with a 0.5-cm expansion for the planning target volume, in axial, coronal, and sagittal perspectives. And doses to the heart and lungs were substantially reduced. And chemotherapy regimens include CTD (Cyclophosphamide + Thalidomide + Dexamethasone), VRD (Bortezomib + Lenalidomide + Dexamethasone), VAD (Bortezomib + Adriamycin + Dexamethasone), and VDT-PACE (Bortezomib + Thalidomide Dexamethasone-Platinum + Adriamycin + Cyclophosphamide + Etoposide). The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental Material).
Survival data
Overall survival (OS) refers to the duration from the initial diagnosis until the death of the patients or their last follow-up. Progression-free survival (PFS) denotes the period from the initial diagnosis until a relapse of SP at its original site, the appearance of new lesions, or when the disease progresses to active MM.
Statistical analyses
Data analysis was conducted using SPSS version 23.0 (IBM Corporation) and GraphPad Prism version 10.0 software (GraphPad Software, LLC). Survival analysis employed the Kaplan-Meier method, with log-rank tests used to compare inter-group differences. χ2 test was utilized to compare clinical characteristics of patients with SBP to those with SEP. Multivariate analysis was performed to analyze potential prognostic factors, where p values less than 0.05 were considered statistically significant.
Results
The sites of SP
A total of 49 patients with SP were included in our study, of which 30 (61.2%) patients were SBP, and 19 (38.8%) patients were SEP. The most common sites of SEP lesions were the upper respiratory tracts, approximately 50%, including the nasal, pharyngeal, and larynx. Only two patients were revolved in the lower respiratory tract (trachea and lung). SBP mainly occurred in the axial skeleton, such as the spine (30.0%), long bones (20.0%), and ribs (16.7%). Other presentations covered the sternum, pelvis, scapula, and ilium. The details of the anatomic locations of SP were summarized in Table 1.
Anatomic locations of SP.

SBP, solitary bone plasmacytoma; SEP, solitary extramedullary plasmacytoma; SP, solitary plasmacytoma.
Clinical characteristics
The clinical characteristics of 49 patients with SP are presented in Table 2. The median age at diagnosis of patients with SP was 57 years (range 34–79), indicating a younger median age compared to patients with MM. The distribution showed a slightly higher prevalence in those under 60 years, with males accounting for approximately 62.5% of the cases, reflecting a male-dominated patient population. However, the difference in positive M protein in blood or urine, bone marrow plasmacytoma infiltration, and a longer diameter of the affected lesion between SEP and SBP was not significant due to the cases was limited. The biopsy immunohistochemical results indicated that a majority of plasmacytoma (69.6%) exhibit L light chain-restricted expression. Of these 49 patients, the majority of patients received radiation therapy alone (35.4%) or radiotherapy plus surgery (39.6%).
Patients characteristics.
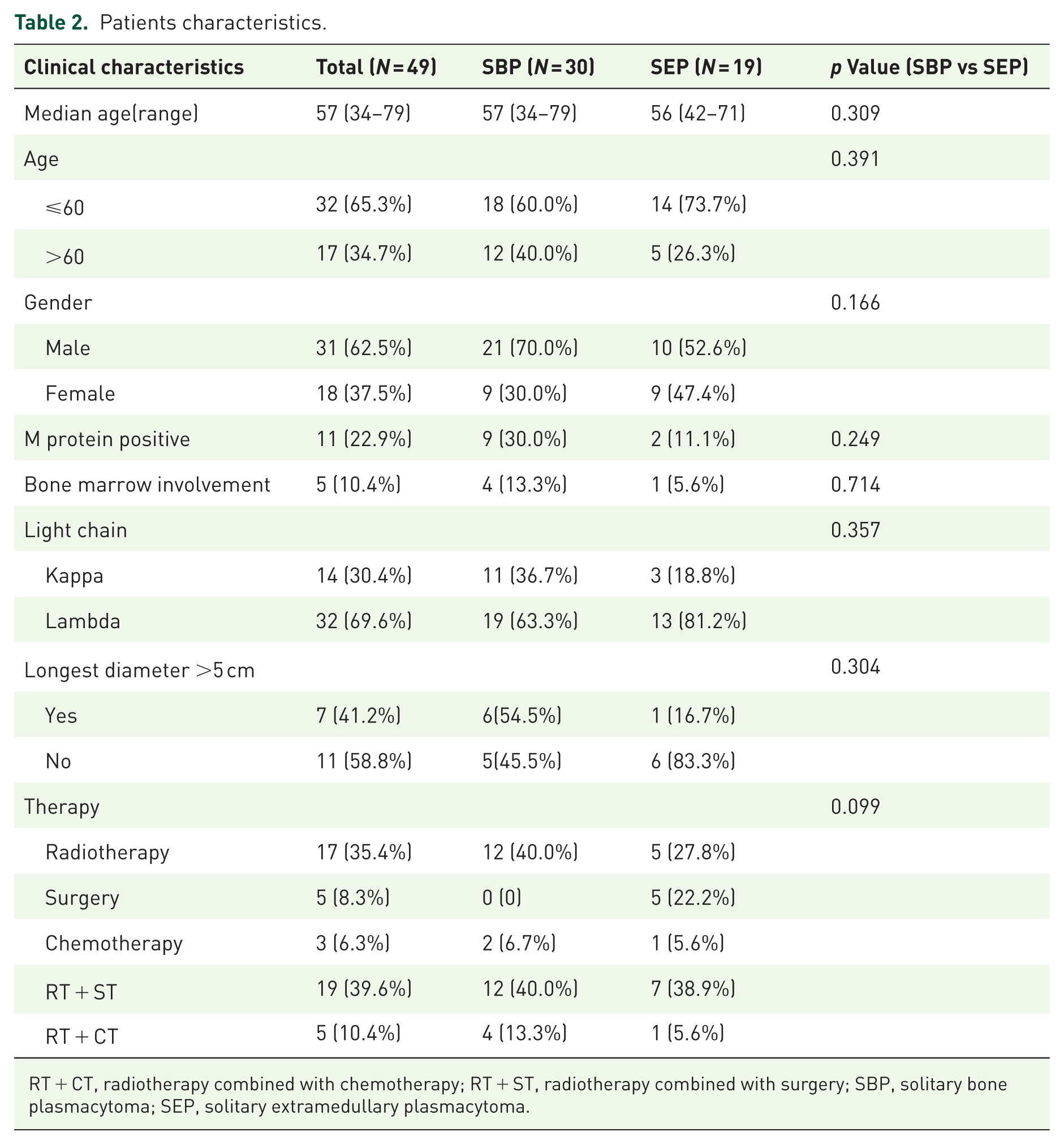
RT + CT, radiotherapy combined with chemotherapy; RT + ST, radiotherapy combined with surgery; SBP, solitary bone plasmacytoma; SEP, solitary extramedullary plasmacytoma.
Survival of patients with SBP and SEP
Following a median follow-up period of 70 months (with a range of 1–173 months), it was noticed that 45 patients (91.8%) remained alive, 4 patients (8.2%) had passed away, of which 3 patients died of MM progression and 1 patient died of an unknown reason. For the overall patients with SP, the 5- and 10-year PFS for the entire series of patients was 60% and 51% (Figure 1(a)), while the 5- and 10-year OS were 92% and 87%, respectively (Figure 1(b)). Of the 19 SEP patients, only one case relapsed, and it was an in situ recurrence. None of the SEP patients progressed to MM. Among the 30 SBP patients, 2 cases experienced local progression, and 15 cases progressed to MM. Compared to SEP, the PFS of SBP patients was poorer (Figure 1(c), p = 0.0002) with an increased rate of MM progression (SBP: 50% vs SEP: 0). The 5-year MM progression rate of SBP was 44.8%. In terms of OS, the 5- and 10-year OS for the SBP group were 88% and 79%, respectively, while the 5- and 10-year OS for the SEP group were both 100%, with no statistically significant difference between the two groups (Figure 1(d), p = 0.1012).
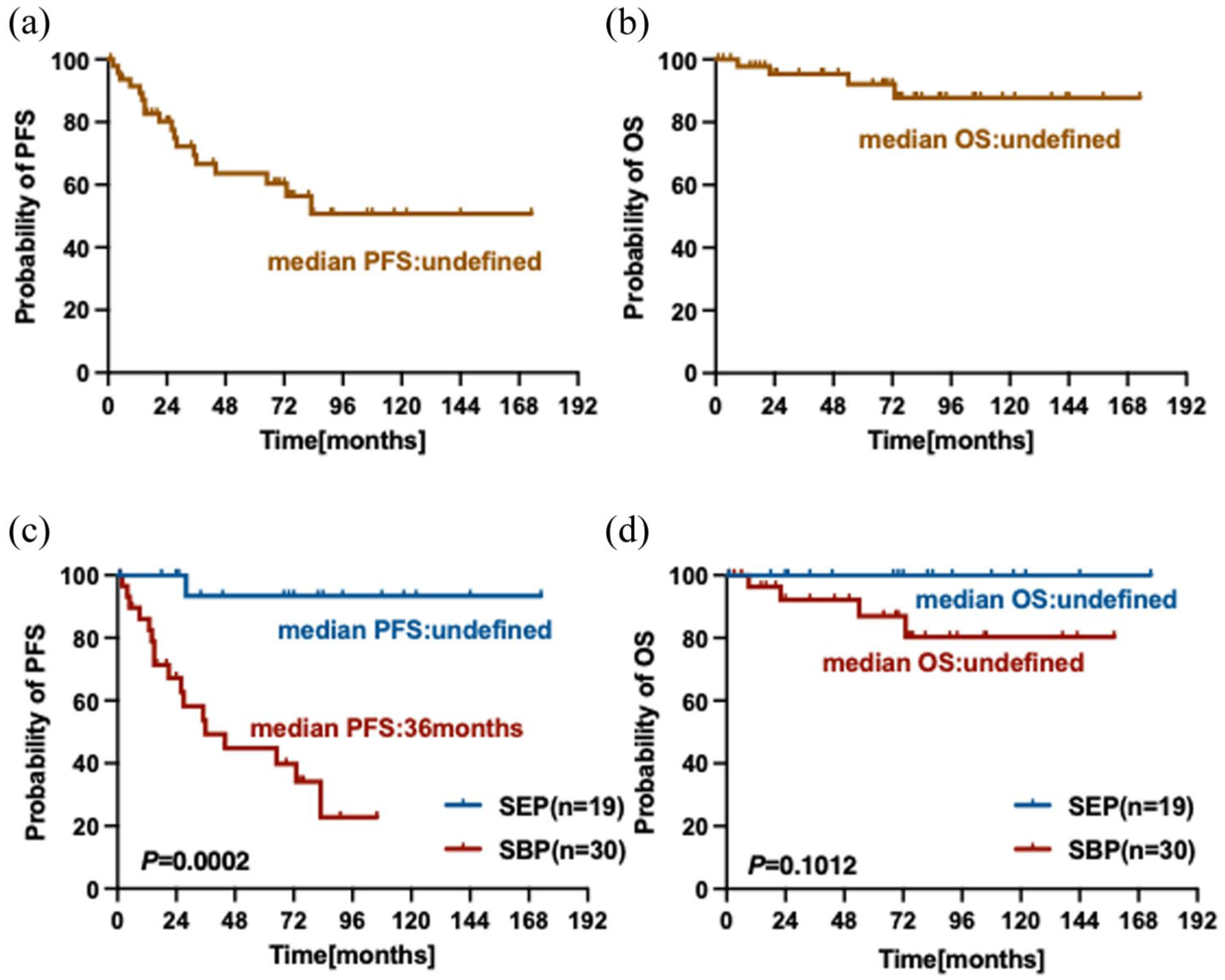
The PFS and OS of patients with SP. (a) The PFS of the 49 patients with SP; (b) The OS of the 49 patients with SP; (c) The PFS of the patients with SBP and SEP. (d) The OS of the patients with SBP and SEP.
Type of treatment administered for survival of patients with SP
All 49 patients with SP were treated with surgery, radiotherapy, or chemotherapy, among which 24 patients received two types of treatment, radiotherapy combined with surgery (RT + ST, 39.6%) or chemotherapy (RT + CT, 10.4%), while 17 patients received radiotherapy alone (R alone, 35.4%). Notably, SP patients treated with combination therapy did not have a significant benefit in disease progression compared to patients treated with radiotherapy alone, which means that radiotherapy is still an important means of SP treatment (Figure 2(a) and (b)).

The effects of type of treatment of patients with SP. (a) The PFS of the patients with SP subjected to different types of treatments; (b) The OS of the patients with SP subjected to different types of treatments.
Ki67 levels for survival of patients with SP
The cut-off of Ki67 level was established at 35% derived from ROC curve statistics. The findings revealed that individuals exhibiting higher Ki67 levels experienced shorter survival compared to those with lower Ki67 expression (PFS: not reached vs 21.0 m, p = 0.0007; OS: not reached vs 73.0 m, p < 0.0001; Figure 3(a) and (b)).
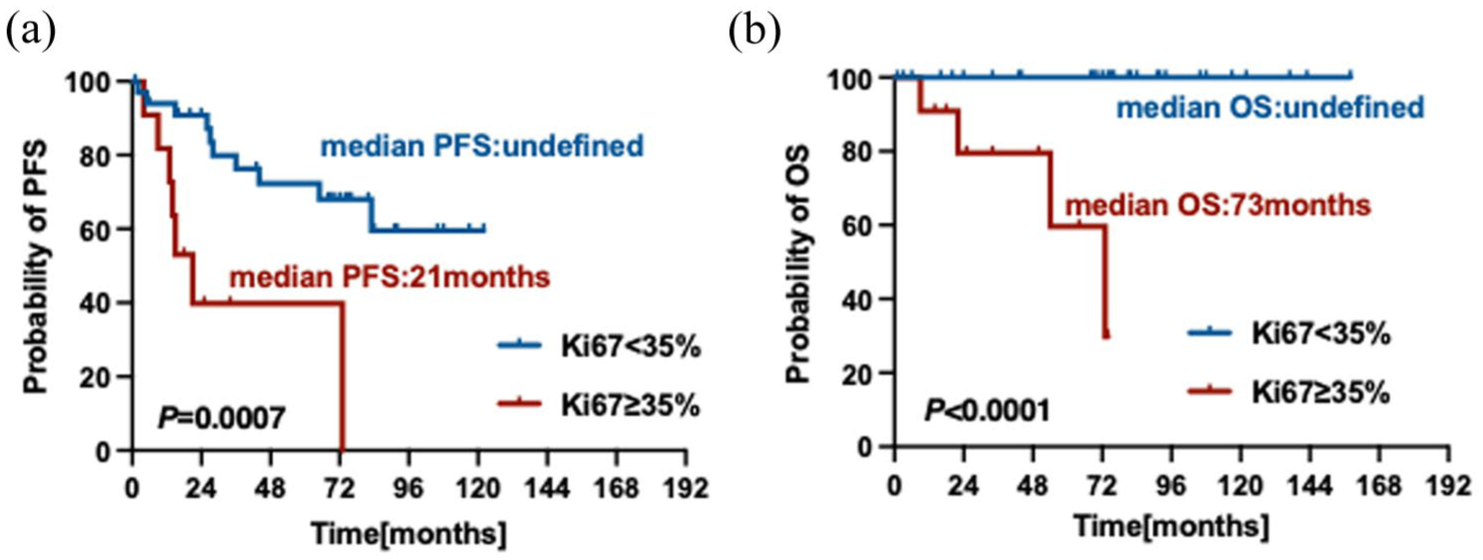
The impact of tumor burden on survival of patients with SP. (a) The prognostic effects of Ki67 expression on PFS of patients with SP; (b) The prognostic effects of Ki67 expression on OS of patients with SP.
Univariate analysis and multivariable analysis of prognostic factors in predicting PFS for patients with SP
We further incorporated covariates involving Ki67 expression, M protein, age, therapy, and SBP or SEP in a univariate analysis and a multivariate analysis. Our results revealed that SBP (p = 0.011) and the Ki67 expression (p = 0.049) were substantial independent predictive variables for PFS in patients with SP (Table 3).
Univariate analysis and multivariable analysis of prognostic factors for PFS for patients with SP.
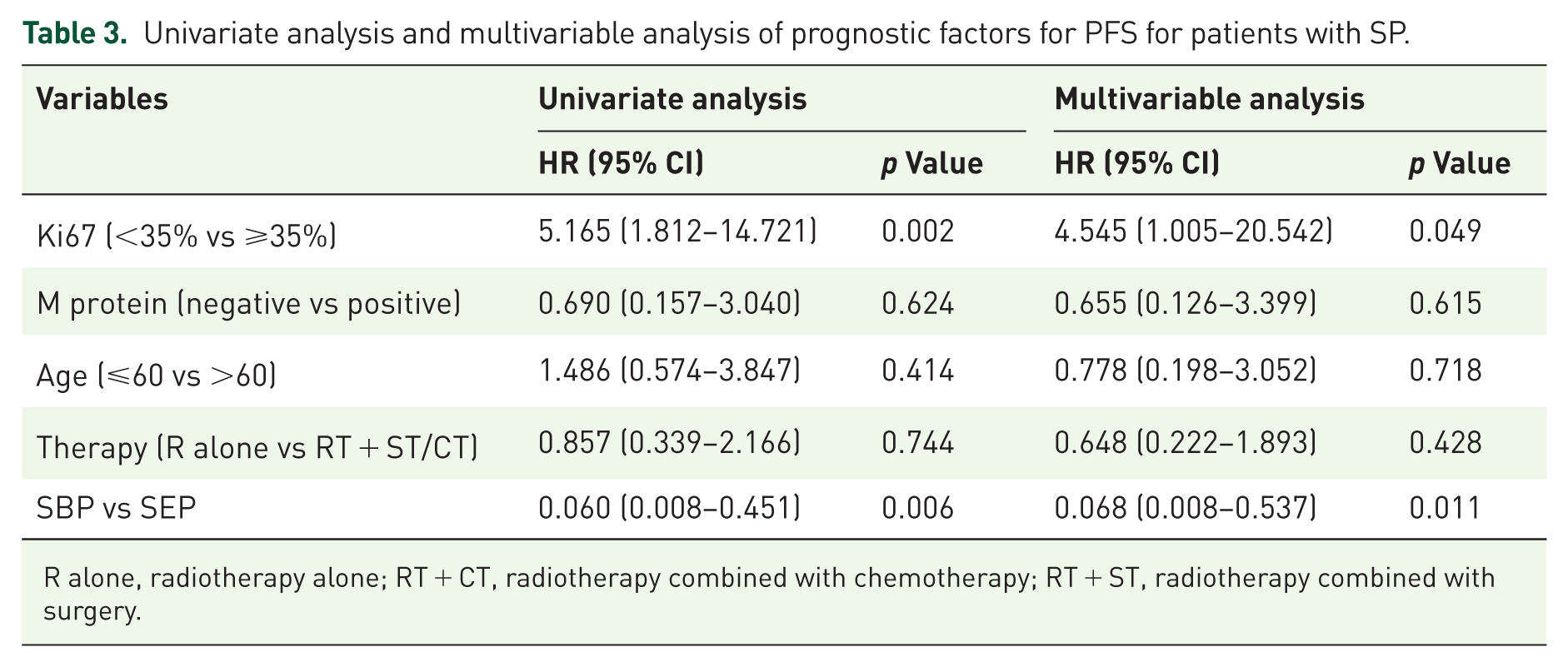
R alone, radiotherapy alone; RT + CT, radiotherapy combined with chemotherapy; RT + ST, radiotherapy combined with surgery.
Discussion
A single mass with minimal or no bone marrow infiltration defines SP. In this study, we analyzed the baseline characteristics and survival of patients with SP. The incidence at diagnosis of SBP and SEP was 61.2% and 38.8%. Our findings indicated that the patients with SBP experienced a worse prognosis and a higher rate of disease progression as compared to SEP. Combination with chemotherapy and surgery does not enable patients with SP to benefit from disease progression, and radiotherapy remains the cornerstone of treatment for SP patients. The prognosis of patients with plasma cell Ki67 expression in plasmacytoma, exceeding 35% is poor, increasing the rate of disease progression.
The subclones in SP exhibit limited capacity for distant invasion, yet high-risk clones diffuse at an early stage, leading to systemic MM. Consequently, the outcome of patients with SP is favorable than those with MM. In our study, the 5- and 10-year OS of patients with SP are 92% and 87%, respectively. Comparable results have been described in previous studies. 17 In contrast to the MM-related extramedullary disease, the risk of MM progression was shown to be higher in SBP (35%) compared with SEP (7%). 18 This could be attributed, at least in part, to variations in disease biology of MM, where extramedullary disease is signified by the presence of multiple lesions and a higher degree of bone marrow infiltration. Since the high risk of MM progression and local/distant relapse, it is recommended to carry out a yearly follow-up using the same imaging method as the initial diagnosis.
There were no appreciable variations in disease progression among the different treatment plans, with the exception of a tendency in favor of radiation therapy. According to some experts, it is recommended to administer a dose of 40–50 Gy for minor lesions and more than 50 Gy for larger lesions that are greater than 5 cm in size.19,20 Nevertheless, a multicenter investigation failed to yield any proof about the efficacy of different radiotherapy doses. 21 Radiotherapy is still considered to be the most sensitive treatment method for the treatment of SP, and the International Lymphoma Radiation Oncology Group has recently released guidelines about this matter. 8 Currently, the medical value of chemotherapy is still a subject of debate. Ascione et al. proposed that adjuvant chemotherapy could be advantageous, especially for SBP patients who remained suffering from disease undergoing radiotherapy. 22 In our series, a total of three patients underwent chemotherapy alone, while five patients received a combination of chemotherapy and radiotherapy. Given the limited size of the study cohort and diversified treatment regimens, no significant advantage of chemotherapy was observed. Approximately half of the SP patients received surgery with/without further radiotherapy. Among them, eight patients have disease progression, who were all SBP patients. We hypothesize that performing eradicative surgery is more challenging due to SBP is situated close to the bone marrow. We further compared the outcome of the patients receiving radiotherapy alone or in combination with surgery/chemotherapy, and not yet discernible benefits of combination therapy were found, suggesting that local radiotherapy remains the milestone of the treatment of SP.
To date, there have been minimal substantial analyses conducted on SP, particularly for SEP. As a result, it proves difficult to identify consistent risk parameters. Previous studies have shown that SBP or SEP, bone marrow infiltration, abnormal ratio of free light chains, persistent M protein positivity, and lesion size were risk factors for the outcome of patients with SP.13,14,23 The rate of MM progression in SPB with minimal bone marrow involvement exceeds 20% in 3 years. Conversely, only 10% of SPB with no bone marrow involvement will progress to MM within a 3-year period. Fouquet et al. found that abnormal serum-free light chain values independently shortened progression time to MM. 14 A Mayo Clinic cohort evaluated 116 patients with SBP and found that only 13% of patients with normal light chains and serum M protein less than 0.5 g/dL would progress to MM. 24 Yet, published studies have not consistently identified predictors of SP recurrence or PFS. Due to the large time span and small sample size of this study, comprehensive data concerning M proteins, free light chain ratios, and bone marrow plasma cell infiltration were restricted.
The histological assessment of biopsies is a prerequisite for the accurate identification of SP. Tumor-related factors, including MVD (micro-vessel density), VEGF (vascular endothelial growth factor), and HIF-2a (hypoxia inducible factor), were detected in SBP and SEP biopsies. 25 However, immunohistochemical staining revealed no statistically significant distinction between SBP and SEP. Whereas Rajkumar et al. suggested that an elevated MVD level is associated with the rate of MM progression. 26 In retrospective research from 12 Greek Myeloma Centers, it was found that CD56 expression was more common in patients with SBP, which was hypothesized that plasma cells in SBP need adhesion molecules to ensure survival. 27 In addition, Li et al. regarded CD38 as a promising immunohistochemical marker for predicting the prognosis of SP. 28 Accordingly, published data on this issue exhibit diversity. In our study, the Ki67 expression in biopsies from 47 individuals was available. The Ki67 criterion was established at 35% applying ROC curve statistics. Our multivariate analysis firstly reported that Ki67 expression in biopsies of more than 35% was an independent risk factor of SP progression. Despite the indicators mentioned above, Ki67, a commonly used pathological marker, can be widely applied in the prognostic evaluation of SP.
Unlike the spatial heterogeneity of tumor cells due to multiple extramedullary lesions, the cytogenetics of SP tissue from a single lesion are consistent. High-risk cytogenetic abnormalities are significantly predictive of the prognosis of SP patients. 17p deletion and 1q gain were found to be the most common cytogenetic abnormalities leading to MM progression in SBP patients. 29 However, unfortunately, fluorescence in situ hybridization (FISH) analysis of plasmacytoma tissues is not routinely tested at our center, so this part of the conclusion is still missing. The incidence of solitary plasma cell tumors is indeed low; hence, we did not apply power analysis for sample size calculation in this study, which may be one of the limitations of this study.
Conclusion
In our research, we verified that patients diagnosed with SBP exhibited a higher prevalence than those exhibiting SEP. The incorporation of surgical intervention or chemotherapy into radiotherapy did not significantly enhance the prognosis for patients suffering from SP. The presence of SBP and increased Ki67 expression were independent predictors of shorter PFS for patients with SP.
Supplemental Material
sj-docx-1-tah-10.1177_20406207251379690 – Supplemental material for Clinical characteristics and prognostic factors of patients with solitary plasmacytoma: a multicenter retrospective study
Supplemental material, sj-docx-1-tah-10.1177_20406207251379690 for Clinical characteristics and prognostic factors of patients with solitary plasmacytoma: a multicenter retrospective study by Xuxing Shen, Wenmin Han, Lina Zhang, Yuanyuan Jin, Xuzhang Lu, Xuezhong Zhang and Lijuan Chen in Therapeutic Advances in Hematology
Supplemental Material
sj-docx-2-tah-10.1177_20406207251379690 – Supplemental material for Clinical characteristics and prognostic factors of patients with solitary plasmacytoma: a multicenter retrospective study
Supplemental material, sj-docx-2-tah-10.1177_20406207251379690 for Clinical characteristics and prognostic factors of patients with solitary plasmacytoma: a multicenter retrospective study by Xuxing Shen, Wenmin Han, Lina Zhang, Yuanyuan Jin, Xuzhang Lu, Xuezhong Zhang and Lijuan Chen in Therapeutic Advances in Hematology
Footnotes
Acknowledgements
We are grateful to all colleagues at the Jiangsu Province Hospital, Affiliated Changzhou Second Hospital of Nanjing Medical University, and Nanjing First Hospital for their collaboration in collecting data.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.