
Abstract
Over the last 20 years, breakthroughs in accessible therapies for the treatment of multiple myeloma (MM) have been made. Nevertheless, patients with MM resistant to immunomodulatory drugs, proteasome inhibitors, and anti-CD38 monoclonal antibodies have a very poor outcome. Therefore, it is necessary to explore new drugs for the treatment of MM. This review summarizes the mechanism of action of selinexor, relevant primary clinical trials, and recent developments in both patients with relapsed/refractory myeloma and patients with newly diagnosed myeloma. Selinexor may be useful for the treatment of refractory MM.
Plain language summary
Multiple myeloma (MM) is a plasma-cell neoplasm that presents with a variety of clinical manifestations, including bone destruction, anemia, renal dysfunction, and hypercalcemia, which pose a serious threat to people’s health. Over the past 20 years, the survival of MM patients has significantly improved thanks to the development of several new treatments. However, the disease remains incurable, and almost all patients eventually develop a disease that is ineffective against available treatments. Therefore, an important area of research is the discovery of drugs with novel mechanisms of action to overcome the resistance mechanisms of current drugs. Selinexor is an oral XPO1 inhibitor that exerts anti-tumor activity through a novel mechanism. Here, we review the current clinical trials evaluating its role in the treatment of multiple myeloma and have a discussion of its mechanism, adverse events, challenges, and limitations. Selinexor is a promising drug. It may be a good addition to the treatment of relapsed and refractory multiple myeloma, but more research is needed to unlock its further potential.
Introduction
Multiple myeloma (MM) is a hematological malignancy that is characterized by plasma cell infiltration and can result in bone destruction and bone marrow failure. Endless new agents have emerged in recent years, for example, proteasome inhibitors (PIs) such as bortezomib, carfilzomib, and ixazomib; immunomodulatory drugs (IMiDs) such as thalidomide, lenalidomide, and pomalidomide; and CD38-targeted monoclonal antibodies (MoAbs). Continuous advances in treatment strategies have significantly improved survival in patients with MM.1–4 However, MM is still an incurable malignancy. The overwhelming majority of patients relapse with more aggressive disease owing to the gain of further genetic alterations that may cause resistance to current salvage therapies.5,6 The median overall survival (mOS) of ‘penta-refractory’ patients (refractory to anti-CD38 MoAbs, two PIs, and two IMiDs) is 5.6 months. 7
XPO1, also called chromosome region maintenance 1 (CRM1) or exportin-1, is a pivotal eukaryotic nuclear export protein that carries an extensive array of proteins and certain RNA species from the nucleus to the cytoplasm.8–10 Increased XPO1 expression has been observed in a variety of malignancies, prompting increased research on XPO1 molecular inhibitors. Selinexor is an oral, reversible, potent, selective XPO1 inhibitor that has shown promising activity against myeloma in preclinical experiments.11,12 The US Food and Drug Administration (FDA) approved the use of selinexor in conjunction with dexamethasone for the treatment of adult patients with relapsed or refractory MM (RRMM) that have been treated with at least four prior therapies and are refractory to at least two PIs, two IMiDs, and anti-CD38 MoAbs in July 2019.
Overview of selinexor
Mechanism of action
The nucleus and cytoplasm are separated in eukaryotic cells to avoid interference with chromatin inside the nucleus of the cell. 13 The selective permeability of the nuclear envelope allows smaller molecules (proteins, RNAs, and ribonucleoproteins) to migrate across compartments. However, macromolecules and complexes larger than 40 kDa cannot pass freely through the nuclear envelope, necessitating the transport of effector molecules.14–16 With the help of the specialized carrier protein XPO1, proteins larger than 40 kDa can be exported from the nucleus to the cytoplasm.17–19 XPO1 belongs to the importin-β superfamily of karyopherins20,21 and is responsible for the nuclear export of at least 221 nuclear export signal-containing proteins into the cytoplasm. 22 The XPO1 protein is increased in a multitude of malignancies,23–33 causing tumor suppressor proteins (TSPs) to be exported to the cytoplasm and unregulated tumor cell proliferation. Increased levels of XPO1 have also been demonstrated in MM patients. In MM, high XPO1 expression correlates with increased bone lysis and inferior outcomes, as well as drug resistance. 11 XPO1 has been identified as a crucial target in MM cell lines by genome-wide short interfering RNA interference screens.12,34 Targeted inhibition of XPO1 induced apoptosis of MM cells both in vivo and in vitro.11,12,35,36 Given these results, XPO1 inhibitors were developed to block XPO1 function.
Selinexor is an oral inhibitor of nuclear export (SINE) that reversibly and selectively binds to cysteine 528 in the cargo binding pocket of XPO1, inactivating its nuclear export function.37–40 The antineoplastic activity of selinexor appears to be mediated through multiple mechanisms: (1) Selinexor inhibits TSP nuclear export and results in their functional inactivation, resulting in proapoptotic action against tumor cells.41–44 (2) Selinexor inhibits oncoprotein mRNA nuclear export. EIF4E, as an XPO1 cargo, can carry some oncoprotein mRNAs (e.g. cyclin D1, B-cell lymphoma 2, c-myc) for translation in the cytoplasm. Selinexor blocks eIF4E–mRNA complex transport, retaining oncoprotein mRNA in the cell nucleus, thereby reducing the level of oncoprotein synthesis in the cytoplasm.45–49 (3) Selinexor has synergistic effects with dexamethasone in a glucocorticoid receptor (GR)-dependent manner. Selinexor markedly enhances the transcription and translation of GR in the presence of dexamethasone, which eventually results in antitumor activity and cell death.35,50 (4) Selinexor directly inhibits osteoclastogenesis and bone resorption with little effect on osteoblasts and bone marrow stromal cells by blocking RANKL-induced nuclear factor κB(NF-κB) and nuclear factor of activated T cell c1(NFATc1). 11 This mechanism is unique to MM. SINEs have been shown to be selectively cytotoxic to neoplastic cells. Inhibition of the nuclear export function of XPO1 leads to the death of malignant cells. However, normal cells are largely spared.38–40
Selinexor-based clinical trials in MM
Efficacy of selinexor and dexamethasone in clinical trials
In an early study (NCT01607892), the efficacy of selinexor monotherapy and selinexor in combination with dexamethasone (Xd) in heavily pretreated RRMM and Waldenstrom macroglobulinemia (WM) patients was tested. Eighty-four subjects, consisting of 81 patients with MM and 3 with WM, were included in the study. Selinexor monotherapy demonstrated limited effectiveness, with an objective response rate (ORR) and a clinical benefit rate (CBR) of 4% and 21%, respectively. But when dexamethasone was added, the ORR went up to 50% and the CBR went up to 58%. The study strongly suggests that selinexor synergizes with dexamethasone to induce MM cell death. This result prompted the pivotal phase II study of selinexor with dexamethasone (STORM trial). Nausea (75%), fatigue (70%), anorexia (64%), vomiting (43%), weight loss (32%), and diarrhea (32%) were the most common nonhematologic adverse events (AEs), of which the majority were grade 1 or 2. Hematologic toxicity was the most prevalent grade 3 or 4 toxicity, with thrombocytopenia (45%), neutropenia (23%), and anemia (23%) being the most common. Hyponatremia in grade 3 was also common (26%). 51
STORM was a global, phase IIb, multicenter, open-label study that explored the curative effect and safety of selinexor in combination with low-dose dexamethasone in patients with heavily pretreated, refractory myeloma. The study consisted of two independent parts. Part 1 enrolled a total of 79 RRMM patients, with 48 patients with quad-refractory disease (myeloma refractory to bortezomib, carfilzomib, lenalidomide, and pomalidomide) and 31 patients with penta-refractory disease (with a subset also refractory to an anti-CD38 antibody). 52 The total ORR was 21%. The ORR was similar between the quad-refractory disease group (21%) and the penta-refractory disease group (20%). The ORR in the high-risk cytogenetic group [including t(4;14), t(14;16), and del(17p) patients] was 35%. Thrombocytopenia (59%) was the most prevalent grade 3 AE, followed by anemia (28%), neutropenia (23%), hyponatremia (22%), leukopenia (15%), and fatigue (15%). The second part of this trial was a confirmatory study that enrolled 122 RRMM patients who were exposed to five agents but refractory to three (at least 1 IMiD and 1 PI and anti-CD 38 antibodies). 1 The total ORR was 26%. The median duration of response (mDOR), median progression-free survival (mPFS), and mOS were 4.4, 3.7, and 8.6 months, respectively. The penta-refractory disease group (83 patients) had an ORR of 25.3%. Based on the results of the penta-refractory disease group analysis, the FDA approved selinexor in combination with dexamethasone for the treatment of MM patients with penta-refractory disease in July 2019. Fatigue, nausea, and decreased appetite were common grade 1 or 2 AEs. Thrombocytopenia occurred in 73% of patients (25% grade 3, 33% grade 4). It is worth noting that a subset analysis showed that in the 16 patients with plasmacytomas (the majority of which were soft tissue), 9 of the patients’ plasmacytomas either completely resolved or decreased in size and/or metabolic activity. 53 MM with extramedullary disease usually responds poorly to conventional chemotherapy and has dismal outcomes. 54 Selinexor may bring new hope for MM with extramedullary disease.
The MARCH study is a bridging study designed to verify the data from STORM. It investigated the efficacy and safety of Xd regimens in Chinese patients with RRMM refractory to both PIs and IMiDs. In the 82 patients included in the study, an ORR of 29.3% was observed. The mPFS and mOS were 3.7 and 13.2 months, respectively. The study also evaluated several high-risk subgroups: a triple-class refractory population (refractory to a PI, an IMiD, and daratumumab), ORR = 25.0%; patients previously treated with chimeric antigen receptor T-cell (CAR-T-cell) therapy, ORR = 50.0%; patients carrying high-risk cytogenetic abnormalities, ORR = 25.5%; and elderly patients (⩾65 years), ORR = 28.6%. The most common grade 3–4 AEs were anemia (57.3%), thrombocytopenia (51.2%), lymphopenia (42.7%), neutropenia (40.2%), hyponatremia (29.3%), and lung infection (26.8%). The MARCH trial verified the effectiveness and safety of selinexor combined with dexamethasone in a Chinese population with RRMM, consistent with the STORM study. 55
Efficacy of selinexor, bortezomib, and dexamethasone in clinical trials
The BOSTON study was a randomized, open-label, single-arm phase III study that evaluated the clinical efficacy of selinexor, bortezomib, and dexamethasone (XVd) group compared with bortezomib and dexamethasone (Vd) group in RRMM. In total, 402 participants were included in the trial; 195 participants were allocated to the XVd group and 207 to the Vd group. The doses of bortezomib and dexamethasone were reduced by 40% and 25%, respectively, in the XVd group compared with the Vd group. With a median follow-up time of 13.2 months, the PFS was 13.93 months in the XVd group. With a median follow-up time of 16.5 months, the PFS was 9.46 months in the Vd group. In the following subgroups, the XVd group outperformed the Vd group in terms of PFS and ORR: patients over 65 years old, frail patients, patients with high-risk cytogenetics [such as del(17p)], patients with moderate renal insufficiency, and patients who had previously received bortezomib or lenalidomide. Notably, a post hoc analysis showed that selinexor can benefit patients with RRMM regardless of cytogenetic status. The most frequent grade 3–4 AEs were thrombocytopenia (39% of patients in the XVd group versus 17% of patients in the Vd group), fatigue (13% versus 1%), anemia (16% versus 10%), and pneumonia (11% versus 11%). Peripheral neuropathy of grade 2 or greater was less common in the XVd group than in the Vd group (21% versus 34%). The adverse effect profiles of the two groups were distinct. Peripheral neuropathy was more prevalent in the Vd group than in the XVd group, whereas thrombocytopenia was more prevalent in the XVd group than in the Vd group. Based on the results of the BOSTON study, the FDA authorized the XVd regimen for MM patients who have received at least one previous treatment. 56
STOMP was a multiarm, phase Ib/II study that evaluated the efficacy and safety of selinexor combined with other treatments (including the XKd, XVd, XPd, XRd, and XDd regimens) in MM patients. The XVd arm included people progressing after more than or equal to one prior therapeutic regimen but were not refractory to bortezomib in their most recent therapy. The XDd arm included people who had received more than or equal to three prior lines of therapy (including a PI and an IMiD) or who were dual-resistant to PI and IMiD. People who had already been treated with PI and lenalidomide were included in the XPd arm. Treated patients who were not resistant to carfilzomib were included in the XKd arm. There were two types of patients in the XRd arm: those who were first-treatment patients and those who had received more than or equal to one prior line of therapy. The XVd group included 42 patients. Patients had received a median of three previous treatments (ranging from 1 to 11), and 50% of them were refractory to a PI. The overall ORR was 63%, with PI-nonrefractory patients having an ORR of 84% and PI-refractory patients having an ORR of 43%. The mPFS for all patients was 9.0 months; for PI-nonrefractory patients, it was 17.8 months, and for PI-refractory patients, it was 6.1 months. These results confirm that the combination of selinexor with bortezomib appears to produce synergistic effects to overcome bortezomib resistance, in agreement with the results of preclinical studies. 57 Common grade 3–4 treatment-related adverse effects included thrombocytopenia (45%), neutropenia (24%), fatigue (14%), and anemia (12%). The incidence of peripheral neuropathy was low (10%). The decreased incidence of peripheral neuropathy was linked to the decreased dose of bortezomib, whereas the increase in hematologic toxicity incidence was linked to the addition of selinexor. 58
A phase II trial (SELVEDEX; EudraCT2014-002444-40) of XVd in patients with progressive or refractory MM was stopped early owing to toxicity. However, in patients for whom this regimen was feasible, effectiveness in terms of ORR, PFS, and overall survival (OS) was seen. 59
There are no studies on XVd used as a first-line treatment for MM patients, and clinical trials of XVd have been conducted primarily in populations previously treated with one to three lines of therapy. In the NCCN guidelines, the XVd regimen is recommended as a category 1 regimen for MM in early relapse (one to three prior therapies). 60 The clinical benefit of using XVd after early relapse appears to be somewhat greater than the clinical benefit of multi-line relapse (Table 1).
Summary of important clinical trials with XVd regimens.
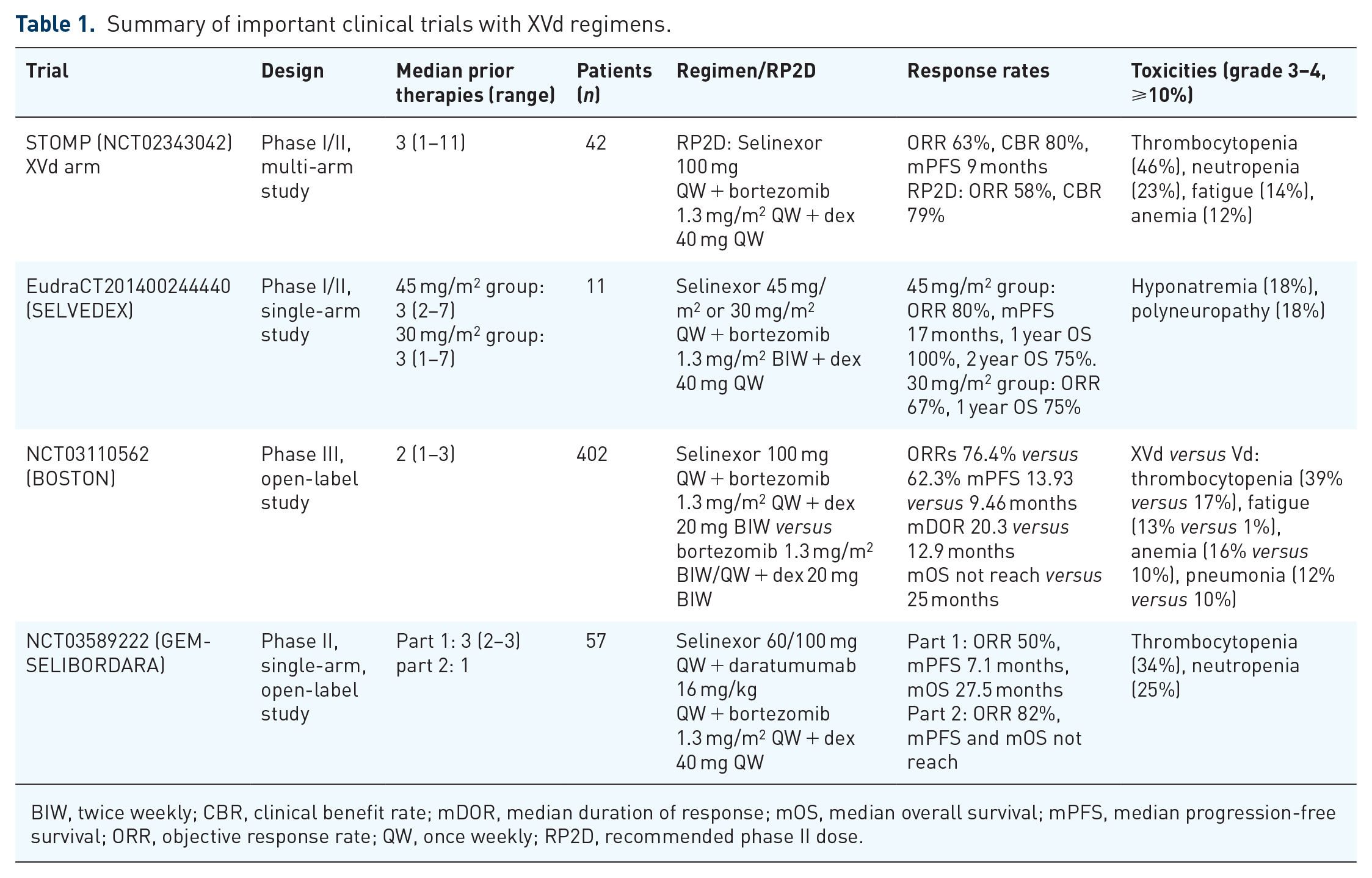
BIW, twice weekly; CBR, clinical benefit rate; mDOR, median duration of response; mOS, median overall survival; mPFS, median progression-free survival; ORR, objective response rate; QW, once weekly; RP2D, recommended phase II dose.
Efficacy of selinexor, carfilzomib, and dexamethasone in clinical trials
The selinexor, carfilzomib, and dexamethasone (XKd) group, which included 32 patients, was a part of the STOMP study. The results revealed that patients had a 78% ORR [including 44% of patients having very good partial response (VGPR) or better], and the mPFS was 15 months. Importantly, efficacy was preserved in patients with genetically high-risk diseases. The high-risk cytogenetics group achieved an ORR of 82.4%, an mPFS of 15 months, and an mDOR of 22.7 months; the mOS was not achieved. Common AEs included thrombocytopenia (72%), nausea (72%), anemia (53%), and fatigue (53%). 61
Another phase I study evaluated the efficacy of the XKd regimen (NCT02199665). The study enrolled 21 RRMM patients who had previously received a median of four lines of therapy. The CBR was 71% and the ORR was 48%. The mPFS and mOS were 3.7 and 22.4 months, respectively. The most common grade 3 and 4 toxicities were thrombocytopenia (71%), anemia (33%), lymphocytopenia (33%), neutropenia (33%), and infections (24%). 62
Efficacy of selinexor, pomalidomide, and dexamethasone in clinical trials
The STOMP study evaluated the efficacy of selinexor, pomalidomide, and dexamethasone (XPd) group. It enrolled 48 patients, of whom 40 had received autologous hematopoietic stem cell transplantation. The ORR was 58% and the mPFS was 12.2 months among pomalidomide-naïve patients. The ORR was 31% and the mPFS was 4.2 months among patients resistant to lenalidomide or pomalidomide. Notably, the XPd regimen has also been shown to work well in patients who do not respond to pomalidomide. This result suggests that the agents can be used together to help overcome resistance. Common hematologic AEs included neutropenia (62%), thrombocytopenia (54%), anemia (46%), and leukopenia (28%). Common nonhematologic AEs included nausea (56%), fatigue (50%), decreased appetite (46%), decreased weight (33%), diarrhea (27%), and vomiting (23%). 63
Efficacy of selinexor, ixazomib, and dexamethasone in clinical trials
A phase I study, which included 18 RRMM patients, tested the efficacy of selinexor, ixazomib, and dexamethasone (XId) group. The ORR was 22% and the longest duration of response was 14 months. The most common non-hematological adverse reactions were gastrointestinal (GI) adverse reactions, including nausea (50%), vomiting (33%), diarrhea (22%), and anorexia (28%). Fatigue (56%), elevated aspartate aminotransferase (22%) and alanine aminotransferase (27%), hyperglycemia (66%), hypophosphatemia (39%), hyperkalemia (21%), hypocalcemia (32%), and hyponatremia (28%) were also relatively common. The hematologic AEs were, in order of frequency, thrombocytopenia (72%), anemia (61%), and neutropenia (28%). GI adverse effects may limit the application and efficacy of this drug combination. 64
Efficacy of selinexor, daratumumab, and dexamethasone in clinical trials
The STOMP study also evaluated the efficacy of selinexor, daratumumab, and dexamethasone (XDd) group in RRMM. The study included 34 RRMM patients, 6% of whom were refractory to daratumumab. The ORR was 73% and the mPFS was 12.5 months in daratumumab-naïve patients. No response was noted in the patients with daratumumab-refractory disease.
The most common AEs were as follows: thrombocytopenia (70.6%), nausea (70.6%), fatigue (61.8%), anemia (61.8%), and neutropenia (50.0%). 65
A multicenter, open-label phase II trial (NCT03589222) evaluated the efficacy and safety of selinexor in combination with daratumumab, bortezomib, and dexamethasone (XVDd) group for RRMM. The study had two parts and included a total of 57 patients. In part 1, 24 patients who had received more than or equal to three prior lines of therapy received XVDd on a 4-week cycle. In total, 96% and 71% of patients had MM refractory to lenalidomide and a PI, respectively, and 71% had MM that was refractory to both agents. The ORR in part 1 was 50%. The mPFS and mOS were 7.1 and 27.5 months, respectively. In part 2, 33 patients who had received more than or equal to one prior line of therapy received XVDd on a 5-week cycle. Forty-five percent of the patients were refractory to lenalidomide and 12% were double refractory. The ORR in part 2 was 82% and the mOS and mPFS were not reached. Thrombocytopenia was the most frequent hematological AE (68.4%), whereas GI toxicity was the most frequent nonhematological AE (38%). A total of 61.4% of patients required dose adjustments. Selinexor was the most frequently modified drug. 66
Efficacy of selinexor, lenalidomide, and dexamethasone in clinical trials
White et al. 67 conducted a multicenter, open-label phase Ib/II study to evaluate the efficacy of selinexor, lenalidomide, and dexamethasone (XRd) group. In total, 24 patients were included, of whom 20 were evaluable. The all-oral XRd regimen had significant efficacy in patients with RRMM who had not received prior lenalidomide treatment. In lenalidomide-naïve patients, the ORR and CBR were 92%. In patients who had previously received lenalidomide treatment, the ORR and CBR were 13% and 38%, respectively. The median PFS was 10.3 months overall. The median PFS for lenalidomide-naïve individuals was not achieved, whereas it was 2.8 months for lenalidomide-exposed patients. Common AEs included nausea (58%), decreased appetite (42%), fatigue (38%), decreased weight (38%), vomiting (33%), constipation (25%), and diarrhea (25%). Most of these AEs were mild (grade 1 or 2) and very manageable. The most common grade 3 or higher AEs were thrombocytopenia and neutropenia (63% each). 67
White et al. 68 also evaluated the safety and efficacy of the XRd regimen in patients with newly diagnosed MM. Eight patients with newly diagnosed MM were included in the study. Among the seven efficacy-evaluable participants, the ORR was 86% after a median follow-up of 6.1 months. The mPFS has not been reached. Grade 3/4 AEs were generally hematologic, including neutropenia (75%), anemia (25%), and thrombocytopenia (25%). Apart from fatigue (38%), nonhematologic AEs were all grade 1 or 2, including diarrhea (63%), nausea (50%), decreased weight (38%), constipation (25%), hypokalemia (25%), and hypomagnesemia (25%). 68 The XRd regimen may be a viable option for induction therapy for newly diagnosed MM patients who cannot tolerate bortezomib. However, the sample size of the study was small.
Efficacy of selinexor, liposomal doxorubicin, and dexamethasone
In a preclinical experiment, selinexor synergistically enhanced the antimyeloma effects of liposomal doxorubicin. 69 While improved outcomes were observed in the preclinical study, emerging outcome data from the observational study of clinical trial patients suggests that the clinical trial efficacy differs from the preclinical experiment efficacy. Baz et al. 70 reported the results of a phase I/II study of selinexor in combination with liposomal doxorubicin and dexamethasone in patients with RRMM. While liposomal doxorubicin added to selinexor and dexamethasone was well tolerated, it did not appear to enhance the ORR of selinexor combined with dexamethasone in the extensively pretreated patient population (the ORR was 15%) (Table 2).
Clinical trials with selinexor in multiple myeloma.

ASCT, autologous stem cell transplantation; CBR, clinical benefit rate; IMiD, immunomodulatory drugs; mDOR, median duration of response; mOS, median overall survival; MM, multiple myeloma; mPFS, median progression-free survival; NDMM, newly diagnosed MM; ORR, objective response rate; PI, proteasome inhibitor; RP2D, recommended phase II dose; VGPR, very good partial response; WM, Waldenstrom macroglobulinemia.
AEs and treatment measures
Adverse effects of selinexor include hematologic toxicity (thrombocytopenia, neutropenia, and anemia), as well as nonhematologic toxicity, including nausea, vomiting, weight loss, diarrhea, decreased appetite, hyponatremia, fatigue, and so on. These adverse effects are typically grade 1/2, reversible, and responsive to supportive treatment.61,71
Hematologic toxicity
Thrombocytopenia is the most common hematological AE and one of the most common causes of discontinuation, which typically occurs at a median time of 22 days. Grade 3/4 thrombocytopenia is more common, although bleeding episodes are infrequent overall (<3%). 72 As is well known, thrombopoietin (TPO) promotes downstream signal transducer and activator of transcription 3 (STAT3) phosphorylation by binding to the TPO receptor (c-MPL), and STAT3 binds to XPO1 and translocates out of the nucleus, contributing to the development and maturation of precursor hematopoietic stem cells into megakaryocytes. Selinexor binds to XPO1 in precursor hematopoietic stem cells and inhibits its function, causing the phosphorylated STAT3 to remain in the nucleus, up-regulating the expression and activity of Klf4 and Oct4, and preventing the differentiation and maturation of megakaryocytes. 73 The selinexor-induced thrombocytopenia is reversible and recovers after 1–2 weeks of discontinuation. 74 Platelet transfusions, TPO receptor agonists (TPO-RAs), dose reductions, and dose interruptions were common strategies used to manage thrombocytopenia. The median time from the start of selinexor therapy to any grade of neutropenia was day 21. Supportive therapy (such as granulocyte colony-stimulating factor) and dose reduction helped to alleviate symptoms. 72
GI toxicity
GI AEs like nausea, vomiting, diarrhea, and decreased appetite are a major safety and tolerability challenge for patients. Fortunately, nausea and vomiting were reduced with the prolonged period of treatment. The median time for selinexor to cause any level of nausea and vomiting was day 3. The BOSTON study showed that the incidence of nausea decreased with the duration of treatment, with more than 90% of patients not experiencing nausea after completing the first two treatment cycles. 75 Vomiting may be related to the ability of selinexor to permeate the blood–brain barrier. 71 In addition to the usual peripheral and central pathways, selinexor may trigger the vomiting response by directly stimulating the vomiting center. Prophylactic therapy can lessen the incidence of nausea and vomiting brought on by selinexor. It is recommended that two combinations of antiemetic agents (a 5-hydroxytryptamine-3 receptor antagonist and either a neurokinin 1 receptor antagonist or olanzapine) be given before and during selinexor therapy and that triple antiemetic therapy (a 5-hydroxytryptamine-3 receptor antagonist in combination with olanzapine and a neurokinin 1 receptor antagonist) be considered if necessary. 72 The median time for any level of anorexia and weight loss to occur with selinexor is day 8. Active weight monitoring, nutritional counseling and supplementation, the use of appetite regulators, and selinexor dosage modifications all work. 72
Other
The median time to any level of hyponatremia in selinexor was day 19.5. The cause of hyponatremia is unknown and may be multifactorial, generally short-lived and reversible. 76 Dietary supplementation is a proven tool. Patients with grade 3 and higher hyponatremia need to be off medication. Fatigue or weakness is also a common adverse effect of selinexor treatment and usually decreases after treatment. Supportive care for this symptom should begin with identifying and correcting underlying factors that may be causing fatigue. 74 Stimulants, such as oral methylphenidate, may also be considered to correct fatigue, and diet and nutritional intake should be monitored.
Recent advances
Selinexor resistance
Selinexor has demonstrated promising therapeutic potential. However, selinexor resistance has been observed in in vitro tumor models.77,78 Kashyap et al. 79 found that elevated NF-κB activity leads to selinexor resistance. Crochiere et al. 77 found that SINE resistance is associated with changes in signaling pathways downstream of XPO1 inhibition and upregulation of the transcription factor E2F1. 78 Neggers et al. 80 found that resistance to selinexor was related to the heterozygous mutation of cysteine 528 in XPO1. Of note, the treatment options for patients with diseases resistant to selinexor are more limited. Scientists are working diligently to explore potential predictors of selinexor efficacy. Through exploratory biomarker analyses (RNA sequencing of biopsies) of 188 patients with advanced unresectable dedifferentiated liposarcoma treated with selinexor, Walker et al. 81 identified genes associated with selinexor sensitivity. The researchers found that low expression of CALB1 and high expression of GRM1 were associated with high sensitivity to selinexor. Restrepo et al. 82 performed RNA sequencing of CD138+ tumor cells from bone marrow samples of MM patients who received selinexor treatment. The researchers found that WNT10A, DUSP1, and ETV7 upregulation were associated with selinexor sensitivity. 82 Pharmacogenomics analysis of selinexor could be helpful for precision medicine strategies.
Second-generation SINEs
Studies of the second-generation SINE eltanexor are ongoing. Compared with selinexor, eltanexor has a decreased ability to penetrate the blood–brain barrier, which leads to lower rates of central nervous system (CNS)-related side effects (e.g. anorexia, weight loss, fatigue, and hyponatremia).83–85 Moreover, in in vivo models of acute myeloid leukemia and chronic lymphocytic leukemia, eltanexor (KPT-8602) has shown better preclinical efficacy than KPT-330 (selinexor). 86 Cornell et al. 87 showed the efficacy of selinexor monotherapy and selinexor combined with dexamethasone in individuals with RRMM. Patients were initially treated with eltanexor monotherapy and 31 patients could be evaluated for efficacy. The ORR was 13% (4/31). The CBR was 45% (14/31). Patients who had a minor response (MR) after one cycle or a partial response (PR) after two cycles were allowed to receive combination dexamethasone. In the patients treated with dexamethasone, the ORR was 29% (2/7), and the CBR was 71% (5/7). Similar to selinexor, eltanexor also produces synergistic effects with dexamethasone. 87 Eltanexor acted synergistically with common anti-MM drugs, including bortezomib, carfilzomib, doxorubicin, melphalan, topotecan, and etoposide and induced apoptosis in numerous MM cell lines, as shown by Turner et al. 88 In the near future, we can expect more data from clinical trials. The published results suggest the therapeutic potential of eltanexor in combination therapy. However, since eltanexor cannot cross the blood–brain barrier, its anti-MM activity in the CNS may be limited.
Selinexor combined with venetoclax
In basic research, the combination of selinexor and venetoclax has shown synergistic effects in MM cell lines. Specifically, t(11;14)-positive cell lines were found to be more sensitive to the drug combination than non-t(11;14) cell lines, and the combination produced greater synergistic effects in the t(11;14)-positive cells. Furthermore, the researchers observed that two patients with t(11;14) RRMM responded to venetoclax but then progressed. The patients then received venetoclax combined with selinexor treatment and achieved and MR. 89
Selinexor + CAR-T-cell therapy
CAR-T-cell therapy is a promising strategy for RRMM treatment. However, treatment options for patients who relapse post-CAR-T-cell therapy are limited. Chari et al. 90 investigated the efficacy of treatment with selinexor after progression on CAR-T-cell therapy. Patients with high-risk cytogenetic features received a median of 10 prior treatments (including autologous hematopoietic stem cell transplantation). After progressing on CAR-T-cell therapy, seven patients received selinexor-based therapy (one received Xd, one received XVd, and five received XKd). One patient achieved stringent complete response, three achieved VGPR, two achieved PR, and one achieved MR. The most common AEs were nausea, fatigue, thrombocytopenia, neutropenia, and anemia. Most patients required a selinexor dose interruption or reduction during the course of treatment. Selinexor is a potentially useful agent for patients who relapse following CAR-T-cell therapy. 90 Disease progression during the CAR-T-cell preparation process is common in the clinic. 91 However, treatment strategies bridging to CAR-T-cell therapy are inadequate. 92 In basic research, when target cells were pretreated with a SINE, CAR-T-cell cytotoxicity rose dramatically, and the exhaustion of CAR-T cells decreased. 93 More clinical trials of selinexor and CAR-T-cell combination therapy are underway. The published data suggest that selinexor-based treatment may also serve as a bridge to cellular therapies.
Selinexor combined with autologous stem cell transplantation
Preliminary findings from the phase I portion of a phase I/II study (NCT02780609) using selinexor and high-dose melphalan as a conditioning regimen for autologous stem cell transplantation (ASCT) show that the combination is well tolerated and does not affect engraftment kinetics. These results have led to the continuation of phase II of this study (NCT02780609). 94
Deeper responses after ASCT have been associated with better PFS and OS. 95 Selinexor is a good candidate to be used in combination with lenalidomide) for maintenance therapy because of its oral bioavailability and weekly frequency. ALLG MM23 SeaLAND is a randomized, multicenter, phase III trial of maintenance therapy after ASCT in MM. Twenty patients have received three–six cycles of induction and recovered post-ASCT. Then they came to a lead-in safety phase with XR: lenalidomide 10 mg QD d1–21 and selinexor 40 mg QW 28d/cycle. If well tolerated, selinexor was increased to 60 mg po QW from cycle 2 and lenalidomide to 15 mg po QD from cycle 4. Safety will be assessed after cycle 2 is completed in 10th and 20th patients. After safety criteria were met, 290 patients were randomized 1:1 to receive XR or lenalidomide and treated until PD. The primary endpoint is a 3-year PFS rate. Secondary endpoints include ORR and minimal residual disease (MRD) negativity rates, PFS on the next treatment line (PFS2), OS, safety and tolerability, quality of life, and cost-effectiveness. In total, 232 patients completed the 3-year follow-up for the primary analysis. However, this clinical trial has yet to post any results or conclusions. 96
Real-world data
A real-world study included 53 patients with RRMM treated with a selinexor combination regimen (XDd, XPd, XVd); 47 patients were evaluable for efficacy. An ORR of 44.7% and a mDOR of almost 8 months were achieved. In terms of safety, the main adverse effects of the selinexor-containing regimens were hematologic toxicity: the incidence of neutropenia, lymphocytopenia, and thrombocytopenia was 83%, 39.6%, and 81.1%, respectively. The incidence of selinexor dose reduction due to bone marrow suppression was 7.7%. Among the nonhematological AEs, the most common AEs included infection (39.6%), malaise (57.8%), and nausea and vomiting (52.8%). The incidence of chemotherapy discontinuation due to adverse reactions was 7.0%. A three-drug combination regimen based on Xd could be an effective treatment option for RRMM in the real world. 97
Discussion
Limitation
Regrettably, selinexor did not show a better treatment effect than CAR-T-cell treatment or ASCT. Selinexor is much less successful than CAR-T-cell therapy in terms of total response rate, depth of response, and durability of response.98,99 Cengiz et al. 100 compared the efficacy of salvage autologous hematopoietic cell transplantation (sAHCT) and XVd in the treatment of RRMM. Compared with sAHCT, XVd achieved similar PFS and OS in RRMM patients. However, there were fewer patients treated with XVd (22 patients treated with sAHCT versus 10 patients treated with XVd). 100 Although selinexor does not appear to be superior to hematopoietic stem cell transplantation or CAR-T-cell therapy in terms of clinical effectiveness, its use as a bridging therapy to CAR-T-cell therapy and a supplement to the conditioning regimen for ASCT appears promising.93,94
AEs are an important concern in treatment, the most prominent of which are hematological toxicity and GI toxicity. 101 This could be because the clinical trial participants have undergone multiline therapy. The real-world patient population is very heterogeneous. Thus, further exploration of AE data is needed. Furthermore, dose adjustment to reach a balance between clinical efficacy and adverse effects is worth exploring. The STORM study employed twice-weekly selinexor (80 mg orally) at a total weekly dose of 160 mg. In total, 18% of patients had treatment interruptions because of AEs. Large doses brought on by twice-weekly dosing have been linked to severe AEs. This study emphasizes the importance of implementing appropriate dose adjustments. In the BOSTON study, selinexor was given orally at a dose of 100 mg once a week (median dose: 80 mg once a week). The STOMP study explored the recommended phase II dose (RP2D) of selinexor-based combination regimens (XVd, XDd, XPd, XKd, and XRd). Selinexor is administered at a lower dose when used in conjunction with other anti-myeloma treatments, ranging from a cumulative dose of 40–100 mg given once weekly. Combining RP2D from different clinical studies, the recommended starting dose range for selinexor when used in conjunction with other antimyeloma drugs is 60–100 mg once/week and 40–60 mg once/week may be taken into consideration as the starting dose for a four-drug combination regimen. 72 Low-dose selinexor initiation may be reasonably safe for individuals who are older, frailer, and have a lower bone marrow reserve. A post hoc analysis compared the efficacy outcomes and AEs between patients whose dose was reduced and those who received the same starting dose. Appropriate dose reductions of selinexor were linked to longer PFS, DOR, and time to next treatment, as well as fewer adverse effects and better tolerability, highlighting the benefit of appropriate dose modification to manage toxicities. 102 ASCT is an important therapeutic option for patients with MM who are eligible for transplantation and have achieved at least a PR after combination chemotherapy. Although Nishihori et al. 94 demonstrated that using selinexor as a conditioning regimen did not affect engraftment kinetics, the effect of selinexor on myelosuppression and stem cell collection was not fully determined. Therefore, selinexor should be offered with caution to people who are receiving hematopoietic stem cell transplantation.
Discontinuation and/or tapering of the selinexor for AEs were common. The management of selinexor-associated adverse effects is always challenging for physicians. Furthermore, resistance to selinexor is also an issue that deserves attention. Next-generation SINEs with enhanced reversibility of XPO1 covalent binding are expected to reduce AEs.
Conclusion
Treatment strategies for MM have gained momentum in recent years. However, the prognosis for RRMM remains poor. Selinexor, a specific inhibitor of XPO1, is already approved for clinical use. Selinexor has shown encouraging results in RRMM. When combined with other medicines, selinexor displays superior therapeutic effects. For instance, there was a significant survival benefit for some patients with RRMM who had high cytogenetic risk, particularly for those with del(17p).
There are many future opportunities for selinexor treatment in MM, and the use of selinexor in the treatment of established and newly diagnosed MM, as well as extramedullary disease and CNS myeloma, needs to be further studied.