
Abstract
Background:
Evidence that a venetoclax (VEN)-combined regimen is effective in relapsed/refractory acute myeloid leukemia (R/R AML) is emerging. However, it is unknown how VEN-combined low intensity treatment compares to intensive chemotherapy (IC) in medically fit patients with R/R AML.
Methods:
We compared AML patients who received IC (n = 89) to those who received a VEN in combination with hypomethylating agents or low dose cytarabine (VEN combination) (n = 54) as their first- or second-line salvage after failing anthracycline-containing intensive chemotherapy.
Results:
The median age was 49 years, and significantly more patients in the VEN combination group were in their second salvage and had received prior stem cell transplantation (SCT). Overall response rates including CR, CRi, and MLFS were comparable (44.0% for IC vs. 59.3% for VEN combination, p = 0.081), but VEN combination group compared to IC group tended to show lower treatment related mortality. The rate of bridging to SCT was the same (68.5%), but the percentage of SCT at blast clearance was significantly higher in the VEN-combined group (62.3% vs. 86.5%, p = 0.010). After median follow-up periods of 22.5 (IC) and 11.3 months (VEN combination), the median overall survival was 8.9 (95% CI, 5.4-12.4) and 12.4 months (95% CI, 9.5-15.2) (p = 0.724), respectively.
Conclusion:
VEN combination provides a comparable anti-leukemic response and survival to salvage IC, and provide a bridge to SCT with better disease control in medically-fit patients with R/R AML.
Keywords
Introduction
Relapsed/refractory acute myeloid leukemia (R/R AML) confers a dismal outcome.1–3 Despite advances in treatment, survival has not improved during the last decade, and treatment remains challenging in this group of patients. For patients who have primary refractory disease or relapse, only a few patients experience blast clearance on salvage regimen and can be bridged successfully to allogeneic stem cell transplantation (allo-SCT).4,5
Venetoclax (VEN), an orally active and potent small molecular inhibitor targeting B-cell lymphoma 2 (BCL2), received accelerated US Food and Drug Administration (FDA) approval in November 2018, for newly diagnosed elderly or medically unfit AML patients when used in combination with a hypomethylating agent (HMA)6,7 or low-dose cytarabine (LDAC).8,9 Although the approval is currently restricted to newly diagnosed AML, recent publications indicate that VEN combination (VEN-comb) therapy is effective in AML patients in the relapsed or refractory setting, with reported response rates ranging from 31% to 64%.10–15 Given that the response rate of salvage intensive chemotherapy (IC) has been reported from 32% to 63%,16–23 it seems that the ability to induce remission in R/R AML is not different between salvage IC and the VEN-comb regimen, although the latter is classified as less-aggressive therapy compared to the conventional cytotoxic IC regimen.
The previous studies that have dealt with the VEN-comb regimen in R/R AML usually include patients of considerable heterogeneity with regard to previous treatment, age, and ability to tolerate intensive therapy such as SCT. For patients with the appropriate condition, aggressive approaches using IC have generally been offered as salvage therapy.4,24,25 However, it is unknown how VEN-comb compares to IC in medically fit patients with R/R AML.
Here, we compared the anti-leukemic response and survival outcomes of IC and VEN-comb when utilized as salvage options in AML patients who were refractory to or relapsed after anthracycline-containing chemotherapy in real-world practice.
Methods
Changes in institutional strategy for salvage therapeutic options in R/R AML
AML patients in our country have been allowed to receive VEN-comb since early 2020, if patients aged ⩾65 years were not eligible for IC or adult patients at any age had relapsed or refractory disease. Before the introduction of this novel agent, our institutional therapeutic strategies in the salvage setting for fit AML were comprised almost entirely of other cytotoxic regimens, which include either an etoposide-, fludarabine-, or high-dose cytarabine-containing regimen, unless patients were enrolled in a clinical trial or suitable for target agents. The use of VEN-combs in R/R setting in our institution was originally started as a salvage therapy for patients who became fragile during the prior IC with aiming to provide safer bridge to transplantation. With accumulation of experiences, we have found that this regimen is not only safe but also just as effective as intensive salvage IC through preliminary internal analysis. Thereafter, we have expanded the use of VEN-combs to R/R patients of better medical condition, and redeveloped our institutional strategies and prioritized the use of VEN-comb regimen over conventional cytotoxic therapeutics in the salvage treatment setting in R/R AML in February 2020.
Patients
Adult AML patients (age ⩾ 18 years) who were refractory to or relapsed after the anthracycline plus cytarabine induction regimen and were candidates for intensive salvage chemotherapy were subjected to this analysis. As a group of interest, R/R AML patients who received VEN-comb therapy were screened first, producing a total of 54 corresponding patients between February 2020 and January 2021. As a comparison, we searched for historical controls who were treated with salvage IC during the past 2 years, revealing a total of 89 patients between January 2018 and January 2020. Patients analyzed here received VEN-comb or IC as their first- or second-line salvage therapy, while patients in the third- or later-line salvage setting were excluded. This study was approved by the Institutional Review Board and Ethics Committee of the Catholic Medical Center in South Korea (KC21RISI0572). We have de-identified all personal details while conducting this retrospective study of 143 consecutive patients. Irrespective of this analysis, all patients had provided written informed consent before treatment. The reporting of this study conforms to the STROBE statement. 26
Treatment procedure
Conventional IC that patients received includes the following regimens: MEC (mitoxantrone 10 mg/m2/day for 4 days, cytarabine 2 g/m2/day for 4 days, and etoposide 100 mg/m2/day for 3 days); 27 FLANG (fludarabine 30 mg/m2/day, cytarabine 1 g/m2/day, mitoxantrone 10 mg/m2day, and G-CSF 300 μg/day for 5 days); 28 and FLAG-IDA (fludarabine 30 mg/m2/day and cytarabine 2 g/m2/day for 5 days, idarubicin 10 mg/m2/day for 3 days, and G-CSF 500 μg/day from day +6 until neutrophil recovery).29,30
As for the VEN-comb, VEN with HMA (VEN/HMA) or with LDAC (VEN/LDAC) was administered in 28-day cycles. In a schedule of VEN/HMA, either decitabine (20 mg/m2 days 1–5, intravenous) or azacitidine (75 mg/m2 days 1–7, subcutaneous) could be chosen at the physician’s discretion and was combined with VEN, dosed at 100 mg on day 1, 200 mg on day 2, and 400 mg on days 3–28 of cycle 1.6,7 In cases of VEN/LDAC, VEN 100 mg on day 1, 200 mg on day 2, 400 mg on day 3, and 600 mg on days 4–28 of cycle 1 were administered with subcutaneous cytarabine (20 mg/m2 days 1–10) injection.8,9 From the second cycle, VEN was started at 400 mg (VEN/HMA) or 600 mg (VEN/LDAC). Dose interactions between VEN and concomitant medications were considered, and the VEN dose was reduced to 1/2 in patients receiving moderate CYP3A4 inhibitors (e.g. fluconazole) and to 1/4 in patients receiving strong CYP3A4 inhibitors (e.g. voriconazole, posaconazole, and itraconazole). If the azole antifungals were replaced by other spectral antifungals such as echinocandin (e.g. caspofungin) or amphotericin B based on clinical situation, the VEN dose was increased to the original target dose.
Regardless of which salvage therapy was used, simultaneous preparation for SCT had begun for all the patients included, with aiming to undergo allo-SCT after salvage therapy cycles unless they became unsuitable for transplantation. Figure 1 represents the sequential steps of the treatment process by therapeutic arm, and detailed information of prior treatment before these salvage therapeutics is presented in Supplementary Table 1. Among the patients receiving salvage IC (n = 89), MEC was most commonly administered (n = 68, 76.4%) while FLANG and FLAG-IDA were used in 19 (21.3%) and two cases (2.2%). For patients of VEN-comb group, the median number of total cycles was 2 (range: 1–9), where more than half of the patients (n = 29, 53.7%) received two cycles; remaining patients received 1 (n = 12, 22.2%), 3 (n = 8, 14.8%), 4 (n = 4, 7.4%), and 9 (n = 1, 1.9%) cycles of treatment. In this study, we did not include patients who had been exposed to VEN or other targetable therapies except sorafenib (in combination with azacitidine) for patients with R/R FLT3-ITD-mutated AML (n = 2).
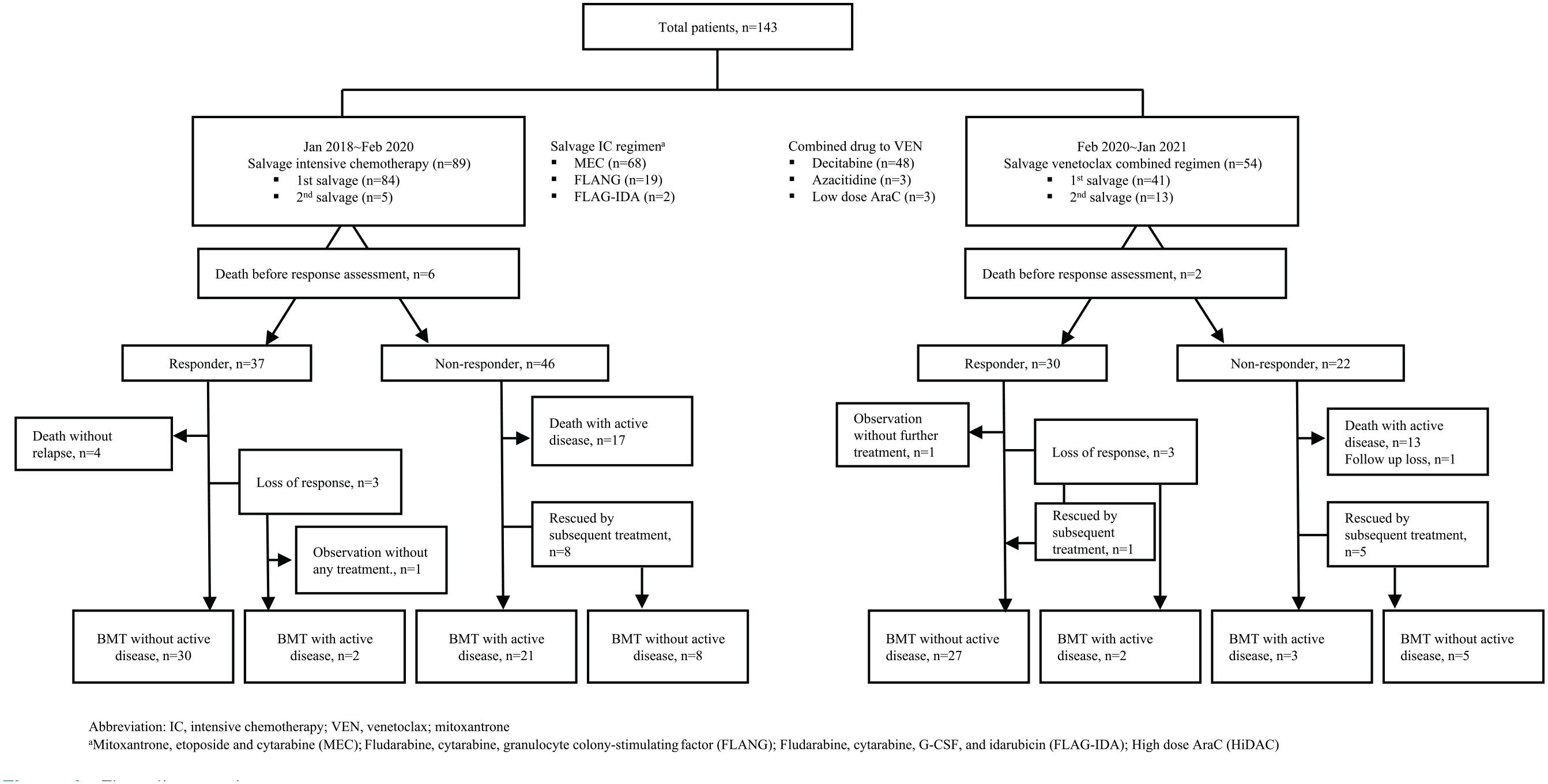
Flow diagram by treatment groups.
Response assessment
Morphological and cytogenetic measurements were performed during each bone marrow (BM) examination, and Wilms’ tumor gene 1 (WT1) transcript levels were used to assess the depth of the molecular response with a cut-off level of 250 copies/104 ABL1: ⩾250 copies for WT1high versus <250 copies for WTlow.31,32 Patients receiving IC were assessed with a BM examination after completion of salvage chemotherapy, usually at around 4–6 weeks of the cycle. For patients receiving VEN-comb, BM exams were performed every cycle until SCT or achieving response, whichever came first, and usually at day 21–28 of the cycle.
Information on genetic mutations
Genomic DNA was extracted from the BM aspirates with the QIAamp DNA Mini Kit (Qiagen, Hamburg, Germany). For detection of genetic mutation, next-generation sequencing (NGS) was performed using a customized St. Mary’s customized NGS panel for acute leukemia (SM acute leukemia panel) including 67 genes,33,34 while the detection of FLT3-ITD mutation, polymerase chain reaction (PCR) for fragment analysis was performed using a modified protocol as previously described.35–38 The mutation results used in this study almost (n = 98, 68.5%) relied on initial NGS results except for patients with available NGS results at relapse. For 37 patients with mutation results at diagnosis and at R/R disease, mutations were compared between the different time points, where 18 patients have shown changes in genetic mutations: gain of 20 mutations in 15 patients (ASXL1, n = 1; BCOR, n = 1; IKZF1, n = 2; CEBPA, n = 1; CSF3R, n = 1; GATA2, n = 4; EZH2, n = 1; WT1, n = 1; TET2, n = 2; KRAS, n = 1; NF1, n = 1; NRAS, n = 2; PTEN, n = 1; RAD21, n = 1), and loss of 10 mutations in five patients (CSF3R, n = 1; FLT3-TKD, n = 1; NRAS, n = 1; PTPN, n = 2; KRAS, n = 1; BCOR, n = 1; MYC, n = 1; RUNX1, n = 1).
Definition of outcomes
Anti-leukemic response after salvage treatment was assessed as per the international working group (IWG) criteria; 39 achievement of morphologic complete remission (CR), CR with incomplete hematologic recovery (CRi), and morphologic leukemia-free state (MLFS) were regarded as response to therapy. Overall survival (OS) was defined from initiation of salvage therapy to death from any cause on an intent-to-treat basis with non-censoring at the time of SCT. In addition to anti-leukemic therapeutic outcomes, hospital length of stay and transfusion requirements for survivors were assessed as a measure of medical resource use. Length of stay was the sum of hospitalization days at all admissions, and the number of red blood cell (RBC) and platelet (PLT) units transfused were counted and censored at the time of SCT.
Statistical analysis
The distributions and frequencies of patients’ characteristics were demonstrated using descriptive statistics. Differences between the two treatment groups were compared using the chi-square test or Fisher’s exact test for categorical variables and a two-sample t-test or Mann–Whitney U-test for continuous variables, and p value was corrected by Bonferroni’s method when multiple testing was indicated. The OS was estimated by the Kaplan–Meier method and compared by the log-rank test. Univariate and multivariate logistics were performed in assessment of factors affecting treatment response, and Cox proportional hazards regression models were used for identifying risk factors for OS. For variable selection in multivariate analysis, we included salvage option in the models as a variable of interest, and co-variables were selected by stepwise back- and forward-selection algorithm (threshold p value: 0.10). Among similar models, the model with the lowest AIC was chosen as the final model. Two-sided p values less than 0.05 were considered statistically significant. All statistical analyses were conducted using IBM SPSS statistics version 25 and R statistical software (version 3.4.3; R Foundation for Statistical Computing, Vienna, Austria).
Results
Comparison between IC and VEN-comb groups
The baseline characteristics of patients are presented in Table 1 and are compared between the treatment groups. Overall, median age was 49 years (range: 19–72 years), and there were 89 (62.2%) and 54 patients (37.8%) receiving salvage IC and VEN-comb, respectively. When the IC and VEN-comb groups were compared, there was no difference in clinical factors including age, sex, or disease types. As for molecular risk features by European Leukemia Net (ELN) 2017, 40 the proportions of ELN-classified favorable, intermediate, and adverse risk groups and cytogenetics were comparable between the groups. However, more patients in the VEN-comb group compared to those in the IC group were in their second-line salvage setting (5.6% for IC vs 24.1% for VEN-comb, p < 0.001) and had received prior SCT (13.5% for IC vs 38.5% for VEN-comb, p < 0.001). Regarding the response to first-line therapy, primary refractory diseases comprised the majority in the IC group, accounting for 75.3% of patients. Such patients comprised more than half of the VEN-comb group as well (57.4%), but cases with relapsed disease were frequently observed in this group compared to the IC group (24.7% for IC vs 42.6% for VEN-comb, p = 0.026).
Baseline characteristics.

ELN, European Leukemia Net; FLAG-IDA, fludarabine + cytarabine + G-CSF + idarubicin; FLANG, fludarabine + cytarabine + granulocyte colony-stimulating factor (G-CSF) + mitoxantrone; MEC, mitoxantrone + etoposide + cytarabine; SCT, stem cell transplantation.
MEC (n = 67), FLANG (n = 16), FLAG-IDA (n = 1).
MEC (n = 1), FLANG (n = 3), FLAG-IDA (n = 1).
Includes both secondary acute myeloid leukemia (AML) from antecedent hematologic disorder (n = 13) and therapy-related AML (n = 4).
Available n = 148.
Anti-leukemic response and bridging to SCT
After salvage treatment, the percentage of patients who had CR, CRi, and MLFS was 37.3%, 6.0%, and 1.2%, respectively, in the IC group and 40.7%, 11.1%, and 7.4% in the VEN-comb group. Among the assessable patients, 55.4% and 40.7% did not respond to the IC and VEN-comb regimens, respectively. Overall response rate (ORR) encompassing CR, CRi, and MLFS appeared to be higher in the VEN-comb group (59.3%) compared to the IC group (44.0%), although there was no statistical difference (p = 0.081). Among the responding patients, cytogenetic response was achieved in 68.8% and 90.9% (p = 0.350), and WT1low responders were observed in 74.3% and 70.4% (p = 0.732) of the IC and VEN-comb groups, respectively. The mortality rate at 30 days, 60 days, and 90 days from initiation of each salvage therapy was 4.5%, 10.1%, and 16.9%, respectively, among patients receiving IC and 0.0%, 5.6%, and 11.1% among patients who received the VEN-comb regimen. Regarding bridging to SCT, the percentage of patients who underwent allo-SCT after salvage therapy was 68.5% in both the IC and VEN-comb groups (p = 0.998), where 62.3% (IC) and 86.5% (VEN) of patients achieved either CR, CRi, or MLFS at SCT (p = 0.010). When comparing the times from initiating salvage therapy to SCT, the median time to SCT was shorter in patients who received VEN-comb (median 103 days) compared to patients receiving IC (median 140 days) (p = 0.013).
If focusing on patients in the first salvage setting only (Supplementary Table 2), ORR significantly differed by treatment group: 46.5% and 65.9% in the IC and VEN-comb groups, respectively (p = 0.035). Significant differences were observed in percentage of bridging to SCT with a leukemia-free state (64.4% in the IC group vs 89.7% in the VEN-comb group, p = 0.012), and median time to SCT (median 142 days in the IC group vs 109 days in the VEN-comb group, p = 0.021).
Relevant factors for clinical outcomes
Response
Table 3 shows the results of the univariate and multivariate analyses for identifying relevant factors affecting response and survival. In the univariate and multivariate analysis, ELN-poor cytogenetics (p = 0.010, odds ratio (OR) 95% confidence interval (CI) 0.138–0.760) decreased the chances of achieving response. Among the patients in the first-line salvage-only setting (Supplementary Table 3), VEN-comb was significantly superior to IC in achieving response (p = 0.023, OR = 3.215 (95% CI: 1.174–8.801)), although a significant difference between the two treatment groups was not shown in the overall patient population. In addition, ELN-poor cytogenetics (p = 0.010, OR = 0.323, (95% CI: 0.138–0.760)), relapsed disease (p = 0.006, OR = 0.134, (95% CI: 0.032–0.565)) and mutated FLT3-ITD (p = 0.039, OR = 0.145, (95% CI: 0.145–0.950)) decreased the chances of achieving response in multivariate analysis.
Survival
Given that the use of VEN-comb was started later in the study period, the median follow-up duration was significantly longer in the IC group (22.5 months) compared to the VEN-comb group (11.3 months) (p < 0.001), after which the median OS was 8.9 months (95% CI, 5.4–12.4) and 12.4 months (95% CI: 9.5–15.2), respectively (p = 0.724) (Table 2) (Figure 2). As shown in Table 3, ELN-poor cytogenetics, relapsed disease (vs primary refractory disease), mutated FLT3-ITD, non-mutated CEBPA, mutated TP53, and no response to salvage therapy were associated with poor survival in univariate analysis. In multivariate analysis, secondary AML (p = 0.023, hazard ratio (HR) = 2.359 (95% CI: 1.128–4.935)), ELN-poor cytogenetics (p = 0.037, HR = 1.910 (95% CI: 1.040–3.508)), mutation in FLT3-ITD (p = 0.001, HR = 2.761 (95% CI: 1.497–5.093)), NPM1 (p = 0.021, HR = 2.187 (95% CI: 1.128–4.242)), or TP53 (p = 0.012, HR = 1.297 (95% CI: 1.289–8.072)), and no response to salvage therapy (p < 0.001, HR = 4.854 (95% CI: 2.867–8.220)) were independent prognostic factors for poor survival. Regarding the salvage options, there was no significant difference in OS between the IC-treated and VEN-comb-treated patients either in univariate or multivariate analysis (p = 0.773, HR = 0.902 (95% CI: 0.448–1.816)).

Overall survival.
Anti-leukemic responses, bridging to stem cell transplantation, and survival.

CI, confidence interval; CR, complete remission; CRi, CR with incomplete hematologic recovery; MLFS, morphologic leukemia-free state; SCT, stem cell transplantation; WT1, Wilms’ tumor gene 1.
Response information was not available in six patients in the IC group, whose death occurred before response assessment.
Cytogenetic response was assessed only in responders with confirmed cytogenetic abnormalities at baseline (prior to salvage treatment) and with available cytogenetic data after salvage treatment.
Univariate and multivariate analyses for response and survival.

CI, confidence interval; ELN, European Leukemia Net; HR, hazard ratio; IC, intensive chemotherapy; OR, odds ratio; SCT, stem cell transplantation; VEN, venetoclax.
Subgroup analysis for response and survival
Figure 3 compares the response rates between the two salvage arms for each subgroup. Among patients aged <50 years, who were in the first salvage setting and had no prior exposure to SCT, the use of VEN-comb was significantly superior to that of IC for blast clearance. For salvage ICs and VEN-comb, the response rate were 39.1% vs 62.9% (p = 0.049, aged <50 years), 45.6% vs 65.9% (p = 0.041, first salvage), and 42.9% vs 63.6% (p = 0.050, no prior SCT), respectively. Regarding the response to first-line therapy, both relapsed and refractory patients tended to have more chance of achieving response with VEN-comb, but without statistical significance. For salvage ICs and VEN-comb, the response rate were 47.7% vs 64.5% in refractory disease (p = 0.320), and 33.3% vs 52.2% in relapsed disease (p = 0.122).

Subgroup analysis of response.
While a trend toward better responses with VEN-comb than with IC was noted across multiple subgroups, treatment option did not significantly impact OS across subgroups (Figure 4), except in patients with FLT3-ITD mutation. In these patients, the median OS was 6.5 months in the IC group versus 13.3 months in the VEN-comb group (p = 0.009) after median follow-up durations of 20.3 months (IC) and 11.3 months (VEN-comb).
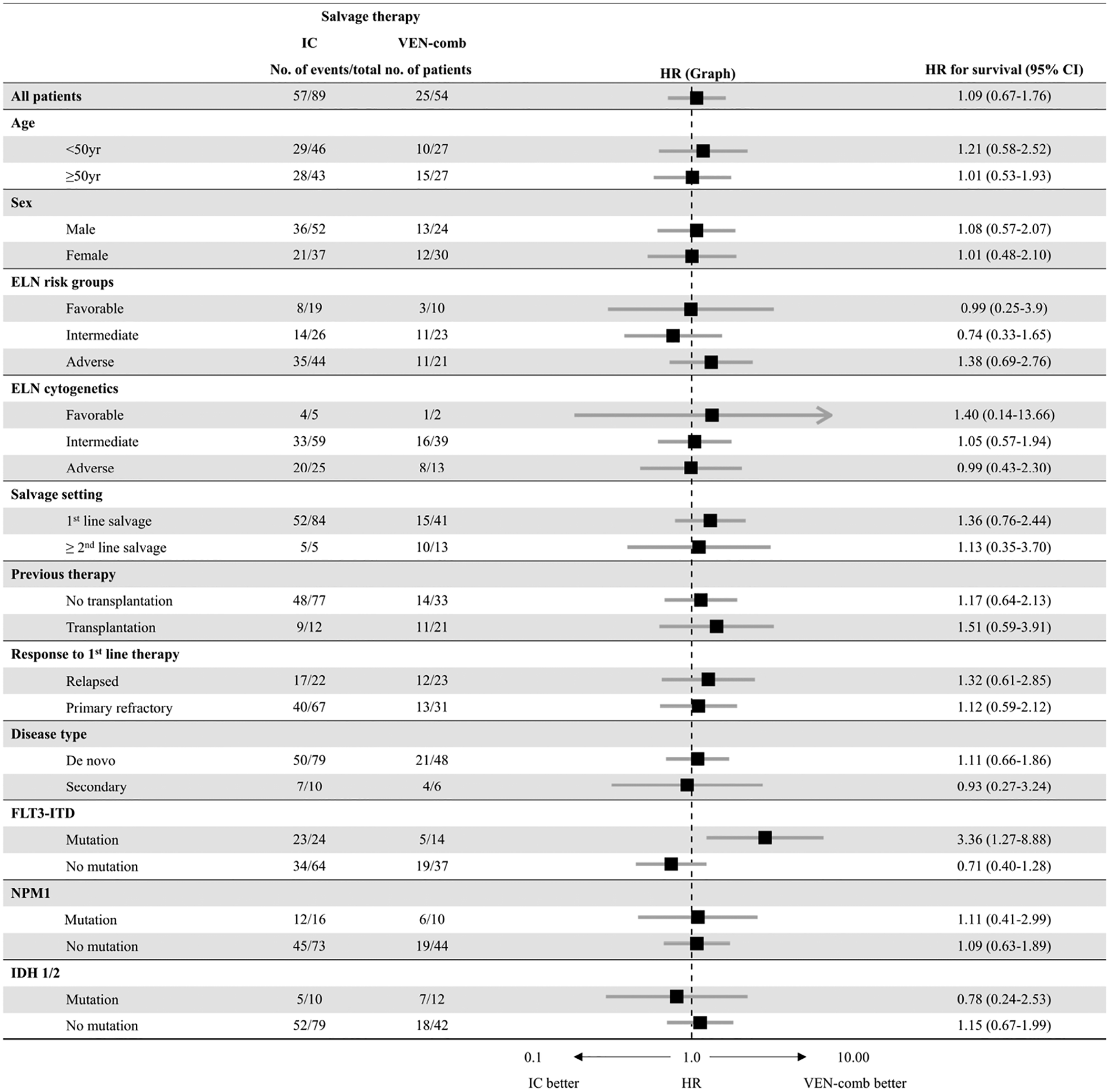
Subgroup analysis of overall survival.
Duration of hospitalization and blood product transfusions
As listed in Table 2, the length of hospital stay and the transfused units of blood product were smaller for the VEN-comb group. The median hospitalization durations in each group were 55 days (IC) and 34 days (VEN-comb) (p = 0.012). Furthermore, the median total transfused amounts were 12 versus 9 units of RBC (IC vs VEN-comb, p = 0.041) and 73 versus 36 units for PLT (IC vs VEN-comb, p = 0.008).
Discussion
VEN-combined therapy, especially VEN with HMA, has been established as a major treatment of newly diagnosed elderly AML patients. At the same time, a VEN-containing regimen has been used off-label for R/R AML in practice,10–12,14 which in turn generates evidence that the regimen is effective in such patients. However, these studies included patients of various medical situations; some initiated treatment aiming to prolong survival through continued cycles of this regimen, whereas others were intending to be cured with bridging to SCT after VEN-comb treatment. In consequence, patients of each study had various prior treatment exposures; for example, HMA, target agents, IC, or SCT, according to the ultimate treatment goal at diagnosis, and clinical outcomes were analyzed regardless of prior treatment lines the patient had received. Furthermore, the studies usually focused on the VEN-comb treatment itself, rather than comparing it with other conventional therapeutics in the R/R setting. From this point of view, we attempted to determine how VEN-comb compares to salvage IC for patients unsuccessful with prior intense treatment but with continued curative intention. Given the idea that the later the salvage lines, the worse the outcomes irrespective of treatment, the patients analyzed here were restricted based on salvage line.
As a result, we revealed that VEN-comb was at least comparable to salvage IC in the aspects of efficacy and survival in the first or second salvage setting of R/R AML. Overall, the respective outcomes of the IC and VEN-comb groups were 44.0% and 59.3% for overall response (p = 0.081) and 8.9 and 12.4 months for median OS (p = 0.724). When focusing on patients in the first salvage setting only, the efficacy of VEN-comb was greater than that of IC, showing a significantly superior ORR. The bridging to SCT rate was the same in the two groups (68.5%), but the percentage of patients who underwent SCT with blast clearance was significantly higher with VEN-comb (86.5%) than with IC (62.3%) (p = 0.010). One of the notable findings of this study was the relatively lower early mortality rate in the VEN-comb group. The median time to SCT was significantly shorter in the VEN-comb group, which might reflect that the steps toward SCT were less problematic in patients with this less-intensive treatment, although the interpretation was limited by the complexity of medical and non-medical issues such as acceptance of national insurance coverage for SCT and shortage of hospital beds for SCT compared to the number of waiting patients, which usually delays the timing of transplantation.
Regarding the response assessment, we classified patients of CR, CRi, and MLFS as responders. In recent publications, MLFS has been regarded as a response, in addition to CR and CRi.6,10–12,14,15,41,42 The term ‘MLFS’ seems to appear more often with the use of VEN-comb in AML and might be on the grounds that its intensity lies between that of HMA (or LDAC) alone and IC. However, the prognostic impact of count recovery on post-transplant outcomes in AML has shown conflicting results.43–45 Recently, Pabon et al. raised this issue, 46 revealing that MLFS following the formal Cheson et al. definition is sufficient for successful SCT by showing long-term remission in a substantial portion of patients, whereas subsets with absolute neutrophil count (ANC) < 200 had poor outcomes following SCT. In this study, MLFS was observed more frequently in responding patients treated with VEN-comb (4 of 32) than with IC (1 of 37). Four patients receiving the VEN-comb regimen were capable of bridging to SCT, among which two had experienced AML from myelodysplastic syndrome. These two patients with secondary AML were vulnerable to count recovery and were severely neutropenic (ANC < 200) during and/or after salvage VEN-comb treatment. The two eventually died from infectious complications at 67 and 76 days after SCT. Relatively higher proportion of MLFS among the responders compared to either CR or CRi, and the unfavorable survival observed in patients with secondary AML receiving the VEN-comb regimen seems to be consistent with the results from previous studies.10,11,47 Although it is uncertain whether higher mortality is caused primarily by its own adverse characteristics or mainly related to lack of count recovery in this distinct group of AML, we suggest that patients with secondary AML who will receive VEN-comb in the R/R setting should be monitored cautiously for prolonged myelosuppression as such with shortening of VEN duration or with strict dose adjustment on concomitant use of CYP3A inhibitors.48,49
In this study, as a partner drug to VEN, a 5-day course of decitabine was used most commonly (48/54), whereas azacitidine (3/54) or LDAC (3/54) accounted for only a small percentage of patients. Regarding the impact of combined agents with VEN, there was a report that azacitidine plus VEN tended to be superior to decitabine plus VEN when used in R/R AML. 14 Although we cannot compare the outcomes between the two HMA regimens due to the small sample size, the outcomes we observed here, where the decitabine combination comprised the majority, were promising, and substantial data either in the new or R/R setting support the comparable or unsurpassed efficacy of decitabine in combination with VEN.6,10,47
Recently, VEN in combination with intensive therapy has also announced excellent results with acceptable toxicity profiles in R/R setting by British and US researchers.50,51 In these reports, VEN in combination with fludarabine, idarubicine, and cytarabine-based attenuated intensive regimen was used in a largely younger R/R AML population (median age 47, 50 49, 50 and 51), 51 which is quite similar to this study. Among the patients receiving FLAG-IDA + VEN as their first or second salvage only, the response rate was remarkably high with the composite CR (CRc, defined by CR and CRi) rate of 76% and the observed median OS was 14 months after median follow-up period of 12 months. 50 When comparing these outcomes with our results in VEN-comb group, OS was comparable but CRc rate (51.8%) was quite lower in our study. This might reflect the possible superiority of VEN in combined with IC rather than combined with less-intensive treatment for medically fit R/R patients. However, this result might also be explained by the larger number of patients with high-risk features (such as prior SCT and FLT3-ITD mutation) included in our study. At this point, it is difficult to conclude which is superior between these two different approaches, unless a solid conclusion is drawn from a head-to-head comparative study.
As for the specific molecular profiles, mutations in NPM1 and IDH 1/2 have conferred better response and survival with VEN-containing treatment.6–9,14,47 In our study, however, neither the survival nor the response rate in NPM1 or IDH 1/2-mutated patients receiving VEN-comb was superior to those of the remaining patients, and the advantageous role of VEN-comb over IC was not prominent. On the contrary, the findings from patients with FLT3-ITD mutation, which showed relatively superior survival in the VEN-comb group than in IC-treated patients, were interesting, although they might be attributed largely to extremely poor outcomes of FLT3-mutated R/R AML patients receiving salvage IC. The presence of this mutation is particularly important because the target inhibitor, gilteritinib, is available. 52 In practice, owing to the delayed approval for use in our country and its cost, VEN-comb was one of the options for patients with mutated FLT3 in the R/R setting outside the context of a clinical trial. In this study, there were 15 FLT3-mutated patients receiving the VEN-comb regimen, 11 of whom (ITD mutation only, n = 9; both ITD and FLT3 mutations, n = 1; TKD mutation only, n = 1) received this regimen as their first-line salvage. In this subgroup, the ORR was 54.5%, and the response rate was 36.4% when accounting for CR/CRi only, in line with data from prior studies.11,14 When considering the result from the Phase-III ADMIRAL trial, 52 where the composite CR was reported up to 54.3%, it might be better to prioritize the FLT3 inhibitor over the VEN-comb regimen if patients have a mutated FLT3 in R/R AML, although the findings we observed should not be generalized.
We acknowledge that there are substantial limitations in this study. One of the major weaknesses was the retrospective nature, in which the baseline characteristics between the two treatment groups were not well balanced and the information on genetic mutations was not obtained in a timely manner. And, the small number of cases made it hard for us to draw a solid conclusion with insufficient statistical power. Furthermore, there was a significant gap in follow-up periods between the two treatment groups, with the VEN-comb group having the much shorter period. This potentially could underestimate the long-term benefit and fail to detect delayed hazards, 53 preventing accurate comparison of survival benefit between the two treatment groups. In addition, although a treatment decision for R/R AML patients with prior HMA exposure is one of the major challenging issues, we could not provide an answer to that issue because this study mainly targeted patients who had previously received IC. Finally, the information on minimal residual disease (MRD) measured by currently recommend method54,55 was not available in this study. Nevertheless, this study had strengths in reflecting reality. Also, to the best of our knowledge, this is the first report comparing the use of VEN-comb with salvage IC confined in the setting of medically fit R/R AML.
In summary, this study showed that VEN-comb treatment is a feasible option for R/R AML. VEN-comb provides a comparable anti-leukemic response and survival to salvage IC and provides a bridge to SCT with better disease control. Lesser use of medical resources represented by shorter hospitalization stays and lower transfusion amounts were additional strengths of this regimen. However, due to the limitations of the small number of cases and the retrospective nature, further analyses using prospective well-designed studies are necessary to confirm our findings and to provide better treatment guidance for R/R AML patients.
Supplemental Material
sj-docx-1-tah-10.1177_20406207221081637 – Supplemental material for A retrospective comparison of salvage intensive chemotherapy versus venetoclax-combined regimen in patients with relapsed/refractory acute myeloid leukemia (AML)
Supplemental material, sj-docx-1-tah-10.1177_20406207221081637 for A retrospective comparison of salvage intensive chemotherapy versus venetoclax-combined regimen in patients with relapsed/refractory acute myeloid leukemia (AML) by Silvia Park, Daehun Kwag, Tong Yoon Kim, Jong Hyuk Lee, Joon yeop Lee, Gi June Min, Sung Soo Park, Seung-Ah Yahng, Young-Woo Jeon, Seung-Hwan Shin, Jae-Ho Yoon, Sung-Eun Lee, Byung Sik Cho, Ki-Seong Eom, Yoo-Jin Kim, Seok Lee, Chang-Ki Min, Seok-Goo Cho, Jong Wook Lee and Hee-Je Kim in Therapeutic Advances in Hematology
Supplemental Material
sj-docx-2-tah-10.1177_20406207221081637 – Supplemental material for A retrospective comparison of salvage intensive chemotherapy versus venetoclax-combined regimen in patients with relapsed/refractory acute myeloid leukemia (AML)
Supplemental material, sj-docx-2-tah-10.1177_20406207221081637 for A retrospective comparison of salvage intensive chemotherapy versus venetoclax-combined regimen in patients with relapsed/refractory acute myeloid leukemia (AML) by Silvia Park, Daehun Kwag, Tong Yoon Kim, Jong Hyuk Lee, Joon yeop Lee, Gi June Min, Sung Soo Park, Seung-Ah Yahng, Young-Woo Jeon, Seung-Hwan Shin, Jae-Ho Yoon, Sung-Eun Lee, Byung Sik Cho, Ki-Seong Eom, Yoo-Jin Kim, Seok Lee, Chang-Ki Min, Seok-Goo Cho, Jong Wook Lee and Hee-Je Kim in Therapeutic Advances in Hematology
Footnotes
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors wish to acknowledge the financial support of the Catholic Medical Center Research Foundation made in the program year of 2020.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.